
Advanced Secondary Intention Healing for Complex Soft-Tissue Defects Using Reprocessed Micronized Acellular Dermal Matrix


Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Inclusion and Exclusion Criteria
2.3. Reprocessed mADM
2.4. Methods
2.5. Statistical Analysis
3. Results
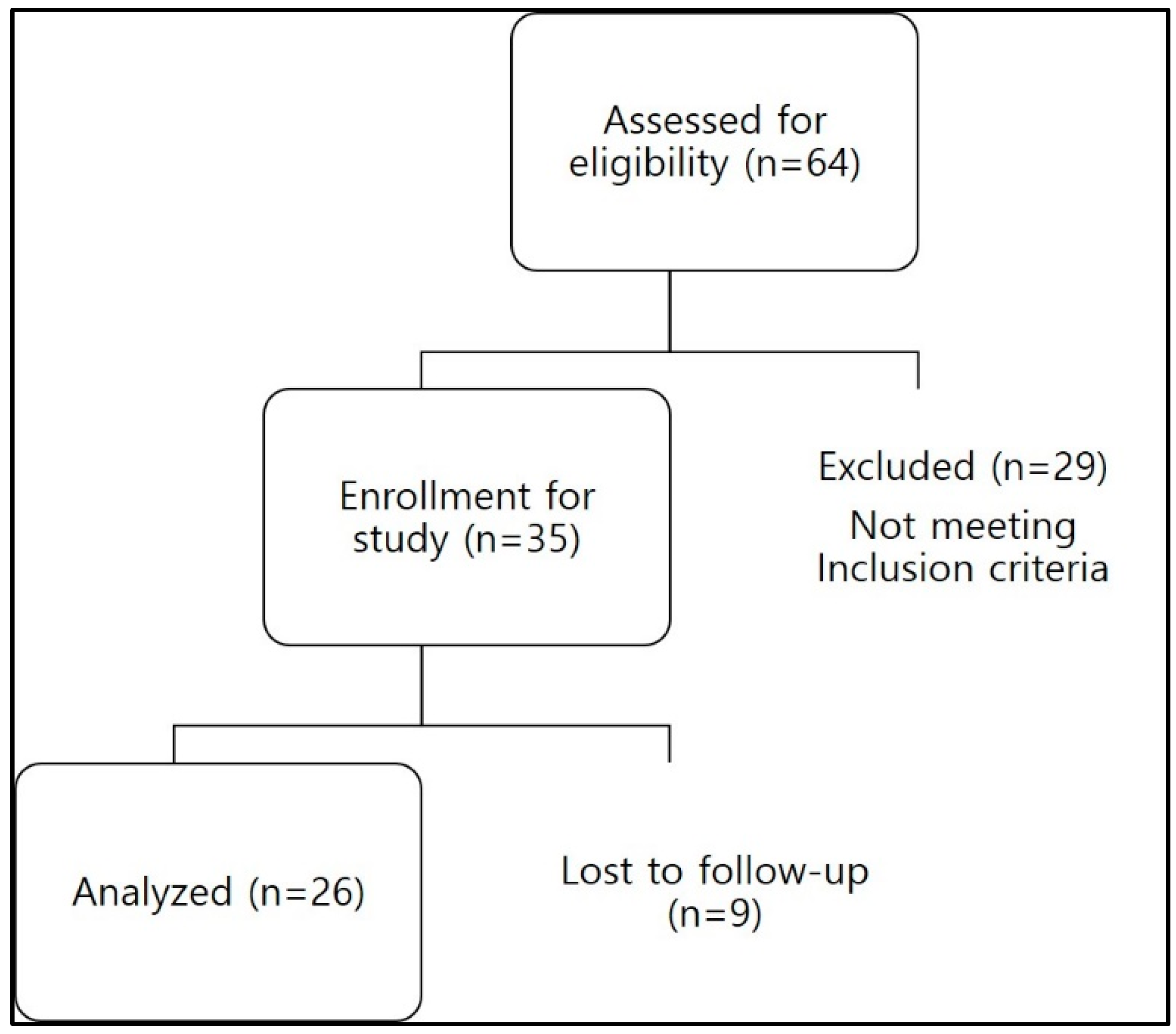
3.1. Patient Enrollment and Exclusion
3.2. Demographic and Clinical Characteristics
3.3. Classification Based on Complex Wound Type
3.4. Wound Area Reduction Results
3.5. Correlation Analysis of Patient Variables and Wound Healing Outcomes
3.6. Cases
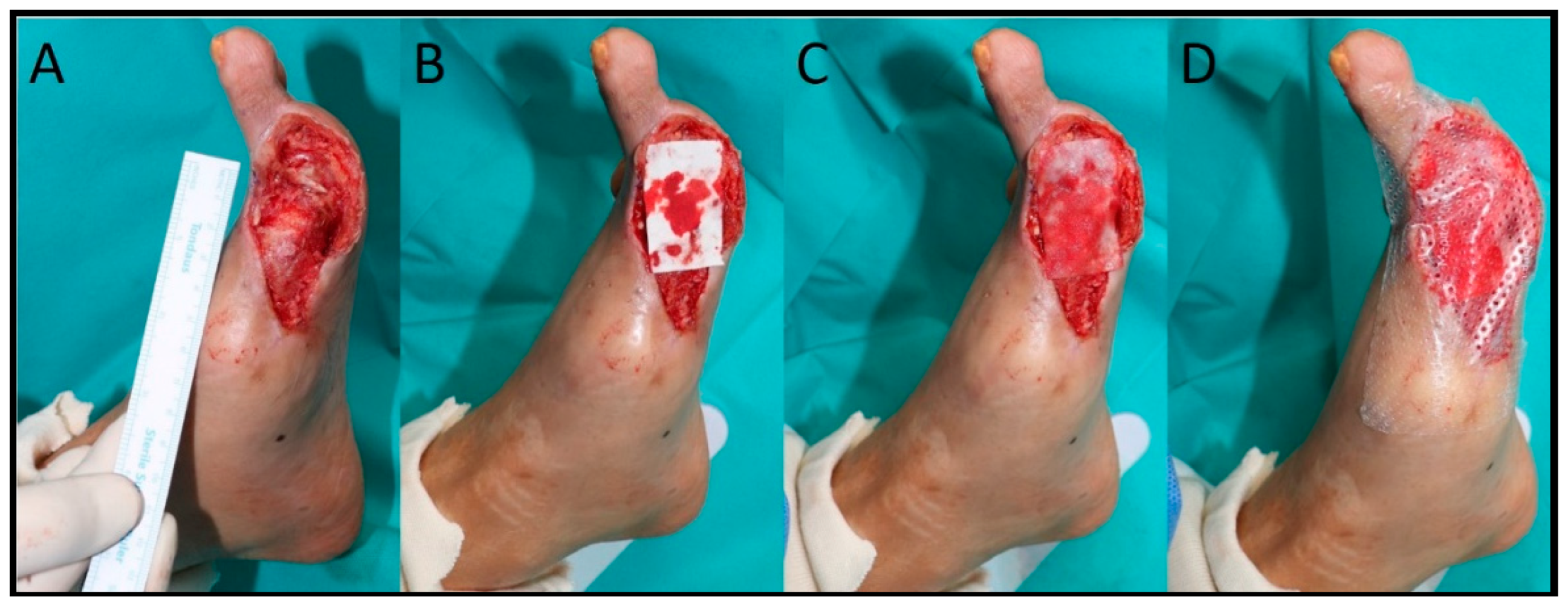
3.6.1. Case 1
3.6.2. Case 2
3.6.3. Case 3
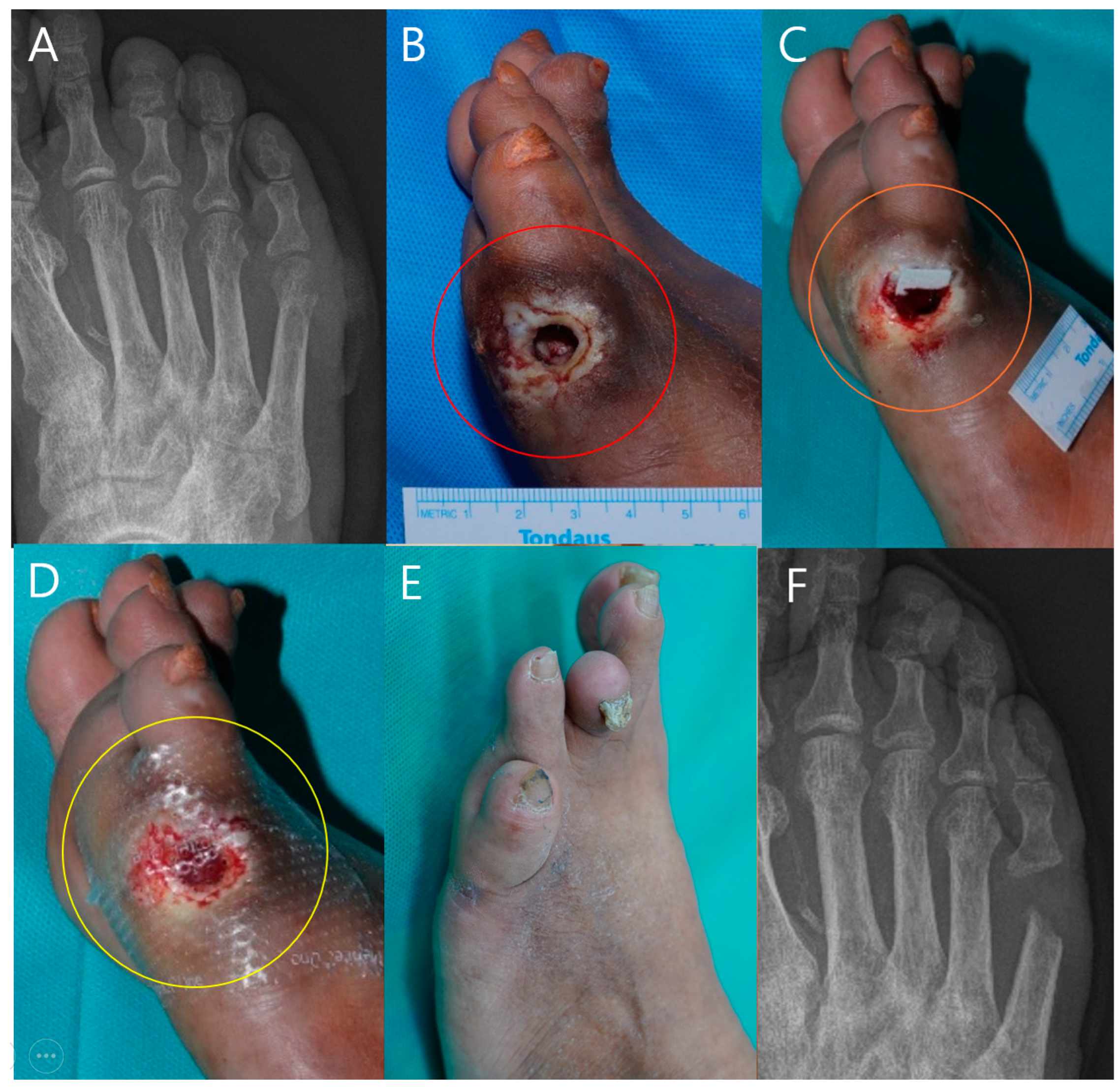
3.6.4. Case 4
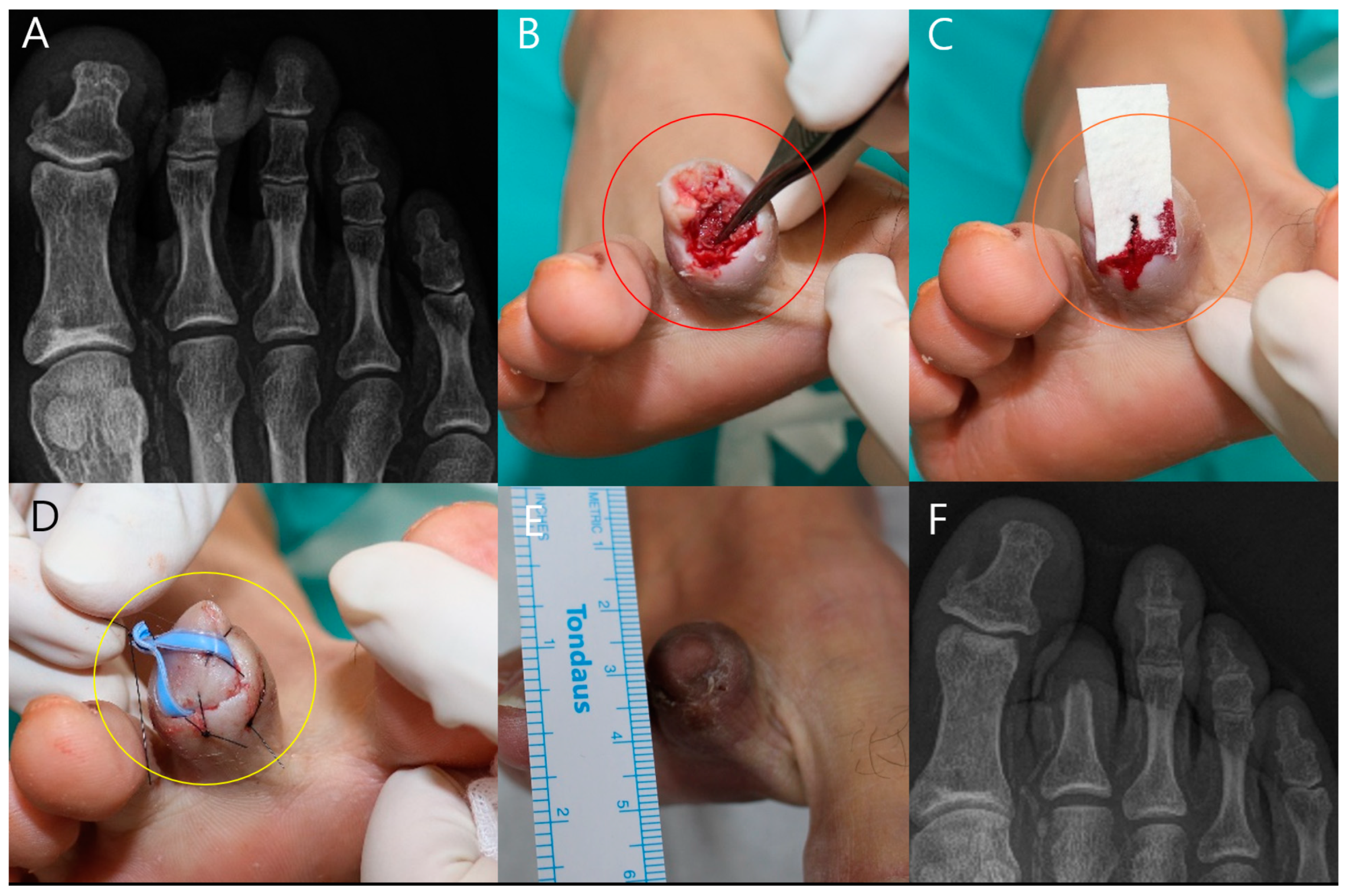
3.6.5. Case 5
3.6.6. Summary of Case
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schultz, G.S.; Sibbald, R.G.; Falanga, V.; Ayello, E.A.; Dowsett, C.; Harding, K.; Romanelli, M.; Stacey, M.C.; Teot, L.; Vanscheidt, W. Wound bed preparation: A systematic approach to wound management. Wound Repair Regen. 2003, 11 (Suppl. S1), S1–S28. [Google Scholar] [CrossRef] [PubMed]
- Falanga, V. Wound healing and its impairment in the diabetic foot. Lancet 2005, 366, 1736–1743. [Google Scholar] [CrossRef] [PubMed]
- Veves, A.; Sheehan, P.; Pham, H.T. A randomized, controlled trial of Promogran (a collagen/oxidized regenerated cellulose dressing) vs standard treatment in the management of diabetic foot ulcers. Arch. Surg. 2002, 137, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Petrie, K.; Cox, C.T.; Becker, B.C.; MacKay, B.J. Clinical applications of acellular dermal matrices: A review. Scars Burn. Heal. 2022, 8, 20595131211038313. [Google Scholar] [CrossRef] [PubMed]
- Tognetti, L.; Pianigiani, E.; Ierardi, F.; Lorenzini, G.; Casella, D.; Liso, F.G.; De Pascalis, A.; Cinotti, E.; Rubegni, P. The use of human acellular dermal matrices in advanced wound healing and surgical procedures: State of the art. Dermatol. Ther. 2021, 34, e14987. [Google Scholar] [CrossRef]
- Ahn, J.; Park, H.Y.; Shetty, A.A.; Hwang, W. Use of injectable acellular dermal matrix combined with negative pressure wound therapy in open diabetic foot amputation. J. Wound Care 2022, 31, 310–320. [Google Scholar] [CrossRef]
