
Low-Level Elevations of Procalcitonin Are Associated with Increased Mortality in Acute Heart Failure Patients, Independent of Concomitant Infection

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Adjudication of Final Diagnoses
2.2. Biomarker Testing
2.3. Diagnostic Performance of NT-ProBNP
2.4. Prognostic Value of NT-ProBNP in the Overall Study Population
2.5. PCT for the Discrimination of Infection
2.6. Diagnostic Added Value of NT-ProBNP and PCT
2.7. Prognostic Value of PCT in the Entire Study Cohort and in AHF with or without Established Respiratory or Other Infection
2.8. Assessment of the Independent Prognostic Performance of NT-ProBNP and PCT
2.9. Statistical Analysis
3. Results
3.1. Characteristics of AHF Patients with and without Respiratory or Other Infection
3.2. Diagnostic Performance of NT-ProBNP at the Established Cutoff Values
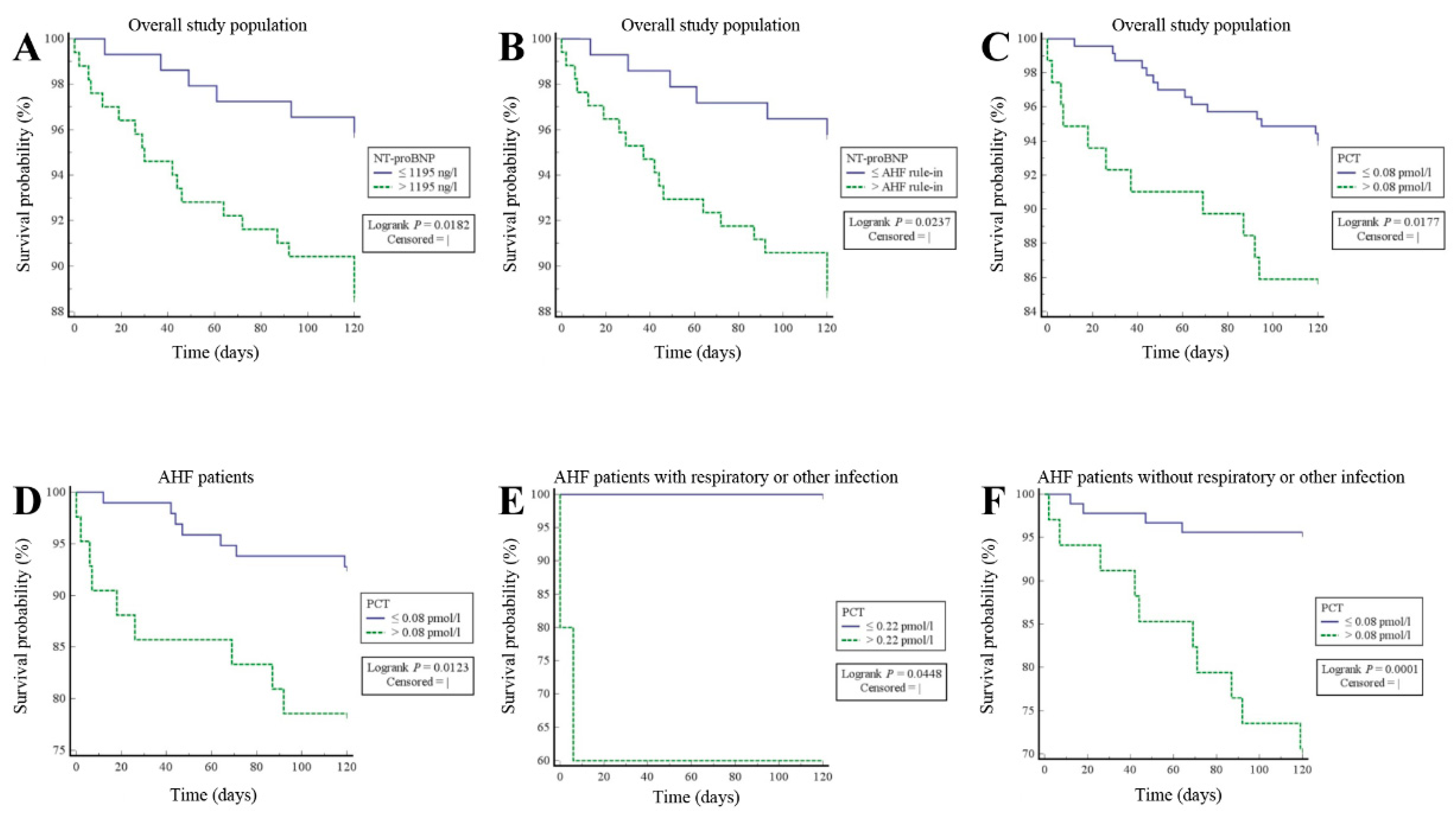
3.3. Prognostic Value of NT-ProBNP in the Overall Study Population
3.4. Diagnostic Performance of PCT for Respiratory or Other Infection in the Overall Study Population and in AHF Patients
3.5. Diagnostic Added Value of NT-ProBNP and PCT
3.6. Prognostic Value of PCT in the Entire Study Cohort and in AHF Patients with or without Respiratory or Other Infection
3.7. Independent Prognostic Performance of NT-ProBNP and PCT in Patients with Acute Dyspnea
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maisel, A.S.; Peacock, W.F.; McMullin, N.; Jessie, R.; Fonarow, G.C.; Wynne, J.; Mills, R.M. Timing of immunoreactive B-type natriuretic peptide levels and treatment delay in acute decompensated heart failure: An ADHERE (Acute Decompensated Heart Failure National Registry) analysis. J. Am. Coll. Cardiol. 2008, 5, 534–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayés-Genís, A.; Santaló-Bel, M.; Zapico-Muñiz, E.; López, L.; Cotes, C.; Bellido, J.; Leta, R.; Casan, P.; Ordóñez-Llanos, J. N-terminal probrain natriuretic peptide (NT-proBNP) in the emergency diagnosis and in-hospital monitoring of patients with dyspnoea and ventricular dysfunction. Eur. J. Heart Fail. 2004, 6, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Lainchbury, J.G.; Campbell, E.; Frampton, C.M.; Yandle, T.G.; Nicholls, M.G.; Richards, A.M. Brain natriuretic peptide and n-terminal brain natriuretic peptide in the diagnosis of heart failure in patients with acute shortness of breath. J. Am. Coll. Cardiol. 2003, 42, 728–735. [Google Scholar] [CrossRef] [Green Version]
- Januzzi, J.L., Jr.; Camargo, C.A.; Anwaruddin, S.; Baggish, A.L.; Chen, A.A.; Krauser, D.G.; Tung, R.; Cameron, R.; Nagurney, J.T.; Chae, C.U.; et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am. J. Cardiol. 2005, 95, 948–954. [Google Scholar] [CrossRef]
- 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. European Society of Cardiology (ESC). Available online: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-and-Chronic-Heart-Failure (accessed on 27 August 2021).
