Persistent Left Superior Vena Cava with Absent Right Superior Vena Cava and Discrete Subaortic Stenosis Diagnosed in a Patient with Sick Sinus Syndrome: A Case Report and Brief Review of the Literature

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Case Report
3. Discussion
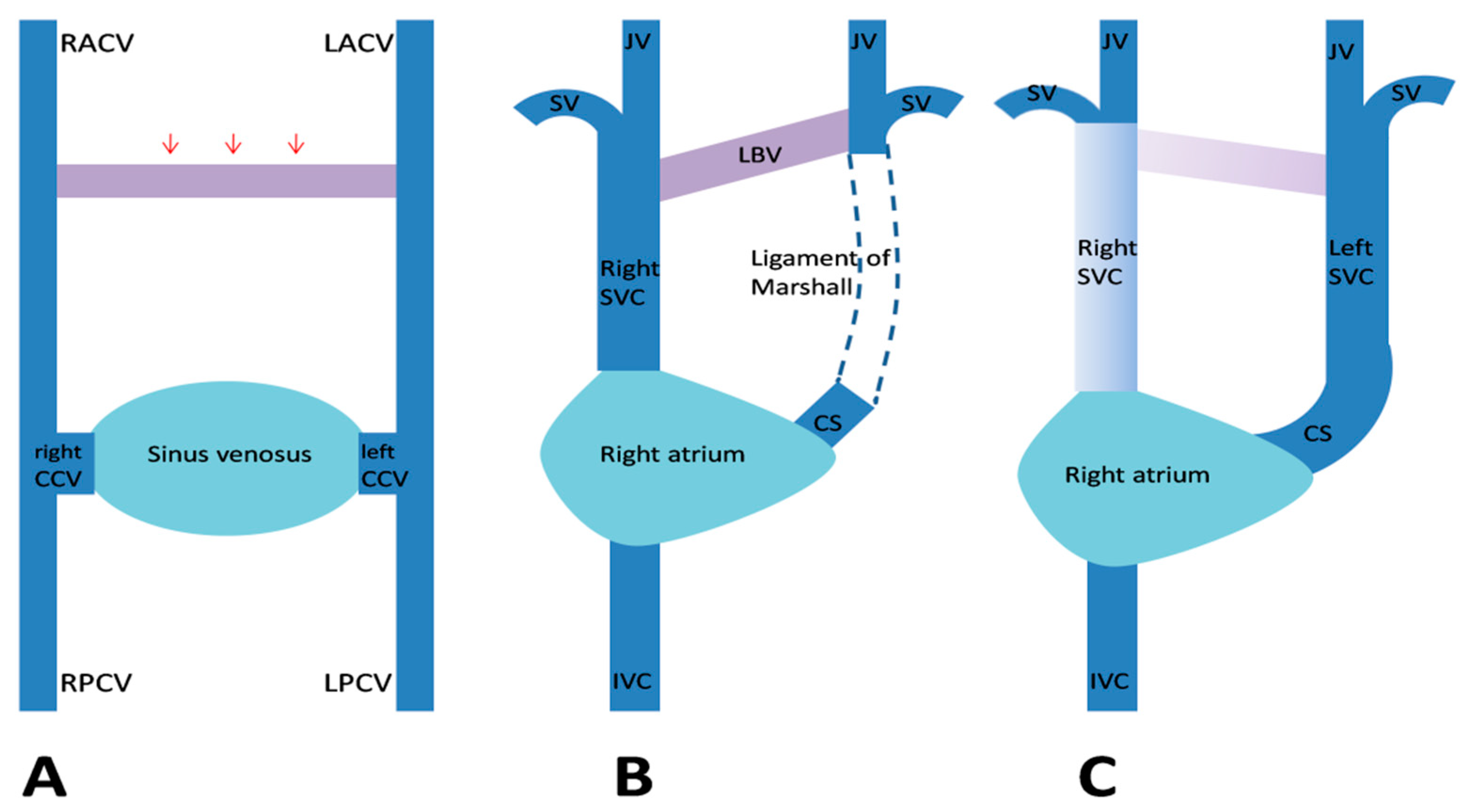
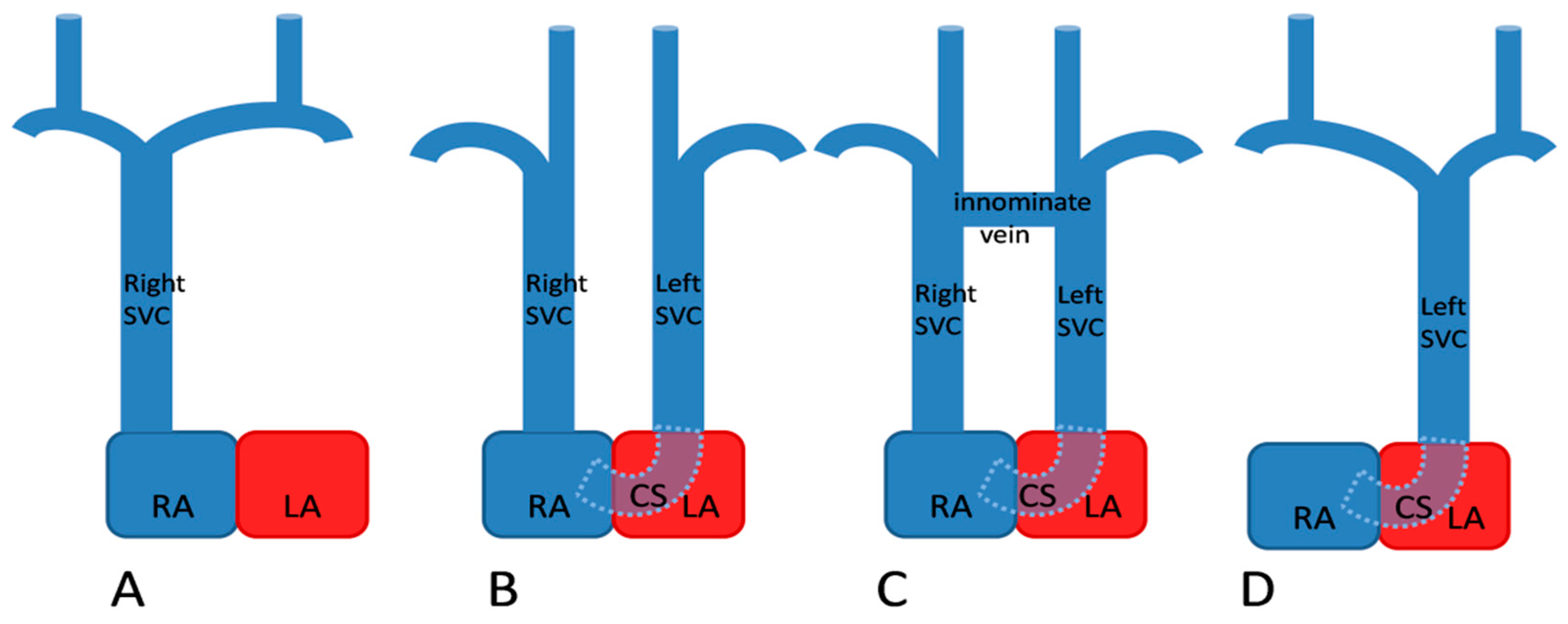
3.1. Embryology and Anatomic Variants
3.2. Associated Congenital Anomalies
3.3. Practical Implications
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Campbell, M.; Deuchar, D.C. The left-sided superior vena cava. Br. Heart J. 1954, 16, 423–439. [Google Scholar] [CrossRef] [PubMed]
- Kochav, J. Persistent Left Superior Vena Cava. In Adult Congenital Heart Disease in Clinical Practice; DeFaria Yeh, D., Bhatt, A., Eds.; Springer: Cham, Switzerland, 2018; pp. 143–150. ISBN 978-3-319-67420-9. [Google Scholar] [CrossRef]
- Bartram, U.; van Praagh, S.; Levine, J.C.; Hines, M.; Bensky, A.S.; van Praagh, R. Absent right superior vena cava in visceroatrial situs solitus. Am. J. Cardiol. 1997, 80, 175–183. [Google Scholar] [CrossRef]
- Biffi, M.; Boriani, G.; Frabetti, L.; Bronzetti, G.; Branzi, A. Left superior vena cava persistence in patients undergoing pacemaker or cardioverter-defibrillator implantation: A 10-year experience. Chest 2001, 120, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Couvreur, T.; Ghaye, B. Left superior vena cava. In Integrated Cardiothoracic Imaging with MDCT; Rémy-Jardin, M., Remy, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 