
Acute Kidney Injury in Patients After Cardiac Arrest: Effects of Targeted Temperature Management

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection Criteria
- A time interval between ROSC and the initiation of cooling exceeding 6 h.
- An initial body temperature <30 °C after ROSC.
- Septic shock, known coagulopathy, or active bleeding.
- Major trauma, recent major surgery (<72 h), or severe burns.
2.3. Clinical Management
- Sedation: Propofol (2 mg/kg bolus—if feasible and safe—then 0.5–3 mg/kg/h infusion) or midazolam (0.03–0.04 mg/kg bolus, then 0.2 mg/kg/h infusion).
- Analgesia: Continuous infusion of remifentanil (0.02–0.2 mcg/kg/min) or fentanyl (1–2 mcg/kg/h).
- Paralysis: Continuous infusion of cisatracurium (2 mcg/kg/min).
- Cooling phase to 33 °C.
- Maintenance phase at 33 °C for 24 h.
- Rewarming phase to 36 °C at 0.25–0.5 °C/h.
- Normothermia phase at 36 °C for 48 h.
2.4. Sample Handling and Data Collection
- Stage 1: An increase in sCr of ≥0.3 mg/dL within 48 h or 1.5–1.9 times the baseline value.
- Stage 2: An increase in sCr of 2.0–2.9 times the baseline value.
- Stage 3: An increase in sCr to ≥3.0 times the baseline value, sCr ≥ 4.0 mg/dL, or the initiation of renal replacement therapy.
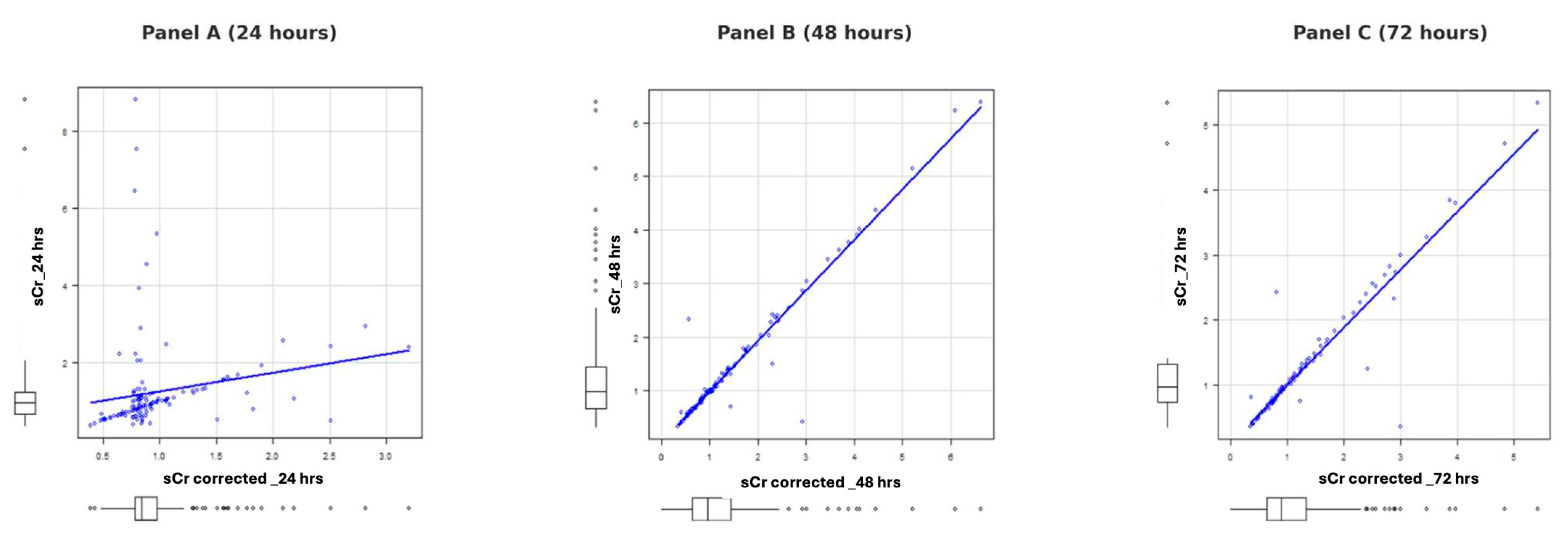
2.5. Fluid Balance-Corrected Serum Creatinine
2.6. Outcomes
2.7. Statistical Analysis
3. Results
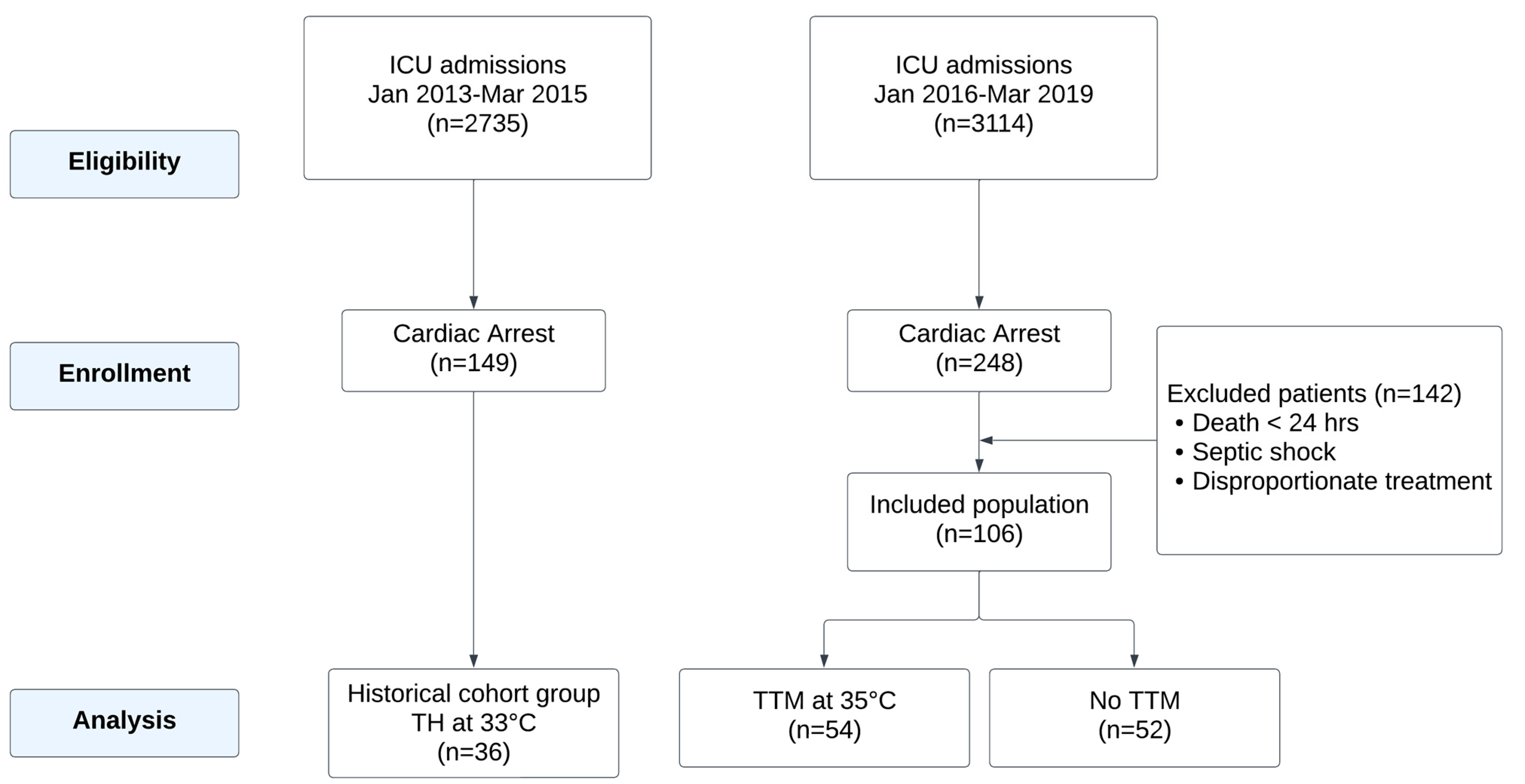
3.1. Study Population
- Historical Control Group (January 2013–March 2015): Patients treated with TH at 33 °C, in line with the guidelines effective during this period.
- Study Group (January 2016–May 2019): Patients eligible for temperature control were treated with TTM at 35 °C following revised ROSC management guidelines.
