
Immediate Effects of Myofascial Release on the Thoracolumbar Fascia and Osteopathic Treatment for Acute Low Back Pain on Spine Shape Parameters: A Randomized, Placebo-Controlled Trial




Abstract
1. Introduction
2. Materials and Methods
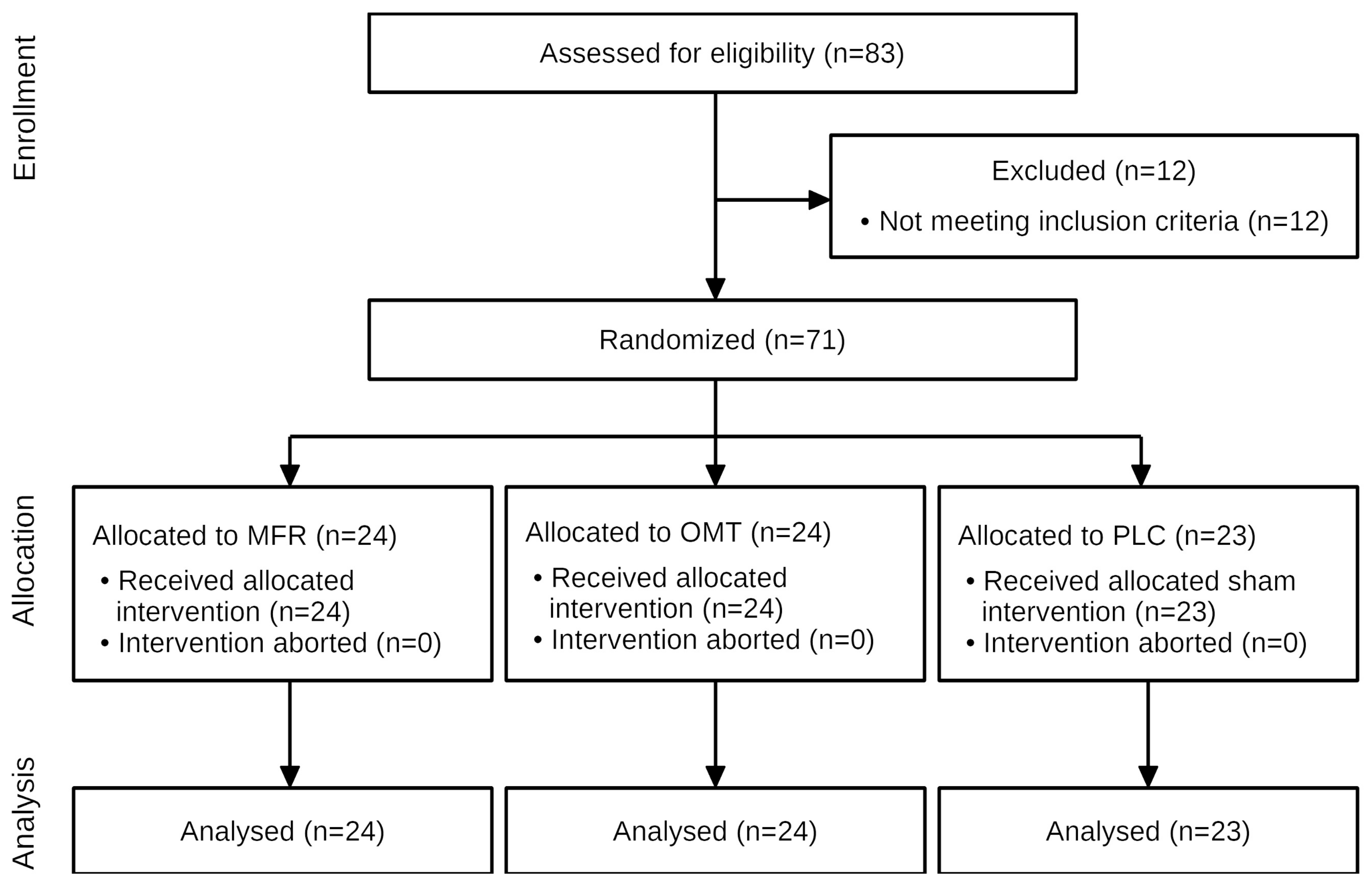
2.1. Study Design Overview
2.2. Setting and Participants
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Randomization and Interventions
2.3.1. Myofascial Release Intervention
2.3.2. Osteopathic Manipulative Treatment
2.3.3. Control
2.4. Outcomes
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Willard, F.H.; Vleeming, A.; Schuenke, M.D.; Danneels, L.; Schleip, R. The thoracolumbar fascia: Anatomy, function and clinical considerations. J. Anat. 2012, 221, 507–536. [Google Scholar] [CrossRef] [PubMed]
- Mense, S. Innervation of the thoracolumbar fascia. Eur. J. Transl. Myol. 2019, 29, 8297. [Google Scholar] [CrossRef] [PubMed]
- Lampert, T.; Prütz, F.; Seeling, S.; Starker, A.; Kroll, L.E.; Rommel, A.; Ryl, L.; Ziese, T. Gesundheit in Deutschland: Gesundheitsberichterstattung des Bundes, Gemeinsam Getragen von RKI und Destatis; Robert Koch-Institut: Berlin, Germany, 2015. [Google Scholar]
- Bundesärztekammer (BÄK); Kassenärztliche Bundesvereinigung (KBV); Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Nicht-spezifischer Kreuzschmerz—Langfassung, 2nd ed.; Bundesärztekammer; Kassenärztliche Bundesvereinigung; Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften: Berlin, Germany, 2017. [Google Scholar]
- Itz, C.J.; Geurts, J.W.; Van Kleef, M.; Nelemans, P. Clinical course of non-specific low back pain: A systematic review of prospective cohort studies set in primary care. Eur. J. Pain 2012, 17, 5–15. [Google Scholar] [CrossRef]
- Pengel, L.; Herbert, R.D.; Maher, C.; Refshauge, K.M. Acute low back pain: Systematic review of its prognosis. BMJ 2003, 327, 323. [Google Scholar] [CrossRef]
- Casser, H.-R.; Seddigh, S.; Rauschmann, M. Acute Lumbar Back Pain: Investigation, Differential Diagnosis, and Treatment. Dtsch. Aerzteblatt Online 2016, 113, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Jeevannavar, J.S.; Ganesh, G.A.; Jeevannavar, S.S. Prevalence of Leg Length Discrepancy in Persons with Non-Specific Low Back Pain. Indian J. Physiother. Occup. Ther.-Int. J. 2018, 12, 58. [Google Scholar] [CrossRef]