289–305. ISBN 978-3-540-72387-5. [Google Scholar] [CrossRef]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.A.; Cleland, J.; Deharo, J.C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: The task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J. 2013, 34, 2281–2329. [Google Scholar] [CrossRef]
- Baumgartner, H.; Bonhoeffer, P.; De Groot, N.M.; de Haan, F.; Deanfield, J.E.; Galie, N.; Gatzoulis, M.A.; Gohlke-Baerwolf, C.; Kaemmerer, H.; Kilner, P.; et al. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010). Eur. Heart J. 2010, 31, 2915–2957. [Google Scholar] [CrossRef]
- van der Linde, D.; Takkenberg, J.J.; Rizopoulos, D.; Heuvelman, H.J.; Budts, W.; van Dijk, A.P.; Witsenburg, M.; Yap, S.C.; Bogers, A.J.; Silversides, C.K.; et al. Natural history of discrete subaortic stenosis in adults: A multicentre study. Eur. Heart J. 2013, 34, 1548–1556. [Google Scholar] [CrossRef]
- Isik, O.; Disli, O.M.; Bas, T.; Kutsal, A. A rare congenital anomaly: Surgery of combined discrete subaortic membrane complicated by the absence of the superior vena cava. J. Turgut Ozal Med. Cent. 2014, 21, 139–141. [Google Scholar] [CrossRef]
- Darcin, O.T.; Yagdi, T.; Atay, Y.; Engin, C.; Levent, E.; Buket, S.; Alayunt, E.A. Discrete subaortic stenosis: Surgical outcomes and follow-up results. Tex. Heart Inst. J. 2003, 30, 286–292. [Google Scholar]
- Ganju, N.K.; Kandoria, A.; Thakur, S.; Ganju, S.A. A Constellation of Cardiac Anomalies: Beyond Shone’s Complex. Heart Views 2016, 17, 23–26. [Google Scholar] [CrossRef]
