1. Introduction
Thumbs are a critical element of human hands as they facilitate dexterity when humans grasp small objects. In general, combination movements involving the thumb and other fingers cover 40% of complete hand movements [
1]. Consequently, patients who lose thumb movement functionality find it challenging to perform daily life activities. Owing to their functional importance, the rehabilitation and grafting of thumbs are of high priority. As a type of therapy, physical rehabilitation aims to recover the movement function of human body parts. Specifically, an external force is used to stimulate the body motor systems of impaired parts. Usually, the therapist provides the required external force during therapy, the magnitude of which depends on the degree of paresis of the patient. The rehabilitation effect depends on various factors such as the detection time of the disease, attitude of the patient, and engagement of the therapist. In particular, the therapist’s engagement with the patient is related to the number of therapy sessions. However, the treatment time is very limited even if the therapists can provide the patients with complete engagement (Only 5.2% in the two weeks [
2].) In addition, the number of young therapists is decreasing due to the aging of society [
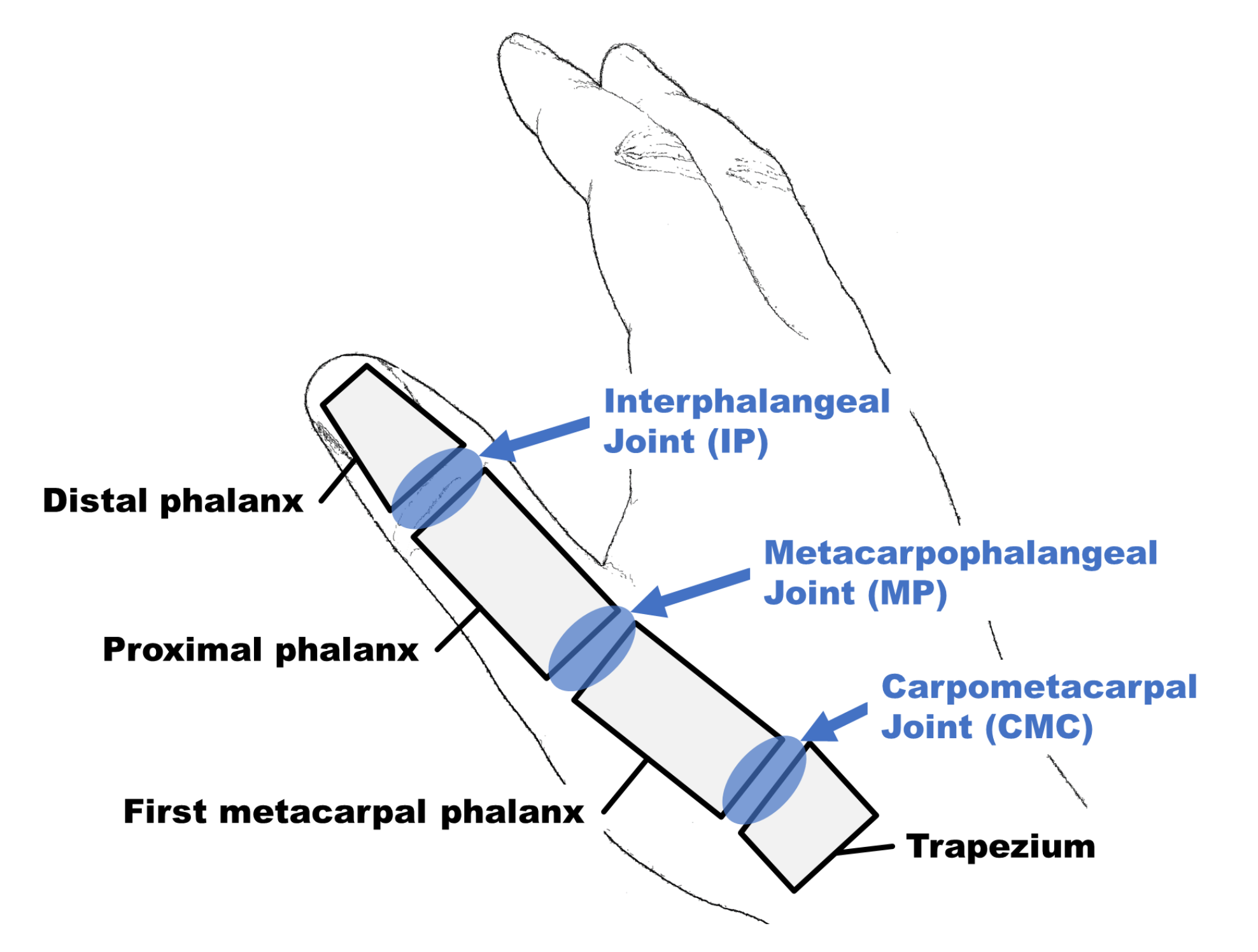
3]. Therefore, measures to address the lack of therapists are being widely researched in various domains. As a potential solution, rehabilitation robots have been introduced. Because robots do not experience fatigue, rehabilitation robots can provide continuous and consistent external force. In general, the human thumb consists of three joints, namely, the interphalangeal (IP) joint, metacarpophalangeal (MP) joint, and carpometacarpal (CMC) joint, as shown in
Figure 1. When the hand is in the anatomically resting position, the thumb MP joint axis is oriented approximately
to the MP axis of the other finger [
4]. The thumb exhibits five movements, namely, abduction, adduction, flexion, extension, and opposition as shown in
Figure 2. Abduction refers to the movement of the thumb moving away from the palm from its resting position. In detail, two kinds of abduction exist regarding the thumb direction [
5]. The palmar abduction is the thumb movement wherein the thumb moves perpendicular to the palm. The radial abduction is the movement wherein the thumb extends away from the palm’s surface. In this paper, abduction refers to radial abduction. Adduction is the movement of the thumb making it aligned with the palm plane. Flexion is the bending movement of the thumb from the resting position to the surface of the palm. Extension is the movement of the thumb from the flexion state to the resting position. Opposition is the movement of the thumb’s tip to the tip of the other fingers. Because the role of the CMC joint is the same in opposition and flexion, the movements are jointly termed as flexion in this work. In terms of the continuous movements such as adduction-abduction (AA) and flexion-extension (FE), the role of the AA is to control the position of the thumb, and FE serves to grasp an object. These roles can be easily visualized considering the situation of catching a ball in one hand.
