


Eight-Year Trends in the Effect of the Great East Japan Earthquake on Obstetrics Outcomes: A Study from the Fukushima Health Management Survey

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
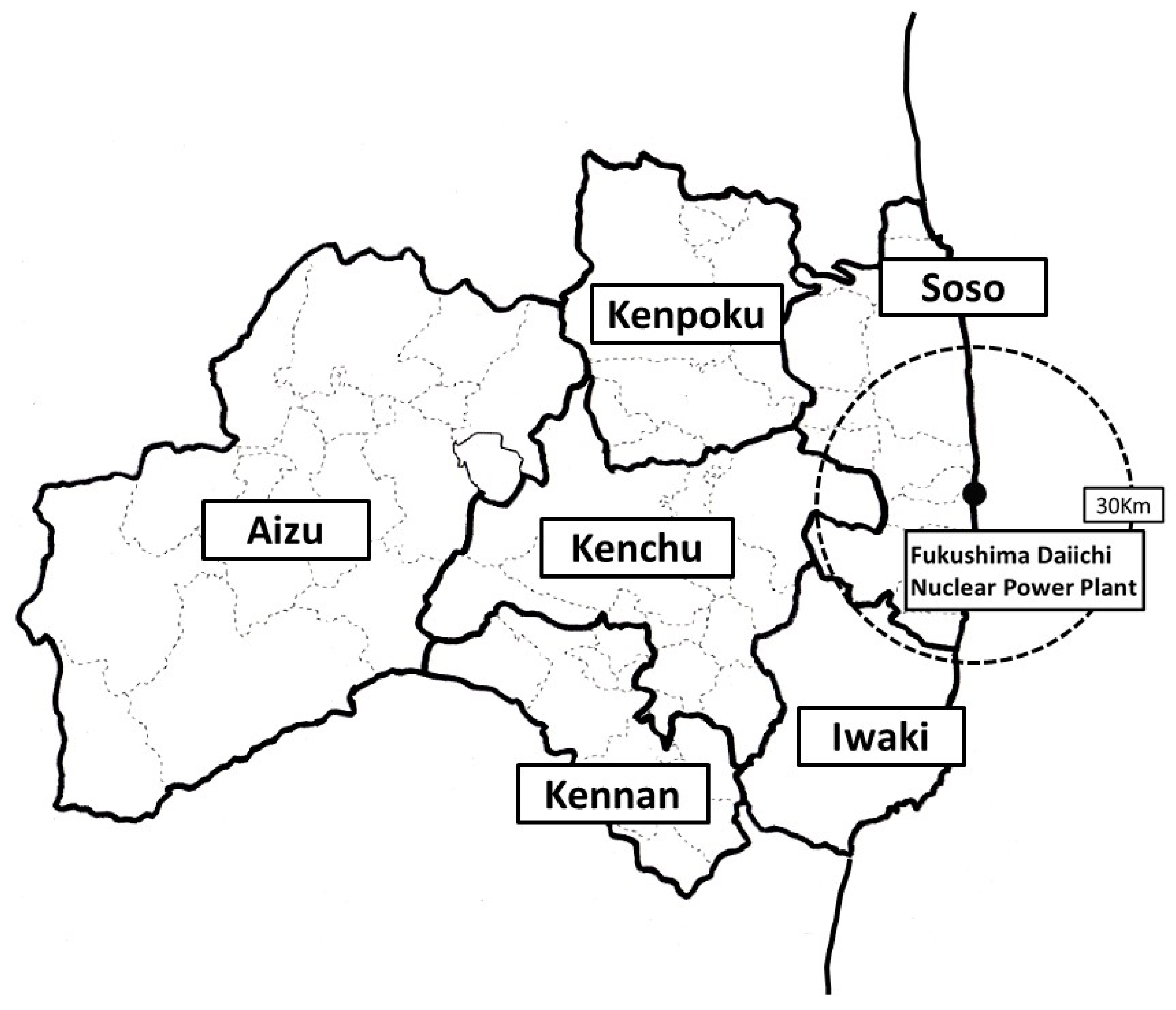
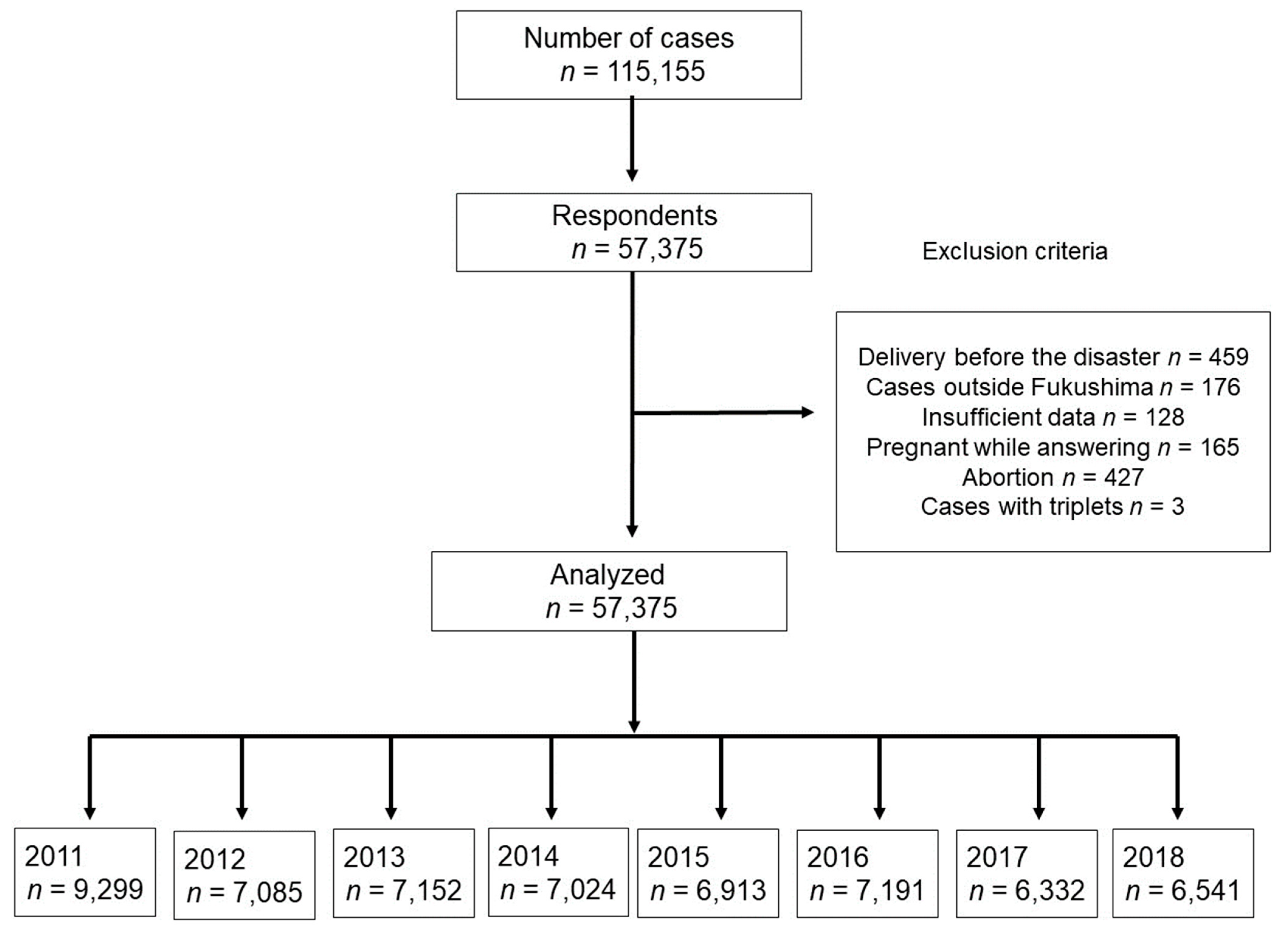
2.1. Study Design
2.2. Maternal Information and Obstetrics Outcome
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Disaster in Fukushima and Preterm Birth or LBW
4.2. Congenital Anomalies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K.; Fukushima Health Management Survey Group. Study protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Harville, E.; Xiong, X.; Buekens, P. Disasters and perinatal health: A systematic review. Obstet. Gynecol. Surv. 2010, 65, 713–728. [Google Scholar] [CrossRef] [PubMed]
- Fujimori, K.; Kyozuka, H.; Yasuda, S.; Goto, A.; Yasumura, S.; Ota, M.; Ohtsuru, A.; Nomura, Y.; Hata, K.; Suzuki, K.; et al. Pregnancy and birth survey after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant accident in Fukushima Prefecture. Fukushima J. Med. Sci. 2014, 60, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Kyozuka, H.; Yasuda, S.; Kawamura, M.; Nomura, Y.; Fujimori, K.; Goto, A.; Yasumura, S.; Abe, M. Impact of the Great East Japan Earthquake on feeding methods and newborn growth at 1 month postpartum: Results from the Fukushima Health Management Survey. Radiat. Environ. Biophys. 2016, 55, 139–146. [Google Scholar] [CrossRef]
- Yasuda, S.; Kyozuka, H.; Nomura, Y.; Fujimori, K.; Goto, A.; Yasumura, S.; Hata, K.; Ohira, T.; Abe, M. Influence of the Great East Japan Earthquake and the Fukushima Daiichi nuclear disaster on the birth weight of newborns in Fukushima Prefecture: Fukushima Health Management Survey. J. Matern. Fetal Neonatal Med. 2017, 30, 2900–2904. [Google Scholar] [CrossRef] [PubMed]
- Kyozuka, H.; Fujimori, K.; Hosoya, M.; Yasumura, S.; Yokoyama, T.; Sato, A.; Hashimoto, K. The Japan environment and children’s study (JECS) in Fukushima Prefecture: Pregnancy outcome after the great east Japan earthquake. Tohoku J. Exp. Med. 2018, 246, 27–33. [Google Scholar] [CrossRef]
