
Impact of Diabetes Duration on Clinical Outcome in Patients Receiving Rotational Atherectomy in Calcified Lesions in Korea—Results from ROCK Registry

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
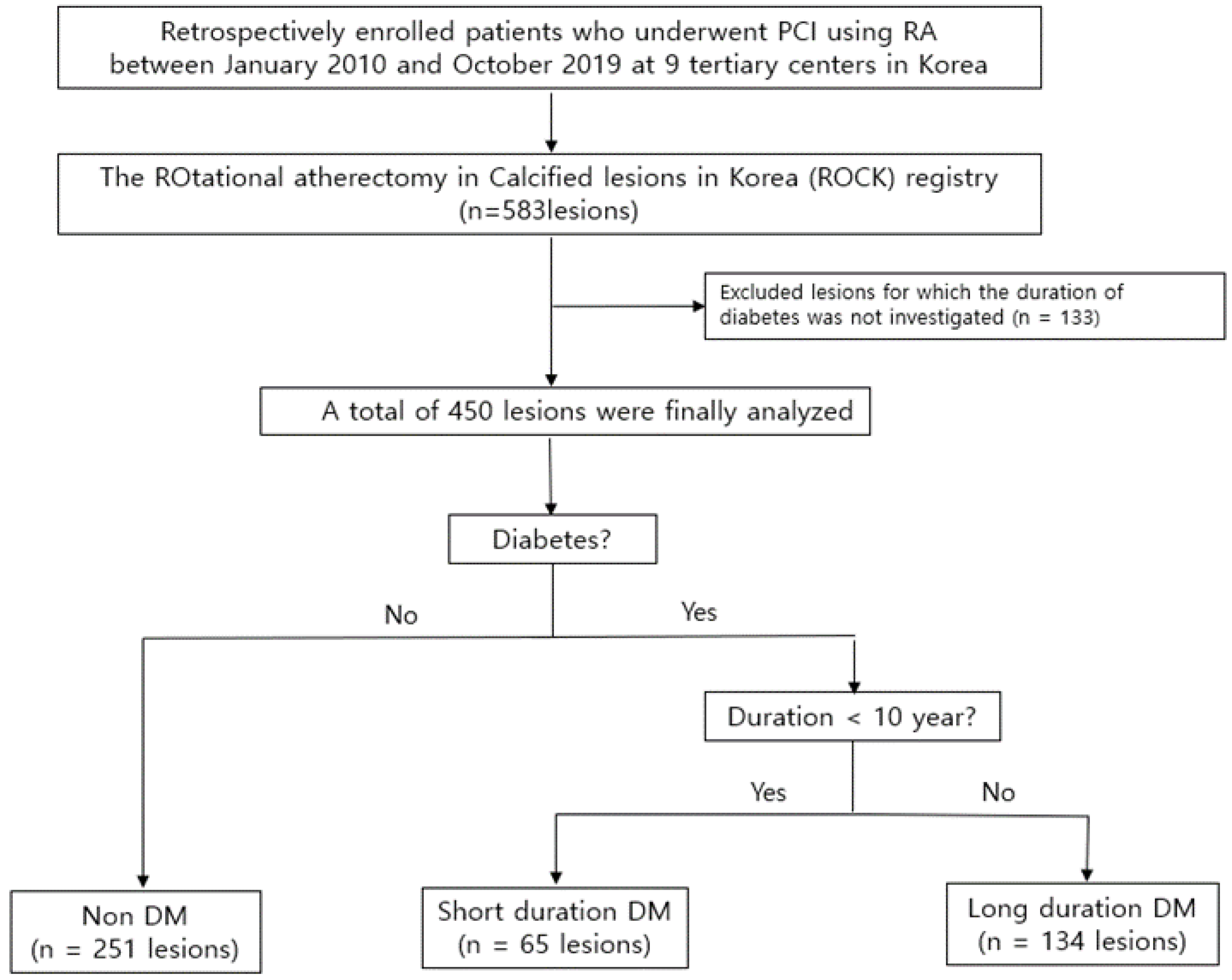
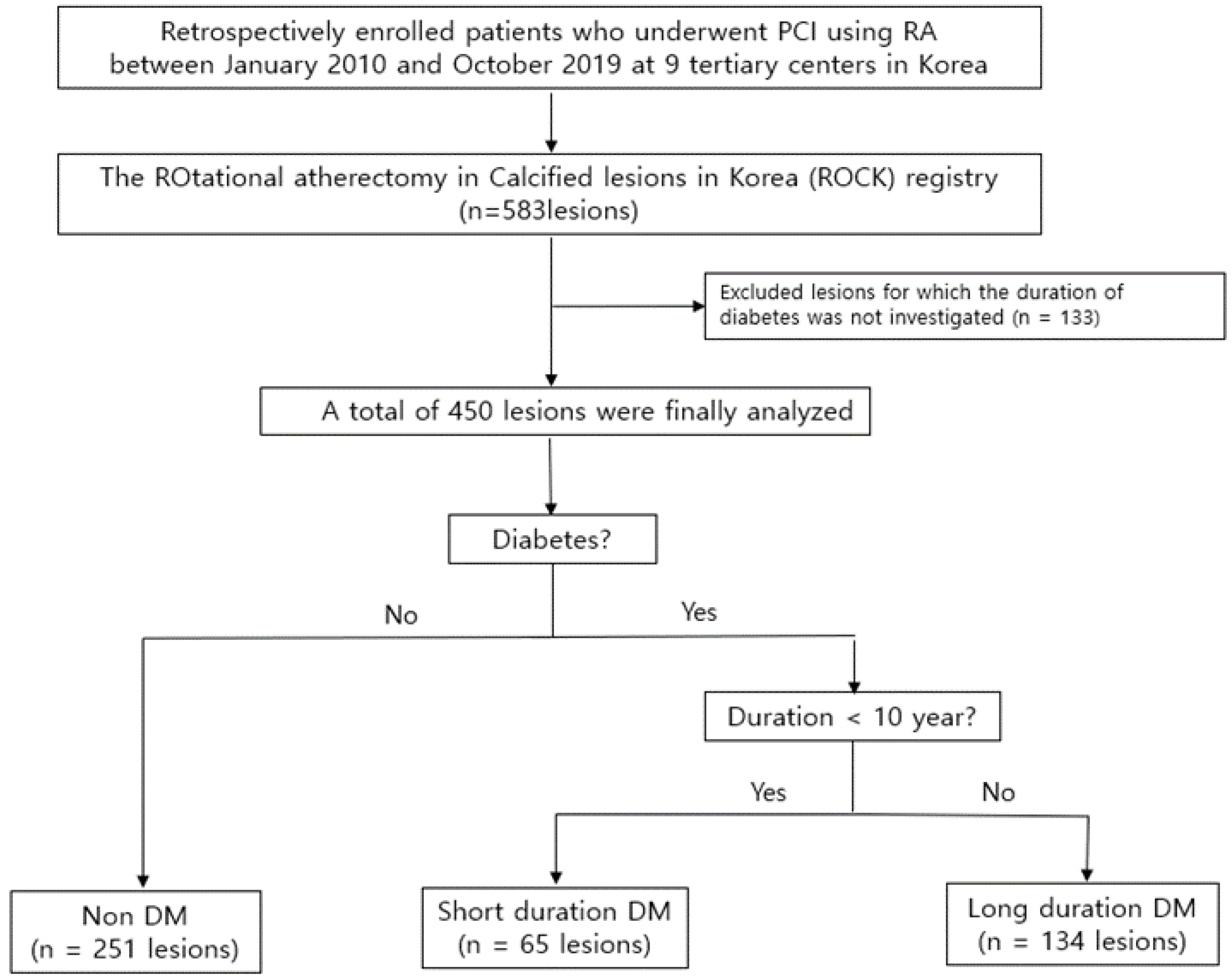
2.1. Study Design and Population
2.2. RA Procedure
2.3. Clinical Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Procedural Details, In-Hospital Events, and Procedure Complications
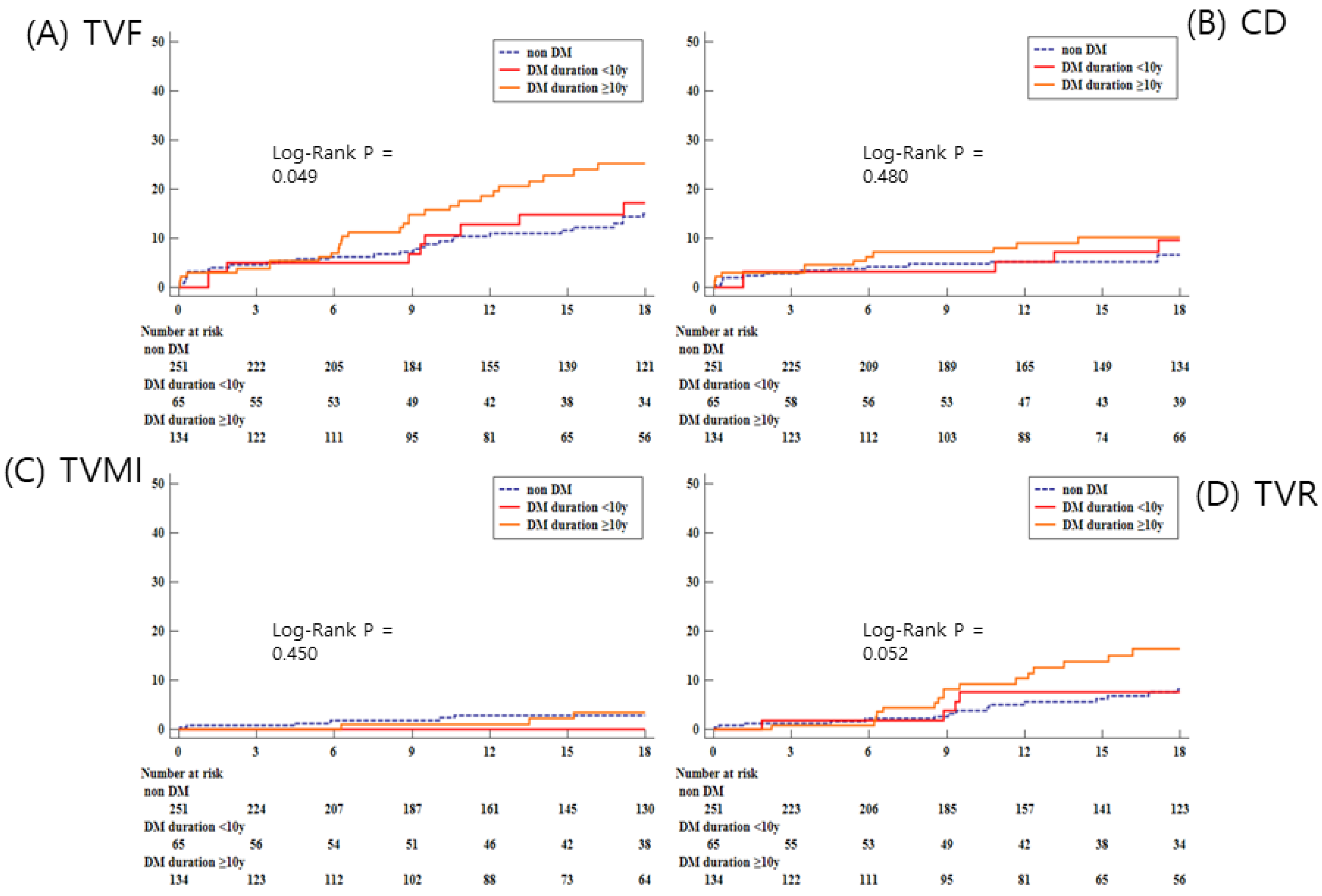
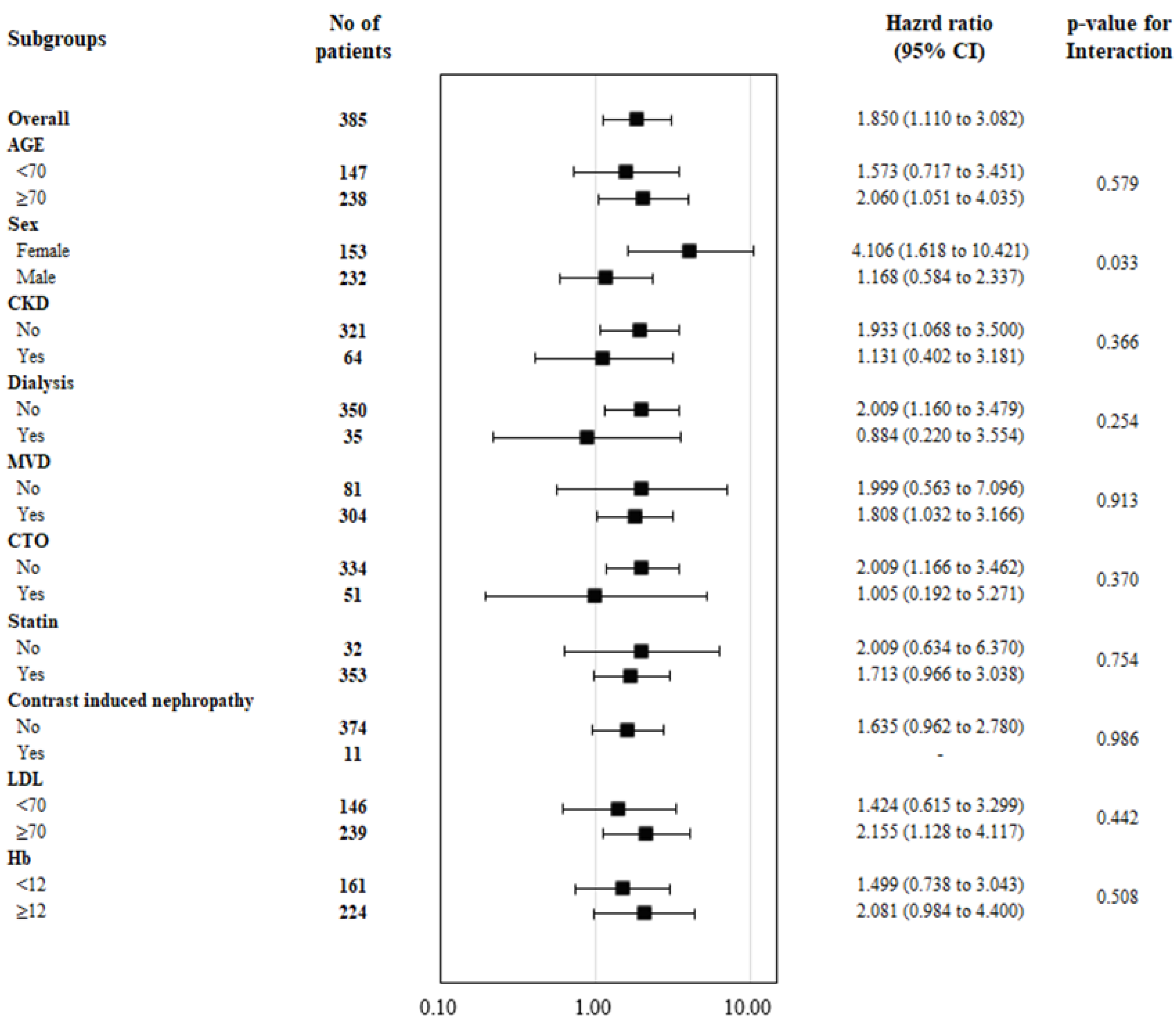
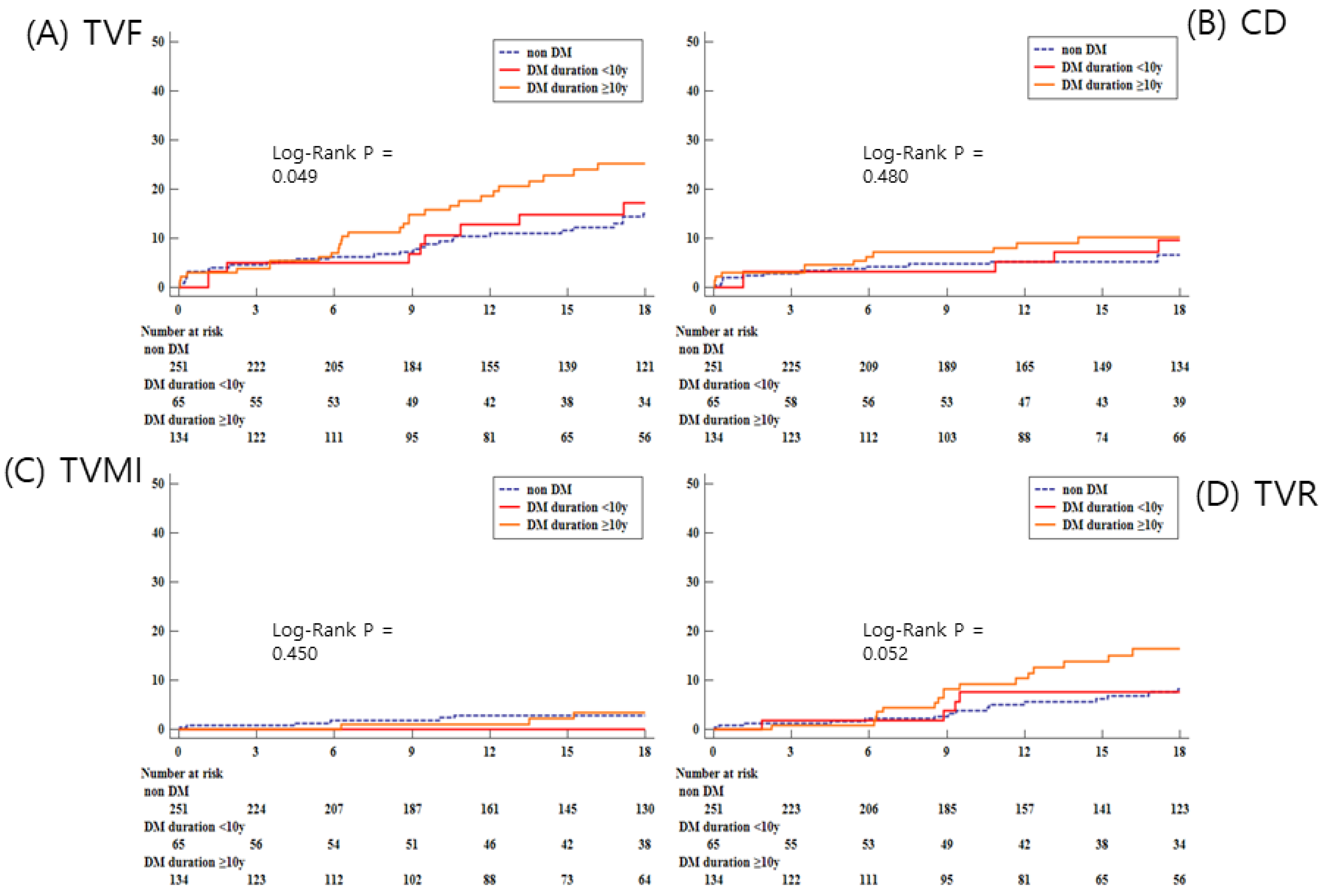
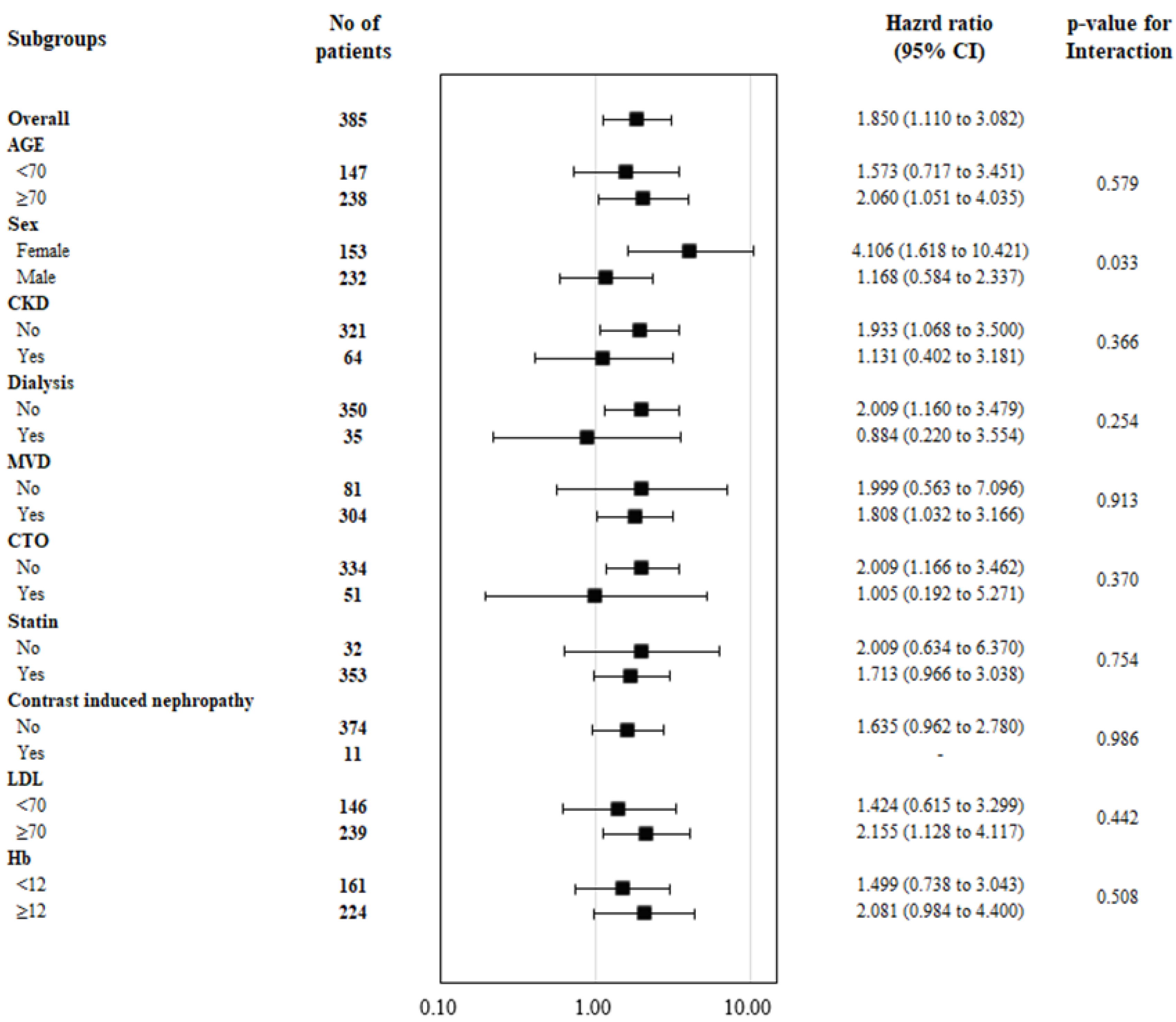
3.3. Mid-Term Clinical Outcomes
4. Discussion
5. Study Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pasterkamp, G. Methods of accelerated atherosclerosis in diabetic patients. Heart 2013, 99, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Tuzcu, E.M.; Kalidindi, S.; Wolski, K.; Moon, K.W.; Sipahi, I.; Schoenhagen, P.; Nissen, S.E. Effect of diabetes on progression of coronary atherosclerosis and arterial remodeling: A pooled analysis of 5 intravascular ultrasound trials. J. Am. Coll. Cardiol. 2008, 52, 255–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abaci, A.; Oguzhan, A.; Kahraman, S.; Eryol, N.K.; Unal, S.; Arinc, H.; Ergin, A. Effect of diabetes mellitus on formation of coronary collateral vessels. Circulation 1999, 99, 2239–2242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elezi, S.; Kastrati, A.; Pache, J.; Wehinger, A.; Hadamitzky, M.; Dirschinger, J.; Neumann, F.J.; Schomig, A. Diabetes mellitus and the clinical and angiographic outcome after coronary stent placement. J. Am. Coll. Cardiol. 1998, 32, 1866–1873. [Google Scholar] [CrossRef] [Green Version]
- Von Birgelen, C.; Kok, M.M.; Sattar, N.; Zocca, P.; Doelman, C.; Kant, G.D.; Lowik, M.M.; van der Heijden, L.C.; Sen, H.; van Houwelingen, K.G.; et al. “Silent” Diabetes and Clinical Outcome After Treatment with Contemporary Drug-Eluting Stents: The BIO-RESORT Silent Diabetes Study. JACC Cardiovasc. Interv. 2018, 11, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Ahn, J.M.; Yoon, Y.H.; Kang, D.Y.; Park, S.Y.; Ko, E.; Park, H.; Cho, S.C.; Park, S.; Kim, T.O.; et al. Long-Term (10-Year) Outcomes of Stenting or Bypass Surgery for Left Main Coronary Artery Disease in Patients With and Without Diabetes Mellitus. J. Am. Heart Assoc. 2020, 9, e015372. [Google Scholar] [CrossRef]