- Kim, T.H.; Park, J.H.; Jeong, H.G.; Wee, S.Y. The utility of novel fish-skin derived acellular dermal matrix (Kerecis) as a wound dressing material. J. Wound Manag. Res. 2021, 17, 39–47. [Google Scholar] [CrossRef]
- Park, J.Y.; Lee, T.G.; Kim, J.Y.; Lee, M.C.; Chung, Y.K.; Lee, W.J. Acellular dermal matrix to treat full thickness skin defects: Follow-up subjective and objective skin quality assessments. Arch. Craniofac. Surg. 2014, 15, 14–21. [Google Scholar] [CrossRef]
- Byeon, J.Y.; Hwang, Y.S.; Choi, H.J.; Kim, J.H.; Lee, D.W. A long-term follow-up study of diabetic foot ulcer using micronized acellular dermal matrix. Int. Wound J. 2023, 20, 1622–1637. [Google Scholar] [CrossRef]
- Hardman, R.L.; Jazaeri, O.; Yi, J.; Smith, M.; Gupta, R. Overview of classification systems in peripheral artery disease. Semin. Intervent. Radiol. 2014, 31, 378–388. [Google Scholar] [CrossRef]
- Aramwit, P. Introduction to biomaterials for wound healing. In Wound Healing Biomaterials; Agren, M.S., Ed.; Woodhead Publishing: Cambridge, UK, 2016; Volume 2, pp. 3–38. [Google Scholar]
- Candage, R.; Jones, K.; Luchette, F.A.; Sinacore, J.M.; Vandevender, D.; Reed, R.L., 2nd. Use of human acellular dermal matrix for hernia repair: Friend or foe? Surgery 2008, 144, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Brigido, S.A. The use of an acellular dermal regenerative tissue matrix in the treatment of lower extremity wounds: A prospective 16-week pilot study. Int. Wound J. 2006, 3, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Mangini, N.; Galvano, F.; Pucci, R.; Battisti, A.; Cassoni, A.; Valentini, V. Dermal regeneration template: Reconstruction in oral cancer defects. J. Maxillofac. Oral Surg. 2023, 22, 151–156. [Google Scholar] [CrossRef]
- Singer, A.J.; Boyce, S.T. Burn wound healing and tissue engineering. J. Burn Care Res. 2017, 38, e605–e613. [Google Scholar] [CrossRef]
- Cho, J.; Hwang, H.; Song, S.Y.; Suh, H.P.; Hong, J.P. Evaluation of wound healing effects of micronized acellular dermal matrix in combination with negative pressure wound therapy: In vivo study. Int. Wound J. 2023, 20, 1053–1060. [Google Scholar] [CrossRef]
