
Outcomes of Traumatic Liver Injuries at a Level-One Tertiary Trauma Center in Saudi Arabia: A 10-Year Experience
 , , , ,
, , , , 
Abstract
1. Introduction
2. Methodology
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://stats.gov.sa/ar/ (accessed on 24 April 2025).
- Kozar, R.A.; Moore, F.A.; Moore, E.E.; West, M.; Cocanour, C.S.; Davis, J.; Biffl, W.L.; McIntyre, R.C. Western Trauma Association Critical Decisions in Trauma: Nonoperative Management of Adult Blunt Hepatic Trauma. J. Trauma 2009, 67, 1144–1149. [Google Scholar] [CrossRef] [PubMed]
- Stassen, N.A.; Bhullar, I.; Cheng, J.D.; Crandall, M.; Friese, R.; Guillamondegui, O.; Jawa, R.; Maung, A.; Rohs, T.J., Jr.; Sangosanya, A.; et al. Nonoperative Management of Blunt Hepatic Injury: An Eastern Association for the Surgery of Trauma Practice Management Guideline. J. Trauma Acute Care Surg. 2012, 73 (Suppl. 4), S288–S293. [Google Scholar] [CrossRef] [PubMed]
- Alferdaus, A.M.; Shaher, A. Current Trauma Care System in Saudi Arabia: Literature Review and a Proposed Action Plan. Saudi J. Health Syst. Res. 2021, 1, 123–133. [Google Scholar] [CrossRef]
- Haddad, S.H.; Yousef, Z.M.; Al-Azzam, S.S.; AlDawood, A.S.; Al-Zahrani, A.A.; AlZamel, H.A.; Tamim, H.M.; Deeb, A.M.; Arabi, Y.M. Profile, outcome and predictors of mortality of abdomino-pelvic trauma patients in a tertiary intensive care unit in Saudi Arabia. Injury 2015, 46, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Coccolini, F.; Coimbra, R.; Ordonez, C.; Kluger, Y.; Vega, F.; Moore, E.E.; Biffl, W.; Peitzman, A.; Horer, T.; Abu-Zidan, F.M.; et al. Liver trauma: WSES 2020 guidelines. World J. Emerg. Surg. 2020, 15, 24. [Google Scholar] [CrossRef] [PubMed]
- Bonny, P.; Bogaert, C.; Abreu de Carvalho, L.F.; Gryspeerdt, F.; Eker, H.; Hermie, L.; Berrevoet, F. Evolution in liver trauma management: A single centre experience. Acta Chir. Belg. 2024, 124, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Boese, C.K.; Hackl, M.; Müller, L.P.; Ruchholtz, S.; Frink, M.; Lechler, P. Nonoperative management of blunt hepatic trauma: A systematic review. J. Trauma Acute Care Surg. 2015, 79, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Lada, N.E.; Gupta, A.; Anderson, S.W.; Dinh, D.C.; Campbell, J.M.; Maggi, A.; Gandhi, J.; Qureshi, M.M.; Wing, H.; Schulze, R.; et al. Liver trauma: Hepatic vascular injury on computed tomography as a predictor of patient outcome. Eur. Radiol. 2020, 31, 3375–3382. [Google Scholar] [CrossRef] [PubMed]
- Küçükaslan, H.; Tayar, S.; Oğuz, Ş.; Topaloglu, S.; Saatci, S.G.; Şenel, A.C.; Calik, A. The role of liver resection in the management of severe blunt liver trauma. Turk. J. Trauma Emerg. Surg. 2022, 29, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Corvino, F.; Giurazza, F.; Marra, P.; Ierardi, A.M.; Corvino, A.; Basile, A.; Galia, M.; Inzerillo, A.; Niola, R. Damage Control Interventional Radiology in Liver Trauma: A Comprehensive Review. J. Pers. Med. 2024, 14, 365. [Google Scholar] [CrossRef] [PubMed]
- Gilyard, S.; Shinn, K.; Nezami, N.; Findeiss, L.K.; Dariushnia, S.; Grant, A.A.; Hawkins, C.M.; Peters, G.L.; Majdalany, B.S.; Newsome, J.; et al. Contemporary Management of Hepatic Trauma: What IRs Need to Know. Semin. Interv. Radiol. 2020, 37, 035–43. [Google Scholar] [CrossRef] [PubMed]
