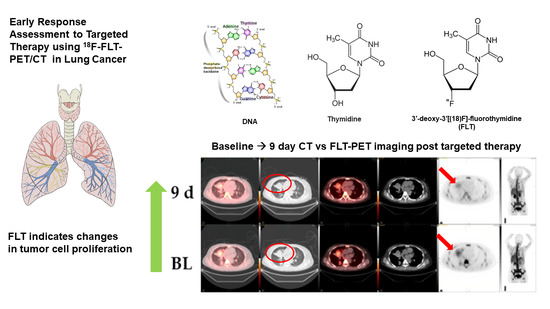
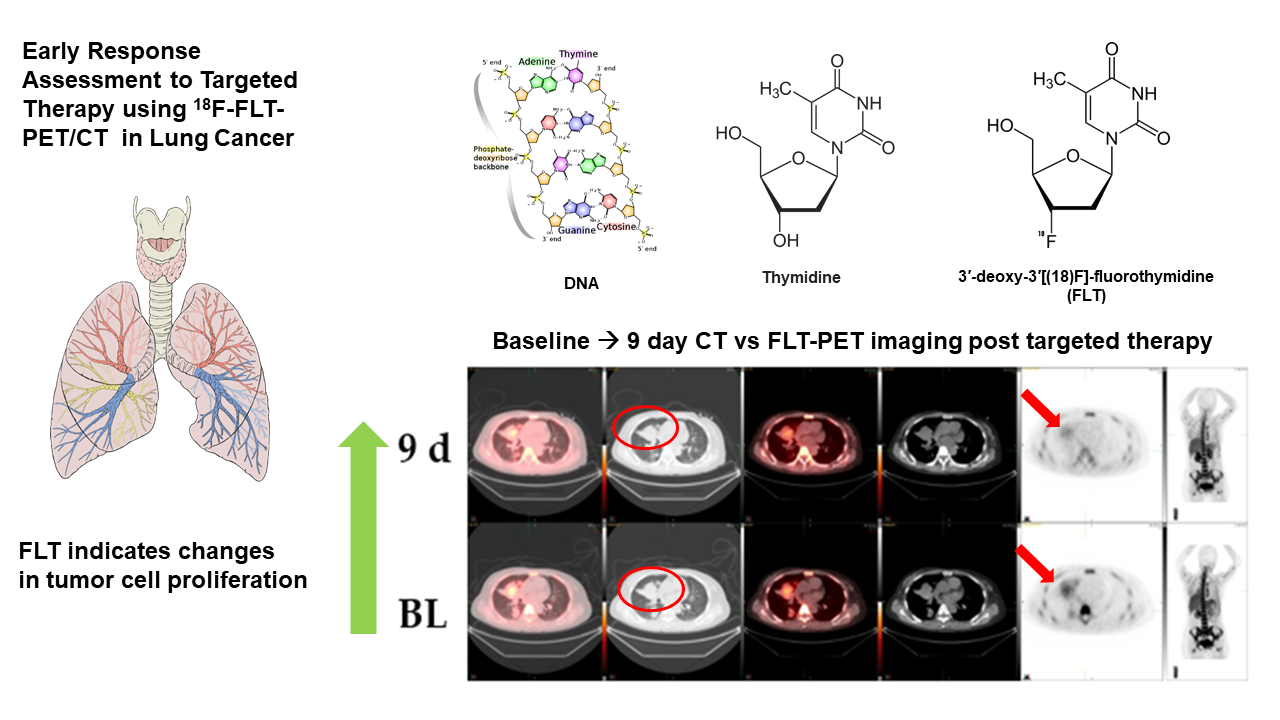
Early Response Assessment to Targeted Therapy Using 3′-deoxy-3′[(18)F]-Fluorothymidine (18F-FLT) PET/CT in Lung Cancer


Abstract
1. Introduction
2. Materials and Methods
2.1. PET/CT Study
2.2. 18F-FLT PET/CT Scan Interpretation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Szyszko, T.A.; Yip, C.; Szlosarek, P.; Goh, V.; Cook, G.J. The role of new PET tracers for lung cancer. Lung Cancer 2016, 94, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Bollineni, V.R.; Kramer, G.M.; Jansma, E.P.; Liu, Y.; Oyen, W.J. A systematic review on [18F]FLT-PET uptake as a measure of treatment response in cancer patients. Eur. J. Cancer 2016, 55, 81–97. [Google Scholar] [CrossRef]
- Xie, X.; Chen, H.; Yang, H.; Lin, H.; Zhou, S.; Shen, R.; Lu, C.; Ling, L.; Lin, W.; Liao, Z. Predictive value of positron emission tomography for the prognosis of molecularly targeted therapy in solid tumors. Onco Targets Ther. 2018, 11, 8885–8899. [Google Scholar] [CrossRef] [PubMed]
- Hiniker, S.M.; Sodji, Q.; Quon, A.; Gutkin, P.M.; Arksey, N.; Graves, E.E.; Chin, F.T.; Maxim, P.G.; Diehn, M.; Loo, B.W., Jr. FLT-PET-CT for the Detection of Disease Recurrence After Stereotactic Ablative Radiotherapy or Hyperfractionation for Thoracic Malignancy: A Prospective Pilot Study. Front. Oncol. 2019, 9, 467. [Google Scholar] [CrossRef]
- Sanghera, B.; Wong, W.L.; Sonoda, L.I.; Beynon, G.; Makris, A.; Woolf, D.; Ardeshna, K. FLT PET-CT in evaluation of treatment response. Indian J. Nuclear Med. 2014, 29, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Drontle, D.P.; Wagner, C.R. Designing a pronucleotide stratagem: Lessons from amino acid phosphoramidates of anticancer and antiviral pyrimidines. Mini Rev. Med. Chem. 2004, 4, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Shields, A.F.; Grierson, J.R.; Dohmen, B.M.; Machulla, H.J.; Stayanoff, J.C.; Lawhorn-Crews, J.M.; Obradovich, J.E.; Muzik, O.; Mangner, T.J. Imaging proliferation in vivo with [18F]FLT and positron emission tomography. Nat. Med. 1998, 4, 1334–1336. [Google Scholar] [CrossRef] [PubMed]
- Shen, G.; Ma, H.; Pang, F.; Ren, P.; Kuang, A. Correlations of 18F-FDG and 18F-FLT uptake on PET with Ki-67 expression in patients with lung cancer: A meta-analysis. Acta Radiol. 2018, 59, 188–195. [Google Scholar] [CrossRef]