- Schultz, G.S.; Wysocki, A. Interactions between extracellular matrix and growth factors in wound healing. Wound Repair Regen. 2009, 17, 153–162. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Raines, R.T. Collagen-based biomaterials for wound healing. Biopolymers 2014, 101, 821–833. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & scaffolds for tissue engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Martin, P. Wound healing--aiming for perfect skin regeneration. Science 1997, 276, 75–81. [Google Scholar] [CrossRef]
- Greenhalgh, D.G. The role of growth factors in wound healing. J. Trauma 1996, 41, 159–167. [Google Scholar] [CrossRef]
- Liakouli, V.; Cipriani, P.; Di Benedetto, P.; Ruscitti, P.; Carubbi, F.; Berardicurti, O.; Panzera, N.; Giacomelli, R. The role of extracellular matrix components in angiogenesis and fibrosis: Possible implication for systemic sclerosis. Mod. Rheumatol. 2018, 28, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Rnjak-Kovacina, J.; Weiss, A.S. The role of elastin in wound healing and dermal substitute design. In Dermal Replacements in General, Burn, and Plastic Surgery; Kamolz, L.P., Lumenta, D., Eds.; Springer: Vienna, Austria, 2013; pp. 57–66. [Google Scholar] [CrossRef]
- Reneker, D.H.; Alexander, L.Y. Electrospinning jets and polymer nanofibers. Polymer 2008, 49, 2387–2425. [Google Scholar] [CrossRef]
- Frykberg, R.G.; Banks, J. Challenges in the treatment of chronic wounds. Adv. Wound Care 2015, 4, 560–582. [Google Scholar] [CrossRef]
- Brett, D. A review of collagen and collagen-based wound dressings. Wounds 2008, 20, 347–356. [Google Scholar]
- Falanga, V. Classifications for wound bed preparation and stimulation of chronic wounds. Wound Repair Regen. 2000, 8, 347–352. [Google Scholar]
- Hahn, H.M.; Lee, D.H.; Lee, I.J. Ready-to-use micronized human acellular dermal matrix to accelerate wound healing in diabetic foot ulcers: A prospective randomized pilot study. Adv. Skin Wound Care 2021, 34, 1–6. [Google Scholar] [CrossRef]