- Lee, S.-H.; Nam, S.-M. Effects of Active Release Technique on Pain, Oswestry Disability Index and Pelvic Asymmetry in Chronic Low Back Pain Patients. J. Korean Soc. Phys. Med. 2020, 15, 133–141. [Google Scholar] [CrossRef]
- Rannisto, S.; Okuloff, A.; Uitti, J.; Paananen, M.; Rannisto, P.-H.; Malmivaara, A.; Karppinen, J. Correction of leg-length discrepancy among meat cutters with low back pain: A randomized controlled trial. BMC Musculoskelet. Disord. 2019, 20, 105. [Google Scholar] [CrossRef]
- Rannisto, S.; Okuloff, A.; Uitti, J.; Paananen, M.; Rannisto, P.-H.; Malmivaara, A.; Karppinen, J. Leg-length discrepancy is associated with low back pain among those who must stand while working. BMC Musculoskelet. Disord. 2015, 16, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, A.; Arab, A.M.; Nourbakhsh, M.R.; Hosseini, S.M.; Forghany, S. Lower limb kinematics in individuals with chronic low back pain during walking. J. Electromyogr. Kinesiol. 2020, 51, 102404. [Google Scholar] [CrossRef]
- da Rosa, B.N.; Furlanetto, T.S.; Noll, M.; Sedrez, J.A.; Schmit, E.F.D.; Candotti, C.T. 4-year Longitudinal Study of the Assessment of Body Posture, Back Pain, Postural and Life Habits of Schoolchildren. Motricidade 2018, 13, 3–12. [Google Scholar] [CrossRef]
- Ajimsha, M.S.; Surendran, P.; Jacob, P.; Shenoy, P.; Bilal, M. Myofascial Force Transmission in the Humans: A Systematic Scoping Review of In-Vivo Studies. Preprints 2020, 2020110212. [Google Scholar] [CrossRef]
- Arguisuelas, M.D.; Lisón, J.F.; Sánchez-Zuriaga, D.; Martínez-Hurtado, I.; Doménech-Fernández, J. Effects of Myofascial Release in Nonspecific Chronic Low Back Pain. Spine 2017, 42, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Arguisuelas, M.; Lisón, J.; Doménech-Fernández, J.; Martínez-Hurtado, I.; Coloma, P.S.; Sánchez-Zuriaga, D. Effects of myofascial release in erector spinae myoelectric activity and lumbar spine kinematics in non-specific chronic low back pain: Randomized controlled trial. Clin. Biomech. 2019, 63, 27–33. [Google Scholar] [CrossRef]
- Farra, F.D.; Risio, R.G.; Vismara, L.; Bergna, A. Effectiveness of osteopathic interventions in chronic non-specific low back pain: A systematic review and meta-analysis. Complement. Ther. Med. 2020, 56, 102616. [Google Scholar] [CrossRef]