- Beltzer, C.; Imach, S.; Wafaisade, A.; Lefering, R.; Kölbel, B.; TraumaRegister, D.G.U. Use of angioembolization, treatment modalities and mortality in association with blunt liver trauma in Germany—A data analysis of the TraumaRegister DGU®. Langenbeck’s Arch. Surg. 2023, 409, 6. [Google Scholar] [CrossRef] [PubMed]
- Achatz, G.; Schwabe, K.; Brill, S.; Zischek, C.; Schmidt, R.; Friemert, B.; Beltzer, C. Correction to: Diagnostic options for blunt abdominal trauma. Eur. J. Trauma Emerg. Surg. 2020, 48, 3591. [Google Scholar] [CrossRef] [PubMed]
- Brillantino, A.; Iacobellis, F.; Festa, P.; Mottola, A.; Acampora, C.; Corvino, F.; Del Giudice, S.; Lanza, M.; Armellino, M.; Niola, R.; et al. Non-Operative Management of Blunt Liver Trauma: Safety, Efficacy and Complications of a Standardized Treatment Protocol. Bull. Emerg. Trauma 2019, 7, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Abo-Elhoda, M.F.; Attia, S.M.; Ahmed, M.E.; Abdeldaiem, K.A.E. Solid organs injuries in blunt abdominal trauma patients. Egypt. J. Hosp. Med. 2021, 83, 1477–1483. [Google Scholar] [CrossRef]
- Albabtain, I.; Alfehaid, O.; Alghunaim, M.; Mamoon, A.; Alshaibi, S.; Albaqami, M.; Aljesh, S. Epidemiology of adult trauma at a tertiary hospital in Riyadh, Saudi Arabia. Int. J. Med. Res. Health Sci. 2019, 8, 101–107. [Google Scholar]
- Braschi, C.; Keeley, J.A.; Balan, N.; Perez, L.C.; Neville, A. Outcomes of Highest Grade (IV and V) Liver Injuries in Blunt and Penetrating Trauma. Am. Surg. 2022, 88, 2551–2555. [Google Scholar] [CrossRef] [PubMed]
- Keizer, A.A.; Arkenbosch, J.H.C.; Kong, V.Y.; Hoencamp, R.; Bruce, J.L.; Smith, M.T.D.; Clarke, D.L. Blunt and Penetrating Liver Trauma have Similar Outcomes in the Modern Era. Scand. J. Surg. 2021, 110, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Javali, R.H.; Krishnamoorthy; Patil, A.; Srinivasarangan, M.; Suraj; Sriharsha. Comparison of injury severity score, new injury severity score, revised trauma score and trauma and injury severity score for mortality prediction in elderly trauma patients. Indian J. Crit. Care Med. 2019, 23, 73–77. [Google Scholar] [CrossRef] [PubMed]
- She, W.H.; Cheung, T.T.; Dai, W.C.; Tsang, S.H.; Chan, A.C.; Tong, D.K.; Leung, G.K.; Lo, C.M. Outcome analysis of management of liver trauma: A 10-year experience at a trauma center. World J. Hepatol. 2016, 8, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Adelin, T.B.; De Tovè Kofi-Mensa, S.; Frederic, T.N.C.; Wilfred, G.E.; Marie, N.D.G.; Alexandre, A.S. Contribution of EFAST ultrasound in the management of chest and abdomen’s blunt trauma in the city of Parakou, Benin. Open J. Anesthesiol. 2020, 10, 388–407. [Google Scholar] [CrossRef]
- Stengel, D.; Bauwens, K.; Rademacher, G.; Mutze, S.; Ekkernkamp, A. Association between Compliance with Methodological Standards of Diagnostic Research and Reported Test Accuracy: Meta-Analysis of Focused Assessment of US for Trauma. Radiology 2005, 236, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Waheed, K.B.; Baig, A.A.; Raza, A.; Hassan, M.Z.U.; Khattab, M.A.; Raza, U. Diagnostic accuracy of Focused Assessment with Sonography for Trauma for blunt abdominal trauma in the Eastern Region of Saudi Arabia. Saudi Med. J. 2018, 39, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Basnet, S.; Shrestha, S.K.; Pradhan, A.; Shrestha, R.; Shrestha, A.P.; Sharma, G.; Bade, S.; Giri, L. Diagnostic performance of the extended focused assessment with sonography for trauma (EFAST) patients in a tertiary care hospital of Nepal. Trauma Surg. Acute Care Open 2020, 5, e000438. [Google Scholar] [CrossRef] [PubMed]
