
Advancements in Beta-Adrenergic Therapy and Novel Personalised Approach for Portal Hypertension: A Narrative Review

 , ,
, ,  , ,
, ,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results and Discussions
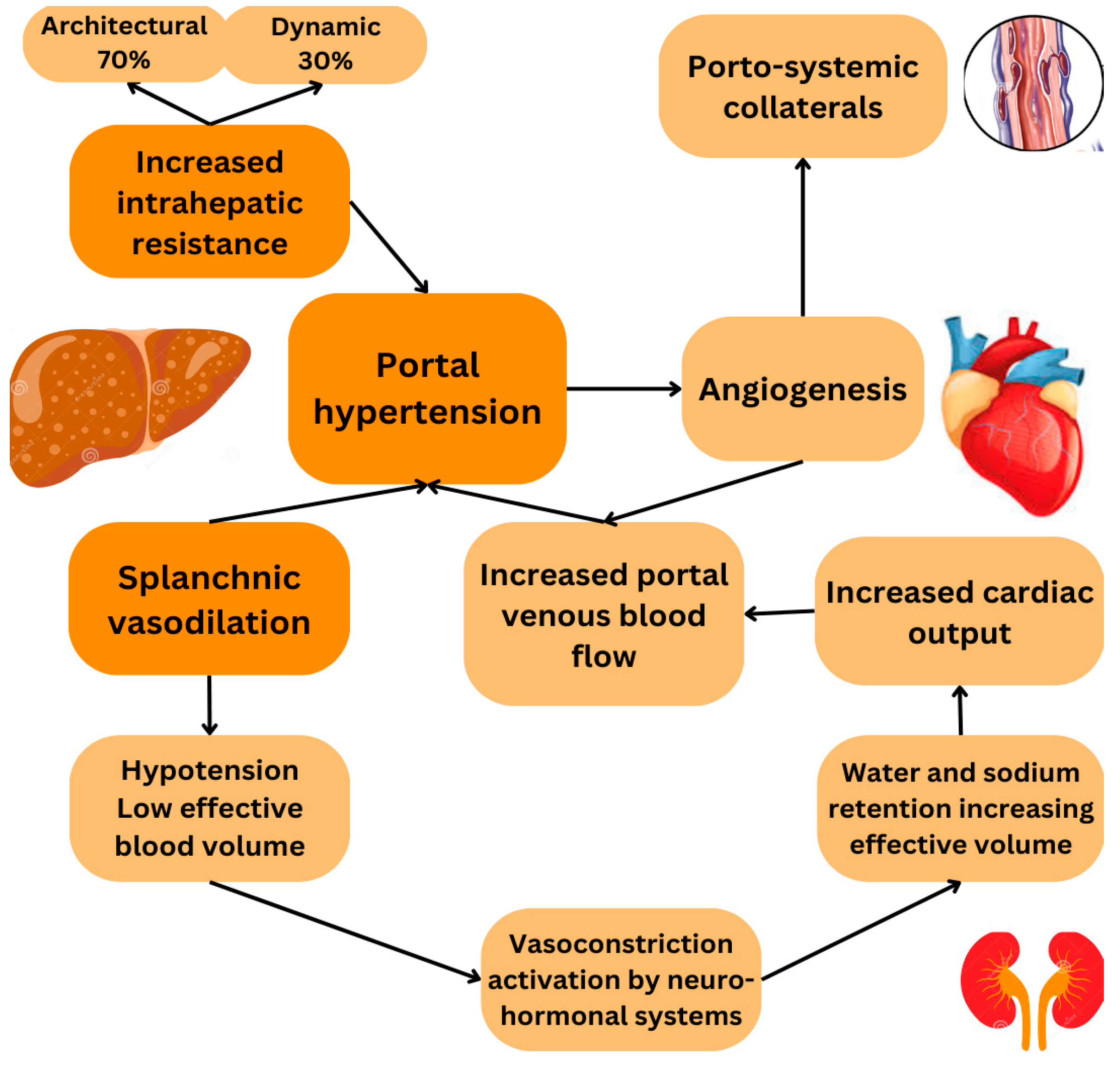
3.1. Portal Hypertension: Pathophysiology and Possible Molecular Targets
3.2. The Mechanisms of Classic Beta-Adrenergic Receptors in Cirrhosis: Beta-1 and Beta-2
- Beta-1 Adrenergic Mechanism
- b.
- Beta-2 Adrenergic Mechanism
3.3. Non-Selective Beta Blockers: Traditional and Carvedilol
3.4. Personalised NSBB Therapy in Cirrhosis: Integrating Biomarkers, Genetics, and Non-Invasive Monitoring
- Biomarkers of Non-Invasive Monitoring of NSBB Efficacy in Cirrhosis
- b.