- Cornwell, K.G.; Landsman, A.; James, K.S. Extracellular matrix biomaterials for soft tissue repair. Clin. Podiatr. Med. Surg. 2009, 26, 507–523. [Google Scholar] [CrossRef]
- Ren, S.Y.; Liu, Y.S.; Zhu, G.J.; Liu, M.; Shi, S.H.; Ren, X.D.; Hao, Y.G.; Gao, R.D. Strategies and challenges in the treatment of chronic venous leg ulcers. World J. Clin. Cases 2020, 8, 5070–5085. [Google Scholar] [CrossRef]
- Attinger, C.E.; Janis, J.E.; Steinberg, J.; Schwartz, J.; Al-Attar, A.; Couch, K. Clinical approach to wounds: Débridement and wound bed preparation including the use of dressings and wound-healing adjuvants. Plast. Reconstr. Surg. 2006, 117, 72S–109S. [Google Scholar] [CrossRef]
- Jabo, B.; Lin, A.C.; Aljehani, M.A.; Ji, L.; Morgan, J.W.; Selleck, M.J.; Kim, H.Y.; Lum, S.S. Impact of breast reconstruction on time to definitive surgical treatment, adjuvant therapy, and breast cancer outcomes. Ann. Surg. Oncol. 2018, 25, 3096–3105. [Google Scholar] [CrossRef]
- Le Joncour, A.; Soudet, S.; Dupont, A.; Espitia, O.; Koskas, F.; Cluzel, P.; Hatron, P.Y.; Emmerich, J.; Cacoub, P.; Resche-Rigon, M.; et al. Long-term outcome and prognostic factors of complications in thromboangiitis obliterans (Buerger’s disease): A multicenter study of 224 patients. J. Am. Heart Assoc. 2018, 7, e010677. [Google Scholar] [CrossRef] [PubMed]
- Olin, J.W. Thromboangiitis obliterans (Buerger’s disease). N. Engl. J. Med. 2000, 343, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Lipsky, B.A. Diabetic foot infections: Stepwise medical and surgical management. Int. Wound J. 2004, 1, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Saricilar, E.C.; Huang, S. Comparison of porcine and human acellular dermal matrix outcomes in wound healing: A deep dive into the evidence. Arch. Plast. Surg. 2021, 48, 433–439. [Google Scholar] [CrossRef]
- Luze, H.; Nischwitz, S.P.; Smolle, C.; Zrim, R.; Kamolz, L.P. The use of acellular fish skin grafts in burn wound management—A systematic review. Medicina 2022, 58, 912. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Patients aged 18 to 90 years with full-thickness skin defects classified as complex wounds. | Patients treated with additional types of ADMs besides mADMs. |