- Netherton, S.; Milenkovic, V.; Taylor, M.; Davis, P.J. Diagnostic accuracy of eFAST in the trauma patient: A systematic review and meta-analysis. CJEM 2019, 21, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.L.H.; Kim, J.; Dobson, B.; Campbell, D.; Wullschleger, M. Time to computed tomography: Does this affect trauma patient outcomes? A retrospective analysis at an Australian major trauma centre. ANZ J. Surg. 2019, 89, 1475–1479. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Johnson, R.; Kashef, E.; Khan, M.; Dick, E. How to deliver an effective primary survey report for the trauma CT: A radiological and surgical perspective. Trauma 2021, 24, 99–108. [Google Scholar] [CrossRef]
- Jin, P.F.K.; Van Geene, A.; Linnau, K.; Jurkovich, G.; Ponsen, K.; Goslings, J. Time factors associated with CT scan usage in trauma patients. Eur. J. Radiol. 2008, 72, 134–138. [Google Scholar] [CrossRef]
- Hilbert, P.; Nieden, K.Z.; Hofmann, G.; Hoeller, I.; Koch, R.; Stuttmann, R. New aspects in the emergency room management of critically injured patients: A multi-slice CT-oriented care algorithm. Injury 2007, 38, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Graham, C.A.; Lam, J.M.; Yeung, J.H.; Ahuja, A.; Rainer, T.H. Impact on trauma patient management of installing a computed tomography scanner in the emergency department. Injury 2009, 40, 873–875. [Google Scholar] [CrossRef] [PubMed]
- Harthi, N.; Goodacre, S.; Sampson, F.C. The current status of trauma care for older adults in Saudi Arabia. Front. Med. 2024, 11, 1505913. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, S.; Mok, D.; Leenen, L. Development of the Saudi Arabian trauma system. J. Med. Life 2022, 15, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Isgrò, S.; Giani, M.; Antolini, L.; Giudici, R.; Valsecchi, M.G.; Bellani, G.; Chiara, O.; Bassi, G.; Latronico, N.; Cabrini, L.; et al. Identifying Trauma Patients in Need for Emergency Surgery in the Prehospital Setting: The Prehospital Prediction of In-Hospital Emergency Treatment (PROPHET) Study. J. Clin. Med. 2023, 12, 6660. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, J.; Clark, G.; Delaney, S.; Grushka, J.; Knopp-Sihota, J.A. Timing of Trauma Team Involvement and the Impact on the Length of Stay and Time to Definitive Care in the Emergency Department: A Retrospective Administrative Data and Chart Review. Can. J. Emerg. Nurs. 2024, 47, 30–37. [Google Scholar] [CrossRef]
- Georgiou, A.; Lockey, D.J. The performance and assessment of hospital trauma teams. Scand. J. Trauma Resusc. Emerg. Med. 2010, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Major Adult Trauma Radiology Guidance. 2024. Available online: https://www.rcr.ac.uk/our-services/all-our-publications/clinical-radiology-publications/major-adult-trauma-radiology-guidance/ (accessed on 24 April 2025).