- Viigimaa, M.; Sachinidis, A.; Toumpourleka, M.; Koutsampasopoulos, K.; Alliksoo, S.; Titma, T. Macrovascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 110–116. [Google Scholar] [CrossRef]
- Fox, C.S.; Sullivan, L.; D’Agostino, R.B., Sr.; Wilson, P.W.; Framingham Heart Study. The significant effect of diabetes duration on coronary heart disease mortality: The Framingham Heart Study. Diabetes Care 2004, 27, 704–708. [Google Scholar] [CrossRef] [Green Version]
- Silbernagel, G.; Rosinger, S.; Grammer, T.B.; Kleber, M.E.; Winkelmann, B.R.; Boehm, B.O.; Marz, W. Duration of type 2 diabetes strongly predicts all-cause and cardiovascular mortality in people referred for coronary angiography. Atherosclerosis 2012, 221, 551–557. [Google Scholar] [CrossRef]
- Venuraju, S.M.; Lahiri, A.; Jeevarethinam, A.; Cohen, M.; Darko, D.; Nair, D.; Rosenthal, M.; Rakhit, R.D. Duration of type 2 diabetes mellitus and systolic blood pressure as determinants of severity of coronary stenosis and adverse events in an asymptomatic diabetic population: PROCEED study. Cardiovasc. Diabetol. 2019, 18, 51. [Google Scholar] [CrossRef]
- Sohrabi, B.; Ghaffari, S.; Habibzadeh, A.; Chaichi, P. Outcome of diabetic and non-diabetic patients undergoing successful percutaneous coronary intervention of chronic total occlusion. J. Cardiovasc. Thorac. Res. 2011, 3, 45–48. [Google Scholar] [PubMed]
- Eftychiou, C.; Barmby, D.S.; Wilson, S.J.; Ubaid, S.; Markwick, A.J.; Makri, L.; Blaxill, J.M.; Spratt, J.C.; Gunning, M.; Greenwood, J.P. Cardiovascular Outcomes Following Rotational Atherectomy: A UK Multicentre Experience. Catheter. Cardiovasc. Interv. 2016, 88, 546–553. [Google Scholar] [CrossRef] [PubMed]