- Genetic Polymorphism in Beta-Blocker Response
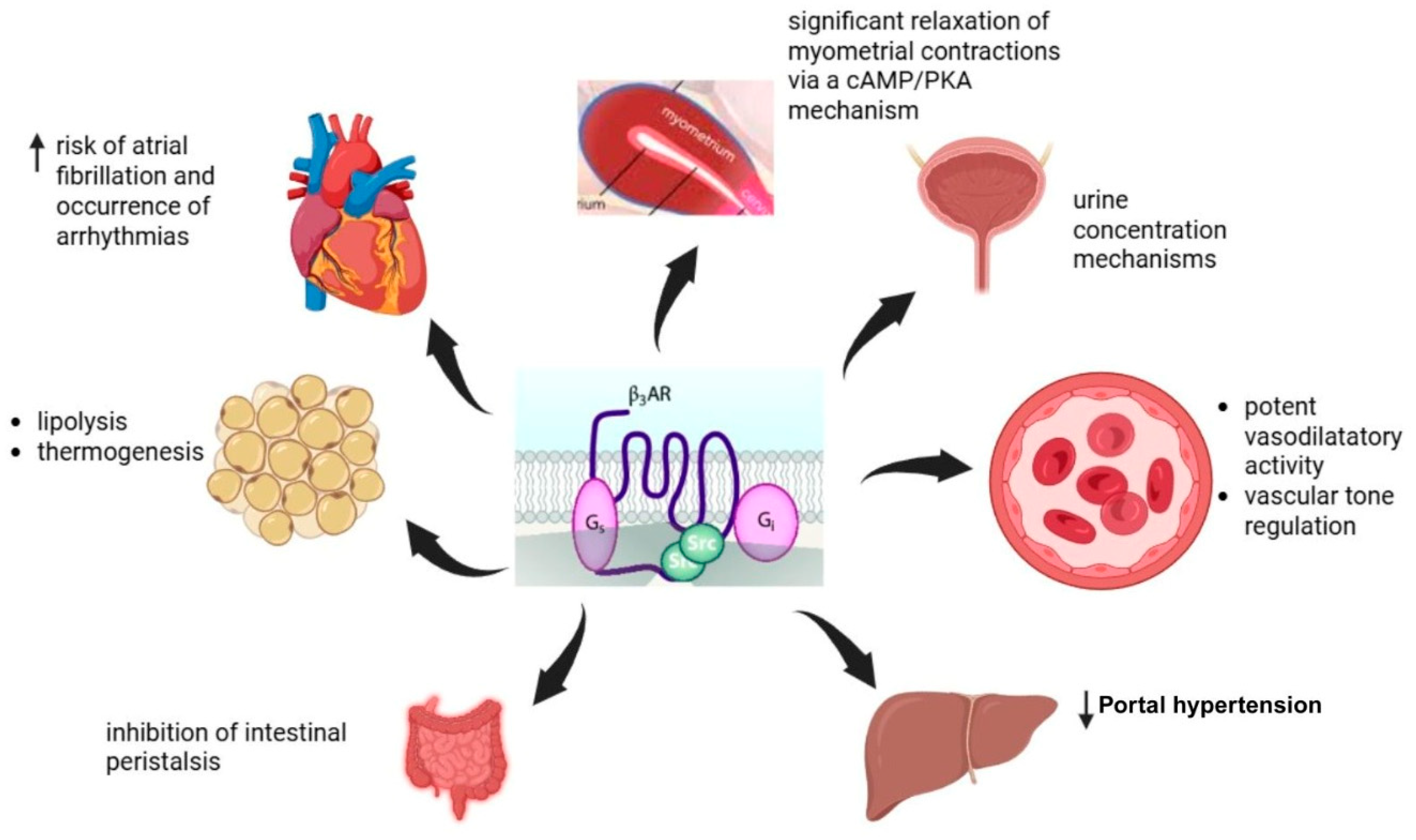
3.5. Beta-3 Adrenergic Mechanism—Emerging Roles in Liver Disease
- Beta 3 effects in fat metabolism
- b.
- Beta 3 in cirrhosis and portal hypertension
4. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ginès, P.; Krag, A.; Abraldes, J.G.; Solà, E.; Fabrellas, N.; Kamath, P.S. Liver cirrhosis. Lancet 2021, 3981, 1359–1376. [Google Scholar] [CrossRef] [PubMed]
- Griffin, C.; Agbim, U.; Ramani, A.; Shankar, N.; Kanwal, F.; Asrani, S.K. Underestimation of Cirrhosis-Related Mortality in the Medicare Eligible Population, 1999–2018. Clin. Gastroenterol. Hepatol. 2023, 21, 223–225.e3. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.; Albillos, A.; Genescà, J.; Garcia-Pagan, J.C.; Calleja, J.L.; Aracil, C.; Bañares, R.; Morillas, R.M.; Poca, M.; Peñas, B.; et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2019, 393, 597–608. [Google Scholar] [CrossRef] [PubMed]
- GBD US Health Disparities Collaborators. The burden of cirrhosis mortality by county, race, and ethnicity in the USA, 2000–2019: A systematic analysis of health disparities. Lancet Public Health 2024, 9, e551–e563. [Google Scholar] [CrossRef] [PubMed]
- Devarbhavi, H.; Asrani, S.K.; Arab, J.P.; Nartey, Y.A.; Pose, E.; Kamath, P.S. Global burden of liver disease: 2023 update. J. Hepatol. 2023, 79, 516–537. [Google Scholar] [CrossRef] [PubMed]
- Rabiee, A.; Ximenes, R.O.; Nikayin, S.; Hickner, A.; Juthani, P.; Rosen, R.H.; Garcia-Tsao, G. Factors associated with health-related quality of life in patients with cirrhosis: A systematic review. Liver Int. 2021, 41, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Medina Pizaño, M.Y.; Loera Arias, M.J.; Montes de Oca Luna, R.; Saucedo Cárdenas, O.; Ventura Juárez, J.; Muñoz Ortega, M.H. Neuroimmunomodulation of Adrenoblockers during Liver Cirrhosis: Modulation of Hepatic Stellate Cell Activity. Int. J. Mol. Sci. 2023, 24, 2689. [Google Scholar] [CrossRef] [PubMed]
- Fei, B.; Zhao, Y.; Wang, J.; Wen, P.; Li, J.; Tanaka, M.; Wang, Z.; Li, S. Leveraging Adrenergic Receptor Blockade for Enhanced Nonalcoholic Fatty Liver Disease Treatment via a Biomimetic Nanoplatform. J. Nanobiotechnol. 2024, 22, 591. [Google Scholar] [CrossRef] [PubMed]
- Sauerbruch, T.; Hennenberg, M.; Trebicka, J.; Schierwagen, R. Beta-blockers in patients with liver cirrhosis: Pragmatism or perfection? Front. Med. 2023, 9, 1100966. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, S.L.; Hanrahan, T.P.; Rockey, D.C.; Majumdar, A.; Hayes, P.C. Review article: Controversies surrounding the use of carvedilol and other beta blockers in the management of portal hypertension and cirrhosis. Aliment. Pharmacol. Ther. 2023, 57, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Labenz, C.; Toenges, G.; Schattenberg, J.M.; Nagel, M.; Huber, Y.; Marquardt, J.U.; Galle, P.R.; Wörns, M.A. Health-related quality of life in patients with compensated and decompensated liver cirrhosis. Eur. J. Intern. Med. 2019, 70, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Gunarathne, L.S.; Rajapaksha, H.; Shackel, N.; Angus, P.W.; Herath, C.B. Cirrhotic portal hypertension: From pathophysiology to novel therapeutics. World J. Gastroenterol. 2020, 26, 6111–6140. [Google Scholar] [CrossRef] [PubMed]
- Frishman, W.H. Beta-Adrenergic Receptor Blockers in Hypertension: Alive and Well. Prog. Cardiovasc. Dis. 2016, 59, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Iwakiri, Y.; Trebicka, J. Portal hypertension in cirrhosis: Pathophysiological mechanisms and therapy. JHEP Rep. 2021, 3, 100316. [Google Scholar] [CrossRef] [PubMed]
- Schrier, R.W.; Arroyo, V.; Bernardi, M.; Epstein, M.; Henriksen, J.H.; Rodés, J. Peripheral arterial vasodilation hypothesis: A proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology 1988, 8, 1151–1157. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Krag, A. Beta-blockers in the era of precision medicine in patients with cirrhosis. J. Hepatol. 2023, 78, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Di Pascoli, M.; Sacerdoti, D.; Pontisso, P.; Angeli, P.; Bolognesi, M. Molecular Mechanisms Leading to Splanchnic Vasodilation in Liver Cirrhosis. J. Vasc. Res. 2017, 54, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Alexander, S.P.; Christopoulos, A.; Davenport, A.P.; Kelly, E.; Mathie, A.; Peters, J.A.; Veale, E.L.; Armstrong, J.F.; Faccenda, E.; Harding, S.D.; et al. The Concise Guide to Pharmacology 2021/22: G protein-coupled receptors. Br. J. Pharmacol. 2021, 178, S27–S156. [Google Scholar] [CrossRef] [PubMed]
- Alhayek, S.; Preuss, C.V. Beta 1 Receptors. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Cromer, M.; Wilcox, C.M.; Shoreibah, M. Beta-blockers and cirrhosis: Striking the right balance. Am. J. Med. Sci. 2024, 367, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Kotani, K.; Kawada, N. Recent Advances in the Pathogenesis and Clinical Evaluation of Portal Hypertension in Chronic Liver Disease. Gut Liver 2024, 18, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Turco, L.; Reiberger, T.; Vitale, G.; La Mura, V. Carvedilol as the new non-selective beta-blocker of choice in patients with cirrhosis and portal hypertension. Liver Int. 2023, 43, 1183–1194. [Google Scholar] [CrossRef] [PubMed]