- Wong, K.-K.; Chai, H.-M.; Chen, Y.-J.; Wang, C.-L.; Shau, Y.-W.; Wang, S.-F. Mechanical deformation of posterior thoracolumbar fascia after myofascial release in healthy men: A study of dynamic ultrasound imaging. Musculoskelet. Sci. Pract. 2017, 27, 124–130. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Chai, H.-M.; Shau, Y.-W.; Wang, C.-L.; Wang, S.-F. Increased sliding of transverse abdominis during contraction after myofascial release in patients with chronic low back pain. Man. Ther. 2015, 23, 69–75. [Google Scholar] [CrossRef]
- Franke, H.; Franke, J.-D.; Fryer, G. Osteopathic manipulative treatment for nonspecific low back pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2014, 15, 1–18. [Google Scholar] [CrossRef]
- Rubinstein, S.M.; De Zoete, A.; Van Middelkoop, M.; Assendelft, W.J.J.; de Boer, M.; van Tulder, M. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: Systematic review and meta-analysis of randomised controlled trials. BMJ 2019, 364, l689. [Google Scholar] [CrossRef] [PubMed]
- Barnes, M.F. Efficacy study of the effect of a myofascial release treatment technique on obtaining pelvic symmetry. J. Bodyw. Mov. Ther. 1997, 1, 289–296. [Google Scholar] [CrossRef]
- Gordon, J.E.; Davis, L.E. Leg Length Discrepancy: The Natural History (And What Do We Really Know). J. Pediatr. Orthop. 2019, 39, S10–S13. [Google Scholar] [CrossRef]
- Brandl, A. Practical Measurement of Changes in Leg Length Discrepancy after a Myofascial Release on the Thoracolumbar Fascia in Patients with Acute Low Back Pain. A Pilot Study. SportRxiv 2021. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association World Medical Association Declaration of Helsinki. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed]
- van Tulder, M.; Becker, A.; Bekkering, T.; Breen, A.; Gil Del Real, M.T.; Hutchinson, A.; Koes, B.; Laerum, E.; Malmivaara, A. On behalf of the COST B13 Working Group on Guidelines for the Management of Acute Low Back Pain in Primary Care Chapter 3 European guidelines for the management of acute nonspecific low back pain in primary care. Eur. Spine J. 2006, 15, s169–s191. [Google Scholar] [CrossRef] [PubMed]
- Gaul, C.; Mette, E.; Schmidt, T.; Grond, S. ODQ—Oswestry Low Back Pain Disability Questionnaire—deutsche Fassung. BioMed Res. Int. 2008, 2008, 51–58. [Google Scholar] [CrossRef]
- Cline, M.E.; Herman, J.; Shaw, E.R.; Morton, R.D. Standardization of the Visual Analogue Scale. Nurs. Res. 1992, 41, 378–379. [Google Scholar] [CrossRef]
- Urbaniak, G.C.; Plous, S. Research Randomizer (Version 4.0) [Computer Software]. Available online: http://www.Randomizer.Org/ (accessed on 22 June 2013).