- White, M.G.; Shaw, J.A.; Taylor, R. Type 2 Diabetes: The Pathologic Basis of Reversible beta-Cell Dysfunction. Diabetes Care 2016, 39, 2080–2088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, I.M.; Adler, A.I.; Neil, H.A.; Matthews, D.R.; Manley, S.E.; Cull, C.A.; Hadden, D.; Turner, R.C.; Holman, R.R. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ 2000, 321, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Jung, J.H.; Lee, M.; Kim, D.W.; Park, M.W.; Choi, I.J.; Lee, J.H.; Lee, J.H.; Lee, S.R.; Lee, P.H.; et al. Clinical Outcome of Rotational Atherectomy in Calcified Lesions in Korea-ROCK Registry. Medicina 2021, 57, 694. [Google Scholar] [CrossRef]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33 (Suppl. 1), S62–S69. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Alfonso, F.; Fernandez, C. Second-generation drug-eluting stents. Moving the field forward. J. Am. Coll. Cardiol. 2011, 58, 26–29. [Google Scholar] [CrossRef] [Green Version]
- Writing Committee Members; Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar]
- Nanayakkara, N.; Ranasinha, S.; Gadowski, A.; Heritier, S.; Flack, J.R.; Wischer, N.; Wong, J.; Zoungas, S. Age, age at diagnosis and diabetes duration are all associated with vascular complications in type 2 diabetes. J. Diabetes Complicat. 2018, 32, 279–290. [Google Scholar] [CrossRef]
- Lindsey, J.B.; House, J.A.; Kennedy, K.F.; Marso, S.P. Diabetes duration is associated with increased thin-cap fibroatheroma detected by intravascular ultrasound with virtual histology. Circ. Cardiovasc. Interv. 2009, 2, 543–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, Z.; Zhou, P.; Liu, C.; Li, J.; Chen, R.; Zhou, J.; Song, L.; Zhao, H.; Yan, H. Relationships of coronary culprit-plaque characteristics with duration of diabetes mellitus in acute myocardial infarction: An intravascular optical coherence tomography study. Cardiovasc. Diabetol. 2019, 18, 136. [Google Scholar] [CrossRef] [PubMed]
- Yahagi, K.; Kolodgie, F.D.; Lutter, C.; Mori, H.; Romero, M.E.; Finn, A.V.; Virmani, R. Pathology of Human Coronary and Carotid Artery Atherosclerosis and Vascular Calcification in Diabetes Mellitus. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 191–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katakami, N. Mechanism of Development of Atherosclerosis and Cardiovascular Disease in Diabetes Mellitus. J. Atheroscler. Thromb. 2018, 25, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Borgharkar, S.S.; Das, S.S. Real-world evidence of glycemic control among patients with type 2 diabetes mellitus in India: The TIGHT study. BMJ Open Diabetes Res. Care 2019, 7, e000654. [Google Scholar] [CrossRef] [Green Version]