| Patients treated exclusively with mADMs without other types of ADMs. | Patients who underwent surgical treatments such as primary closure, skin grafts, or flap coverage. |
| Patients who were lost to follow-up during the treatment period. | |
| Patients with uncontrolled chronic conditions that could interfere with wound healing (e.g., severe uncontrolled diabetes, active malignancy). |
| Grade | Category | Clinical Description | Objective Criteria |
|---|---|---|---|
| 0 | 0 | Asymptomatic—no hemodynamically significant occlusive disease | Normal treadmill or reactive hyperemia test |
| 1 | Mild claudication | Completes treadmill exercise; AP after exercise > 50 mmHg but at least 20 mmHg lower than the resting value | |
| I | 2 | Moderate claudication | Between categories 1 and 3 |
| 3 | Severe claudication | Cannot complete standard treadmill exercise, and AP after exercise < 50 mmHg | |
| II | 4 | Ischemic rest pain | Resting AP < 40 mmHg, flat or barely pulsatile ankle or metatarsal PVR; TP < 30 mmHg |
| III | 5 | Minor tissue loss—nonhealing ulcer, focal gangrene with diffuse pedal ischemia | Resting AP < 60 mmHg, ankle or metatarsal PVR flat or barely pulsatile; TP < 40 mmHg |
| 6 | Major tissue loss—extending above TM level, functional foot no longer salvageable | Same as category 5 |
| Characteristic | N (%) |
|---|---|
| Sex | |
| Male | 24 (92.3%) |
| Female | 2 (7.7%) |
| Age (years) | 65.00 (18.00) |
| <65 | 12 (46.2%) |
| ≥65 | 14 (53.8%) |
| BMI (kg/m2) | 23.907 (5.004) |
| <25 | 17 (65.4%) |
| ≥25 | 9 (34.6%) |
| Smoking | |
| Non-smoker | 13 (50.0%) |
| Smoker | 13 (50.0%) |
| DM | |
| None | 6 (23.1%) |
| Diagnosed | 20 (76.9%) |
| HbA1c | 6.900 (2.3) |
| Controlled < 6.0 | 7 (26.9%) |
| Uncontrolled ≥ 6.0 | 19 (73.1%) |
| ABI | 1.100 (0.24) |
| ≥1.2 | 4 (21.1%) |
| <1.2 | 15 (78.9%) |
| CRP | 3.590 (20.60) |
| <5.00 | 15 (57.7%) |
| ≥5.00 | 11 (42.3%) |
| ESRD | |
| None | 20 (76.9%) |
| Diagnosed | 6 (23.1%) |
| PTA | |
| None | 23 (88.5%) |
| Identified | 3 (11.5%) |
| Location | |
| Sacral area | 3 (11.54%) |
| Lower extremity (except foot) | 2 (7.69%) |