3.2. Demographic Data, CPR Quality, and Comorbidities
3.3. Renal and Hemodynamic Outcomes
3.4. ICU and Ventilation Outcomes
3.5. Development of AKI and Target Temperature Maintenance Times
4. Discussion
4.1. Major Findings
4.2. Role of Hypothermia in Renal Protection
4.3. Impact of Cold Diuresis and Rewarming on Renal Function
4.4. Biomarkers in AKI Risk Stratification
4.5. Acute Kidney Injury After Cardiac Arrest: Integration of Study Findings, Biomarkers, and Literature Comparison
4.6. Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AHA | American Heart Association |
| AKI | Acute Kidney Injury |
| CA | cardiac arrest |
| CKD | chronic kidney disease |
| COPD | Chronic Obstructive Pulmonary Disease |
| CRRT | Continuous Renal Replacement Therapy |
| ICU | Intensive Care Unit |
| ILCOR | International Liaison Committee on Resuscitation |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| MAP | Mean Arterial Pressure |
| MDRD | Modification of Diet in Renal Disease |
| No TTM | No Targeted Temperature Management |
| ROSC | Return of Spontaneous Circulation |
| sCr | serum creatinine |
| SOFA | Sequential Organ Failure Assessment |
| TTM | Targeted Temperature Management |
| TH | therapeutic hypothermia |
| TIMP-2 | Tissue Inhibitor of Metalloproteinases 2 |
| IGFBP7 | Insulin-like Growth Factor-Binding Protein 7 |
| VIS | Vasoactive Inotropic Score |
References
- Zabel, K.M.; Quazi, M.A.; Leyba, K.; Millhuff, A.C.; Madi, M.; Madrid, W.H.; Goyal, A.; Bilal, M.I.; Sohail, A.H.; Sagheer, S.; et al. Cardiac Arrest Mortality and Disposition Patterns in United States Emergency Departments. J. Clin. Med. 2024, 13, 5585. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.W.; Holmberg, M.J.; Berg, K.M.; Donnino, M.W.; Granfeldt, A. In-Hospital Cardiac Arrest: A Review. JAMA 2019, 321, 1200. [Google Scholar] [CrossRef] [PubMed]
- Gräsner, J.-T.; Herlitz, J.; Tjelmeland, I.B.M.; Wnent, J.; Masterson, S.; Lilja, G.; Bein, B.; Böttiger, B.W.; Rosell-Ortiz, F.; Nolan, J.P.; et al. European Resuscitation Council Guidelines 2021: Epidemiology of Cardiac Arrest in Europe. Resuscitation 2021, 161, 61–79. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.S.; McNally, B.; Tang, F.; Kellermann, A. Recent Trends in Survival from Out-of-Hospital Cardiac Arrest in the United States. Circulation 2014, 130, 1876–1882. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, C.A.; Coppler, P.J.; Skolnik, A.B. The Immunology of the Post-Cardiac Arrest Syndrome. Resuscitation 2022, 179, 116–123. [Google Scholar] [CrossRef]