- Hemetsberger, R.; Abdelghani, M.; Toelg, R.; Mankerious, N.; Allali, A.; Garcia-Garcia, H.M.; Windecker, S.; Lefevre, T.; Saito, S.; Slagboom, T.; et al. Impact of Coronary Calcification on Clinical Outcomes After Implantation of Newer-Generation Drug-Eluting Stents. J. Am. Heart Assoc. 2021, 10, e019815. [Google Scholar] [CrossRef]
- Lee, M.S.; Yang, T.; Lasala, J.; Cox, D. Impact of coronary artery calcification in percutaneous coronary intervention with paclitaxel-eluting stents: Two-year clinical outcomes of paclitaxel-eluting stents in patients from the ARRIVE program. Catheter. Cardiovasc. Interv. 2016, 88, 891–897. [Google Scholar] [CrossRef]
- Genereux, P.; Madhavan, M.V.; Mintz, G.S.; Maehara, A.; Palmerini, T.; Lasalle, L.; Xu, K.; McAndrew, T.; Kirtane, A.; Lansky, A.J.; et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) TRIALS. J. Am. Coll. Cardiol. 2014, 63, 1845–1854. [Google Scholar]
- Chun, S.; Qiu, F.; Austin, P.C.; Ko, D.T.; Mamdani, M.; Wijeysundera, D.N.; Czarnecki, A.; Bennell, M.C.; Wijeysundera, H.C. Predictors and Outcomes of Routine Versus Optimal Medical Therapy in Stable Coronary Heart Disease. Am. J. Cardiol. 2015, 116, 671–677. [Google Scholar] [CrossRef]
- Mashaly, A.; Rha, S.W.; Choi, B.G.; Baek, M.J.; Ryu, Y.G.; Choi, S.Y.; Byun, J.K.; Li, H.; Shim, M.S.; Jang, W.Y.; et al. Impact of diabetes mellitus on 5-year clinical outcomes in patients with chronic total occlusion lesions. Coron. Artery Dis. 2018, 29, 119–126. [Google Scholar] [CrossRef]
- Johannsen, L.; Soldat, J.; Krueger, A.; Mahabadi, A.A.; Dykun, I.; Totzeck, M.; Janosi, R.A.; Rassaf, T.; Al-Rashid, F. Impact of Diabetes Mellitus on Outcomes after High-Risk Interventional Coronary Procedures. J. Clin. Med. 2020, 9, 3414. [Google Scholar] [CrossRef] [PubMed]