- Darche, F.F.; Baumgärtner, C.; Biener, M.; Müller-Hennessen, M.; Vafaie, M.; Koch, V.; Stoyanov, K.; Rivinius, R.; Katus, H.A.; Giannitsis, E. Comparative accuracy of NT-proBNP and MR-proANP for the diagnosis of acute heart failure in dyspnoeic patients. ESC Heart Fail. 2017, 4, 232–240. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Manzano-Fernández, S.; Boronat, M.; Casas, T.; Garrido, I.P.; Bonaque, J.C.; Pastor-Perez, F.; Valdés, M.; Januzzi, J.L. Soluble ST2, high-sensitivity troponin T- and N-terminal pro-B-type natriuretic peptide: Complementary role for risk stratification in acutely decompensated heart failure. Eur. J. Heart Fail. 2011, 13, 718–725. [Google Scholar] [CrossRef]
- Möckel, M.; Searle, J.; Maisel, A. The role of procalcitonin in acute heart failure patients. ESC Heart Fail. 2017, 4, 203–208. [Google Scholar] [CrossRef] [Green Version]
- Schuetz, P.; Kutz, A.; Grolimund, E.; Haubitz, S.; Demann, D.; Vögeli, A.; Hitz, F.; Christ-Crain, M.; Thomann, R.; Falconnier, C.; et al. Excluding infection through procalcitonin testing improves outcomes of congestive heart failure patients presenting with acute respiratory symptoms: Results from the randomized ProHOSP trial. Int. J. Cardiol. 2014, 175, 464–472. [Google Scholar] [CrossRef]
- Möckel, M.; de Boer, R.A.; Slagman, A.C.; von Haehling, S.; Schou, M.; Vollert, J.O.; Wiemer, J.C.; Ebmeyer, S.; Martín-Sánchez, F.J.; Maisel, A.S.; et al. Improve Management of acute heart failure with ProcAlCiTonin in EUrope: Results of the randomized clinical trial IMPACT EU Biomarkers in Cardiology (BIC) 18. Eur. J. Heart Fail. 2020, 22, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Mollar, A.; Villanueva, M.P.; Carratalá, A.; Núñez, E.; Sanchis, J.; Núñez, J. Determinants of procalcitonin concentration in acute heart failure. Int. J. Cardiol. 2014, 177, 532–534. [Google Scholar] [CrossRef]
- Boulogne, M.; Sadoune, M.; Launay, J.M.; Baudet, M.; Cohen-Solal, A.; Logeart, D. Inflammation versus mechanical stretch biomarkers over time in acutely decompensated heart failure with reduced ejection fraction. Int. J. Cardiol. 2017, 226, 53–59. [Google Scholar] [CrossRef]
- Baggish, A.L.; Siebert, U.; Lainchbury, J.G.; Cameron, R.; Anwaruddin, S.; Chen, A.; Krauser, D.G.; Tung, R.; Brown, D.F.; Richards, A.M.; et al. A validated clinical and biochemical score for the diagnosis of acute heart failure: The ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) Acute Heart Failure Score. Am. Heart J. 2006, 151, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Mathewkutty, S.; Sethi, S.S.; Aneja, A.; Shah, K.; Iyengar, R.L.; Hermann, L.; Khakimov, S.; Razzouk, L.; Esquitin, R.; Vedanthan, R.; et al. Biomarkers after risk stratification in acute chest pain (from the BRIC Study). Am. J. Cardiol. 2013, 111, 493–498. [Google Scholar] [CrossRef] [Green Version]
- Morgenthaler, N.G.; Struck, J.; Thomas, B.; Bergmann, A. Immunoluminometric assay for the midregion of pro-atrial natriuretic peptide in human plasma. Clin. Chem. 2004, 50, 234–236. [Google Scholar] [CrossRef] [Green Version]