- McKinley, E.T.; Ayers, G.D.; Smith, R.A.; Saleh, S.A.; Zhao, P.; Washington, M.K.; Coffey, R.J.; Manning, H.C. Limits of [18F]-FLT PET as a biomarker of proliferation in oncology. PLoS ONE 2013, 8, e58938. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Nishiyama, Y.; Ishikawa, S.; Nakano, J.; Chang, S.S.; Bandoh, S.; Kanaji, N.; Haba, R.; Kushida, Y.; Ohkawa, M. Correlation of 18F-FLT and 18F-FDG uptake on PET with Ki-67 immunohistochemistry in non-small cell lung cancer. Eur. J. Nuclear Med. Mol. Imaging 2007, 34, 1610–1616. [Google Scholar] [CrossRef]
- Deppen, S.A.; Blume, J.D.; Kensinger, C.D.; Morgan, A.M.; Aldrich, M.C.; Massion, P.P.; Walker, R.C.; McPheeters, M.L.; Putnam, J.B., Jr.; Grogan, E.L. Accuracy of FDG-PET to diagnose lung cancer in areas with infectious lung disease: A meta-analysis. JAMA 2014, 312, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, Y.; Sui, X.; Zhang, W.; Shi, R.; Zhang, Y.; Dang, Y.; Qiao, Z.; Zhang, B.; Song, W.; et al. Performance of FLT-PET for pulmonary lesion diagnosis compared with traditional FDG-PET: A meta-analysis. Eur. J. Radiol. 2015, 84, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Tian, J.; Yang, X.; Yu, L.; Chen, P.; Xin, J.; Ma, L.; Feng, H.; Tan, Y.; Zhao, Z.; Wu, W. A multicenter clinical trial on the diagnostic value of dual-tracer PET/CT in pulmonary lesions using 3’-deoxy-3’-18F-fluorothymidine and 18F-FDG. J. Nuclear Med. 2008, 49, 186–194. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Xu, B.; Guan, Z.; Liu, C.; Wang, R.; Yin, D.; Zhang, J.; Chen, Y.; Yao, S.; Shao, M.; Wang, H.; et al. Can multimodality imaging using 18F-FDG/18F-FLT PET/CT benefit the diagnosis and management of patients with pulmonary lesions? Eur. J. Nuclear Med. Mol. Imaging 2011, 38, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Li, X.F.; Dai, D.; Song, X.Y.; Liu, J.J.; Zhu, Y.J.; Xu, W.G. Comparison of the diagnostic performance of 18F-fluorothymidine versus 18F-fluorodeoxyglucose positron emission tomography on pulmonary lesions: A meta-analysis. Mol. Clin. Oncol. 2015, 3, 101–108. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pasquini, G.; Giaccone, G. C-MET inhibitors for advanced non-small cell lung cancer. Expert Opin Investig Drugs. Expert Opin. Investig. Drugs 2018, 27, 363–375. [Google Scholar] [CrossRef]