- Kyozuka, H.; Murata, T.; Yasuda, S.; Fujimori, K.; Goto, A.; Yasumura, S.; Abe, M.; Pregnancy and Birth Survey Group of the Fukushima Health Management Survey. The effect of the Great East Japan Earthquake on hypertensive disorders during pregnancy: A study from the Fukushima Health Management Survey. J. Matern. Fetal Neonatal Med. 2020, 33, 4043–4048. [Google Scholar] [CrossRef]
- Cordero, J.F. The epidemiology of disasters and adverse reproductive outcomes: Lessons learned. Environ. Health Perspect. 1993, 101 (Suppl. S2), 131–136. [Google Scholar] [CrossRef]
- Goldman, L.R.; Paigen, B.; Magnant, M.M.; Highland, J.H. Low birth weight, prematurity and birth defects in children living near the hazardous waste site, love Canal. Hazard Waste Hazard Mater. 1985, 2, 209–223. [Google Scholar] [CrossRef]
- Levi, R.; Lundberg, U.; Hanson, U.; Frankenhacuser, M. Anxiety during pregnancy after the Chernobyl accident as related to obstetric outcome. J. Psychosom. Obstet. Gynecol. 1989, 10, 221–230. [Google Scholar] [CrossRef]
- Tan, C.E.; Li, H.J.; Zhang, X.G.; Zhang, H.; Han, P.Y.; An, Q.; Ding, W.J.; Wang, M.Q. The impact of the Wenchuan earthquake on birth outcomes. PLoS ONE 2009, 4, e8200. [Google Scholar] [CrossRef] [PubMed]
- Kyozuka, H.; Fujimori, K.; Hosoya, M.; Yasumura, S.; Yokoyama, T.; Sato, A.; Hashimoto, K. The effect of maternal age at the first childbirth on gestational age and birth weight: The Japan environment and children’s study (JECS). J. Epidemiol. 2019, 29, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Kyozuka, H.; Yamaguchi, A.; Suzuki, D.; Fujimori, K.; Hosoya, M.; Yasumura, S.; Yokoyama, T.; Sato, A.; Hashimoto, K.; Japan Environment and Children’s Study (JECS) Group. Risk factors for placenta accreta spectrum: Findings from the Japan environment and children’s study. BMC Preg. Childbirth 2019, 27, 447. [Google Scholar] [CrossRef]