- Von Haehling, S.; Jankowska, E.A.; Morgenthaler, N.G.; Vassanelli, C.; Zanolla, L.; Rozentryt, P.; Filippatos, G.S.; Doehner, W.; Koehler, F.; Papassotiriou, J.; et al. Comparison of midregional pro-atrial natriuretic peptide with N-terminal pro-B-type natriuretic peptide in predicting survival in patients with chronic heart failure. J. Am. Coll. Cardiol. 2007, 50, 1973–1980. [Google Scholar] [CrossRef] [Green Version]
- Gegenhuber, A.; Struck, J.; Poelz, W.; Pacher, R.; Morgenthaler, N.G.; Bergmann, A.; Haltmayer, M.; Mueller, T. Midregional pro-A-type natriuretic peptide measurements for diagnosis of acute destabilized heart failure in short-of-breath patients: Comparison with B-type natriuretic peptide (BNP) and amino-terminal proBNP. Clin. Chem. 2006, 52, 827–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gegenhuber, A.; Struck, J.; Dieplinger, B.; Poelz, W.; Pacher, R.; Morgenthaler, N.G.; Bergmann, A.; Haltmayer, M.; Mueller, T. Comparative evaluation of B-type natriuretic peptide, mid-regional pro-A-type natriuretic peptide, mid-regional pro-adrenomedullin, and Copeptin to predict 1-year mortality in patients with acute destabilized heart failure. J. Card. Fail. 2007, 13, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Januzzi, J.L., Jr.; Chen-Tournoux, A.A.; Christenson, R.H.; Doros, G.; Hollander, J.E.; Levy, P.D.; Nagurney, J.T.; Nowak, R.M.; Pang, P.S.; Patel, D.; et al. N-Terminal Pro-B-Type Natriuretic Peptide in the Emergency Department: The ICON-RELOADED Study. J. Am. Coll. Cardiol. 2018, 71, 1191–1200. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef]
- Demissei, B.G.; Cleland, J.G.; O’Connor, C.M.; Metra, M.; Ponikowski, P.; Teerlink, J.R.; Davison, B.; Givertz, M.M.; Bloomfield, D.M.; Dittrich, H.; et al. Procalcitonin-based indication of bacterial infection identifies high risk acute heart failure patients. Int. J. Cardiol. 2016, 204, 164–171. [Google Scholar] [CrossRef]
- Villanueva, M.P.; Mollar, A.; Palau, P.; Carratalá, A.; Núñez, E.; Santas, E.; Bodí, V.; Chorro, F.J.; Miñana, G.; Blasco, M.L.; et al. Procalcitonin and long-term prognosis after an admission for acute heart failure. Eur. J. Intern. Med. 2015, 26, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.; Mueller, C.; Nowak, R.; Peacock, W.F.; Landsberg, J.W.; Ponikowski, P.; Mockel, M.; Hogan, C.; Wu, A.H.; Richards, M.; et al. Mid-region pro-hormone markers for diagnosis and prognosis in acute dyspnea: Results from the BACH (Biomarkers in Acute Heart Failure) trial. J. Am. Coll. Cardiol. 2010, 55, 2062–2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuetz, P.; Mueller, B.; Trampuz, A. Serum procalcitonin for discrimination of blood contamination from bloodstream infection due to coagulase-negative staphylococci. Infection 2007, 35, 352–355. [Google Scholar] [CrossRef] [Green Version]
- Müller, F.; Christ-Crain, M.; Bregenzer, T.; Krause, M.; Zimmerli, W.; Mueller, B.; Schuetz, P.; ProHOSP Study Group. Procalcitonin levels predict bacteremia in patients with community-acquired pneumonia: A prospective cohort trial. Chest 2010, 138, 121–129. [Google Scholar] [CrossRef]