- Dolmatova, E.V.; Wang, K.; Mandavilli, R.; Griendling, K.K. The Effects of Sepsis on Endothelium and Clinical Implications. Cardiovasc. Res. 2021, 117, 60–73. [Google Scholar] [CrossRef]
- Sugita, A.; Kinoshita, K.; Sakurai, A.; Chiba, N.; Yamaguchi, J.; Kuwana, T.; Sawada, N.; Hori, S. Systemic Impact on Secondary Brain Aggravation Due to Ischemia/Reperfusion Injury in Post-Cardiac Arrest Syndrome: A Prospective Observational Study Using High-Mobility Group Box 1 Protein. Crit. Care 2017, 21, 247. [Google Scholar] [CrossRef]
- De Rosa, S.; Antonelli, M.; Ronco, C. Hypothermia and Kidney: A Focus on Ischaemia–Reperfusion Injury. Nephrol. Dial. Transplant. 2016, 32, gfw038. [Google Scholar] [CrossRef]
- Tujjar, O.; Mineo, G.; Dell’Anna, A.; Poyatos-Robles, B.; Donadello, K.; Scolletta, S.; Vincent, J.-L.; Taccone, F.S. Acute Kidney Injury after Cardiac Arrest. Crit. Care 2015, 19, 169. [Google Scholar] [CrossRef]
- Roman-Pognuz, E.; Elmer, J.; Rittenberger, J.C.; Guyette, F.X.; Berlot, G.; De Rosa, S.; Peratoner, A.; de Arroyabe, B.M.L.; Lucangelo, U.; Callaway, C.W. Markers of Cardiogenic Shock Predict Persistent Acute Kidney Injury after out of Hospital Cardiac Arrest. Heart Lung 2019, 48, 126–130. [Google Scholar] [CrossRef]
- Sandroni, C.; Dell’anna, A.M.; Tujjar, O.; Geri, G.; Cariou, A.; Taccone, F.S. Acute Kidney Injury after Cardiac Arrest: A Systematic Review and Meta-Analysis of Clinical Studies. Minerva Anestesiol. 2016, 82, 989–999. [Google Scholar] [PubMed]
- Geri, G.; Guillemet, L.; Dumas, F.; Charpentier, J.; Antona, M.; Lemiale, V.; Bougouin, W.; Lamhaut, L.; Mira, J.-P.; Vinsonneau, C.; et al. Acute Kidney Injury after Out-of-Hospital Cardiac Arrest: Risk Factors and Prognosis in a Large Cohort. Intensive Care Med. 2015, 41, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, E.; Kwiatkowski, S.; Dziedziejko, V.; Tomasiewicz, I.; Domański, L. Renal Microcirculation Injury as the Main Cause of Ischemic Acute Kidney Injury Development. Biology 2023, 12, 327. [Google Scholar] [CrossRef]
- Perman, S.M.; Bartos, J.A.; Del Rios, M.; Donnino, M.W.; Hirsch, K.G.; Jentzer, J.C.; Kudenchuk, P.J.; Kurz, M.C.; Maciel, C.B.; Menon, V.; et al. Temperature Management for Comatose Adult Survivors of Cardiac Arrest: A Science Advisory from the American Heart Association. Circulation 2023, 148, 982–988. [Google Scholar] [CrossRef]
- Bray, J.E.; Grasner, J.-T.; Nolan, J.P.; Iwami, T.; Ong, M.E.H.; Finn, J.; McNally, B.; Nehme, Z.; Sasson, C.; Tijssen, J.; et al. Cardiac Arrest and Cardiopulmonary Resuscitation Outcome Reports: 2024 Update of the Utstein Out-of-Hospital Cardiac Arrest Registry Template. Circulation 2024, 150, e203–e223. [Google Scholar] [CrossRef]