The thumb’s CMC joint exhibits a biconcave-convex surface between the first MP phalanx and trapezium. This joint is usually known as a saddle joint owing to its saddle-like shape. Owing to this shape, an additional sliding movement occurs when the thumb moves. This sliding movement is not independent of the thumb movements; and thus, although the number of degrees of freedom (DOF) of the thumb is 2, the sliding motion has an effect of the position of the thumb. Previous studies of rehabilitation robots, exoskeleton type, and end-effector type, were reported [
6]. Specifically, in the exoskeleton type, the robot was attached to the human body, and the actuator axis was aligned to the axis of the human joints sequentially. The end-effector type is a mechanical design that connects the mechanism’s end-effector to the fingertip, but the base of the device is far from the body.
In previous studies, the most frequently used type of thumb rehabilitation robot was the exoskeleton. These existing researches pertaining to the thumb can be divided into three categories depending on the consideration of the thumb DOF [
7,
8,
9,
10]. In the first approach, one DOF is fixed, and the actuator controls the other. This mechanism is primarily designed to control the FE movement, which, as mentioned previously, is more important than the AA movement. However, this method cannot be used to provide the complete range of DOF of the CMC joint. In the second approach, the actuator controls one DOF, and the other DOF is implemented through a passive joint. The complete range of DOF of the CMC joint can be considered. However, most rehabilitation users are patients with paresis. In general, the impaired limbs easily exhibit flexor motions (bending), and the patient cannot control their fingers well. Therefore, the passive DOF is fixed in the direction of the paralyzed side. Due to this, the motion of the controlled DOF may be disrupted by the paralysis of the passive DOF. Because of the disruption caused by the passive DOF, the range of DOF may decrease or be completely blocked. Considering this situation, this method may not be able to provide adequate control for the whole thumb movement. Therefore, this design is not suitable to be applied for rehabilitation purposed. In the third approach, the two DOF are controlled by two actuators. Each actuator adapts one DOF. However, the aforementioned sliding movements are not considered.
Furthermore, the exoskeleton type has an issue called misalignment. Misalignment occurs when there is a mismatch between the axes of the human joint and the kinematic joint. In this situation, the actuator of the rehabilitation robot may provide an uncontrolled force to the user’s finger, leading to a high possibility of injury. It is a very critical problem for the safety of the users. As a solution to this issue, mechanical linkage designs (redundant linkage [
11,
12], remote center of rotation mechanisms [
13,
14,
15,
16], and serial linkage mechanisms [
8,
9,
10]) were reported. However, these linkages only considered the other fingers. Therefore, these designs cannot be considered for thumb rehabilitation due to the difference in DOF and CMC joint complexity. Even if the mechanism would be designed to suit of the DOF of the CMC joint, there is a possibility that the complexity of the mechanism would increase significantly because of the narrow space of the hand.
On the other hand, the end-effector type was designed such that its attachment part is connected to the tip of the finger, and the mechanism’s joints do not control each finger joint angle. For this reason, the consideration of misalignment is not necessary because this mechanism’s design does not align its kinematic joints with the finger joints [
6,
17]. This mechanism design provides several advantages. One such advantage is that this mechanism can easily adapt to the different sizes of various patient hands. Furthermore, the attachment part does not have a heavy weight because its base part, where the heaviest part of the mechanism is located, is usually installed on a table or stand. However, this type of mechanism results in a lower mobility than the exoskeleton type. Furthermore, the attaching point is mostly the distal part of the finger, and sensitive control for the individual finger joint angles is difficult.