- Fortea, J.I.; Alvarado-Tapias, E.; Simbrunner, B.; Ezcurra, I.; Hernández-Gea, V.; Aracil, C.; Llop, E.; Puente, A.; Roig, C.; Reiberger, T.; et al. Carvedilol vs. propranolol for the prevention of decompensation and mortality in patients with compensated and decompensated cirrhosis. J. Hepatol. 2024, S0168-8278, 02772–02777. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Lockman, K.A.; Mallawaarachchi, N.; Robertson, M.; Plevris, J.N.; Hayes, P.C. Carvedilol use is associated with improved survival in patients with liver cirrhosis and ascites. J. Hepatol. 2017, 67, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, A.P.; Jeyaraj, R.; Hobolth, L.; Bendtsen, F.; Gluud, L.L.; Morgan, M.Y. Carvedilol versus traditional, non-selective beta-blockers for adults with cirrhosis and gastroesophageal varices. Cochrane Database Syst. Rev. 2018, 10, CD011510. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.G.; Mendoza, Y.P.; Bosch, J. Beta-blockers in cirrhosis: Evidence-based indications and limitations. JHEP Rep. 2019, 1, 100063. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.; Torres, F.; Sarin, S.K.; Shah, H.A.; Tripathi, D.; Brujats, A.; Rodrigues, S.G.; Bhardwaj, A.; Azam, Z.; Hayes, P.C.; et al. Carvedilol-IPD-MA-group and the Baveno Cooperation: An EASL Consortium. Carvedilol reduces the risk of decompensation and mortality in patients with compensated cirrhosis in a competing-risk meta-analysis. J. Hepatol. 2022, 77, 1014–1025. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Rawat, R.; Saraya, A. Carvedilol versus propranolol effect on hepatic venous pressure gradient at 1 month in patients with index variceal bleed: RCT. Hepatol. Int. 2017, 11, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Bañares, R.; Moitinho, E.; Piqueras, B.; Casado, M.; García-Pagán, J.C.; de Diego, A.; Bosch, J. Carvedilol, a new nonselective beta-blocker with intrinsic anti-Alpha1-adrenergic activity, has a greater portal hypotensive effect than propranolol in patients with cirrhosis. Hepatology 1999, 30, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Bañares, R.; Moitinho, E.; Matilla, A.; García-Pagán, J.C.; Lampreave, J.L.; Piera, C.; Abraldes, J.G.; De Diego, A.; Albillos, A.; Bosch, J. Randomized comparison of long-term carvedilol and propranolol administration in the treatment of portal hypertension in cirrhosis. Hepatology 2002, 36, 1367–1373. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, D.; Therapondos, G.; Lui, H.F.; Stanley, A.J.; Hayes, P.C. Haemodynamic effects of acute and chronic administration of low-dose carvedilol, a vasodilating beta-blocker, in patients with cirrhosis and portal hypertension. Aliment. Pharmacol. Ther. 2002, 16, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Reiberger, T.; Ulbrich, G.; Ferlitsch, A.; Payer, B.A.; Schwabl, P.; Pinter, M.; Heinisch, B.B.; Trauner, M.; Kramer, L.; Peck-Radosavljevic, M.; et al. Carvedilol for primary prophylaxis of variceal bleeding in cirrhotic patients with haemodynamic non-response to propranolol. Gut 2013, 62, 1634–1641. [Google Scholar] [CrossRef] [PubMed]
- Sinagra, E.; Perricone, G.; D’Amico, M.; Tine, F.; D’Amico, G. Systematic review with meta-analysis: The haemodynamic effects of carvedilol compared with propranolol for portal hypertension in cirrhosis. Aliment. Pharmacol. Ther. 2014, 39, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Bond, R.A.; Lucero Garcia-Rojas, E.Y.; Hegde, A.; Walker, J.K.L. Therapeutic Potential of Targeting ß-Arrestin. Front. Pharmacol. 2019, 10, 124. [Google Scholar] [CrossRef] [PubMed]
- Lashen, S.A.; Shamseya, M.M.; Madkour, M.A.; Abdel Salam, R.M.; Mostafa, S.S. β-arrestin-2 predicts the clinical response to β-blockers in cirrhotic portal hypertension patients: A prospective study. World J. Hepatol. 2022, 14, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Trebicka, J.; von Heydebrand, M.; Lehmann, J.; Tofteng, F.; Busk, T.; Jensen, H.L.; Rohde, J.; Reiberger, T.; Mortensen, C.; Schierwagen, R.; et al. Assessment of response to beta-blockers by expression of βArr2 and RhoA/ROCK2 in antrum mucosa in cirrhotic patients. J. Hepatol. 2016, 64, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Luttrell, L.M.; Premont, R.T.; Rockey, D.C. β-Arrestin2 is a critical component of the GPCR-eNOS signalosome. Proc. Natl. Acad. Sci. USA 2020, 117, 11483–11492. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.S.; Lin, W.S.; Lin, C.L.; Kao, C.H. Carvedilol use is associated with reduced cancer risk: A nationwide population-based cohort study. Int. J. Cardiol. 