| Foot | 21 (80.77%) |
| Wound Type | N (%) | Characteristics |
|---|---|---|
| Poor blood supply due to obstruction in the lower extremities | 10 (38.5%) | Wounds with poor vascular supply, often resulting in inadequate healing conditions. Includes cases where PTA has failed. |
| Deep tissue defects exposing the bone, tendon, or articular surface | 6 (23.1%) | Wounds with significant tissue loss and exposure of deeper structures such as the bone or tendon. |
| Infected or inflamed wounds unsuitable for grafting | 5 (19.2%) | Wounds complicated due to infection or inflammation, including resistant bacteria, making grafting difficult or impossible. |
| Systemic vasculopathy (e.g., Buerger’s disease) | 3 (11.5%) | Wounds in patients with systemic vascular diseases affecting the overall blood supply and healing. |
| Poor general condition preventing surgery | 2 (7.7%) | Wounds in patients with severe comorbidities or poor general health precluding surgical options. |
| Median (IQR) | |
|---|---|
| Initial wound area | 436.600 mm2 (1084.099) |
| Wound duration | 45.5 days (10.2) |
| Wound area at follow-up | 45.359 mm2 (368.446) |
| Treatment period | 35.00 days (16.00) |
| Follow-up period | 84.00 days (30.9) |
| Recovery rate | 81.359% (54.699) |
| Spearman’s Rho | p-Value | |
|---|---|---|
| Age | −0.163 | 0.427 |
| BMI | −0.109 | 0.597 |
| ABI | −0.074 | 0.765 |
| CRP | −0.049 | 0.813 |
| HbA1c | −0.079 | 0.702 |
| Age | −0.163 | 0.427 |
| Case | Age | Gender | Medical History | Wound Location | Wound Size (mm2) | mADM Applications | Healing Time (Weeks) | Follow-Up Period (Weeks) | Additional Procedures | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 62 | Male | Hypertension, Diabetes | Left Foot | 56 × 22 | 4 | 12 | 16 | None | Healing without complication |
| 2 | 57 | Male | Hypertension, Diabetes | Left Plantar | 42 × 38 | 6 | 6 | 10 | None | Healing without complication |
| 3 | 71 | Male | Diabetes, Angina | Left Foot | 87 × 31 | 8 | Excluded | 12 | Revision, Local Flap | Healing without complication |
| 4 | 65 | Male | Diabetes, Peripheral Arterial Disease | Left Foot | 30 × 40 | 5 | 8 | 12 | None | Healing without complication |