- Derbent, M.; Orün, U.A.; Varan, B.; Mercan, S.; Yilmaz, Z.; Sahin, F.I.; Tokel, K. A new syndrome within the oculo-auriculo-vertebral spectrum: Microtia, atresia of the external auditory canal, vertebral anomaly, and complex cardiac defects. Clin. Dysmorphol. 2005, 14, 27–30. [Google Scholar] [CrossRef]
- Demirkol, S. A Combination of Persistent Left Superior Vena Cava and Subaortic Discrete Membrane. J. Clin. Anal. Med. 2013, 4, 349–351. [Google Scholar] [CrossRef]
- Nemani, L.; Barik, R.; Patnaik, A.N.; Mishra, R.C.; Rao, A.M.; Kapur, P. Coffin-Siris syndrome with the rarest constellation of congenital cardiac defects: A case report with review of literature. Ann. Pediatr. Cardiol. 2014, 7, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Ratliff, H.L.; Yousufuddin, M.; Lieving, W.R.; Watson, B.E.; Malas, A.; Rosencrance, G.; McCowan, R.J. Persistent left superior vena cava: Case reports and clinical implications. Int. J. Cardiol. 2006, 113, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Irwin, R.B.; Greaves, M.; Schmitt, M. Left superior vena cava: Revisited. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Benson, R.E.; Songrug, T. CT appearance of persistent left superior vena cava, anomalous right superior pulmonary venous return into the right-sided superior vena cava and a sinus venosus-type atrial septal defect. Br. J. Radiol. 2009, 82, e235–e239. [Google Scholar] [CrossRef] [PubMed]
- Tal Geva. Thoracic Key Home Page. Available online: https://thoracickey.com/abnormal-systemic-venous-connections/ (accessed on 15 May 2020).