- Awad, M.M.; Oxnard, G.R.; Jackman, D.M.; Heng, J.C.; Dahlberg, S.E.; Jänne, P.A.; Savukoski, D.O.; Hall, D.; Shivdasani, P.; Verma, S.; et al. MET Exon 14 Mutations in Non-Small-Cell Lung Cancer Are Associated With Advanced Age and Stage-Dependent MET Genomic Amplification and c-Met Overexpression. J. Clin. Oncol. 2016, 34, 721–730. [Google Scholar] [CrossRef]
- Cascone, T.; Xu, L.; Lin, H.Y.; Liu, W.; Tran, H.T.; Liu, Y.; Howells, K.; Haddad, V.; Hanrahan, E.; Nilsson, M.B.; et al. The HGF/c-MET Pathway Is a Driver and Biomarker of VEGFR-inhibitor Resistance and Vascular Remodeling in Non-Small Cell Lung Cancer. Clin. Cancer Res. 2017, 23, 5489–5501. [Google Scholar] [CrossRef]
- Allen, M.D.; Luong, P.; Hudson, C.; Leyton, J.; Delage, B.; Ghazaly, E.; Cutts, R.; Yuan, M.; Syed, N.; Lo Nigro, C.; et al. Prognostic and therapeutic impact of argininosuccinate synthetase 1 control in bladder cancer as monitored longitudinally by PET imaging. Cancer Res. 2014, 74, 896–907. [Google Scholar] [CrossRef]
- Sohn, H.J.; Yang, Y.J.; Ryu, J.S.; Oh, S.J.; Im, K.C.; Moon, D.H.; Lee, D.H.; Suh, C.; Lee, J.S.; Kim, S.W. [18F]Fluorothymidine positron emission tomography before and 7 days after gefitinib treatment predicts response in patients with advanced adenocarcinoma of the lung. Clin. Cancer Res. 2008, 14, 7423–7429. [Google Scholar] [CrossRef]
- Trigonis, I.; Koh, P.K.; Taylor, B.; Tamal, M.; Ryder, D.; Earl, M.; Anton-Rodriguez, J.; Haslett, K.; Young, H.; Faivre-Finn, C.; et al. Early reduction in tumour [18F]fluorothymidine (FLT) uptake in patients with non-small cell lung cancer (NSCLC) treated with radiotherapy alone. Eur. J. Nuclear Med. Mol. Imaging 2014, 41, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Everitt, S.J.; Ball, D.L.; Hicks, R.J.; Callahan, J.; Plumridge, N.; Collins, M.; Herschtal, A.; Binns, D.; Kron, T.; Schneider, M.; et al. Differential (18)F-FDG and (18)F-FLT Uptake on Serial PET/CT Imaging Before and During Definitive Chemoradiation for Non-Small Cell Lung Cancer. J. Nuclear Med. 2014, 55, 1069–1074. [Google Scholar] [CrossRef] [PubMed]
- Frings, V.; Yaqub, M.; Hoyng, L.L.; Golla, S.S.; Windhorst, A.D.; Schuit, R.C.; Lammertsma, A.A.; Hoekstra, O.S.; Smit, E.F.; Boellaard, R.; et al. Assessment of simplified methods to measure 18F-FLT uptake changes in EGFR-mutated non-small cell lung cancer patients undergoing EGFR tyrosine kinase inhibitor treatment. J. Nuclear Med. 2014, 55, 1417–1423. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Leimgruber, A.; Möller, A.; Everitt, S.J.; Chabrot, M.; Ball, D.L.; Solomon, B.; MacManus, M.; Hicks, R.J. Effect of Platinum-Based Chemoradiotherapy on Cellular Proliferation in Bone Marrow and Spleen, Estimated by (18)F-FLT PET/CT in Patients with Locally Advanced Non-Small Cell Lung Cancer. J. Nuclear Med. 2014, 55, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Yap, C.S.; Czernin, J.; Fishbein, M.C.; Cameron, R.B.; Schiepers, C.; Phelps, M.E.; Weber, W.A. Evaluation of thoracic tumors with 18F-fluorothymidine and 18F-fluorodeoxyglucosepositron emission tomography. Chest 2006, 129, 393–401. [Google Scholar] [CrossRef]
- Troost, E.G.; Bussink, J.; Oyen, W.J.; Kaanders, J.H. 18F-FDG and 18F-FLT do not discriminate between reactive and metastatic lymph nodes in oral cancer. J. Nuclear Med. 2009, 50, 490–491. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age/Gender/ New Therapy | Diagnosis | Previous Chemotherapy | 18F-FLT SUV Change | Comments |
|---|---|---|---|---|
| 49/male c-MET-inhibitor | small cell lung cancer | cisplatin, etoposide | −38% | FDG-change +2% CT-change 0 % |
| 51/female c-MET-inhibitor | lung adenocarcinoma | erlotinib, carboplatin, gemcitabine/docetaxel, pemetrexed, sorafenib, irinotecan, bevacizumab | −24% | EGFR positive CT-change +2% |
| 59/female MDM2 inhibitor | lung adenocarcinoma | cisplatin, vinorelbine, pemetrexed, cetuximab | −31% | EGFR negative CT-change -6% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kairemo, K.; Santos, E.B.; Macapinlac, H.A.; Subbiah, V. Early Response Assessment to Targeted Therapy Using 3′-deoxy-3′[(18)F]-Fluorothymidine (18F-FLT) PET/CT in Lung Cancer. Diagnostics 2020, 10, 26. https://doi.org/10.3390/diagnostics10010026
Kairemo K, Santos EB, Macapinlac HA, Subbiah V. Early Response Assessment to Targeted Therapy Using 3′-deoxy-3′[(18)F]-Fluorothymidine (18F-FLT) PET/CT in Lung Cancer. Diagnostics. 2020; 10(1):26. https://doi.org/10.3390/diagnostics10010026
Chicago/Turabian StyleKairemo, Kalevi, Elmer B. Santos, Homer A. Macapinlac, and Vivek Subbiah. 2020. "Early Response Assessment to Targeted Therapy Using 3′-deoxy-3′[(18)F]-Fluorothymidine (18F-FLT) PET/CT in Lung Cancer" Diagnostics 10, no. 1: 26. https://doi.org/10.3390/diagnostics10010026
APA StyleKairemo, K., Santos, E. B., Macapinlac, H. A., & Subbiah, V. (2020). Early Response Assessment to Targeted Therapy Using 3′-deoxy-3′[(18)F]-Fluorothymidine (18F-FLT) PET/CT in Lung Cancer. Diagnostics, 10(1), 26. https://doi.org/10.3390/diagnostics10010026