- Orchard, T.J.; Dorman, J.S.; Maser, R.E.; Becker, D.J.; Drash, A.L.; Ellis, D.; LaPorte, R.E.; Kuller, L.H. Prevalence of complications in IDDM by sex and duration. Pittsburgh Epidemiology of Diabetes Complications Study II. Diabetes 1990, 39, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Mann, J.F.; Pogue, J.; Dinneen, S.F.; Halle, J.P.; Hoogwerf, B.; Joyce, C.; Rashkow, A.; Young, J.; Zinman, B.; et al. Prevalence and determinants of microalbuminuria in high-risk diabetic and nondiabetic patients in the Heart Outcomes Prevention Evaluation Study. The HOPE Study Investigators. Diabetes Care 2000, 23 (Suppl. 2), B35–B39. [Google Scholar] [PubMed]
- Martin-Timon, I.; Sevillano-Collantes, C.; Segura-Galindo, A.; Del Canizo-Gomez, F.J. Type 2 diabetes and cardiovascular disease: Have all risk factors the same strength? World J. Diabetes 2014, 5, 444–470. [Google Scholar] [CrossRef]
- Tomizawa, N.; Fujino, Y.; Kamitani, M.; Chou, S.; Yamamoto, K.; Inoh, S.; Nojo, T.; Nakamura, S. Longer diabetes duration reduces myocardial blood flow in remote myocardium assessed by dynamic myocardial CT perfusion. J. Diabetes Complicat. 2018, 32, 609–615. [Google Scholar] [CrossRef]
- Peters, S.A.; Huxley, R.R.; Woodward, M. Diabetes as risk factor for incident coronary heart disease in women compared with men: A systematic review and meta-analysis of 64 cohorts including 858,507 individuals and 28,203 coronary events. Diabetologia 2014, 57, 1542–1551. [Google Scholar] [CrossRef]
- Kannel, W.B.; McGee, D.L. Diabetes and cardiovascular disease. The Framingham study. JAMA 1979, 241, 2035–2038. [Google Scholar] [CrossRef]
- Arnetz, L.; Ekberg, N.R.; Alvarsson, M. Sex differences in type 2 diabetes: Focus on disease course and outcomes. Diabetes Metab. Syndr. Obes. 2014, 7, 409–420. [Google Scholar] [CrossRef] [Green Version]
- De Ritter, R.; de Jong, M.; Vos, R.C.; van der Kallen, C.J.H.; Sep, S.J.S.; Woodward, M.; Stehouwer, C.D.A.; Bots, M.L.; Peters, S.A.E. Sex differences in the risk of vascular disease associated with diabetes. Biol. Sex Differ. 2020, 11, 1. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Non-DM (n = 251) | S-DM (n = 65) | L-DM (n = 134) | p-Value | Post-Hoc | |
|---|---|---|---|---|---|
| DM duration, years | 5 (0.17–7.33) | 20 (13.75–26) | |||
| Age, years | 71.8 ± 10.9 | 71.9 ± 9.7 | 70.5 ± 9.0 | 0.50 | |