- Grand, J.; Hassager, C.; Winther-Jensen, M.; Rundgren, M.; Friberg, H.; Horn, J.; Wise, M.P.; Nielsen, N.; Kuiper, M.; Wiberg, S.; et al. Mean Arterial Pressure during Targeted Temperature Management and Renal Function after Out-of-Hospital Cardiac Arrest. J. Crit. Care 2019, 50, 234–241. [Google Scholar] [CrossRef]
- Belur, A.D.; Sedhai, Y.R.; Truesdell, A.G.; Khanna, A.K.; Mishkin, J.D.; Belford, P.M.; Zhao, D.X.; Vallabhajosyula, S. Targeted Temperature Management in Cardiac Arrest: An Updated Narrative Review. Cardiol. Ther. 2023, 12, 65–84. [Google Scholar] [CrossRef]
- Ilaria, G.; Kianoush, K.; Ruxandra, B.; Francesca, M.; Mariarosa, C.; Davide, G.; Claudio, R. Clinical Adoption of Nephrocheck® in the Early Detection of Acute Kidney Injury. Ann. Clin. Biochem. 2021, 58, 6–15. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N.; KDIGO AKI Guideline Work Group. Diagnosis, Evaluation, and Management of Acute Kidney Injury: A KDIGO Summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef]
- De Rosa, S.; Samoni, S.; Ronco, C. Creatinine-Based Definitions: From Baseline Creatinine to Serum Creatinine Adjustment in Intensive Care. Crit. Care 2016, 20, 69. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Zarbock, A.; Goldstein, S.; Kashani, K.; Macedo, E.; Murugan, R.; Bell, M.; Forni, L.; Guzzi, L.; Joannidis, M.; et al. Recommendations on Acute Kidney Injury Biomarkers from the Acute Disease Quality Initiative Consensus Conference: A Consensus Statement. JAMA Netw. Open 2020, 3, e2019209. [Google Scholar] [CrossRef] [PubMed]
- Kashani, K.; Al-Khafaji, A.; Ardiles, T.; Artigas, A.; Bagshaw, S.M.; Bell, M.; Bihorac, A.; Birkhahn, R.; Cely, C.M.; Chawla, L.S.; et al. Discovery and Validation of Cell Cycle Arrest Biomarkers in Human Acute Kidney Injury. Crit. Care 2013, 17, R25. [Google Scholar] [CrossRef]
- De Rosa, S.; De Cal, M.; Joannidis, M.; Villa, G.; Pacheco, J.L.S.; Virzì, G.M.; Samoni, S.; D’ippoliti, F.; Marcante, S.; Visconti, F.; et al. The Effect of Whole-Body Cooling on Renal Function in Post-Cardiac Arrest Patients. BMC Nephrol. 2017, 18, 376. [Google Scholar] [CrossRef]
- Adler, C.; Heller, T.; Schregel, F.; Hagmann, H.; Hellmich, M.; Adler, J.; Reuter, H. TIMP-2/IGFBP7 Predicts Acute Kidney Injury in out-of-Hospital Cardiac Arrest Survivors. Crit. Care 2018, 22, 126. [Google Scholar] [CrossRef]
- Latoch, E.; Konończuk, K.; Taranta-Janusz, K.; Muszyńska-Rosłan, K.; Szymczak, E.; Wasilewska, A.; Krawczuk-Rybak, M. Urine NGAL and KIM-1: Tubular Injury Markers in Acute Lymphoblastic Leukemia Survivors. Cancer Chemother. Pharmacol. 2020, 86, 741–749. [Google Scholar] [CrossRef]