| 5 | 62 | Female | Poorly Controlled Diabetes | Right Second Toe | 20 × 20 | 1 | 6 | 10 | None | Healing without complication |
| Indication | Explanation |
|---|---|
| Small wound size | When the wound size is small, it is feasible to achieve healing without surgical intervention. |
| Infeasibility of primary surgical interventions due to infection or inflammation | When primary surgical interventions such as flap or graft are infeasible due to infection or inflammation. |
| Patient condition prohibits prolonged surgery or general anesthesia | When the patient cannot undergo general anesthesia or prolonged surgery due to their overall condition. |
| Delayed surgical intervention due to medical conditions or need for further debridement | When a free or local flap is planned but delayed due to medical conditions or the need for further debridement to expose critical structures, immediate skin grafting becomes infeasible. |
| Insufficient vascularity for surgical intervention | When vascularity is insufficient for surgical intervention due to severe obstruction or failed PTA, procedures such as free flap are hindered. |
| Systemic vasculopathy such as Buerger’s disease | When systemic vasculopathy (e.g., Buerger’s disease) makes flap procedures impossible. |
| Need for sequential localized debridement and dressing | When sequential localized debridement and dressing are necessary due to poor wound perfusion or the patient’s medical condition. |
| CGDerm® (mADM) | Kerecis® | AlloDerm® | Integra® | MatriDerm® | |
|---|---|---|---|---|---|
| Source Material | Human dermis (micronized, reprocessed) | Fish skin | Human skin | Bovine tendon | Bovine dermis and shark cartilage |
| Thickness | Adjustable (layering) | Variable | Fixed | Fixed | Fixed |
| Hydration | Rapid plasma absorption | Requires saline hydration | Requires saline hydration | Requires saline hydration | Requires saline hydration |
| Handling | Easy (thin, uniform sheet) | Moderate (requires rehydration) | Moderate (requires rehydration) | Moderate (requires rehydration) | Moderate (requires rehydration) |
| Metabolic Burden | Low | Low | Moderate | Moderate | Moderate |