| Sex | 0.018 | 1 > 3 | |||
| Male | 164 (65.3) | 37 (56.9) | 68 (50.8) | ||
| Female | 87 (34.7) | 28 (43.1) | 66 (49.2) | ||
| Smoking | 53 (21.1) | 14 (21.5) | 26 (19.4) | 0.91 | |
| BMI | 24.18 ± 4.23 | 24.40 ± 3.26 | 24.03 ± 3.51 | 0.82 | |
| HTN | 182 (72.5) | 52 (80.0) | 106 (79.1) | 0.24 | |
| Hyperlipidemia | 95 (37.9) | 40 (61.5) | 64 (47.8) | 0.002 | 1 < 2 |
| CKD | 27 (10.8) | 8 (12.3) | 37 (27.6) | <0.001 | 1, 2 < 3 |
| Dialysis | 15 (6.0) | 5 (7.7) | 20 (14.9) | 0.012 | 1 < 3 |
| Previous PCI | 54 (21.5) | 22 (33.9) | 38 (28.4) | 0.08 | |
| Previous CABG | 9 (3.6) | 6 (9.2) | 8 (6.0) | 0.16 | |
| Previous MI | 32 (12.8) | 8 (12.3) | 12 (9.0) | 0.53 | |
| CVA | 29 (11.6) | 16 (24.6) | 20 (14.9) | 0.028 | 1 < 2 |
| PVD | 12 (4.8) | 9 (13.9) | 16 (11.9) | 0.011 | 1 < 2, 3 |
| Chronic lung disease | 19 (7.6) | 8 (12.3) | 5 (3.7) | 0.08 | |
| Heart failure | 32 (12.8) | 16 (24.6) | 22 (16.4) | 0.06 | |
| Atrial fibrillation | 23 (9.2) | 11 (16.9) | 10 (7.5) | 0.10 | |
| Clinical diagnosis | 0.66 | ||||
| Stable angina, | 100 (39.8) | 24 (36.9) | 58 (43.3) | ||
| Acute coronary syndrome | 151 (60.2) | 41 (63.1) | 76 (56.7) | ||
| HbA1C | 5.8 ± 0.5 | 7.0 ± 1.3 | 7.6 ± 1.9 | <0.001 | 1 < 2 < 3 |
| Total cholesterol | 152.5 ± 41.7 | 139.0 ± 37.6 | 138.1 ± 34.5 | 0.001 | 1 > 2, 3 |
| LDL cholesterol | 90.8 ± 36.2 | 73.4 ± 28.1 | 76.8 ± 30.2 | <0.001 | 1 > 2, 3 |
| HDL cholesterol | 48.5 ± 15.3 | 43.8 ± 13.5 | 43.3 ± 14.1 | 0.003 | 1 > 2, 3 |
| Triglyceride | 118.9 ± 78.0 | 140.7 ± 70.3 | 124.1 ± 73.8 | 0.15 |
| Non-DM (n = 251) | S-DM (n = 65) | L-DM (n = 134) | p-Value | |
|---|---|---|---|---|
| Lesion classification | 0.22 | |||
| B1, n (%) | 11 (4.4) | 1 (1.5) | 4 (3.0) | |
| B2, n (%) | 23 (9.2) | 2 (3.1) | 16 (11.9) | |
| C, n (%) | 217 (86.5) | 62 (95.4) | 114 (85.1) | |
| MVD, n (%) | 189 (75.3) | 56 (86.2) | 115 (85.8) | 0.02 |
| CTO, n (%) | 34 (13.6) | 4 (6.2) | 17 (12.7) | 0.26 |
| Pre EF | 54.80 ± 13.08 | 52.98 ± 13.24 | 51.90 ± 14.77 | 0.13 |
| Procedure time, min | 83.03 ± 49.32 | 82.10 ± 40.84 | 74.39 ± 55.24 | 0.26 |
| Mean stent diameter, mm | 3.01 ± 0.38 | 3.01 ± 0.39 | 2.96 ± 0.38 | 0.38 |
| Total number of stent | 2.35 ± 1.15 | 2.19 ± 1.03 | 2.55 ± 1.26 | 0.11 |