- Bjerregaard, P.; Laursen, H.B. Persistent left superior vena cava. Incidence, associated congenital heart defects and frontal plane P-wave axis in a paediatric population with congenital heart disease. Acta Paediatr. Scand. 1980, 69, 105–108. [Google Scholar] [CrossRef]
- Cape, E.G.; Vanauker, M.D.; Sigfússon, G.; Tacy, T.A.; del Nido, P.J. Potential role of mechanical stress in the etiology of pediatric heart disease: Septal shear stress in subaortic stenosis. J. Am. Coll. Cardiol. 1997, 30, 247–254. [Google Scholar] [CrossRef]
- Agnoletti, G.; Annecchino, F.; Preda, L.; Borghi, A. Persistence of the left superior caval vein: Can it potentiate obstructive lesions of the left ventricle? Cardiol. Young 1999, 9, 285–290. [Google Scholar] [CrossRef]
- Kalfa, D.; Ghez, O.; Kreitmann, B.; Metras, D. Secondary subaortic stenosis in heart defects without any initial subaortic obstruction: A multifactorial postoperative event. Eur. J. Cardiothorac. Surg. 2007, 32, 582–587. [Google Scholar] [CrossRef]
- Sheikh, A.S.; Mazhar, S. Persistent left superior vena cava with absent right superior vena cava: Review of the literature and clinical implications. Echocardiography 2014, 31, 674–679. [Google Scholar] [CrossRef]
- Shah, S.S.; Teague, S.D.; Lu, J.C.; Dorfman, A.L.; Kazerooni, E.A.; Agarwal, P.P. Imaging of the coronary sinus: Normal anatomy and congenital abnormalities. Radiographics 2012, 32, 991–1008. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, I.A.; Shala, M.B.; Johns, C. Echocardiography of the coronary sinus in adults. Clin. Cardiol. 2000, 23, 149–154. [Google Scholar] [CrossRef]
- Saranteas, T.; Mandila, C.; Poularas, J.; Papanikolaou, J.; Patriankos, A.; Karakitsos, D.; Karabinis, A. Transesophageal echocardiography and vascular ultrasound in the diagnosis of catheter-related persistent left superior vena cava thrombosis. Eur. J. Echocardiogr. 2009, 10, 452–455. [Google Scholar] [CrossRef] [PubMed]
- Batouty, N.M.; Sobh, D.M.; Gadelhak, B.; Sobh, H.M.; Mahmoud, W.; Tawfik, A.M. Left superior vena cava: Cross-sectional imaging overview. Radiol. Med. 2020, 125, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Lenox, C.C.; Hashida, Y.; Anderson, R.H.; Hubbard, J.D. Conduction tissue anomalies in absence of the right superior caval vein. Int. J. Cardiol. 1985, 8, 251–260. [Google Scholar] [CrossRef]
- Morgan, D.R.; Hanratty, C.G.; Dixon, L.J.; Trimble, M.; O’Keeffe, D.B. Anomalies of cardiac venous drainage associated with abnormalities of cardiac conduction system. Europace 2002, 4, 281–287. [Google Scholar] [CrossRef]
- Moorthy, N.; Kapoor, A.; Kumar, S. Isolated persistent left-sided superior vena cava, giant coronary sinus, atrial tachycardia and heart failure in a child. Indian Heart J. 2013, 65, 603–606. [Google Scholar] [CrossRef]
- Mora, G. A novel method of placing right ventricular leads in patients with persistent left superior vena cava using a conventional j stylet. Indian Pacing Electrophysiol. J. 2014, 14, 65–74. [Google Scholar] [CrossRef]
- Yildiz, O. How to Safely Implant a Dual-Chamber Pacemaker for Right Ventricular Outflow Tract Pacing in a Patient with Persistent Left Superior Vena Cava: A Step by Step Guide. Acta Cardiol. Sin. 2019, 35, 430–432. [Google Scholar] [CrossRef]
- Sinha, S.K.; Goel, A.; Razi, M.; Jha, M.J.; Mishra, V.; Aggarwaal, P.; Thakur, R.; Krishna, V.; Pandey, U.; Varma, C.M. Permanent Pacemaker Implantation in Patients With Isolated Persistent Left Superior Vena Cava From a Right-Sided Approach: Technical Considerations and Follow-Up Outcome. Cardiol. Res. 2019, 10, 18–23. [Google Scholar] [CrossRef]