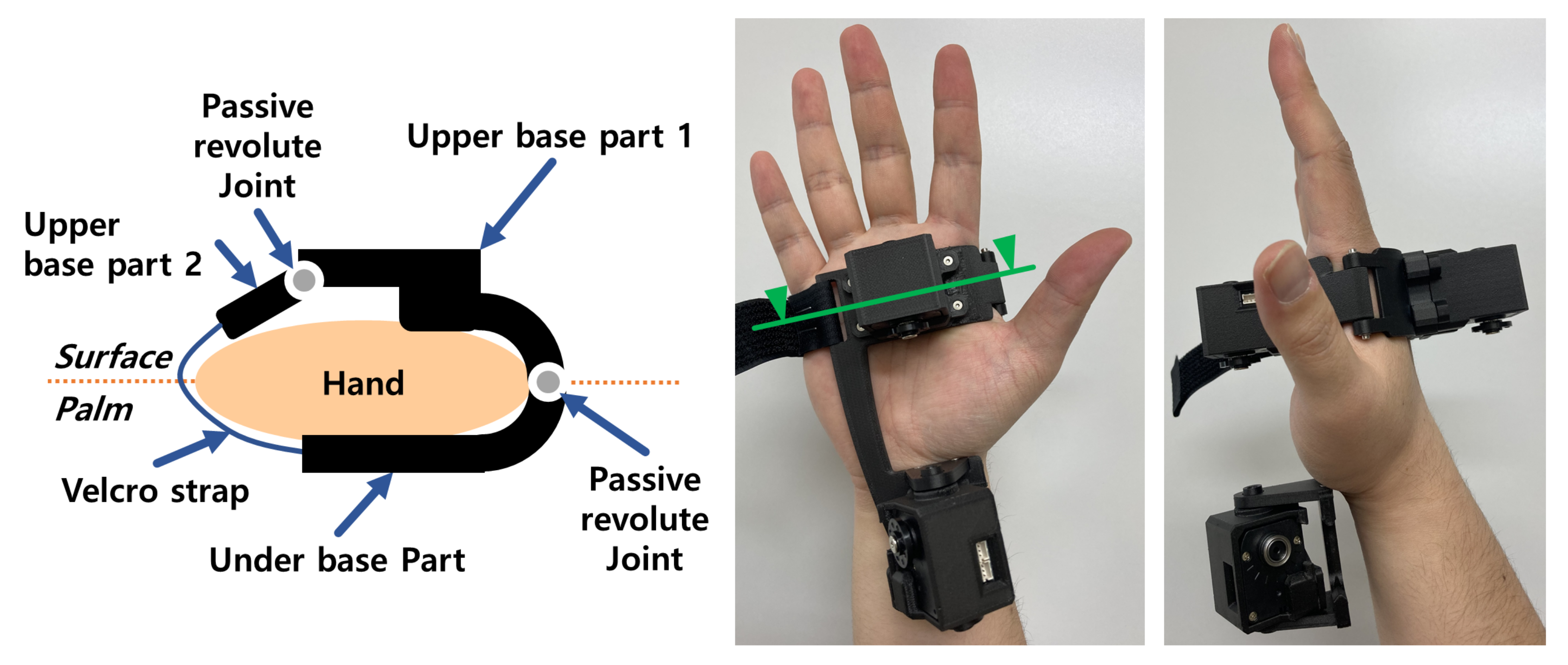
In summary, the sliding motion of CMC joint should be considered for providing accurate finger movement to develop a thumb rehabilitation robot. Furthermore, the mechanism is required to be designed so that it does not exert an unexpected force in order to maintain user safety. A hybrid mechanism, combined with the advantage of the exoskeleton and end-effector types, is proposed as an idea for the mechanism. In detail, the design is considered so that multiple linkages connecting only to the attachment point are designed, similar to an end-effector type mechanism, and the base parts of the mechanism are designed to be attached to the hand like an exoskeleton type.
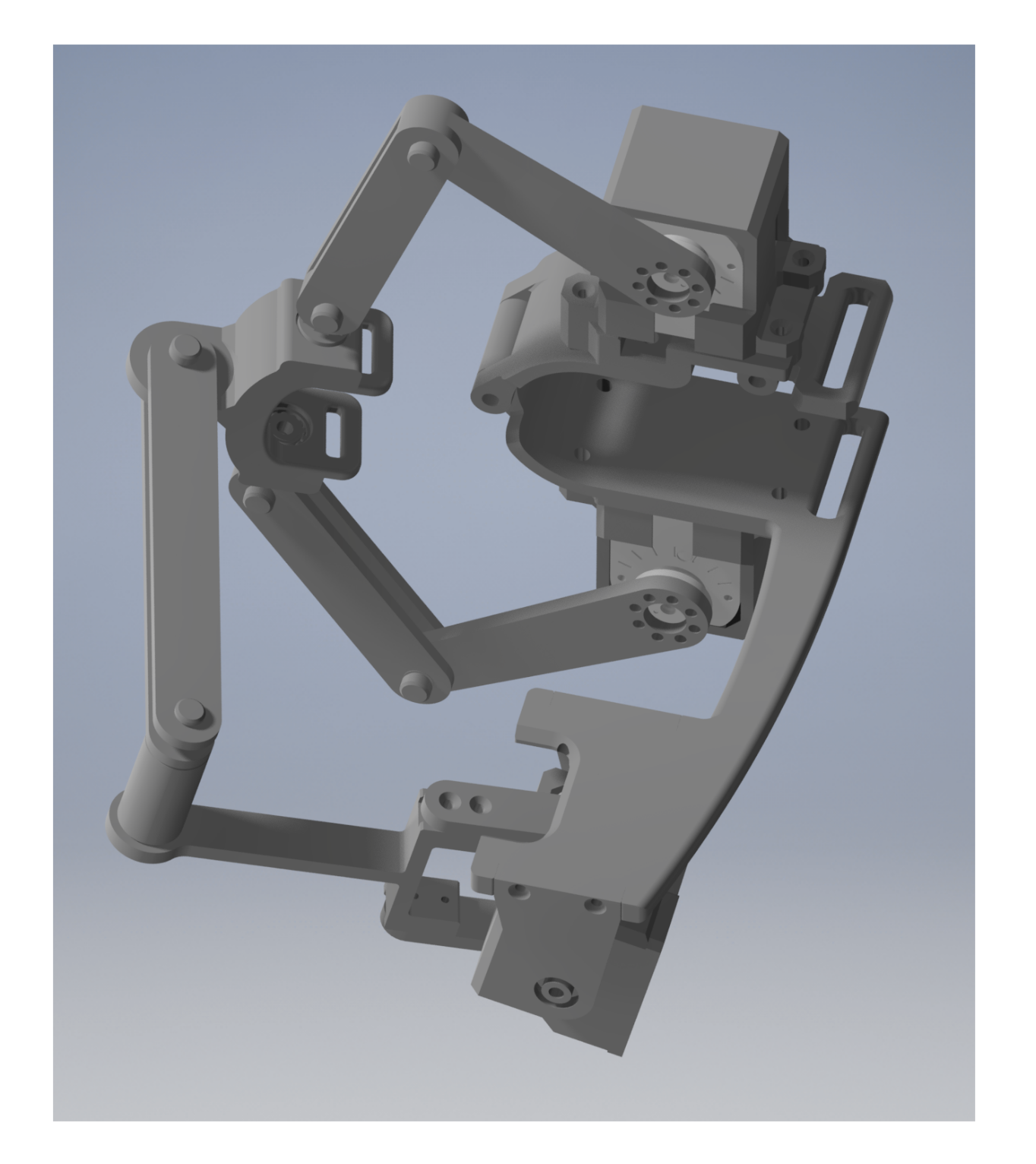
Moreover, it is necessary to perform an ergonomic design to ensure that the patient’s hand does not feel uncomfortable and adapts their hand size. Therefore, some parts would be better to be designed by many curve-linear forms, complex shapes, and tiny sizes. Thanks to the recent progress of the Additive Manufacturing (AM), fabrications of these parts are enabled at low cost. For this reason, some parts will be designed to consider the manufacturing by AM in this research.
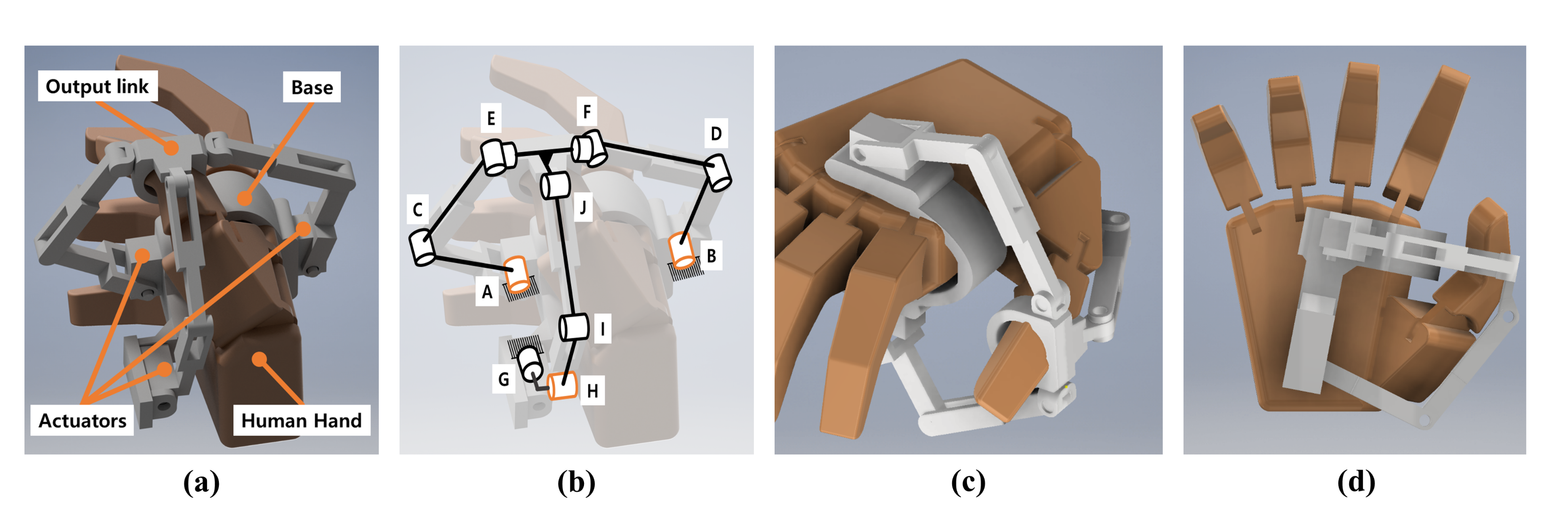
Based on this concept, a (2–RRU)–URR parallel mechanism is proposed, as shown in
Figure 3 [
18,
19,
20]. This mechanism is an overconstrained mechanism, with three DOF. The mechanism can output two rotational DOF and one translational DOF. The proposed mechanism consists of three chains, the output link, and the base. Structurally, the first and second chains are connected with the output link through a universal joint. The third chain is connected with the output link through a revolute joint. In previous work [
18,
19,
20], we reported the basic kinematics such as mobility, displacement, workspace analysis, and static analysis for calculating the actuation torque against the external load on the output link. In detail, a numerical example was used for calculating each analysis for the confirmation of the kinematics. Furthermore, the static analysis of the proposed mechanism had been confirmed through an experiment with the experimental apparatus. Through the results of the previous works, the kinematic characteristics were confirmed for the design of the mechanism. However, because the proposed mechanism being designed for thumb rehabilitation, the mechanism design should take into consideration the human measurement data, which provides kinesiological/anatomical information. Moreover, the proposed mechanism is designed to be attached to the hand. To realize the implementation of the proposed mechanism, user experiments are necessary.