2015, 184, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.M.; Liang, S.; Yeung, S.; Oiyemhonlan, E.; Cleveland, K.H.; Parsa, C.; Orlando, R.; Meyskens, F.L., Jr.; Andresen, B.T.; Huang, Y. Topically Applied Carvedilol Attenuates Solar Ultraviolet Radiation Induced Skin Carcinogenesis. Cancer Prev. Res. 2017, 10, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.Y.; Lin, H.C.; Lin, H.L.; Uang, Y.S.; Keller, J.J.; Wang, L.H. Association Between Nonselective Beta-Blocker Use and Hepatocellular Carcinoma in Patients with Chronic Hepatitis B Without Cirrhosis and Decompensation. Front. Pharmacol. 2022, 12, 805318. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.Y.; Chung, C.H.; Chang, W.C.; Lin, C.S.; Lin, H.H.; Dai, M.S.; Ho, C.L.; Chien, W.C. The effect of propranolol on the prognosis of hepatocellular carcinoma: A nationwide population-based study. PLoS ONE 2019, 14, e0216828. [Google Scholar] [CrossRef] [PubMed]
- Reiberger, T.; Mandorfer, M. Beta adrenergic blockade and decompensated cirrhosis. J. Hepatol. 2017, 66, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Santos, U.C.; Souza, M.D.G.C.; Ferreira da Motta Rezende, G. Selection of patients with portal hypertension and cirrhosis who will benefit from beta-blockers: Still a current challenge. J. Hepatol. 2024, 80, e34–e35. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Rojo, M.A.; Pearen, M.A.; Burgess, A.G.; Ikonomopoulou, M.P.; Hoang-Le, D.; Genz, B.; Saggiomo, S.L.; Nawaratna, S.S.K.; Poli, M.; Reissmann, R.; et al. The heavy subunit of ferritin stimulates NLRP3 inflammasomes in hepatic stellate cells through ICAM-1 to drive hepatic inflammation. Sci. Signal 2024, 17, eade4335. [Google Scholar] [CrossRef] [PubMed]
- Almenara, S.; Lozano-Ruiz, B.; Herrera, I.; Gimenez, P.; Miralles, C.; Bellot, P.; Rodriguez, M.; Palazon, J.M.; Tarín, F.; Sarmiento, H.; et al. Immune changes over time and survival in patients with cirrhosis treated with non-selective beta-blockers: A prospective longitudinal study. Biomed. Pharmacother. 2023, 163, 114885. [Google Scholar] [CrossRef] [PubMed]
- Reiberger, T.; Ferlitsch, A.; Payer, B.A.; Mandorfer, M.; Heinisch, B.B.; Hayden, H.; Lammert, F.; Trauner, M.; Peck-Radosavljevic, M.; Vogelsang, H.; et al. Non-selective betablocker therapy decreases intestinal permeability and serum levels of LBP and IL-6 in patients with cirrhosis. J. Hepatol. 2013, 58, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Bui, T.M.; Wiesolek, H.L.; Sumagin, R. ICAM-1: A master regulator of cellular responses in inflammation, injury resolution, and tumorigenesis. J. Leukoc. Biol. 2020, 108, 787–799. [Google Scholar] [CrossRef] [PubMed]
- Hintermann, E.; Christen, U. The Many Roles of Cell Adhesion Molecules in Hepatic Fibrosis. Cells 2019, 8, 1503. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Martin-Mateos, R.; Van der Merwe, S.; Wiest, R.; Jalan, R.; Álvarez-Mon, M. Cirrhosis-associated immune dysfunction. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 112–134. [Google Scholar] [CrossRef] [PubMed]
- Jachs, M.; Hartl, L.; Schaufler, D.; Desbalmes, C.; Simbrunner, B.; Eigenbauer, E.; Bauer, D.J.M.; Paternostro, R.; Schwabl, P.; Scheiner, B.; et al. Amelioration of systemic inflammation in advanced chronic liver disease upon beta-blocker therapy translates into improved clinical outcomes. Gut 2021, 70, 1758–1767. [Google Scholar] [CrossRef] [PubMed]
- Ezhilarasan, D. Endothelin-1 in portal hypertension: The intricate role of hepatic stellate cells. Exp. Biol. Med. 2020, 245, 1504–1512. [Google Scholar] [CrossRef] [PubMed]
- Popa, E.; Avram, R.I.; Popa, A.E.; Coman, A.E. Non-invasive Serological Markers of Hepatic Fibrosis—Mini Review. Arch. Surg. Clin. Res. 2024, 8, 32–38. [Google Scholar]
- Wereszczynka-Siemiatkowska, U.; Swidnicka-Siergiejko, A.; Siemiatkowski, A.; Bondyra, Z.; Wasielica-Berger, J.; Mroczko, B.; Janica, J.; Dabrowski, A. Endothelin 1 and transforming growth factor-β1 correlate with liver function and portal pressure in cirrhotic patients. Cytokine 2015, 76, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Elhence, A. Von Willebrand Factor as a Biomarker for Liver Disease—An Update. J. Clin. Exp. Hepatol. 2023, 13, 1047–1060. [Google Scholar] [CrossRef] [PubMed]
- Pomej, K.; Scheiner, B.; Balcar, L.; Nussbaumer, R.J.; Weinzierl, J.; Paternostro, R.; Simbrunner, B.; Bauer, D.; Pereyra, D.; Starlinger, P.; et al. Clinical significance of substantially elevated von Willebrand factor antigen levels in patients with advanced chronic liver disease. Dig. Liver Dis. 2022, 54, 1376–1384. [Google Scholar] [CrossRef] [PubMed]
- Garcia Garcia de Paredes, A.; Villanueva, C.; Blanco, C.; Genescà, J.; Manicardi, N.; Garcia-Pagan, J.C.; Calleja, J.L.; Aracil, C.; Morillas, R.M.; Poca, M.; et al. Serum miR-181b-5p predicts ascites onset in patients with compensated cirrhosis. JHEP Rep. 2021, 3, 100368. [Google Scholar] [CrossRef] [PubMed]