| Total stent length, mm | 67.09 ± 32.72 | 60.31 ± 28.42 | 72.18 ± 39.17 | 0.08 |
| Number of burr, mm | 1.19 ± 0.45 | 1.25 ± 0.44 | 1.15 ± 0.36 | 0.32 |
| Technical success, n (%) | 243 (96.8) | 61 (93.9) | 128 (95.5) | 0.52 |
| Procedure success, n (%) | 233 (92.8) | 60 (92.3) | 131 (97.8) | 0.11 |
| Non-DM (n = 251) | S-DM (n = 65) | L-DM (n = 134) | p-Value | |
|---|---|---|---|---|
| In-hospital MACCEs | 35 (13.9) | 5 (7.7) | 15 (11.2) | 0.36 |
| In-hospital death | 6 (2.4) | 1 (1.5) | 4 (3.0) | 0.82 |
| Urgent revascularization | 4 (1.6) | 0 (0.0) | 4 (3.0) | 0.31 |
| In-hospital stroke | 2 (0.8) | 0 (0.0) | 0 (0.0) | 0.45 |
| Peri-procedure MI | 26 (10.4) | 5 (7.7) | 8 (6.0) | 0.33 |
| Procedural Complications | ||||
| Severe coronary dissection * | 35 (13.9) | 10 (15.4) | 19 (14.2) | 0.96 |
| Temporary pacemaker during procedure | 7 (2.8) | 5 (7.7) | 5 (3.7) | 0.18 |
| Coronary perforation | 6 (2.4) | 1 (1.5) | 1 (0.8) | 0.50 |
| Contrast-Induced Nephropathy | 4 (1.6) | 0 (0.0) | 7 (5.2) | 0.035 |
| In-hospital bleeding | 11 (4.4) | 6 (9.2) | 8 (6.0) | 0.31 |
| Non-DM (n = 251) | S-DM (n = 65) | L-DM (n = 134) | p-Value | |
|---|---|---|---|---|
| TVF, n (%) | 30 (12.0) | 9 (13.9) | 29 (21.6) | 0.039 |
| All cause death, n (%) | 19 (7.6) | 8 (12.3) | 12 (9.0) | 0.48 |
| Cardiac death, n (%) | 14 (5.6) | 5 (7.7) | 12 (9.0) | 0.44 |
| Any myocardial infarction, n (%) | 10 (4.0) | 0 (0.0) | 5 (3.7) | 0.27 |
| Target-vessel MI, n (%) | 6 (2.4) | 0 (0.0) | 3 (2.2) | 0.46 |
| Any repeat revascularization, n (%) | 19 (7.6) | 6 (9.2) | 21 (15.7) | 0.042 |
| TVR, n (%) | 15 (6.0) | 4 (6.2) | 17 (12.7) | 0.06 |
| Univariable | Multivariable ** | ||||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Target vessel failure | No DM | 1.00 | 1.00 | ||||
| S-DM | 1.13 | 0.54–2.38 | 0.75 | 1.04 | 0.45–2.44 | 0.92 | |
| L-DM | 1.85 | 1.11–3.01 | 0.018 | 1.86 | 1.04–3.34 | 0.037 | |
| All cause death | No DM | 1.00 | 1.00 | ||||
| S-DM | 1.55 | 0.68–3.54 | 0.30 | 0.77 | 0.25–2.35 | 0.65 | |
| L-DM | 1.18 | 0.57–2.43 | 0.66 | 0.98 | 0.44–2.21 | 0.97 | |
| Cardiac death | No DM | 1.00 | 1.00 | ||||
| S-DM | 1.32 | 0.47–3.66 | 0.60 | 0.66 | 0.16–2.67 | 0.56 | |