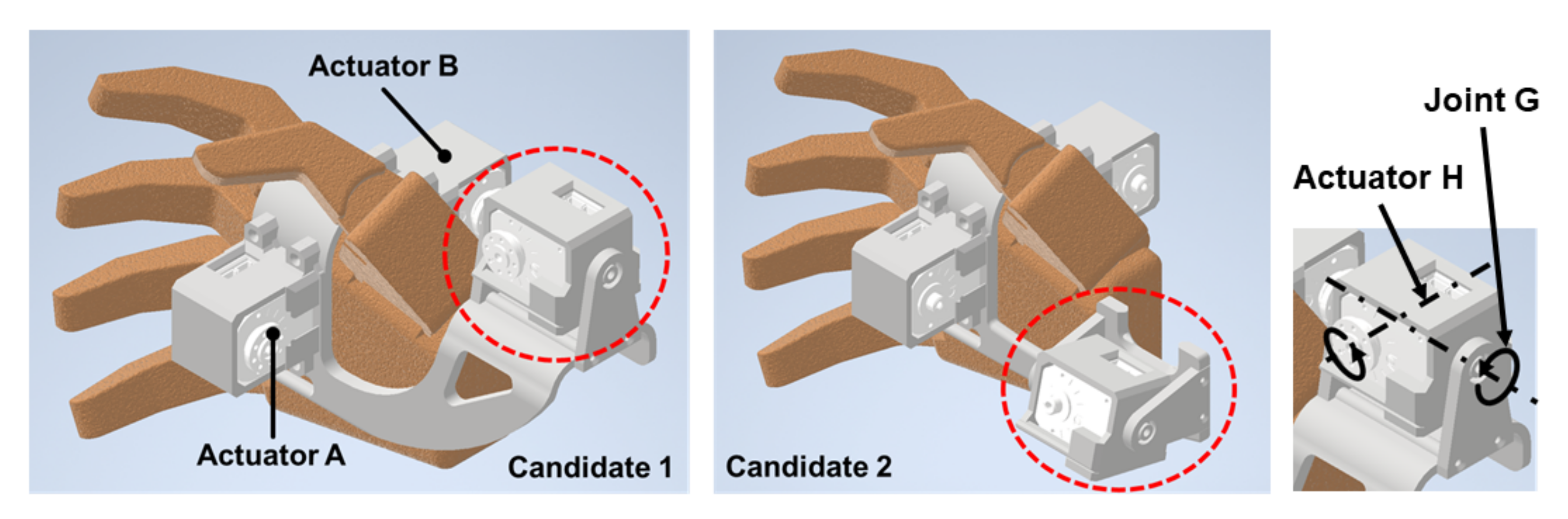
In this paper, we discuss the geometric design, prototyping, and user test results taking into consideration the application of the mechanism for thumb rehabilitation therapy based on the methods of analysis from the previous works of [
18,
19,
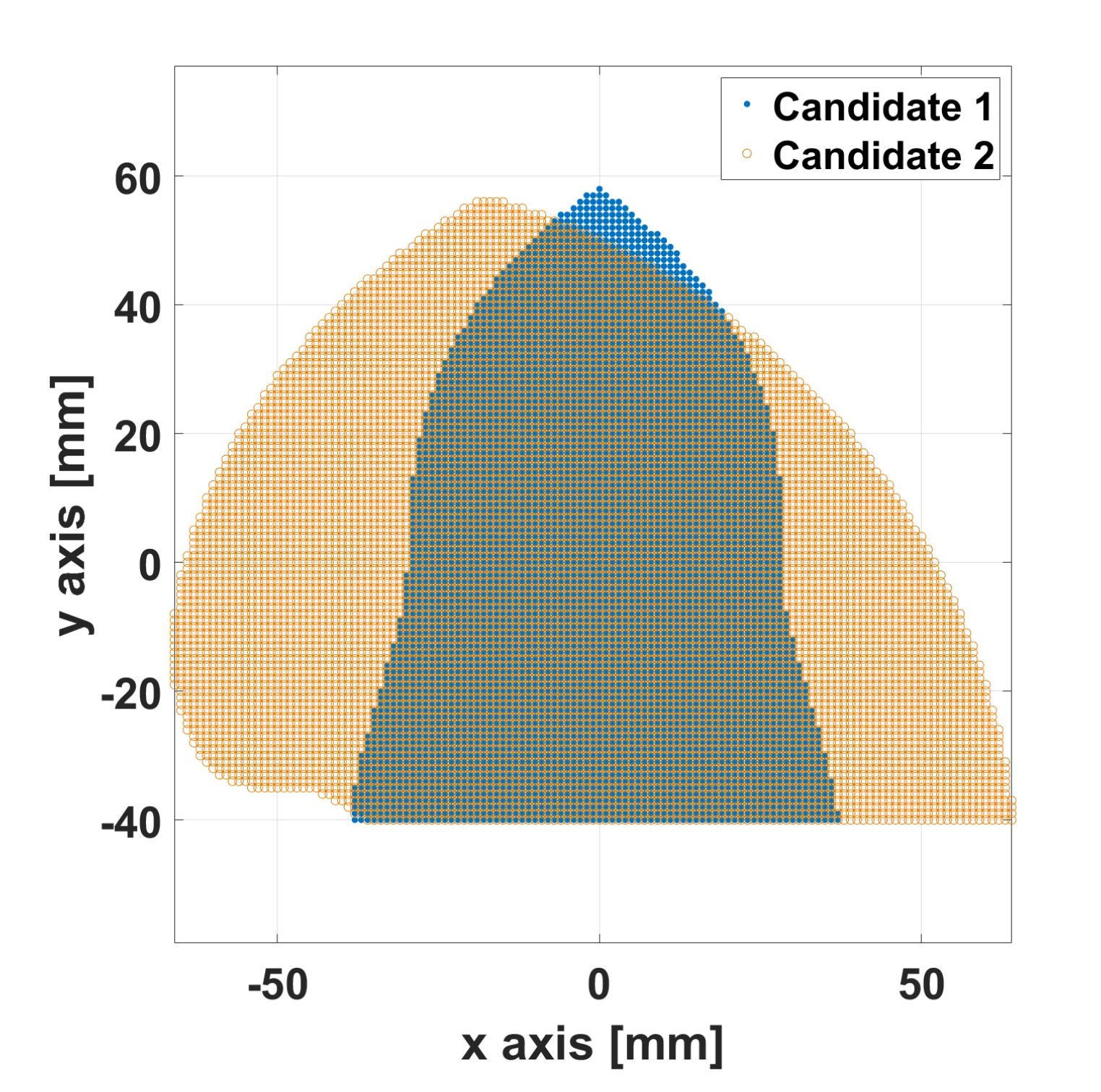
20]. The thumb trajectory was measured through a motion capture system to determine the target workspace and the required range of the thumb orientation angle. The motion capture system used is an optical type, which uses passive markers with an infrared light camera. Because this system does not necessarily install encoders with the actuators, the weight of the proposed mechanism can be reduced. Furthermore, it can measure the points located in the narrow space through the estimation of the center points between two markers. Collisions between the finger and mechanism may occur accidentally. This causes damage of the finger, and it affects the range of the workspace. For this reason, avoiding collision is considered in the design process. To avoid collisions and secure the workspace, the design considerations such as the placement of the actuator and the inclusion of link offset must be considered. For this reason, two candidates of mechanism design are considered in this paper. Each candidate has a different placement of the actuator. Because the workspace is affected by the actuator’s placement, each workspace has a different range, even those set with the same design variables. To select a suitable candidate, two reachable workspaces are compared. The candidate, which has wider workspace than the other was chosen. The suitable link length of the prototype was determined through the coverage of the effective workspace in the target workspace. Considering these aspects, the prototype was manufactured and the user test was conducted considering AA and FE movements.
2. (2–RRU)–URR Parallel Mechanism and Its Analysis Methods
In the design process of this paper, the analysis methods that are reported from previous works [
18,
19] are used. To help understand the contents of the paper, the mechanism explanation and the kinematic analysis are described briefly in this section.