- Yamaguchi, A.; Kyozuka, H.; Fujimori, K.; Hosoya, M.; Yasumura, S.; Yokoyama, T.; Sato, A.; Hashimoto, K.; Japan Environment and Children’s Study Group. Risk of preterm birth, low birthweight and small-for-gestational-age infants in pregnancies with adenomyosis: A cohort study of the Japan Environment and children’s Study. Acta Obstet. Gynecol. Scand. 2019, 98, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, M.; Fujimori, K.; Yasumura, S.; Goto, A.; Nakai, A. Obstetric outcomes in women in Fukushima Prefecture during and after the Great East Japan Earthquake and Fukushima Nuclear Power Plant Accident: The Fukushima Health Management Survey. Open J. Obstet. Gynecol. 2016, 6, 705–713. [Google Scholar] [CrossRef]
- Goto, A.; Bromet, E.J.; Fujimori, K.; Pregnancy and Birth Survey Group of Fukushima Health Management Survey. Immediate effects of the Fukushima nuclear power plant disaster on depressive symptoms among mothers with infants: A prefectural-wide cross-sectional study from the Fukushima Health Management Survey. BMC Psychiatry 2015, 15, 59. [Google Scholar] [CrossRef]
- Suzuki, K.; Goto, A.; Fujimori, K. Effect of medical institution change on gestational duration after the Great East Japan Earthquake: The Fukushima Health Management Survey. J. Obstet. Gynaecol. Res. 2016, 42, 1704–1711. [Google Scholar] [CrossRef]
- Chang, H.L.; Chang, T.C.; Lin, T.Y.; Kuo, S.S. Psychiatric morbidity and pregnancy outcome in a disaster area of Taiwan 921 earthquake. Psychiatry Clin. Neurosci. 2002, 56, 139–144. [Google Scholar] [CrossRef]
- Xiong, X.; Harville, E.W.; Mattison, D.R.; Elkind-Hirsch, K.; Pridjian, G.; Buekens, P. Exposure to Hurricane Katrina, post-traumatic stress disorder and birth outcomes. Am. J. Med. Sci. 2008, 336, 111–115. [Google Scholar] [CrossRef]
- Tong, V.T.; Zotti, M.E.; Hsia, J. Impact of the Red River catastrophic flood on women giving birth in North Dakota, 1994–2000. Matern. Child Health J. 2011, 15, 281–288. [Google Scholar] [CrossRef]
- Hamilton, B.E.; Sutton, P.D.; Mathews, T.J.; Martin, J.A.; Ventura, S.J. The effect of Hurricane Katrina: Births in the U.S. Gulf Coast region, before and after the storm. Natl. Vital Stat. Rep. 2009, 58, 1–32. [Google Scholar]