- Klompas, M.; Branson, R.; Cawcutt, K.; Crist, M.; Eichenwald, E.C.; Greene, L.R.; Lee, G.; Maragakis, L.L.; Powell, K.; Priebe, G.P.; et al. Strategies to prevent ventilator-associated pneumonia, ventilator-associated events, and nonventilator hospital-acquired pneumonia in acute-care hospitals: 2022 Update. Infect. Control Hosp. Epidemiol. 2022, 43, 687–713. [Google Scholar] [CrossRef] [PubMed]
- Arumugam, S.K.; Mudali, I.; Strandvik, G.; El-Menyar, A.; Al-Hassani, A.; Al-Thani, H. Risk factors for ventilator-associated pneumonia in trauma patients: A descriptive analysis. World J. Emerg. Med. 2018, 9, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Ladhani, H.A.; Tseng, E.S.; Claridge, J.A.; Towe, C.W.; Ho, V.P. Catheter-Associated Urinary Tract Infections among Trauma Patients: Poor Quality of Care or Marker of Effective Rescue? Surg. Infect. 2020, 21, 752–759. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Nationality, n (%) | Non-Saudi, 36 (32.4%), vs. Saudi, 75 (67.6%) |
| Gender, n (%) | Male, 87 (78.4%), vs. Female, 24 (21.6%) |
| Age median (±IQR) | 30 ± 14 years |
| Admission diagnosis, n (%) | MVAs, 84 (75.7%) |
| Pedestrian vs. Car, 11 (9.9%) | |