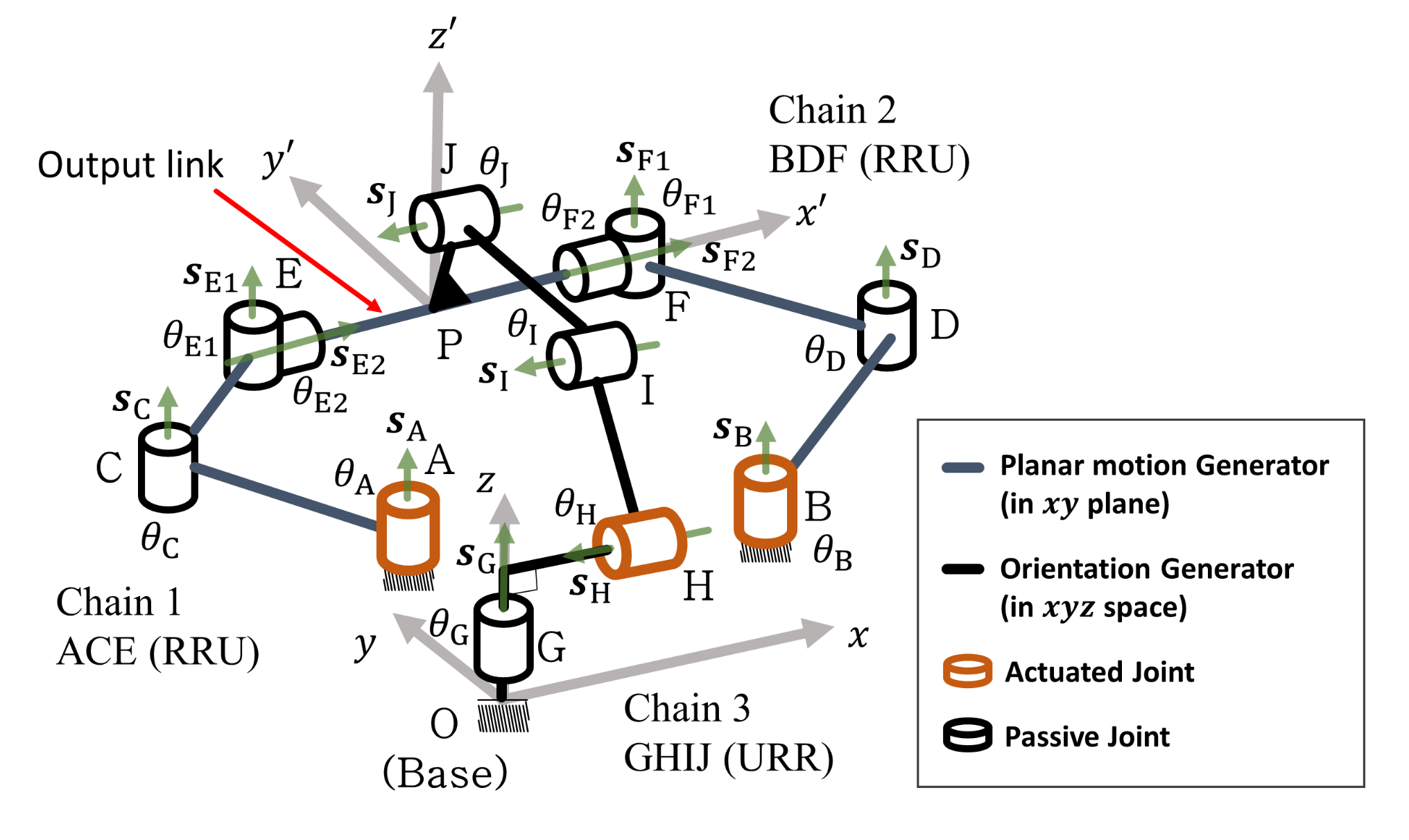
The (2–RRU)–URR parallel mechanism is shown in
Figure 4. In this Figure, chains ACE, BDF, and GHIJ are denoted as chains 1, 2, and 3, respectively. The number of DOFs for this mechanism is zero, as calculated using Gruebler’s formula. However, this mechanism actually exhibits three DOFs and this can be confirmed from the constraint wrenches [
18]. Hence, this mechanism is categorized as a lower-mobility overconstrained mechanism. Furthermore, the proposed mechanism is composed of two planar chains, namely the planar motion generator (PMG: ACEFDB in
Figure 4) and orientation motion generator (OG: OGHIJP). The PMG has formed the planar 6-bar linkage and The OG has formed the planar 4-bar linkage. for this reason, the kinematic analysis of each generator can be performed based on the planar kinematics [
18,
19]. As the mobility of this mechanism, the rotational mobility is along
-axis, the rotational mobility is along
z-axis, and the translational mobility is along the
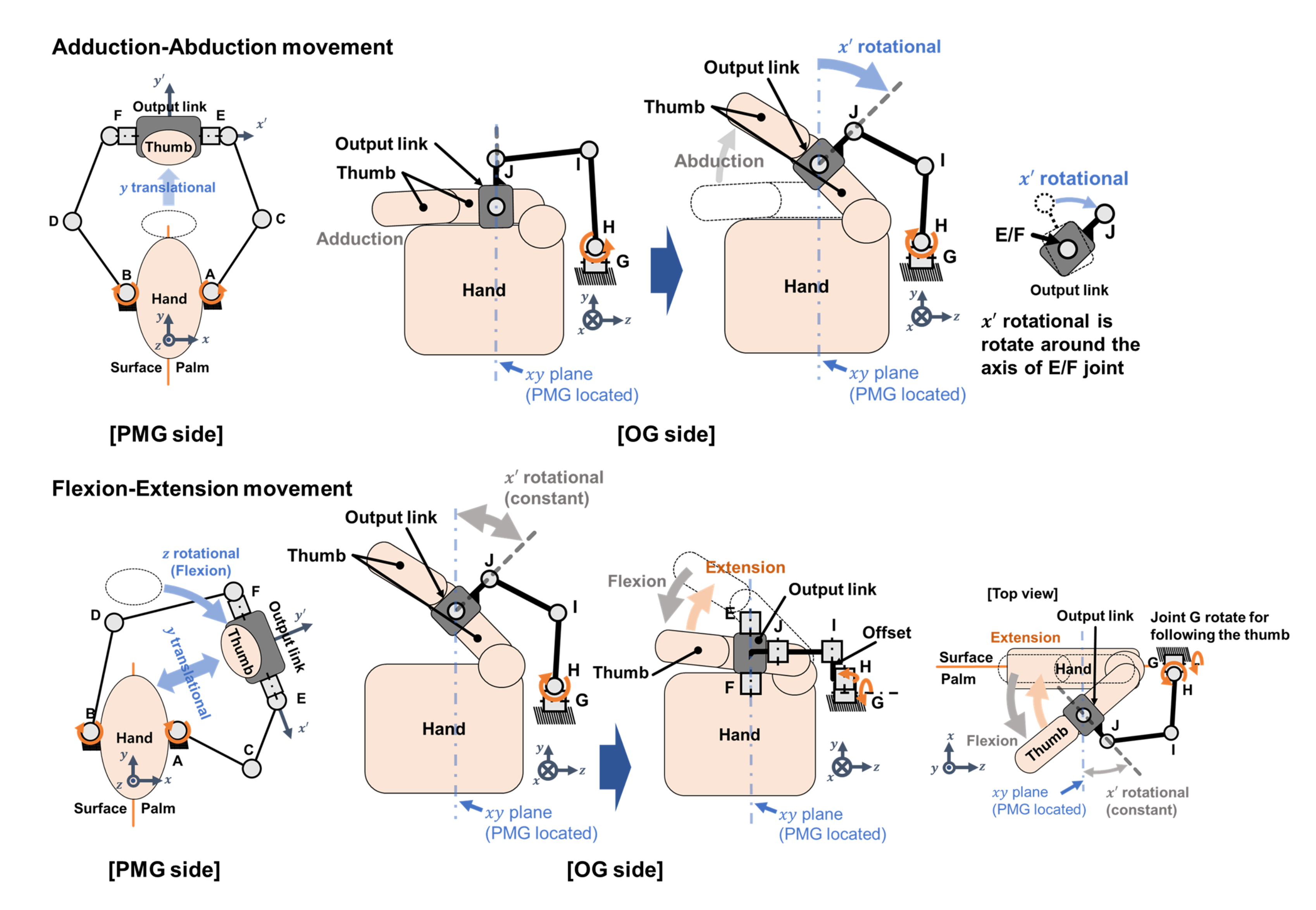
y-axis. The mechanism achieves the target movement of AA and FE, by combining the three mobilities of the mechanism for the target movement as shown in
Figure 5. In the case of AA, when the thumb is far away from the palm, and returns, its thumb position is controlled by the
y translational mobility. Simultaneously, the orientation of the thumb is changed, and this orientation is controlled by the rotational mobility along the
-axis. Regarding the FE movement, assuming that the orientation angle is not changed, the rotation mobility along the
-axis is set as constants. Furthermore, the thumb position is controlled in the
plane by combining motion from two mobilities of the rotational mobility along the
z-axis and the translational mobility to the
y-axis.
Through these structural characteristics, the proposed mechanism can simply assist the thumb motions by controlling the attachment point like an end-effector type, and the complex motion of the CMC joint is not considered. However, because the attachment point is in the Proximal phalanx of the thumb finger, the motion of IP joints could not control. Moreover, the thumb finger’s sliding motion may occur depending on the size of the hand due to the controlled motion provided in the plane.
4. User Experiments
Because the proposed mechanism is to be applied for rehabilitation therapy, it was necessary to verify the presented movement while considering the effect on the human hand. In the experiment, each volunteer’s planned trajectory and the range of the required orientation angle were used to control the prototype. When the output movement of the prototype is following through the input trajectory, we assume that the prototype has the feasibility of the