- Leppold, C.; Nomura, S.; Sawano, T.; Ozaki, A.; Tsubokura, M.; Hill, S.; Kanazawa, Y.; Anbe, H. Birth outcomes after the Fukushima Daiichi nuclear power plant disaster: A long-term retrospective study. Int. J. Environ. Res. Public Health 2017, 14, 542. [Google Scholar] [CrossRef]
- Wertelecki, W. Malformations in a Chornobyl-impacted region. Pediatrics 2010, 125, e836–e843. [Google Scholar] [CrossRef] [PubMed]
- Wertelecki, W.; Chambers, C.D.; Yevtushok, L.; Zymak-Zakutnya, N.; Sosyniuk, Z.; Lapchenko, S.; Ievtushok, B.; Akhmedzhanova, D.; Komov, O. Chornobyl 30 years later: Radiation, pregnancies, and developmental anomalies in Rivne, Ukraine. Eur. J. Med. Genet. 2017, 60, 2–11. [Google Scholar] [CrossRef]
- Wertelecki, W.; Yevtushok, L.; Kuznietsov, I.; Komov, O.; Lapchenko, S.; Akhmedzanova, D.; Ostapchuk, L. Chornobyl, radiation, neural tube defects, and microcephaly. Eur. J. Med. Genet. 2018, 61, 556–563. [Google Scholar] [CrossRef]
- Dolk, H.; Nichols, R. Evaluation of the impact of Chernobyl on the prevalence of congenital anomalies in 16 regions of Europe. EUROCAT Working Group. Int. J. Epidemiol. 1999, 28, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, W. Fallout from the Chernobyl nuclear disaster and congenital malformations in Europe. Arch. Environ. Health 2001, 56, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Little, J. The Chernobyl accident, congenital anomalies and other reproductive outcomes. Paediatr. Perinat. Epidemiol. 1993, 7, 121–151. [Google Scholar] [CrossRef] [PubMed]
- Cragan, J.D.; Gilboa, S.M. Including prenatal diagnoses in birth defects monitoring: Experience of the Metropolitan Atlanta Congenital Defects Program. Birth Defects Res. A Clin. Mol. Teratol. 2009, 85, 20–29. [Google Scholar] [CrossRef]
- Dolk, H.; Loane, M.; Garne, E. The prevalence of congenital anomalies in Europe. Adv. Exp. Med. Biol. 2010, 686, 349–364. [Google Scholar] [CrossRef]
- ICBDSR (International Clearinghouse for Birth Defects Surveillance and Research) Japan Center. Available online: https://icbdsr-j.jp/data.html (accessed on 13 July 2020). (In Japanese).