- van Nieuwkoop, C.; Bonten, T.N.; van’t Wout, J.W.; Kuijper, E.J.; Groeneveld, G.H.; Becker, M.J.; Koster, T.; Wattel-Louis, G.H.; Delfos, N.M.; Ablij, H.C.; et al. Procalcitonin reflects bacteremia and bacterial load in urosepsis syndrome: A prospective observational study. Crit. Care 2010, 14, R206. [Google Scholar] [CrossRef] [Green Version]
- Christ-Crain, M.; Stolz, D.; Bingisser, R.; Müller, C.; Miedinger, D.; Huber, P.R.; Zimmerli, W.; Harbarth, S.; Tamm, M.; Müller, B. Procalcitonin guidance of antibiotic therapy in community-acquired pneumonia: A randomized trial. Am. J. Respir. Crit. Care Med. 2006, 174, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Christ-Crain, M.; Albrich, W.; Zimmerli, W.; Mueller, B.; ProHOSP Study Group. Guidance of antibiotic therapy with procalcitonin in lower respiratory tract infections: Insights into the ProHOSP study. Virulence 2010, 1, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Suter-Widmer, I.; Chaudri, A.; Christ-Crain, M.; Zimmerli, W.; Mueller, B. Antibiotic Therapy and Hospitalisation in Patients with Lower Respiratory Tract Infections (ProHOSP) Study Group. Prognostic value of procalcitonin in community-acquired pneumonia. Eur. Respir. J. 2011, 37, 384–392. [Google Scholar] [CrossRef] [Green Version]
- Müller, B.; Harbarth, S.; Stolz, D.; Bingisser, R.; Mueller, C.; Leuppi, J.; Nusbaumer, C.; Tamm, M.; Christ-Crain, M. Diagnostic and prognostic accuracy of clinical and laboratory parameters in community-acquired pneumonia. BMC Infect. Dis. 2007, 7, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gogos, C.A.; Drosou, E.; Bassaris, H.P.; Skoutelis, A. Pro- versus anti-inflammatory cytokine profile in patients with severe sepsis: A marker for prognosis and future therapeutic options. J. Infect. Dis. 2000, 181, 176–180. [Google Scholar] [CrossRef]
- Levine, B.; Kalman, J.; Mayer, L.; Fillit, H.M.; Packer, M. Elevated circulating levels of tumor necrosis factor in severe chronic heart failure. N. Engl. J. Med. 1990, 323, 236–241. [Google Scholar] [CrossRef]
- Ferrari, R.; Bachetti, T.; Confortini, R.; Opasich, C.; Febo, O.; Corti, A.; Cassani, G.; Visioli, O. Tumor necrosis factor soluble receptors in patients with various degrees of congestive heart failure. Circulation 1995, 92, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Rauchhaus, M.; Doehner, W.; Francis, D.P.; Davos, C.; Kemp, M.; Liebenthal, C.; Niebauer, J.; Hooper, J.; Volk, H.D.; Coats, A.J.; et al. Plasma cytokine parameters and mortality in patients with chronic heart failure. Circulation 2000, 102, 3060–3067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasan, R.S.; Sullivan, L.M.; Roubenoff, R.; Dinarello, C.A.; Harris, T.; Benjamin, E.J.; Sawyer, D.B.; Levy, D.; Wilson, P.W.; D’Agostino, R.B.; et al. Inflammatory markers and risk of heart failure in elderly subjects without prior myocardial infarction: The Framingham Heart Study. Circulation 2003, 107, 1486–1491. [Google Scholar] [CrossRef] [PubMed]