- Polderman, K.H.; Peerdeman, S.M.; Girbes, A.R.J. Hypophosphatemia and Hypomagnesemia Induced by Cooling in Patients with Severe Head Injury. J. Neurosurg. 2001, 94, 697–705. [Google Scholar] [CrossRef]
- Stocks, J.M.; Taylor, N.A.S.; Tipton, M.J.; Greenleaf, J.E. Human Physiological Responses to Cold Exposure. Aviat. Space Environ. Med. 2004, 75, 444–457. [Google Scholar]
- Granberg, P.O. Human Physiology under Cold Exposure. Arctic Med. Res. 1991, 50 (Suppl. S6), 23–27. [Google Scholar]
- Weinberg, A.D. Hypothermia. Ann. Emerg. Med. 1993, 22, 370–377. [Google Scholar] [CrossRef]
- Bellomo, R.; Märtensson, J.; Eastwood, G.M. Metabolic and Electrolyte Disturbance after Cardiac Arrest: How to Deal with It. Best Pract. Res. Clin. Anaesthesiol. 2015, 29, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Basken, R.; Finger, J.; Erstad, B. Targeted Temperature Management: Quantifying the Extent of Serum Electrolyte and Blood Glucose Shifts in Postcardiac Arrest Patients. Ther. Hypothermia Temp. Manag. 2020, 10, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Mazer-Amirshahi, M.; Perman, S.M.; Grossestreuer, A.V.; Neumar, R.W.; Gaieski, D.F. Magnesium Depletion in Patients Treated with Therapeutic Hypothermia After Cardiac Arrest. Ther. Hypothermia Temp. Manag. 2014, 4, 188–192. [Google Scholar] [CrossRef]
- Hou, S.; Zhang, L.; Ji, H.; Zhao, T.; Hu, M.; Jiang, Y.; Sun, Q.; Zhang, M.; Dou, M. Development and Evaluation of the Model for Acute Kidney Injury in Patients with Cardiac Arrest after Successful Resuscitation. BMC Cardiovasc. Disord. 2024, 24, 440. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Entire Cohort (n = 142) | TH 33 °C (n = 36) | TTM 35 °C (n = 54) | No Treatment (n = 52) | p-Value |
|---|---|---|---|---|---|
| Male (%) | 102 (71.8%) | 29 (80.6%) | 32 (59.3%) | 41 (78.8%) | 0.102 |
| Age (yrs) | 62 (52–74) | 60 (53–68) | 58 (50–72) | 66 (51–76) | 0.295 |
| BMI (kg/m2) | 25.2 (23.8–27.7) | 25.8 (23.1–28.2) | 24.9 (24.0–26.8) | 25.2 (23.7–27.7) | 0.967 |
| SOFA score | 9 (7–11) | 9 (8.2–10.3) | 9 (7.5–12.0) | 8 (7–11) | 0.177 |
| SAPS II score | 57 (48–66) | 54 (50–60) | 61 (52–68) | 54 (42–71) | 0.079 |
| Cardiac arrest rhythm | 0.008 | ||||
| -Shockable (VF/VT) (%) | 93 (64.5%) | 30 (83.4%) | 37 (68.5%) | 25 (49.0%) | |
| -Non-shockable (%) | 49 (34.8%) | 6 (16.7%) | 17 (31.5%) | 26 (51.0%) | |
| Re-arrest after ROSC (%) | 0.196 | ||||
| -Shockable (%) | 19.0 | 30.6 | 18.5 | 11.5 | |
| -Non-shockable (%) | 7.7 | 2.8 | 9.3 | 9.6 | |
| -No re-arrest (%) | 73.2 | 66.7 | 72.2 | 78.8 | |
| GCS post-ROSC | 3 (3–4) | 3 (3–3.25) | 3 (3–3) | 3 (3–7.5) | 0.010 |