- Chila, A.G.; O’Connell, J.A. (Eds.) Foundations of Osteopathic Medicine, 3rd ed.; Lippincott Williams & Wilkins: London, UK, 2010; ISBN 978-0-7817-6671-5. [Google Scholar]
- Ajimsha, M.; Al-Mudahka, N.R.; Al-Madzhar, J. Effectiveness of myofascial release: Systematic review of randomized controlled trials. J. Bodyw. Mov. Ther. 2015, 19, 102–112. [Google Scholar] [CrossRef]
- Triano, J.J.; Gissler, T.; Forgie, M.; Milwid, D. Maturation in Rate of High-Velocity, Low-Amplitude Force Development. J. Manip. Physiol. Ther. 2011, 34, 173–180. [Google Scholar] [CrossRef]
- Degenhardt, B.F.; Starks, Z.; Bhatia, S. Reliability of the DIERS Formetric 4D Spine Shape Parameters in Adults without Postural Deformities. BioMed Res. Int. 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Schleip, R. Fascial plasticity—A new neurobiological explanation: Part 1. J. Bodyw. Mov. Ther. 2003, 7, 11–19. [Google Scholar] [CrossRef]
- Schleip, R. Fascial plasticity—A new neurobiological explanation Part 2. J. Bodyw. Mov. Ther. 2003, 7, 104–116. [Google Scholar] [CrossRef]
- Jeon, C.K.; Hospital, A.; Han, S.Y.; Yoo, K.T. The Effects of Manual Therapy on Lower Extremity Alignment in Pelvic Malalignment. J. Int. Acad. Phys. Ther. Res. 2018, 9, 1543–1548. [Google Scholar] [CrossRef][Green Version]
- Schmidt, T.; Burger, S.; Fetzer, J.; Reer, R.; Braumann, K.-M. Auswirkung von thorakalen Manipulationen auf die sagittale Ausrichtung der Wirbelsäule. Man. Med. 2012, 50, 197–203. [Google Scholar] [CrossRef]
- Vleeming, A.; Buyruk, H.M.; Stoeckart, R.; Karamursel, S.; Snijders, C.J. An integrated therapy for peripartum pelvic instability: A study of the biomechanical effects of pelvic belts. Am. J. Obstet. Gynecol. 1992, 166, 1243–1247. [Google Scholar] [CrossRef]
- Kiapour, A.; Joukar, A.; Elgafy, H.; Erbulut, D.U.; Agarwal, A.K.; Goel, V.K. Biomechanics of the Sacroiliac Joint: Anatomy, Function, Biomechanics, Sexual Dimorphism, and Causes of Pain. Int. J. Spine Surg. 2019, 14, S3–S13. [Google Scholar] [CrossRef]
- Stecco, A.; Gesi, M.; Stecco, C.; Stern, R. Fascial Components of the Myofascial Pain Syndrome. Curr. Pain Headache Rep. 2013, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sheha, E.D.; Steinhaus, M.E.; Kim, H.J.; Cunningham, M.E.; Fragomen, A.T.; Rozbruch, S.R. Leg-Length Discrepancy, Functional Scoliosis, and Low Back Pain. JBJS Rev. 2018, 6, e6. [Google Scholar] [CrossRef]
- Wilczyński, J.; Karolak, P.; Janecka, S.; Kabała, M.; Habik-Tatarowska, N. The Relationship between the Angle of Curvature of the Spine and SEMG Amplitude of the Erector Spinae in Young School-Children. Appl. Sci. 2019, 9, 3115. [Google Scholar] [CrossRef]