- Miettinen, K.H.; Lassus, J.; Harjola, V.P.; Siirilä-Waris, K.; Melin, J.; Punnonen, K.R.; Nieminen, M.S.; Laakso, M.; Peuhkurinen, K.J. Prognostic role of pro- and anti-inflammatory cytokines and their polymorphisms in acute decompensated heart failure. Eur. J. Heart Fail. 2008, 10, 396–403. [Google Scholar] [CrossRef] [Green Version]
- Anker, S.D.; Egerer, K.R.; Volk, H.D.; Kox, W.J.; Poole-Wilson, P.A.; Coats, A.J. Elevated soluble CD14 receptors and altered cytokines in chronic heart failure. Am. J. Cardiol. 1997, 79, 1426–1430. [Google Scholar] [CrossRef]
- Niebauer, J.; Volk, H.D.; Kemp, M.; Dominguez, M.; Schumann, R.R.; Rauchhaus, M.; Poole-Wilson, P.A.; Coats, A.J.; Anker, S.D. Endotoxin and immune activation in chronic heart failure: A prospective cohort study. Lancet 1999, 353, 1838–1842. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, X.; Ge, N.; Liu, J.; Yuan, H.; Zhang, P.; Liu, W.; Wen, D. Procalcitonin testing for diagnosis and short-term prognosis in bacterial infection complicated by congestive heart failure: A multicenter analysis of 4698 cases. Crit. Care 2014, 18, R4. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Parameter | AHF Patients without Respiratory or Other Infection n = 125 | AHF Patients with Respiratory or Other Infection n = 14 | p-Value |
|---|---|---|---|
| Gender (male), n (%) | 90 of 125 (72.0%) | 11 of 14 (78.6%) | 0.6022 |
| Arterial hypertension, n (%) | 103 of 125 (82.4%) | 12 of 14 (85.7%) | 0.7565 |
| Dyslipidemia, n (%) | 73 of 125 (58.4%) | 6 of 14 (42.9%) | 0.2672 |
| Diabetes mellitus, n (%) | 49 of 125 (39.2%) | 3 of 14 (21.4%) | 0.1941 |
| History of smoking, n (%) | 83 of 125 (66.2%) | 9 of 14 (66.2%) | 0.8745 |
| Obesity (BMI ≥ 30 kg/m2), n (%) | 41 of 124 (33.1%) | 6 of 14 (42.9%) | 0.4652 |
| Impaired systolic LV function, n (%) | 94 of 121 (77.7%) | 10 of 13 (76.9%) | 0.9502 |
| Kidney failure (GFR < 60/mL), n (%) | 67 of 125 (53.6%) | 9 of 14 (54.7%) | 0.4479 |
| Age (a), mean ± SEM | 72.9 ± 1.0 | 74.1 ± 2.2 | 0.7086 |
| NT-proBNP (ng/L), mean ± SEM | 8307.4 ± 819.0 | 24,102.6 ± 6930.8 | <0.001 * |
| PCT (ng/mL), mean ± SEM | 0.10 ± 0.03 | 0.39 ± 0.23 | <0.001 * |
| CRP (mg/L), mean ± SEM | 7.7 ± 0.8 | 85.7 ± 18.7 | <0.001 * |
| WBC (n/nL), mean ± SEM | 9.6 ± 0.8 | 14.0 ± 1.2 | <0.001 * |
| Biomarker | Sensitivity (95% CI) | Specificity (95% CI) | Positive Predictive Value (95% CI) | Negative Predictive Value (95% CI) | Cutoff Value | AUC (95% CI) |
|---|---|---|---|---|---|---|
| NT-proBNP Patient’s age: <50 years, n = 27 | 100% (47.8 to 100%) | 81.8% (59.7 to 94.8%) | 55.5% (34.0 to 75.2%) | 100% | 450 ng/L (established cutoff value) | 0.945 (0.784 to 0.996) |
| NT-proBNP Patient’s age: 50–75 years, n = 165 | 92.5% (83.4 to 97.5%) | 72.5% (62.5 to 81.0%) | 69.7% (62.3 to 76.2%) | 93.4% (85.8 to 97.1%) | 900 ng/L (established cutoff value) | 0.910 (0.856 to 0.949) |