| Hypertension (%) | 46.5 | 38.9 | 44.4 | 53.8 | 0.357 |
| Previous renal disease (%) | 14.1 | 13.9 | 9.3 | 19.2 | 0.337 |
| Previous cardiac surgery (%) | 4.2 | 5.6 | 3.7 | 3.8 | 0.038 |
| -CABG | 17.6 | 0.0 | 25.9 | 21.2 | |
| -Valve Surgery (%) | 0.7 | 0.0 | 0.0 | 1.9 | |
| Coronary artery disease (%) | 45.1 | 66.7 | 44.4 | 36.5 | 0.040 |
| Insulin-dependent diabetes (%) | 10.6 | 22.9 | 3.7 | 1.9 | 0.041 |
| COPD (%) | 7.0 | 8.3 | 1.9 | 11.5 | 0.141 |
| Variable | Entire Cohort (n = 142) | TH 33 °C (n = 36) | TTM 35 °C (n = 54) | No Treatment (n = 52) | p-Value |
|---|---|---|---|---|---|
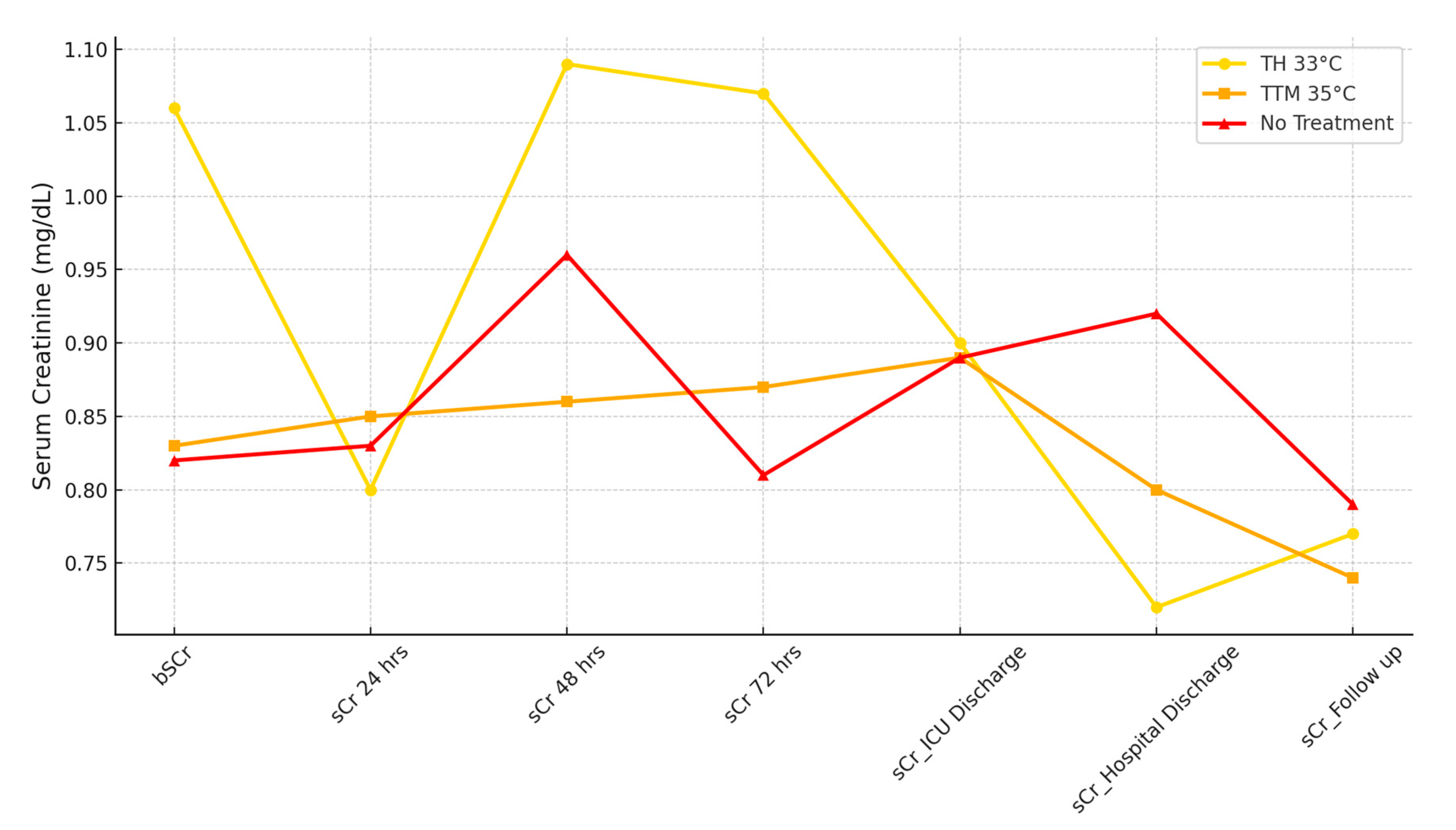
| Baseline Creatinine (mg/dL) | 0.84 (0.80–1.02) | 1.06 (1.02–1.09) | 0.83 (0.80–0.86) | 0.82 (0.80–0.89) | <0.001 |
| Creatinine at Admission | 1.03 (0.85–1.26) | 1.15 (0.95–1.21) | 1.02 (0.81–1.26) | 1.03 (0.81–1.27) | 0.523 |
| Creatinine (Corrected for Fluid Balance) | |||||
| 0.84 (0.78–0.98) | 0.80 (0.65–1.07) | 0.85 (0.80–1.06) | 0.83 (0.80–0.89) | 0.333 |
| 0.96 (0.64–1.44) | 1.09 (0.80–1.40) | 0.86 (0.59–1.73) | 0.96 (0.61–1.36) | 0.516 |
| 0.90 (0.64–1.33) | 1.07 (0.79–1.41) | 0.87 (0.60–1.47) | 0.81 (0–1.13) | 0.037 |
| Creatinine at ICU Discharge | 0.90 (0.61–1.12) | 0.90 (0.42–2.32) | 0.89 (0.33–1.12) | 0.89 (0.6–1.19) | 0.12 |
| Creatinine at Hospital Discharge | 0.82 (0.60–1.12) | 0.72 (0.57–0.91) | 0.80 (0.54–1.02) | 0.92 (0.70–1.42) | 0.017 |
| Creatinine at Follow-Up | 0.78 (0.63–1.0) | 0.77 (0.66–0.90) | 0.74 (0.56–0.91) | 0.79 (0.66–1.49) | 0.546 |
| Urinary Output (mL) | |||||
| 1750 (1080–2762) | 2242 (1403–2844) | 1552 (964–2408) | 1600 (1080–2870) | 0.07 |
| 2800 (2122–3477) | 2877 (2362–3552) | 2540 (2105–3487) | 2465 (1372–3255) | 0.236 |
| 2560 (1880–3764) | 3185 (2538–4060) | 2460 (1665–3482) | 2001 (960–3200) | 0.004 |
| Fluid Balance (mL) | |||||
| 49.8 (−931–1092) | 333 (−434–1280) | 347 (−578–1777) | 250 (−1067–1054) | 0.43 |
| 748 (−196.7–1669) | 1522 (488–2236) | 382 (−397–1553) | 228 (−393–1530) | 0.003 |
| 418 (−691–1393) | 621 (−389–1749) | 801 (−503–1552) | −176 (−739–671) | 0.17 |
| Cumulative Fluid Balance | 1342 (−1073–2853) | 2441 (437–4043) | 500 (541–2781) | 1166 (−1705–2122) | 0.034 |
| ICU Stay (Days) | 8 (4–14) | 9 (4.5–12.5) | 10 (7–19) | 3 (2–7.25) | <0.001 |
| Ventilation Days | 7 (3–12) | 8 (4–12.7) | 9.5 (5.25–17.7) | 2 (1–6.25) | <0.001 |
| Parameter | TH 33 °C (n = 36) | TTM 35 °C (n = 54) | No Treatment (n = 52) | p-Value |
|---|---|---|---|---|
| AKI Development (%) | ||||
| AKI at 24 h | 5 (13.9) | 8 (14.9) | 9 (17.3) | 0.896 |
| AKI at 48 h | 15 (41.7) | 20 (37.1) | 10 (18.8) | 0.047 |
| AKI at 72 h | 12 (33.3) | 15 (27.8) | 17 (32.7) | 0.809 |