| L-DM | 1.60 | 0.74–3.46 | 0.23 | 1.67 | 0.69–4.04 | 0.26 | |
| Myocardial infarction | No DM | 1.00 | 1.00 | ||||
| S-DM | - | - | - | - | - | - | |
| L-DM | 0.91 | 0.31–2.67 | 0.87 | 0.85 | 0.23–3.21 | 0.81 | |
| Target vessel MI | No DM | 1.00 | 1.00 | ||||
| S-DM | - | - | - | - | - | - | |
| L-DM | 0.92 | 0.23–3.69 | 0.91 | 0.82 | 0.12–5.12 | 0.85 | |
| Any revascularization | No DM | 1.00 | 1.00 | ||||
| S-DM | 1.22 | 0.49–3.05 | 0.68 | 1.27 | 0.47–3.46 | 0.64 | |
| L-DM | 2.20 | 1.18–4.10 | 0.013 | 2.40 | 1.17–4.89 | 0.017 | |
| TVR | No DM | 1.00 | 1.00 | ||||
| S-DM | 1.01 | 0.33–3.03 | 0.99 | 0.87 | 0.26–2.98 | 0.83 | |
| L-DM | 2.21 | 1.10–4.43 | 0.025 | 2.16 | 0.94–4.94 | 0.07 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.; Her, S.-H.; Lee, K.; Jung, J.-H.; Yoo, K.-D.; Moon, K.-W.; Moon, D.; Lee, S.-N.; Jang, W.-Y.; Choi, I.-J.; et al. Impact of Diabetes Duration on Clinical Outcome in Patients Receiving Rotational Atherectomy in Calcified Lesions in Korea—Results from ROCK Registry. Life 2022, 12, 993. https://doi.org/10.3390/life12070993
Jung J, Her S-H, Lee K, Jung J-H, Yoo K-D, Moon K-W, Moon D, Lee S-N, Jang W-Y, Choi I-J, et al. Impact of Diabetes Duration on Clinical Outcome in Patients Receiving Rotational Atherectomy in Calcified Lesions in Korea—Results from ROCK Registry. Life. 2022; 12(7):993. https://doi.org/10.3390/life12070993
Chicago/Turabian StyleJung, Jin, Sung-Ho Her, Kyusup Lee, Ji-Hoon Jung, Ki-Dong Yoo, Keon-Woong Moon, Donggyu Moon, Su-Nam Lee, Won-Young Jang, Ik-Jun Choi, and et al. 2022. "Impact of Diabetes Duration on Clinical Outcome in Patients Receiving Rotational Atherectomy in Calcified Lesions in Korea—Results from ROCK Registry" Life 12, no. 7: 993. https://doi.org/10.3390/life12070993
APA StyleJung, J., Her, S.-H., Lee, K., Jung, J.-H., Yoo, K.-D., Moon, K.-W., Moon, D., Lee, S.-N., Jang, W.-Y., Choi, I.-J., Lee, J.-H., Lee, J.-H., Lee, S.-R., Lee, S.-W., Yun, K.-H., & Lee, H.-J. (2022). Impact of Diabetes Duration on Clinical Outcome in Patients Receiving Rotational Atherectomy in Calcified Lesions in Korea—Results from ROCK Registry. Life, 12(7), 993. https://doi.org/10.3390/life12070993