| NT-proBNP Patient’s age: >75 years, n = 120 | 80.6% (69.1 to 89.2%) | 69.8% (55.7 to 81.7%) | 77.1% (68.8 to 83.8%) | 74.0% (62.9 to 82.7%) | 1800 ng/L (established cutoff value) | 0.834 (0.755 to 0.896) |
| PCT Overall study population, n = 312 | 25.6% (13.0 to 42.1%) | 97.8% (95.3 to 99.2%) | 62.4% (39.0 to 81.2%) | 90.2% (88.4 to 91.7%) | 0.25 ng/mL (established cutoff value) | 0.774 (0.723 to 0.819) |
| PCT AHF patients, n = 139 | 28.6% (8.4 to 58.1%) | 98.4% (94.3 to 99.8%) | 66.7% (28.7 to 90.9%) | 92.5% (89.8 to 94.5%) | 0.25 ng/mL (established cutoff value) | 0.801 (0.725 to 0.864) |
| PCT Overall study population, n = 312 | 64.1% (47.2 to 78.8%) | 89.4% (85.1 to 92.8%) | 46.3% (36.3 to 56.7%) | 94.6% (92.0 to 96.4%) | 0.10 ng/mL (ROC optimal cutoff value) | 0.774 (0.723 to 0.819) |
| PCT AHF patients, n = 139 | 71.4% (41.9 to 91.6%) | 88.0% (81.0 to 93.1%) | 40.0% (27.2 to 54.3%) | 96.5% (92.3 to 98.4%) | 0.11 ng/mL (ROC optimal cutoff value) | 0.801 (0.725 to 0.864) |
| Biomarker | AUC (95% CI) | ΔAUC = AUCNT-proBNP–AUCBiomarker (95% CI; p-Value) | ΔAUC = AUCNT-proBNP + PCT–AUCBiomarker (95% CI; p-Value) |
|---|---|---|---|
| NT-proBNP | 0.955 (0.911 to 0.981) | 0 | −0.006 (−0.003–0.015; p = 0.1615) |
| PCT | 0.822 (0.754 to 0.877) | 0.133 (0.005 to 0.262; p = 0.0412) | 0.127 (0.003 to 0.251; p = 0.0440) |
| NT-proBNP + PCT | 0.949 (0.903 to 0.977) | 0.006 (0.003 to 0.015; p = 0.1615) | 0 |
| Biomarker | p-Value |
|---|---|
| PCT retains NT-proBNP positive patients with increased mortality | 0.0205 |
| NT-proBNP retains PCT positive patients with increased mortality | 0.0372 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darche, F.F.; Biener, M.; Müller-Hennessen, M.; Rivinius, R.; Stoyanov, K.M.; Milles, B.R.; Katus, H.A.; Frey, N.; Giannitsis, E. Low-Level Elevations of Procalcitonin Are Associated with Increased Mortality in Acute Heart Failure Patients, Independent of Concomitant Infection. Life 2021, 11, 1429. https://doi.org/10.3390/life11121429
Darche FF, Biener M, Müller-Hennessen M, Rivinius R, Stoyanov KM, Milles BR, Katus HA, Frey N, Giannitsis E. Low-Level Elevations of Procalcitonin Are Associated with Increased Mortality in Acute Heart Failure Patients, Independent of Concomitant Infection. Life. 2021; 11(12):1429. https://doi.org/10.3390/life11121429
Chicago/Turabian StyleDarche, Fabrice F., Moritz Biener, Matthias Müller-Hennessen, Rasmus Rivinius, Kiril M. Stoyanov, Barbara R. Milles, Hugo A. Katus, Norbert Frey, and Evangelos Giannitsis. 2021. "Low-Level Elevations of Procalcitonin Are Associated with Increased Mortality in Acute Heart Failure Patients, Independent of Concomitant Infection" Life 11, no. 12: 1429. https://doi.org/10.3390/life11121429
APA StyleDarche, F. F., Biener, M., Müller-Hennessen, M., Rivinius, R., Stoyanov, K. M., Milles, B. R., Katus, H. A., Frey, N., & Giannitsis, E. (2021). Low-Level Elevations of Procalcitonin Are Associated with Increased Mortality in Acute Heart Failure Patients, Independent of Concomitant Infection. Life, 11(12), 1429. https://doi.org/10.3390/life11121429