| Fall, 12 (10.8%) | |
| Motorcycle crash, 3 (2.7%) | |
| Stab wound, 1 (0.9%) | |
| BMI, n (±SD) | 27.4 ± 6 kg/m2 |
| Temperature, n (±SD) | 36.6 ± 0.5 °C |
| HR, n (±SD) | 105.3 ± 24.4 bpm |
| RR, n (±SD) | 21.8 ± 5.8 breaths per minute |
| SBP, n (±SD) | 114.7 ± 28.7 mmHg |
| DBP, n (±SD) | 70 ± 18.7 mmHg |
| SpO2%, n (±SD) | 96.7 ± 6.5% |
| Shock index, n (±SD) | 1.1 ± 0.4 |
| ISS median (±IQR) | 27 ± 14 |
| GCS at arrival, mean (±SD) | 11.9 ± 4.1 |
| Loss of consciousness, n (%) | Yes, 34 (30.6%) |
| e-FAST, n (%) * | Positive, 38 (34.2%) |
| Morison pouch, n (%) * | Positive, 28 (25.2%) |
| Peri Splenic recess, n (%) * | Positive, 7 (6.3%) |
| Lung, n (%) * | Positive, 3 (2.7%) |
| Subxiphoid window, n (%) * | Negative, 104 (93.7%) |
| Douglas pouch, n (%) * | Positive, 7 (6.3%) |
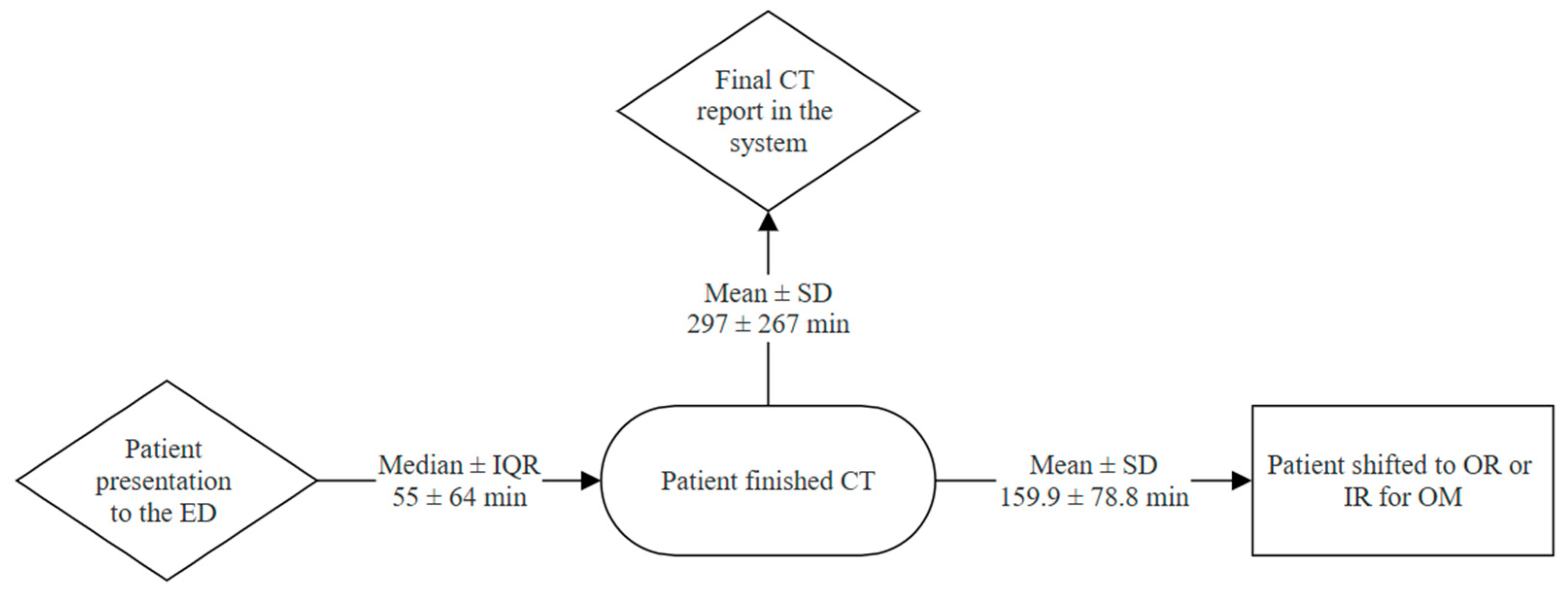
| Time to CT median (±IQR) | 55 ± 64 min |
| Time to CT report median (±IQR) | 297 ± 267 min |
| Time to OR/IR, mean (±SD) | 159.9 ± 78.8 min |
| Intubation in ED, n (%) | Yes, 42 (40%) |
| Monitored unit admission before intervention, n (%) | Yes, 47 (42.3%) |
| Monitored unit admission after intervention, n (%) | Yes, 44 (39.6%) |
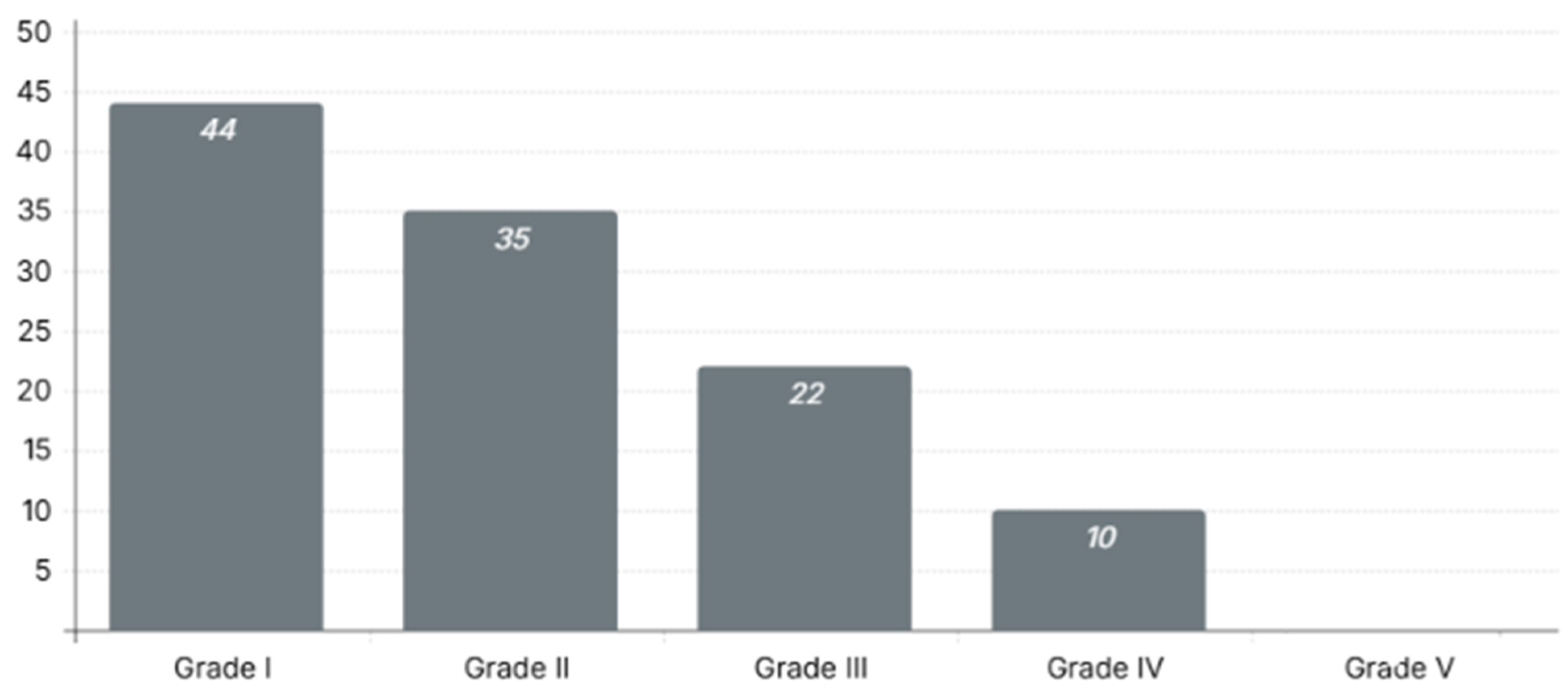