- Gurney, J.K.; McGlynn, K.A.; Stanley, J.; Merriman, T.; Signal, V.; Shaw, C.; Edwards, R.; Richiardi, L.; Hutson, J.; Sarfati, D. Risk factors for cryptorchidism. Nat. Rev. Urol. 2017, 14, 534–548. [Google Scholar] [CrossRef] [PubMed]
- Kojima, Y.; Yokoya, S.; Kurita, N.; Idaka, T.; Ishikawa, T.; Tanaka, H.; Ezawa, Y.; Ohto, H. Cryptorchidism after the Fukushima Daiichi Nuclear Power Plant accident:causation or coincidence? Fukushima J. Med. Sci. 2019, 65, 76–98. [Google Scholar] [CrossRef] [PubMed]
- Hirata, Y.; Shimizu, H.; Kumamaru, H.; Takamoto, S.; Motomura, N.; Miyata, H.; Okita, Y. Congenital heart disease After the Fukushima nuclear accident: The Japan cardiovascular surgery database study. J. Am. Heart Assoc. 2020, 9, e014787. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p-Value † | |
|---|---|---|---|---|---|---|---|---|---|
| Response rate | |||||||||
| All of Fukushima, % | 58.2 | 49.1 | 47.3 | 46.8 | 47.8 | 51.3 | 47.1 | 51.4 | <0.001 |
| (Res/Send) | (9299/15,972) | (7085/14,420) | (7152/15,108) | (7024/15,017) | (6913/14,454) | (7191/14,019) | (6332/13,435) | (6541/12,730) | |
| Kenpoku, % | 62.8 * | 55.5 * | 53.2 * | 52.4 * | 52.3 * | 55.9 * | 50.9 * | 56.5 * | <0.001 |
| (Res/Send) | (2289/3647) | (1857/3347) | (1936/3637) | (1841/3515) | (1806/3453) | (1875/3352) | (1634/3212) | (1702/3015) | |
| Kenchu, % | 59.3 | 48.7 | 44.5 * | 44.8 * | 45.2 * | 49.8 ** | 46.8 | 51.1 | <0.001 |
| (Res/Send) | (2858/4819) | (2067/4243) | (1982/4453) | (1961/4376) | (1924/4261) | (2065/4150) | (1862/3980) | (2006/3923) | |
| Kennan, % | 50.2 * | 48.1 | 48.5 | 46.5 | 47.9 | 51.1 | 45.1 | 50.0 | 0.652 |
| (Res/Send) | (631/1256) | (560/1164) | (588/1213) | (553/1188) | (560/1168) | (571/1118) | (473/1048) | (504/1008) | |
| Soso, % | 65.6 † | 43.7 * | 45.4 | 42.2 * | 44.2 * | 43.6 * | 40.5 * | 42.3 * | <0.001 |
| (Res/Send) | (963/1468) | (500/1145) | (535/1178) | (512/1213) | (523/1183) | (511/1171) | (442/1091) | (424/1003) | |
| Iwaki, % | 55.9 * | 47.8 | 45.1 ** | 45.8 | 46.6 | 50.1 | 45.5 | 49.1 ** | <0.001 |
| (Res/Send) | (1515/2711) | (1203/2516) | (1195/2649) | (1213/2648) | (1148/2461) | (1192/2377) | (1054/2317) | (1034/2105) | |
| Aizu, % | 50.4 * | 44.8 * | 46.3 | 45.5 | 49.4 | 52.8 | 48.5 | 52.0 | 0.001 |
| (Res/Send) | (1043/2071) | (898/2005) | (916/1978) | (944/2077) | (952/1928) | (977/1851) | (867/1787) | (871/1676) | |
| p-value ‡ | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Maternal age, mean ± SD | 30.7 ± 5.0 | 31.0 ± 5.0 | 31.3 ± 5.0 | 31.4 ± 5.1 | 31.6 ± 5.0 | 31.4 ± 5.0 | 31.6 ± 5.0 | 31.8 ± 5.0 | <0.001 § |