- Koes, B.W.; van Tulder, M.; Thomas, S. Diagnosis and treatment of low back pain. BMJ 2006, 332, 1430–1434. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | MFR Group (n = 24) Mean ± SD | OMT Group (n = 24) Mean ± SD | PLC Group (n = 23) Mean ± SD | Total (n = 71) Mean ± SD |
|---|---|---|---|---|
| Gender (men/woman) | 12/12 | 14/10 | 8/15 | 34/37 |
| Age (years) min–max (years) | 45.7 ± 9.4 20.4–59.9 | 43.2 ± 11.4 20.5–59.2 | 42.3 ± 10.6 23.9–59.3 | 43.8 ± 10.5 20.4–59.9 |
| Height (m) min–max (m) | 1.72 ± 0.1 1.60–1.92 | 1.75 ± 0.1 1.61–1.89 | 1.70 ± 0.1 1.59–1.89 | 1.72 ± 0.1 1.59–1.92 |
| Weight (kg) min–max (kg) | 75.8 ± 13.4 47–97 | 78.3 ± 14.3 60–110 | 72.3 ± 9.6 60–92 | 75.5 ± 12.7 47–110 |
| BMI (kg/m2) min–max (kg/m2) | 25.5 ± 3.6 17.9–35.2 | 25.5 ± 3.5 18.7–33.9 | 25.2 ± 3.7 21.7–35.2 | 25.4 ± 3.5 17.9–35.2 |
| fLLD (mm) min–max (mm) | 7.3 ± 4.0 0–13 | 9.4 ± 5.0 1–18 | 8.0 ± 4.9 0–17 | 8.2 ± 4.7 0–18 |
| ODQ-D (0–100) min–max | 23.2 ± 13.5 10–68 | 21.8 ± 11.0 11–48 | 22.6 ± 10.3 10–46 | 22.5 ± 11.5 10–68 |
| VAS (0–10) min–max | 5.0 ± 2.1 3–10 | 5.5 ± 1.9 3–10 | 4.7 ± 1.4 3–9 | 5.1 ± 1.8 3–10 |
| Pain duration (days) min–max | 11.7 ± 6.8 1–24 | 10.1 ± 8.5 1–29 | 14.4 ± 6.9 2–29 | 12.0 ± 7.6 1–29 |
| Outcome | MFR Group (n = 24) Mean (95% CI) | OMT Group (n = 24) Mean (95% CI) | PLC Group (n = 23) Mean (95% CI) |
|---|---|---|---|
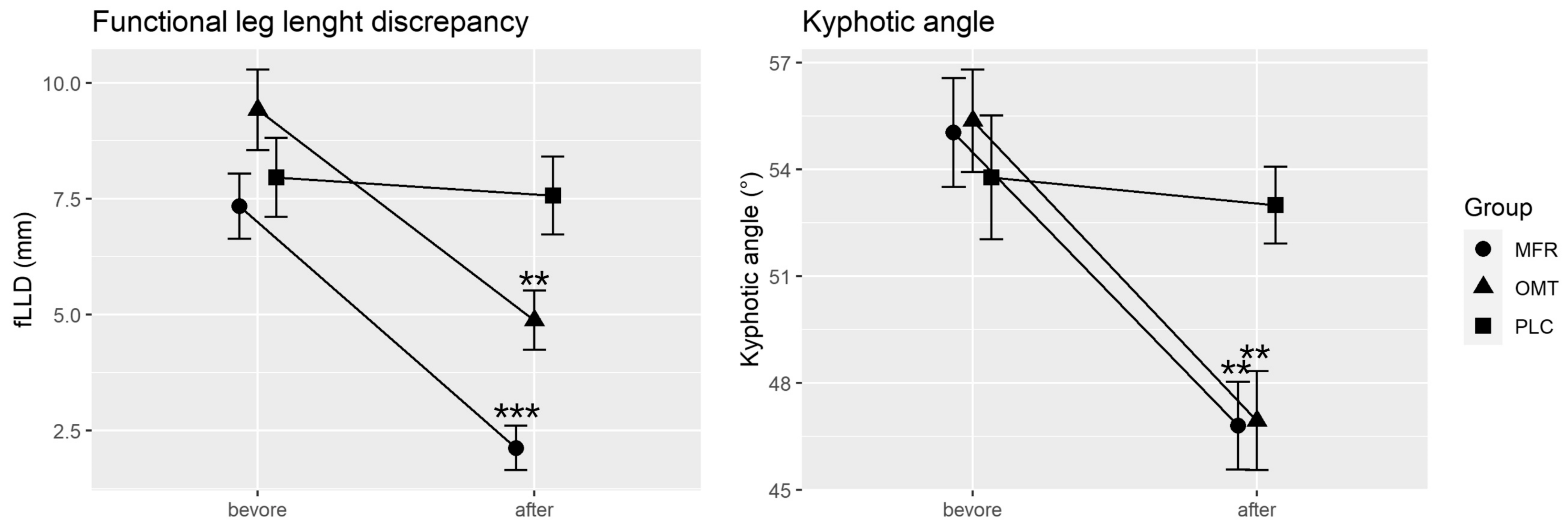
| fLLD (mm) | −5.2 (−8.8–−1.6) *** | −4.5 (−8.1–−1.0) ** | −0.4 (−4.0–3.2) |
| Kyphotic angle (°) | −8.23 (−15–−1.4) ** | −8.42 (−15–−1.6) ** | −0.8 (−7.7–6.1) |
| Lordotic angle (°) | 1.5 (−5.8–8.7) | −5.0 (−12.3–2.3) | 0.1 (−7.4–7.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brandl, A.; Egner, C.; Schleip, R. Immediate Effects of Myofascial Release on the Thoracolumbar Fascia and Osteopathic Treatment for Acute Low Back Pain on Spine Shape Parameters: A Randomized, Placebo-Controlled Trial. Life 2021, 11, 845. https://doi.org/10.3390/life11080845
Brandl A, Egner C, Schleip R. Immediate Effects of Myofascial Release on the Thoracolumbar Fascia and Osteopathic Treatment for Acute Low Back Pain on Spine Shape Parameters: A Randomized, Placebo-Controlled Trial. Life. 2021; 11(8):845. https://doi.org/10.3390/life11080845
Chicago/Turabian StyleBrandl, Andreas, Christoph Egner, and Robert Schleip. 2021. "Immediate Effects of Myofascial Release on the Thoracolumbar Fascia and Osteopathic Treatment for Acute Low Back Pain on Spine Shape Parameters: A Randomized, Placebo-Controlled Trial" Life 11, no. 8: 845. https://doi.org/10.3390/life11080845
APA StyleBrandl, A., Egner, C., & Schleip, R. (2021). Immediate Effects of Myofascial Release on the Thoracolumbar Fascia and Osteopathic Treatment for Acute Low Back Pain on Spine Shape Parameters: A Randomized, Placebo-Controlled Trial. Life, 11(8), 845. https://doi.org/10.3390/life11080845