- Garcia Garcia de Paredes, A.; Manicardi, N.; Tellez, L.; Ibañez, L.; Royo, F.; Bermejo, J.; Blanco, C.; Fondevila, C.; Fernandez Lanza, V.; Garcia-Bermejo, L.; et al. Molecular Profiling of Decompensated Cirrhosis by a Novel MicroRNA Signature. Hepatol. Commun. 2020, 5, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Sanchez, A.; Matilla, A.; Nuñez, O.; Rincon, D.; Lorente, R.; Lo Iacono, O.; Merino, B.; Hernando, A.; Campos, R.; Clemente, G.; et al. Serum level of soluble vascular cell adhesion molecule in patients with hepatocellular carcinoma and its association with severity of liver disease. Ann. Hepatol. 2013, 12, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Pepine, C.J.; Handberg, E.M.; Cooper-DeHoff, R.M.; Marks, R.G.; Kowey, P.; Messerli, F.H.; Mancia, G.; Cangiano, J.L.; Garcia-Barreto, D.; Keltai, M.; et al. A Calcium Antagonist vs a Non–Calcium Antagonist Hypertension Treatment Strategy for Patients with Coronary Artery Disease. The International Verapamil-Trandolapril Study (INVEST): A Randomized Controlled Trial. JAMA 2003, 290, 2805–2816. [Google Scholar] [CrossRef] [PubMed]
- Fasolato, S.; Bonaiuto, E.; Rossetto, M.; Vanzani, P.; Ceccato, F.; Vittadello, F.; Zennaro, L.; Rigo, A.; Mammano, E.; Angeli, P.; et al. Serum Vascular Adhesion Protein-1 and Endothelial Dysfunction in Hepatic Cirrhosis: Searching for New Prognostic Markers. Int. J. Mol. Sci. 2024, 25, 7309. [Google Scholar] [CrossRef] [PubMed]
- El-Shayeb, A.F.; Degheidy, A.A.; El-Mallah, S.; Farid, J.; Abbasy, A.N. Validity of serum resistin level and Il-6 as prognostic biomarkers of decompensated liver cirrhosis in chronic hepatitis C virus patients. Egypt Liver J. 2023, 13, 56. [Google Scholar] [CrossRef]
- Siemiatkowska, U.; Siemiatkowski, A.; Wasielica-Berger, J.; Janica, J.; Mroczko, B.; Dabrowski, A. The imbalance of peripheral interleukin-18 and transforming growth factor-β1 levels in patients with cirrhosis and esophageal varices. Cytokine 2019, 113, 440–445. [Google Scholar]
- Jachs, M.; Hartl, L.; Simbrunner, B.; Bauer, D.; Paternostro, R.; Scheiner, B.; Schwabl, P.; Stättermayer, A.F.; Pinter, M.; Eigenbauer, E.; et al. Decreasing von Willebrand Factor Levels Upon Nonselective Beta Blocker Therapy Indicate a Decreased Risk of Further Decompensation, Acute-on-chronic Liver Failure, and Death. Clin. Gastroenterol. Hepatol. 2022, 20, 1362–1373.e6. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.J.; Mukherjee, S.; Yun, J.W. Loss of ADAMTS15 Promotes Browning in 3T3-L1 White Adipocytes via Activation of β3-adrenergic Receptor. Biotechnol. Bioproc. E 2021, 26, 188–200. [Google Scholar] [CrossRef]
- Kong, D.R.; Wang, J.G.; Sun, B.; Wang, M.Q.; Chen, C.; Yu, F.F.; Xu, J.M. β-2 Adrenergic receptor gene polymorphism and response to propranolol in cirrhosis. World J. Gastroenterol. 2015, 21, 7191–7196. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Duan, X.; Zhang, M.; Li, Z.; He, Q.; Wang, Y.; Miao, C.; Zhong, W.; Zou, X.; Zhuge, Y. Influence of CYP2D6 and β2-adrenergic receptor gene polymorphisms on the hemodynamic response to propranolol in Chinese Han patients with cirrhosis. J. Gastroenterol. Hepatol. 2016, 31, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.D.; Johnson, J.A. Pharmacogenetic factors affecting β-blocker metabolism and response. Expert Opin. Drug Metab. Toxicol. 2020, 16, 953–964. [Google Scholar] [CrossRef] [PubMed]
- Guerra, L.A.; Lteif, C.; Arwood, M.J.; McDonough, C.W.; Dumeny, L.; Desai, A.A.; Cavallari, L.H.; Duarte, J.D. Genetic polymorphisms in ADRB2 and ADRB1 are associated with differential survival in heart failure patients taking β-blockers. Pharmacogenom. J. 2022, 22, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Møller, S.; Danielsen, K.V.; Nabilou, P.; Kimer, N.; Bendtsen, F. Beta-adrenergic blockade in cirrhosis—Harmful or helpful? Expert Rev. Gastroenterol. Hepatol. 2023, 17, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Pasha, A.; Tondo, A.; Favre, C.; Calvani, M. Inside the Biology of the β3-Adrenoceptor. Biomolecules 2024, 14, 159. [Google Scholar] [CrossRef] [PubMed]
- Schena, G.; Caplan, M.J. Everything You Always Wanted to Know about β3-AR * (* But Were Afraid to Ask). Cells 2019, 8, 357. [Google Scholar] [CrossRef] [PubMed]
- Wortham, A.; Khalifa, A.; Rockey, D.C. The natural history of patients with compensated cirrhosis and elevated hepatic venous pressure gradient. Portal Hypertens. Cirrhosis 2022, 1, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Vasina, V.; Giannone, F.; Domenicali, M.; Latorre, R.; Berzigotti, A.; Caraceni, P.; Zoli, M.; De Ponti, F.; Bernardi, M. Portal hypertension and liver cirrhosis in rats: Effect of the β3-adrenoceptor agonist SR58611A. Br. J. Pharmacol. 2012, 167, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Wagg, A.; Staskin, D.; Engel, E.; Herschorn, S.; Kristy, R.M.; Schermer, C.R. Efficacy, safety, and tolerability of mirabegron in patients aged ≥65 yr with overactive bladder wet: A phase IV, double-blind, randomised, placebo-controlled study (PILLAR). Eur. Urol. 2020, 77, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, D.; Plakkot, B.; Tiwari, K.; Ekambaram, S.; Wang, W.; Rudolph, M.; Mohammad, M.A.; Chacko, S.K.; Subramanian, M.; Tarantini, S.; et al. Chronic β3-AR stimulation activates distinct thermogenic mechanisms in brown and white adipose tissue and improves systemic metabolism in aged mice. Aging Cell 2024, 23, e14321. [Google Scholar] [CrossRef] [PubMed]