| n | 8598 | 6940 | 7044 | 6940 | 6815 | 7091 | 6288 | 6463 | |
| Twin pregnancy, % | 0.9 | 0.9 | 1,1 | 1.0 | 0.9 | 0.8 | 0.8 | 0.9 | 0.368 ‡ |
| Gestational week, mean ± SD | 38.9 ± 1.7 | 38.9 ± 1.7 | 38.9 ± 1.7 | 38.9 ± 1.8 | 38.8 ± 1.8 | 38.9 ± 1.7 | 38.8 ± 1.7 | 38.8 ± 1.8 | <0.001 § |
| n | 8566 | 6926 | 7015 | 6930 | 6801 | 7086 | 6286 | 6453 | |
| Neonatal weight, mean ± SD | 3013 ± 418 | 2993 ± 435 | 3003 ± 435 | 2996 ± 455 | 2994 ± 445 | 2999 ± 432 | 3007 ± 432 | 3003 ± 438 | 0.912 § |
| n | 8603 | 6935 | 7088 | 6999 | 6859 | 7122 | 6319 | 6504 | |
| Mode of pregnancy | |||||||||
| Sterility treatment, % | 4.3 | 5.4 | 6.0 | 6.6 | 6.9 | 7.9 | 8.0 | 8.4 | <0.001 ‡ |
| Sex of newborn | |||||||||
| male, % | 51.4 | 52.5 | 50.4 | 51.3 | 50.1 | 50.3 | 50.7 | 50.8 | 0.046 ‡ |
| Stillbirth, % | 0.25 | 0.29 | 0.34 | 0.21 | 0.25 | 0.21† | 0.22 † | 0.18 † | 0.690 ‡ |
| Mode of delivery | |||||||||
| cesarean delivery, % | 20.7 | 21.7 | 20.3 | 21.0 | 22.3 | 21.2 | 21.8 | 22.6 | 0.005 ‡ |
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p-Value † | |
|---|---|---|---|---|---|---|---|---|---|
| All of Fukushima, n (%) | 395 (4.6) | 393 (5.6) | 373 (5.3) | 375 (5.4) | 386 (5.6) | 380 (5.3) | 335 (5.3) | 341 (5.2) | 0.197 |
| Kenpoku, n (%) | 91 (4.3) | 82 (4.5) * | 94 (4.9) | 96 (5.2) | 105 (5.9) | 91 (4.9) | 72 (4.4) | 89 (5.3) | 0.247 |
| Kenchu, n (%) | 114 (4.3) | 127 (6.2) | 95 (4.8) | 107 (5.5) | 119 (6.2) | 103 (5.0) | 103 (5.6) | 108 (5.4) | 0.254 |
| Kennan, n (%) | 28 (4.7) | 23 (4.1) | 33 (5.7) | 25 (4.6) | 34 (6.1) | 30 (5.3) | 27 (5.7) | 29 (5.8) | 0.197 |
| Soso, n (%) | 38 (4.3) | 31 (6.5) | 35 (6.6) | 31 (6.1) | 30 (5.8) | 29 (5.7) | 21 (4.8) | 9 (2.2) | 0.207 |
| Iwaki, n (%) | 71 (5.1) | 65 (5.5) | 69 (5.9) | 72 (5.9) | 46 (4.1) | 63 (5.3) | 62 (5.9) | 56 (5.5) | 0.886 |
| Aizu, n (%) | 53 (5.4) | 65 (7.3) * | 47 (5.2) | 44 (4.7) | 52 (5.5) | 64 (6.6) | 50 (5.8) | 50 (5.7) | 0.962 |
| p-value ‡ | 0.633 | 0.020 | 0.501 | 0.718 | 0.215 | 0.498 | 0.481 | 0.111 |
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p-Value † | |
|---|---|---|---|---|---|---|---|---|---|
| All of Fukushima, n (%) | 736 (8.6) | 640 (9.3) | 681 (9.6) | 683 (9.8) | 650 (9.5) | 659 (9.3) | 584 (9.3) | 589 (9.1) | 0.500 |
| Kenpoku, n (%) | 160 (7.6) ** | 138 (7.6) * | 171 (8.9) | 168 (9.2) | 155 (8.7) | 151 (8.1) | 155 (9.5) | 145 (8.6) | 0.107 |
| Kenchu, n (%) | 217 (8.3) | 208 (10.3) | 191 (9.7) | 192 (9.8) | 208 (10.9) | 187 (9.2) | 166 (9.0) | 180 (9.0) | 0.908 |