| Angiogenesis Stimulation | High | Moderate | High | High | High |
| Structural Support | High | High | High | High | High |
| Clinical Applications | Secondary intention healing, wound bed preparation | Acute and chronic wounds, burns | Acute and chronic wounds, reconstructive | Acute and chronic wounds, burns | Acute and chronic wounds, burns, reconstructive |
| Advantages | Versatile, rapid absorption, easy handling, can be layered, quickly hydrates, fits contoured wounds easily | Omega-3 rich, anti-inflammatory | High integration, regenerative properties | Dual layer for epidermal and dermal regeneration | Contains glycosaminoglycans, promoting rapid vascularization and cell ingrowth |
| Disadvantages | Requires careful application to avoid shearing | Fish allergy concerns, requires rehydration | Requires rehydration, potential for immune response | Requires rehydration, potential for immune response | Requires rehydration, potential for immune response |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, H.J.; Kim, D.G.; Byeon, J.Y.; Lee, D.W.; Kim, J.H.; Kim, S.Y.; Choi, H.J. Advanced Secondary Intention Healing for Complex Soft-Tissue Defects Using Reprocessed Micronized Acellular Dermal Matrix. Life 2024, 14, 1479. https://doi.org/10.3390/life14111479
Nam HJ, Kim DG, Byeon JY, Lee DW, Kim JH, Kim SY, Choi HJ. Advanced Secondary Intention Healing for Complex Soft-Tissue Defects Using Reprocessed Micronized Acellular Dermal Matrix. Life. 2024; 14(11):1479. https://doi.org/10.3390/life14111479
Chicago/Turabian StyleNam, Ha Jong, Dong Gyu Kim, Je Yeon Byeon, Da Woon Lee, Jun Hyuk Kim, Se Young Kim, and Hwan Jun Choi. 2024. "Advanced Secondary Intention Healing for Complex Soft-Tissue Defects Using Reprocessed Micronized Acellular Dermal Matrix" Life 14, no. 11: 1479. https://doi.org/10.3390/life14111479
APA StyleNam, H. J., Kim, D. G., Byeon, J. Y., Lee, D. W., Kim, J. H., Kim, S. Y., & Choi, H. J. (2024). Advanced Secondary Intention Healing for Complex Soft-Tissue Defects Using Reprocessed Micronized Acellular Dermal Matrix. Life, 14(11), 1479. https://doi.org/10.3390/life14111479