- Clare, K.; Dillon, J.F.; Brennan, P.N. Reactive Oxygen Species and Oxidative Stress in the Pathogenesis of MAFLD. J. Clin. Transl. Hepatol. 2022, 10, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, C.; Clària, J.; Szabo, G.; Bosch, J.; Bernardi, M. Pathophysiology of decompensated cirrhosis: Portal hypertension, circulatory dysfunction, inflammation, metabolism and mitochondrial dysfunction. J. Hepatol. 2021, 75 (Suppl. S1), S49–S66. [Google Scholar] [CrossRef] [PubMed]
- Sangro, P.; de la Torre Aláez, M.; Sangro, B.; D’Avola, D. Metabolic dysfunction–associated fatty liver disease (MAFLD): An update of the recent advances in pharmacological treatment. J. Physiol. Biochem. 2023, 79, 869–879. [Google Scholar] [CrossRef] [PubMed]
- Elbadr, M.M.; El Badre, H.M. Hepatoprotective and antiobesity effects of mirabegron, a novel β3-adrenoceptor agonist, on carbon tetrachloride-induced hepatotoxicity in obese rats. J. Curr. Med. Res. Pract. 2020, 5, 254–261. [Google Scholar] [CrossRef]
- Wang, Z.; Li, S.; Wang, R.; Guo, L.; Xu, D.; Zhang, T.; Xu, Y.; Wang, W.; Wang, M.; Gan, Z.; et al. The protective effects of the β3 adrenergic receptor agonist BRL37344 against liver steatosis and inflammation in a rat model of high-fat diet-induced nonalcoholic fatty liver disease (NAFLD). Mol. Med. 2020, 26, 54. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Wang, R.; Chai, Y.; Zhang, L.; Chen, R.; Li, R.; Pan, J.; Zhu, J.; Sun, Q.; Liu, C. β3 adrenergic receptor activation alleviated PM2.5-induced hepatic lipid deposition in mice. Sci. Total Environ. 2023, 907, 168167. [Google Scholar] [CrossRef] [PubMed]
- Bassal, T.; Basheer, M.; Boulos, M.; Assy, N. Nonalcoholic Fatty Liver Disease—A Concise Review of Noninvasive Tests and Biomarkers. Metabolites 2022, 12, 1073. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Friedman, S.L.; Shulman, G.I. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell 2021, 184, 2537–2564. [Google Scholar] [CrossRef] [PubMed]
- Vairappan, B. Endothelial dysfunction in cirrhosis: Role of inflammation and oxidative stress. World J. Hepatol. 2015, 7, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Nababan, S.H.H.; Lesmana, C.R.A. Portal Hypertension in Nonalcoholic Fatty Liver Disease: From Pathogenesis to Clinical Practice. J. Clin. Transl. Hepatol. 2022, 10, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Golshiri, K.; Ataei Ataabadi, E.; Portilla Fernandez, E.C.; Jan Danser, A.H.; Roks, A.J.M. The importance of the nitric oxide-cGMP pathway in age-related cardiovascular disease: Focus on phosphodiesterase-1 and soluble guanylate cyclase. Basic Clin. Pharmacol. Toxicol. 2020, 127, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Potocka, N.; Skrzypa, M.; Zadarko-Domaradzka, M.; Barabasz, Z.; Penar-Zadarko, B.; Sakowicz, A.; Zadarko, E.; Zawlik, I. Effects of the Trp64Arg Polymorphism in the ADRB3 Gene on Body Composition, Cardiorespiratory Fitness, and Physical Activity in Healthy Adults. Genes 2023, 14, 1541. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.J.F.; Glastras, S.J.; Tang, O.; Figtree, G.A. Therapeutic Potential for Beta-3 Adrenoreceptor Agonists in Peripheral Arterial Disease and Diabetic Foot Ulcers. Biomedicines 2023, 11, 3187. [Google Scholar] [CrossRef] [PubMed]
- Chapple, C.R.; Cruz, F.; Cardozo, L.; Staskin, D.; Herschorn, S.; Choudhury, N.; Stoelzel, M.; Heesakkers, J.; Siddiqui, E. Safety and Efficacy of Mirabegron: Analysis of a Large Integrated Clinical Trial Database of Patients with Overactive Bladder Receiving Mirabegron, Antimuscarinics, or Placebo. Eur. Urol. 2020, 77, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, A.; Ye, M.; Zhang, C. Examining the safety of mirabegron: An analysis of real-world pharmacovigilance data from the US FDA adverse event reporting system (FAERS) database. Front. Pharmacol. 2024, 15, 1376535. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Type of Study | Number of Patients | Main Findings | Limitations | Reference |
|---|---|---|---|---|
| RCT | Carvedilol-14 Propranolol-14 Placebo-7 | HVPG was lowered more after carvedilol (decreased by 20%) than after propranolol (decreased by 13%) at 1 h HVPG was lowered consistently more with carvedilol (64%) than with propranolol (14%) | Low number of patients included, short-term follow-up, single center design, limited patient heterogeneity, primary focus on surrogate outcomes, not direct clinical endpoints | [29] |