| Liver injury grade, n (%) | Grade I, 44 (39.6%) |
| Grade II, 35 (31.5%) | |
| Grade III, 22 (19.8%) | |
| Grade IV, 10 (9%) | |
| Grade V, 0 (0%) | |
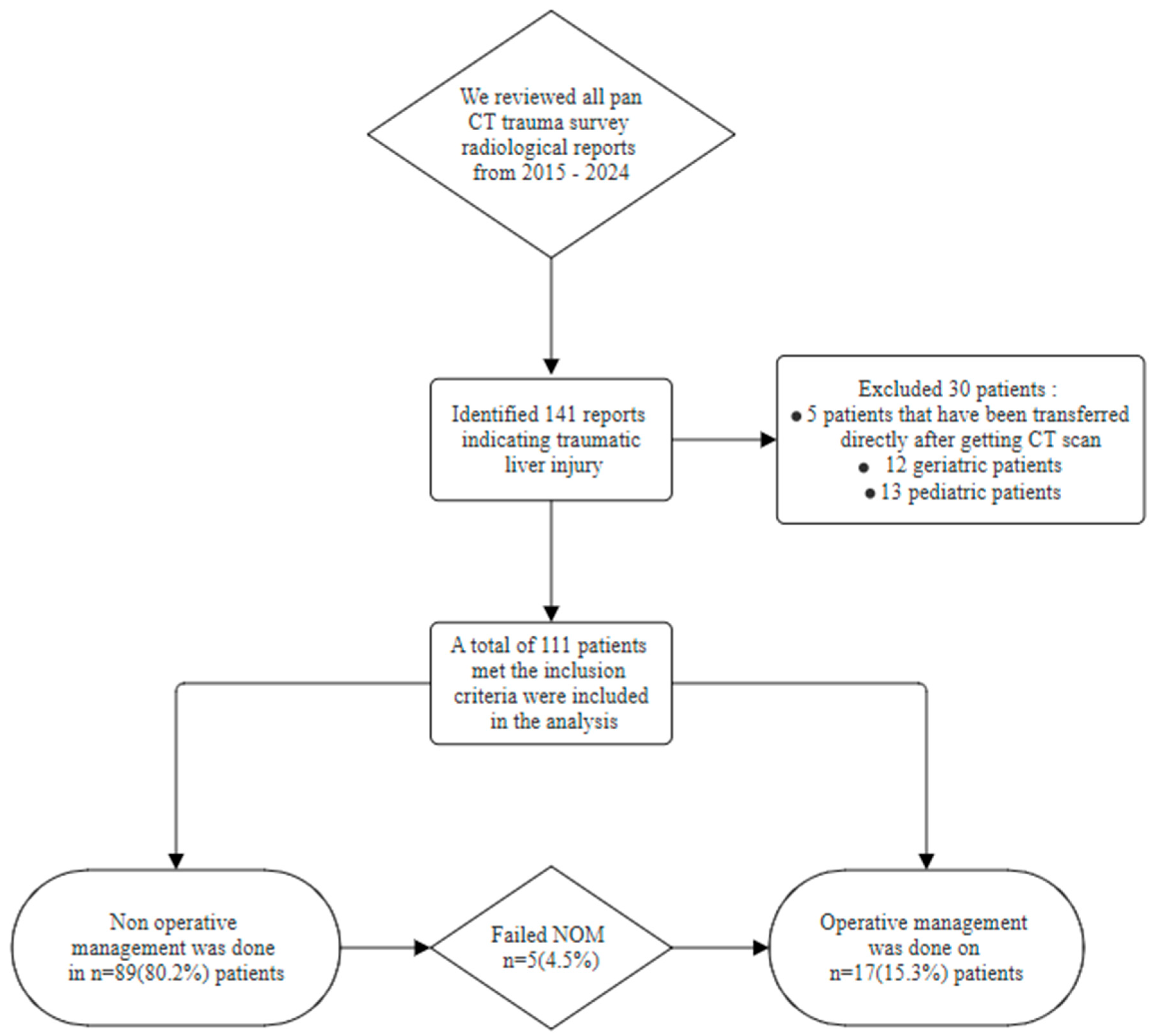
| Management, n (%) | NOM, 89 (80.2%) |
| OM, 17 (15.3%) | |
| Failure of NOM, 5 (4.5%) |
| Hospital LOS median (±IQR) | 13 ± 15.5 days |
| Monitored unit LOS median (±IQR) | 3 ± 10 days |
| Disposition, n (%) | Home, 96 (86.5%) |
| Rehabilitation, 6 (5.4%) | |
| Mortem, 9 (8.1%) | |
| Complications, n (%) | Total complications, 36 (32.4%) |
| VAP, 22 (19.8%) | |
| SSI, 7 (6.3%) | |
| CAUTI, 8 (7.2%) | |
| Sepsis, 7 (6.3%) | |
| Pneumothorax, 3 (2.7%) | |
| Pleural effusion, 2 (1.8%) | |
| Bleeding, 6 (5.4%) | |
| Other, 12 (10.8%) | |
| Total mortality, n (%) | 9 (8.1%) |
| Mortality in 30 days, n (%) | 7 (6.3%) |
| ED visit within 30 days, n (%) | 13 (11.7%) |
| Readmission within 30 days, n (%) | 10 (9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlShahwan, N.; Aldeligan, S.H.; Althunayan, S.T.; Alkodari, A.; Bin Manee, M.; Albassam, F.A.; Aloraini, A.; Alburakan, A.; Mashbari, H.; AlKanhal, A.; et al. Outcomes of Traumatic Liver Injuries at a Level-One Tertiary Trauma Center in Saudi Arabia: A 10-Year Experience. Life 2025, 15, 1138. https://doi.org/10.3390/life15071138