| Kennan, n (%) | 47 (8.0) | 51 (9.2) | 58 (9.9) | 49 (9.1) | 54 (9.8) | 56 (9.9) | 38 (8.1) | 46 (9.3) | 0.756 |
| Soso, n (%) | 70 (7.9) | 43 (9.3) | 47 (8.9) | 57 (11.3) | 56 (10.9) | 46 (9.1) | 50 (11.3) | 34 (8.2) | 0.254 |
| Iwaki, n (%) | 143 (10.3) * | 101 (8.6) | 120 (10.3) | 119 (9.8) | 99 (8.7) | 118 (10.0) | 98 (9.3) | 99 (9.7) | 0.759 |
| Aizu, n (%) | 99 (10.2) | 99 (11.3) ** | 94 (10.4) | 98 (10.4) | 78 (8.4) | 101 (10.4) | 77 (8.9) | 85 (9.7) | 0.210 |
| p-value ‡ | 0.031 | 0.025 | 0.761 | 0.736 | 0.099 | 0.349 | 0.638 | 0.867 |
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p-Value † | |
|---|---|---|---|---|---|---|---|---|---|
| All of Fukushima, n (%) | 238 (2.85) | 161 (2.35) | 170 (2.44) | 163 (2.36) | 150 (2.21) | 176 (2.49) | 153 (2.44) | 144 (2.23) | 0.069 |
| Kenpoku, n (%) | 55 (2.66) | 39 (2.17) | 44 (2.32) | 54 (2.99) | 31 (1.75) | 41 (2.22) | 40 (2.47) | 41 (2.45) | 0.684 |
| Kenchu, n (%) | 78 (3.07) | 49 (2.43) | 50 (2.60) | 49 (2.54) | 48 (2.54) | 57 (2.81) | 34 (1.85) | 36 (1.82) | 0.011 |
| Kennan, n (%) | 24 (4.20) | 13 (2.39) | 9 (1.56) | 11 (2.04) | 18 (3.26) | 12 (2.14) | 9 (1.92) | 10 (2.01) | 0.088 |
| Soso, n (%) | 18 (2.09) | 13 (2.86) | 9 (1.75) | 9 (1.79) | 7 (1.36) | 13 (2.60) | 8 (1.82) | 12 (2.88) | 0.800 |
| Iwaki, n (%) | 38 (2.81) | 26 (2.23) | 35 (3.04) | 22 (1.83) | 27 (2.41) | 26 (2.24) | 33 (3.15) | 22 (2.15) | 0.694 |
| Aizu, n (%) | 25 (2.63) | 21 (2.40) | 23 (2.58) | 18 (1.93) | 19 (2.04) | 27 (2.80) | 29 (3.36) | 23 (2.67) | 0.408 |
| p-value ‡ | 0.268 | 0.970 | 0.411 | 0.261 | 0.181 | 0.787 | 0.099 | 0.607 |
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | p-Value † | |
|---|---|---|---|---|---|---|---|---|---|
| All anomalies | 238/8345 | 161/6858 | 170/6954 | 163/6915 | 150/6790 | 176/7064 | 153/6278 | 144/6455 | 0.069 |
| % | 2.85% | 2.35% | 2.44% | 2.36% | 2.21% | 2.49% | 2.44% | 2.23% | |
| Cataract | 1 | 2 | 1 | 0 | 0 | 1 | 1 | 1 | 0.743 |
| % | 0.01% | 0.03% | 0.01% | 0.00% | 0.00% | 0.01% | 0.02% | 0.03% | |
| Cardiac malformation | 77 | 54 | 70 | 53 | 53 | 66 | 38 | 60 | 0.445 |
| % | 0.92% | 0.79% | 1.01% | 0.77% | 0.78% | 0.93% | 0.61% | 0.93% | |
| Kidney/urinary tract malformation | 22 | 14 | 12 | 24 | 14 | 16 | 25 | 14 | 0.451 |
| % | 0.26% | 0.20% | 0.17% | 0.35% | 0.21% | 0.23% | 0.40% | 0.22% | |
| Spina bifida | 5 | 5 | 3 | 5 | 4 | 3 | 4 | 3 | 0.678 |
| % | 0.06% | 0.07% | 0.04% | 0.07% | 0.06% | 0.04% | 0.06% | 0.05% | |
| Microcephaly | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0.129 |
| % | 0.01% | 0.01% | 0.00% | 0.01% | 0.00% | 0.00% | 0.00% | 0.00% | |