| RCT, prospective | Carvedilol-26 Propranolol-25 | HVPG was lowered more after carvedilol (decreased by 19%) than after propranolol (decreased by 12%) at 1 h HVPG was lowered consistently more with carvedilol (54%) than with propranolol (23%) | Low number of patients included, short-term follow-up, single center design, limited patient heterogeneity, primary focus on surrogate outcomes, not direct clinical endpoints | [30] |
| Prospective, non-randomised | Carvedilol-10 | HVPG was lowered by ~23% with carvedilol after 1 h | Low number of patients included, lack of control group, short-term follow-up, primary focus on surrogate outcomes, not direct clinical endpoints, potential for measurement bias | [31] |
| Prospective, non-randomised | Carvedilol-38 Propranolol-37 EVL-29 | Carvedilol has better lowering of HVPG effects than propranolol + carvedilol has a hemodynamic response in Propranolol non-responders | Lack of randomization, restriction to compensated cirrhotic patients, empirically defined dosing categories, absence of blinding, no formal dose-finding for carvedilol, potential underestimation of side effects, and limited generalizability to routine practice. | [32] |
| Systematic review with metanalyses | 5 RCT-175 patients | Carvedilol lowers portal hypertension more than propranolol, but without an accurate comparison of the adverse effects | Low number of patients and trials included, heterogeneity in study design, poor trial quality, inadequate adverse event reporting | [33] |
| RCT, prospective | Carvedilol-30 patients Propranolol-29 patients | Carvedilol showed a better HVPG response 1 month after variceal bleeding (75%) than propranolol (50%) | High risk of bias (study not double-blinded), short-term follow-up, primary focus on surrogate outcomes, not direct clinical endpoints, small sample size, selection bias | [28] |
| Systematic review of multiple RCTs | 10 RCT-810 patients | Carvedilol is superior to other beta-blockers in lowering HVPG | Low heterogeneity of included studies, small sample sizes, short follow-up periods, high risk of bias, insufficient power | [25] |
| Metanalyses | 4 RCT-352 patients (Carvedilol-181, Control-171) | Survival was improved, and a lowered risk of decompensation was achieved, primarily in the form of ascites, with carvedilol therapy | Partial blinding, endpoint variability, risk of publication/data availability bias, limited applicability to decompensated cirrhosis, small sample sizes in some subgroups, and potential for bias in open-label designs. | [27] |
| Type of Molecule | Main Findings | Type of Study | Clinical Applicability/Limitations | References |
|---|---|---|---|---|
| sVCAM-1 | Serum levels are significantly higher in decompensated cirrhosis (p < 0.01) moderate correlation between the variation in HVPG and sVCAM-1 after treatment with NSBBs (p = 0.03) Elevated levels in decompensated cirrhosis; correlated with Child–Pugh, MELD, and hyperdynamic circulation. Associated with sVAP-1 in early disease stages; currently under evaluation in NSBB treatment response (NCT03720067). | Retrospective and prospective cohort studies; ongoing interventional trial | No standardized cut-off values; not yet validated for clinical use; under investigation in clinical trials | [43,58,59] |
| IL-6, IL-10, IFN-γ | Higher levels of IL-6, IL-10, IFN- γ—more clinical events; NSBBs treatment—significantly better event-free survival, including hepatocellular carcinoma, death, and the need for liver transplantation (HR = 0.36, 95%CI = 0.18–0.71) NSBB therapy modulates immune response and improves survival. IL-6 > 37 pg/mL predicts short-term complications. | Prospective longitudinal and case-control studies | Promising prognostic value, particularly for IL-6; clinical implementation needs further validation | [43,45,59,60] |
| ET-1 | Peripheral ET-1 levels significantly increased after NSBB treatment (from 1.33 fmol/L to 3.0 fmol/L—p = 0.032) Serum ET-1 levels are significantly increased in cirrhotic patients and correlate with HVPG and liver dysfunction. NSBB therapy is associated with increased ET-1 levels in non-responders, suggesting a role in intrahepatic vasoconstriction and therapeutic resistance. A related cytokine imbalance involving TGF-β1 may further influence portal pressure and variceal development. | Prospective observational studies | Potential indicator of hepatic vascular tone; clinical utility remains exploratory and requires validation in interventional studies | [53,61] |
| TGF-β2 | Peripheral levels of TGF-b2 significantly decreased and maintained their low levels, compared to the controls (from 263.17 pg/mL to 180.18 pg/mL, p < 0.001); lower levels of peripheral TGF- β2 in normalised HVPG patients in comparison to the patients without HVPG normalisation (p = 0.033) Peripheral levels of TGF-β2 decrease significantly in patients treated with NSBBs and remain low over time. Lower TGF-β2 is associated with HVPG normalization, suggesting a link to vascular remodeling and response to therapy. | Prospective observational study | potential marker of endothelial and fibrotic modulation under NSBBs; clinical use is exploratory and requires further validation. | [53,62] |