| KDIGO Staging at 24 h | ||||
| KDIGO Stage 1 (%) | 5 (13.9) | 6 (11.1) | 7 (13.5) | 0.734 |
| KDIGO Stage 2 (%) | 0 (0) | 2 (3.7) | 2 (3.8) | 0.472 |
| KDIGO Stage 3 (%) | 0 (0) | 0 (0) | 0 (0) | - |
| KDIGO Staging at 48 h | ||||
| KDIGO Stage 1 (%) | 12 (33.3) | 9 (16.7) | 5 (9.6) | 0.054 |
| KDIGO Stage 2 (%) | 2 (5.6) | 5 (9.3) | 0 (0) | 0.029 |
| KDIGO Stage 3 (%) | 1 (2.8) | 6 (11.1) | 10 (19.2) | 0.016 |
| KDIGO Staging at 72 h | ||||
| KDIGO Stage 1 (%) | 8 (22.2) | 6 (11.1) | 7 (13.5) | 0.392 |
| KDIGO Stage 2 (%) | 3 (8.3) | 4 (7.4) | 0 (0) | 0.104 |
| KDIGO Stage 3 (%) | 1 (2.8) | 5 (9.3) | 10 (19.2) | 0.024 |
| Nephrocheck Results | ||||
| Risk Class | Not performed | Intermediate | AKI Subclinical [22] | - |
| Median Value | Not performed | 1.54 [0.8–3.46] | 1.0 [0.19–2.18] | 0.105 |
| sCr at Admission (mg/dL) | 1.15 [0.95–1.21] | 1.02 [0.81–1.26] | 1.03 [0.81–1.27] | 0.742 |
| Time Variable | Entire Cohort | TH 33 °C | TTM 35 °C | p-Value |
|---|---|---|---|---|
| Time to 33 °C (CA onset) | 273 [209–390] | 280.5 [240–385] | 275 [180–395] | 0.740 |
| Time to 33 °C (TH Induction) | 180 [90–260] | 184.5 [120–248] | 120 [34–293] | 0.329 |
| Maintenance Duration | 1440 [1440–1440] | 1440 [1440–1557] | 1440 [1440–1440] | 0.027 |
| Rewarming Time to 36 °C | 720 [540–1960] | 600 [480–720] | 1960 [1041–2880] | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Rosa, S.; Lassola, S.; Visconti, F.; De Cal, M.; Cattin, L.; Rizzello, V.; Lampariello, A.; Zannato, M.; Danzi, V.; Marcante, S. Acute Kidney Injury in Patients After Cardiac Arrest: Effects of Targeted Temperature Management. Life 2025, 15, 265. https://doi.org/10.3390/life15020265
De Rosa S, Lassola S, Visconti F, De Cal M, Cattin L, Rizzello V, Lampariello A, Zannato M, Danzi V, Marcante S. Acute Kidney Injury in Patients After Cardiac Arrest: Effects of Targeted Temperature Management. Life. 2025; 15(2):265. https://doi.org/10.3390/life15020265
Chicago/Turabian StyleDe Rosa, Silvia, Sergio Lassola, Federico Visconti, Massimo De Cal, Lucia Cattin, Veronica Rizzello, Antonella Lampariello, Marina Zannato, Vinicio Danzi, and Stefano Marcante. 2025. "Acute Kidney Injury in Patients After Cardiac Arrest: Effects of Targeted Temperature Management" Life 15, no. 2: 265. https://doi.org/10.3390/life15020265
APA StyleDe Rosa, S., Lassola, S., Visconti, F., De Cal, M., Cattin, L., Rizzello, V., Lampariello, A., Zannato, M., Danzi, V., & Marcante, S. (2025). Acute Kidney Injury in Patients After Cardiac Arrest: Effects of Targeted Temperature Management. Life, 15(2), 265. https://doi.org/10.3390/life15020265