| Hydrocephalus | 1 | 3 | 4 | 2 | 1 | 2 | 1 | 1 | 0.478 |
| % | 0.01% | 0.04% | 0.06% | 0.03% | 0.01% | 0.03% | 0.02% | 0.02% | |
| Cleft lip/palate | 17 | 14 | 14 | 14 | 14 | 11 | 8 | 7 | 0.079 |
| % | 0.20% | 0.20% | 0.20% | 0.20% | 0.21% | 0.16% | 0.13% | 0.11% | |
| Intestinal atresia | 6 | 7 | 7 | 9 | 4 | 10 | 7 | 5 | 0.710 |
| % | 0.07% | 0.10% | 0.10% | 0.13% | 0.06% | 0.14% | 0.11% | 0.08% | |
| Imperforate anus | 4 | 2 | 2 | 5 | 2 | 2 | 3 | 4 | 0.695 |
| % | 0.05% | 0.03% | 0.03% | 0.07% | 0.03% | 0.03% | 0.05% | 0.06% | |
| Poly/syndactylism | 22 | 15 | 22 | 14 | 14 | 18 | 16 | 13 | 0.554 |
| % | 0.26% | 0.22% | 0.32% | 0.20% | 0.21% | 0.25% | 0.25% | 0.20% | |
| Others | 104 | 61 | 55 | 63 | 58 | 64 | 59 | 54 | 0.070 |
| % | 1.25% | 0.89% | 0.79% | 0.91% | 0.85% | 0.91% | 0.94% | 0.84% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyozuka, H.; Ohhira, T.; Murata, T.; Yasuda, S.; Ishii, K.; Yasumura, S.; Fujimori, K.; Ohto, H.; Kamiya, K., on behalf of the Pregnancy and Birth Survey Group of the Fukushima Health Management Survey. Eight-Year Trends in the Effect of the Great East Japan Earthquake on Obstetrics Outcomes: A Study from the Fukushima Health Management Survey. Life 2023, 13, 1702. https://doi.org/10.3390/life13081702
Kyozuka H, Ohhira T, Murata T, Yasuda S, Ishii K, Yasumura S, Fujimori K, Ohto H, Kamiya K on behalf of the Pregnancy and Birth Survey Group of the Fukushima Health Management Survey. Eight-Year Trends in the Effect of the Great East Japan Earthquake on Obstetrics Outcomes: A Study from the Fukushima Health Management Survey. Life. 2023; 13(8):1702. https://doi.org/10.3390/life13081702
Chicago/Turabian StyleKyozuka, Hyo, Tetsuya Ohhira, Tsuyoshi Murata, Shun Yasuda, Kayoko Ishii, Seiji Yasumura, Keiya Fujimori, Hitoshi Ohto, and Kenji Kamiya on behalf of the Pregnancy and Birth Survey Group of the Fukushima Health Management Survey. 2023. "Eight-Year Trends in the Effect of the Great East Japan Earthquake on Obstetrics Outcomes: A Study from the Fukushima Health Management Survey" Life 13, no. 8: 1702. https://doi.org/10.3390/life13081702
APA StyleKyozuka, H., Ohhira, T., Murata, T., Yasuda, S., Ishii, K., Yasumura, S., Fujimori, K., Ohto, H., & Kamiya, K., on behalf of the Pregnancy and Birth Survey Group of the Fukushima Health Management Survey. (2023). Eight-Year Trends in the Effect of the Great East Japan Earthquake on Obstetrics Outcomes: A Study from the Fukushima Health Management Survey. Life, 13(8), 1702. https://doi.org/10.3390/life13081702