| vWF | Increased levels of vWF were correlated with disease severity (p < 0.001); increased levels of vWF were predictive of decompensation/liver-related mortality (p = 0.031); Elevated vWF levels are significantly associated with advanced liver disease severity, increased risk of hepatic decompensation or liver-related mortality, and correlate with the degree of portal hypertension and reduced transplant-free survival. Decreases in vWF levels after NSBB therapy were linked to better outcomes. | Retrospective analysis of prospectively characterized cohort | Promising non-invasive marker of portal hypertension severity; lacks standardization for routine prognostic use. | [55,63] |
| miR-181b-5p | Levels at 1 year, but not at baseline, for patients who achieved HVPG normalization were higher in patients who developed ascites efficient in predicting decompensation (ascites) AUC = 0.7 (95% CI 0.59–0.78), p < 0.01 Predicts ascites onset in compensated cirrhosis and is associated with decompensation risk (AUC = 0.7). May support early risk stratification. | Prospective studies | Not yet validated for NSBB response monitoring. Prognostic role under investigation. | [56,57,64] |
| β1 Blockers | β2 Blockers | β3 Agonists | |
|---|---|---|---|
| Primary site of pharmacological action | Myocardium | Splanchnic vasculature | Endothelial cells, liver, adipose tissue |
| Mechanism of action and receptor specificity | Decrease heart rate and cardiac output → ↓ portal inflow [20,21,22] | Induce splanchnic vasoconstriction → ↓ portal venous flow [22,23,72] | Stimulate NO production and vasodilation via endothelial β3-AR activation [73,74,75,76] |
| Hemodynamic effect on (portal circulation) | Reduce portal pressure via decreased cardiac output [23,28] | Reduce portal inflow via vasoconstriction of splanchnic circulation [21,22,23] | Lower intrahepatic vascular resistance and portal pressure [73,76] |
| Effect on systemic arterial pressure | Moderate reduction; hypotension risk at high doses [22,30] | Mild systemic effect; usually used with β1 blockers [23,72] | Minimal systemic impact: preserves mean arterial pressure [73,76,77] |
| Common side effects | Bradycardia, hypotension, fatigue [7,22,23]; β1-selective blockers rarely cause bronchospasm, but caution is advised in asthma or COPD, especially at high doses. | Bronchospasm, systemic hypotension; caution in cirrhosis and respiratory disease [23] | Favorable tolerability profile; minimal cardiovascular effects; safety under ongoing investigation [73,78,79,80] |
| Therapeutic limitations due to safety profile | Heterogeneous response; adverse events; genetic polymorphisms (β-AR) may affect efficacy [10,21,25] | Not used as monotherapy due to limited tolerability [21] | Not currently approved for portal hypertension; additional clinical evidence is required [73,74,75] |
| Clinical evidence and use in cirrhosis | Standard of care in cirrhosis (e.g., propranolol, carvedilol); proven efficacy [10,23,28,29,30] | Used as component of NSBBs; enhances β1 effect; no role alone [23,72] | Preclinical and early clinical studies indicate potential efficacy; not yet integrated into standard practice [64,65,67,70,73] |
| Pleiotropic effects and potential therapeutic benefits | Reduces risk of variceal bleeding, decompensation; potential antifibrotic effect [10,29] | Enhances β1 blockade in NSBBs; synergistic in reducing portal pressure [23] | Antifibrotic, anti-inflammatory, improves metabolic profile; induces NO-mediated vasodilation [73,74,75,76,77,78,79,80] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avram, R.-I.; Minea, H.O.; Huiban, L.; Damian, I.-R.; Muset, M.-C.; Juncu, S.; Muzica, C.M.; Zenovia, S.; Singeap, A.M.; Girleanu, I.; et al. Advancements in Beta-Adrenergic Therapy and Novel Personalised Approach for Portal Hypertension: A Narrative Review. Life 2025, 15, 1173. https://doi.org/10.3390/life15081173
Avram R-I, Minea HO, Huiban L, Damian I-R, Muset M-C, Juncu S, Muzica CM, Zenovia S, Singeap AM, Girleanu I, et al. Advancements in Beta-Adrenergic Therapy and Novel Personalised Approach for Portal Hypertension: A Narrative Review. Life. 2025; 15(8):1173. https://doi.org/10.3390/life15081173
Chicago/Turabian StyleAvram, Raluca-Ioana, Horia Octav Minea, Laura Huiban, Ioana-Roxana Damian, Mihaela-Cornelia Muset, Simona Juncu, Cristina Maria Muzica, Sebastian Zenovia, Ana Maria Singeap, Irina Girleanu, and et al. 2025. "Advancements in Beta-Adrenergic Therapy and Novel Personalised Approach for Portal Hypertension: A Narrative Review" Life 15, no. 8: 1173. https://doi.org/10.3390/life15081173
APA StyleAvram, R.-I., Minea, H. O., Huiban, L., Damian, I.-R., Muset, M.-C., Juncu, S., Muzica, C. M., Zenovia, S., Singeap, A. M., Girleanu, I., Stanciu, C., & Trifan, A. (2025). Advancements in Beta-Adrenergic Therapy and Novel Personalised Approach for Portal Hypertension: A Narrative Review. Life, 15(8), 1173. https://doi.org/10.3390/life15081173