AlShahwan N, Aldeligan SH, Althunayan ST, Alkodari A, Bin Manee M, Albassam FA, Aloraini A, Alburakan A, Mashbari H, AlKanhal A, et al. Outcomes of Traumatic Liver Injuries at a Level-One Tertiary Trauma Center in Saudi Arabia: A 10-Year Experience. Life. 2025; 15(7):1138. https://doi.org/10.3390/life15071138
Chicago/Turabian StyleAlShahwan, Nawaf, Saleh Husam Aldeligan, Salman T. Althunayan, Abdullah Alkodari, Mohammed Bin Manee, Faris Abdulaziz Albassam, Abdullah Aloraini, Ahmed Alburakan, Hassan Mashbari, Abdulaziz AlKanhal, and et al. 2025. "Outcomes of Traumatic Liver Injuries at a Level-One Tertiary Trauma Center in Saudi Arabia: A 10-Year Experience" Life 15, no. 7: 1138. https://doi.org/10.3390/life15071138
APA StyleAlShahwan, N., Aldeligan, S. H., Althunayan, S. T., Alkodari, A., Bin Manee, M., Albassam, F. A., Aloraini, A., Alburakan, A., Mashbari, H., AlKanhal, A., & Nouh, T. (2025). Outcomes of Traumatic Liver Injuries at a Level-One Tertiary Trauma Center in Saudi Arabia: A 10-Year Experience. Life, 15(7), 1138. https://doi.org/10.3390/life15071138