- Biffi, M.; Bertini, M.; Ziacchi, M.; Martignani, C.; Valzania, C.; Diemberger, I.; Branzi, A.; Boriani, G. Clinical implications of left superior vena cava persistence in candidates for pacemaker or cardioverter-defibrillator implantation. Heart Vessel. 2009, 24, 142–146. [Google Scholar] [CrossRef]
- Rathakrishnan, S.S.; Kaliappan, T.; Gopalan, R. Beware of Venous Anomalies in Young Patients with Sick Sinus Syndrome: A Report of Two Cases of Sick Sinus Syndrome with Systemic Venous Anomalies. Heart Views 2015, 16, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Xu, Q.; Liao, H.T.; Asvestas, D.; Letsas, K.P.; Li, Y. Transvenous dual-chamber pacemaker implantation in patients with persistent left superior vena cava. BMC Cardiovasc. Disord. 2019, 19, 100. [Google Scholar] [CrossRef] [PubMed]
- Razi, M.; Madaan, A.; Goel, A.; Sinha, S.K. Troubleshooting during pacemaker implant in persistent left superior vena cava with absence of right superior vena cava (isolated persistent left superior vena cava). Avicenna J. Med. 2016, 6, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.K.; Punnam, S.R.; Verma, G.; Ruberg, F.L. Persistent left superior vena cava: A case report and review of literature. Cardiovasc. Ultrasound 2008, 6, 50. [Google Scholar] [CrossRef] [PubMed]
- Fernando, R.J.; Johnson, S.D. Inability to Utilize Retrograde Cardioplegia due to a Persistent Left Superior Vena Cava. Case Rep. Anesthesiol. 2017, 2017, 4671856. [Google Scholar] [CrossRef]
- Calcagni, G.; Ou, P.; Marini, D.; Bonnet, D.; Agnoletti, G. Atresia of the coronary sinus ostium: Surgical implications. Int. J. Cardiol. 2007, 116, 92–94. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demșa, I.; Crișu, D.; Haba, C.M.Ș.; Ursaru, A.M.; Afrăsânie, V.-A.; Costache, I.I.; Petriș, A.O.; Tesloianu, D.N. Persistent Left Superior Vena Cava with Absent Right Superior Vena Cava and Discrete Subaortic Stenosis Diagnosed in a Patient with Sick Sinus Syndrome: A Case Report and Brief Review of the Literature. Diagnostics 2020, 10, 847. https://doi.org/10.3390/diagnostics10100847
Demșa I, Crișu D, Haba CMȘ, Ursaru AM, Afrăsânie V-A, Costache II, Petriș AO, Tesloianu DN. Persistent Left Superior Vena Cava with Absent Right Superior Vena Cava and Discrete Subaortic Stenosis Diagnosed in a Patient with Sick Sinus Syndrome: A Case Report and Brief Review of the Literature. Diagnostics. 2020; 10(10):847. https://doi.org/10.3390/diagnostics10100847
Chicago/Turabian StyleDemșa, Irina, Daniela Crișu, Cristian Mihai Ștefan Haba, Andreea Maria Ursaru, Vlad-Adrian Afrăsânie, Irina Iuliana Costache, Antoniu Octavian Petriș, and Dan Nicolae Tesloianu. 2020. "Persistent Left Superior Vena Cava with Absent Right Superior Vena Cava and Discrete Subaortic Stenosis Diagnosed in a Patient with Sick Sinus Syndrome: A Case Report and Brief Review of the Literature" Diagnostics 10, no. 10: 847. https://doi.org/10.3390/diagnostics10100847
APA StyleDemșa, I., Crișu, D., Haba, C. M. Ș., Ursaru, A. M., Afrăsânie, V.-A., Costache, I. I., Petriș, A. O., & Tesloianu, D. N. (2020). Persistent Left Superior Vena Cava with Absent Right Superior Vena Cava and Discrete Subaortic Stenosis Diagnosed in a Patient with Sick Sinus Syndrome: A Case Report and Brief Review of the Literature. Diagnostics, 10(10), 847. https://doi.org/10.3390/diagnostics10100847