thumb rehabilitation robot. For this reason, the control of the prototype for two movements were done and the position of the output link was measured. After measuring, the experimental data with the input trajectory was compared. Moreover, an experiment was conducted on publicly recruited volunteers to perform a performance evaluation and identify any unexpected problems by obtaining feedback through a questionnaire.
In the experiment, the two movements, namely AA and FE, were considered. To control the prototype, the thumb trajectory, which was measured with the motion capture system in
Figure 6, was used. The thumb data were measured before the experiment by using the prototype and these were also used in the determination of the target workspace of
Figure 8. The volunteers were briefed prior to the experiment regarding the thumb measurement. Moreover, these data were considered to be the target group and the measured thumb data were used for generating the planned path of the experiment. The planned path was an individual path for each user and did not use the same path for other users. Before the experiment, the user was asked to sit near the camera of the motion capture system, and the prototype was attached to his/her right hand. The movement was provided by the prototype to the user five times, for each movement.
Figure 20 shows the experimental scenario. Because the results of the experiment were not expected to be influenced by factors such as the temperature and humidity of the room, these factors were not limited. To measure the trajectory of the prototype performance, motion markers were attached to the prototype during the experiment.
Figure 21 shows the attached markers on the prototype. The measurement point is the middle point of four markers: 8, 9, 10, and 11. In the experiment, the following safety clauses were implemented:
The torque of the used actuator was less than that of the thumb.
To prevent damage to the human body, mechanical and electrical safety measures were implemented, such as the installation of electrical circuits to prevent overload and electrical back-flow.
Two emergency stop switches were used. The first emergency stop switch was provided to the users to stop operation during the experiment if they felt any pain or discomfort. The second switch was installed for the organizer of the experiment to stop the operation of the device.
Figure 20.
Concept of the experimental scenario.
Figure 20.
Concept of the experimental scenario.
Figure 21.
Measurement markers on the prototype in the experiment.
Figure 21.
Measurement markers on the prototype in the experiment.
The experiment scenario and safety clauses were approved by the research ethics committee of Tokyo Institute of Technology (Registration number: A19190).
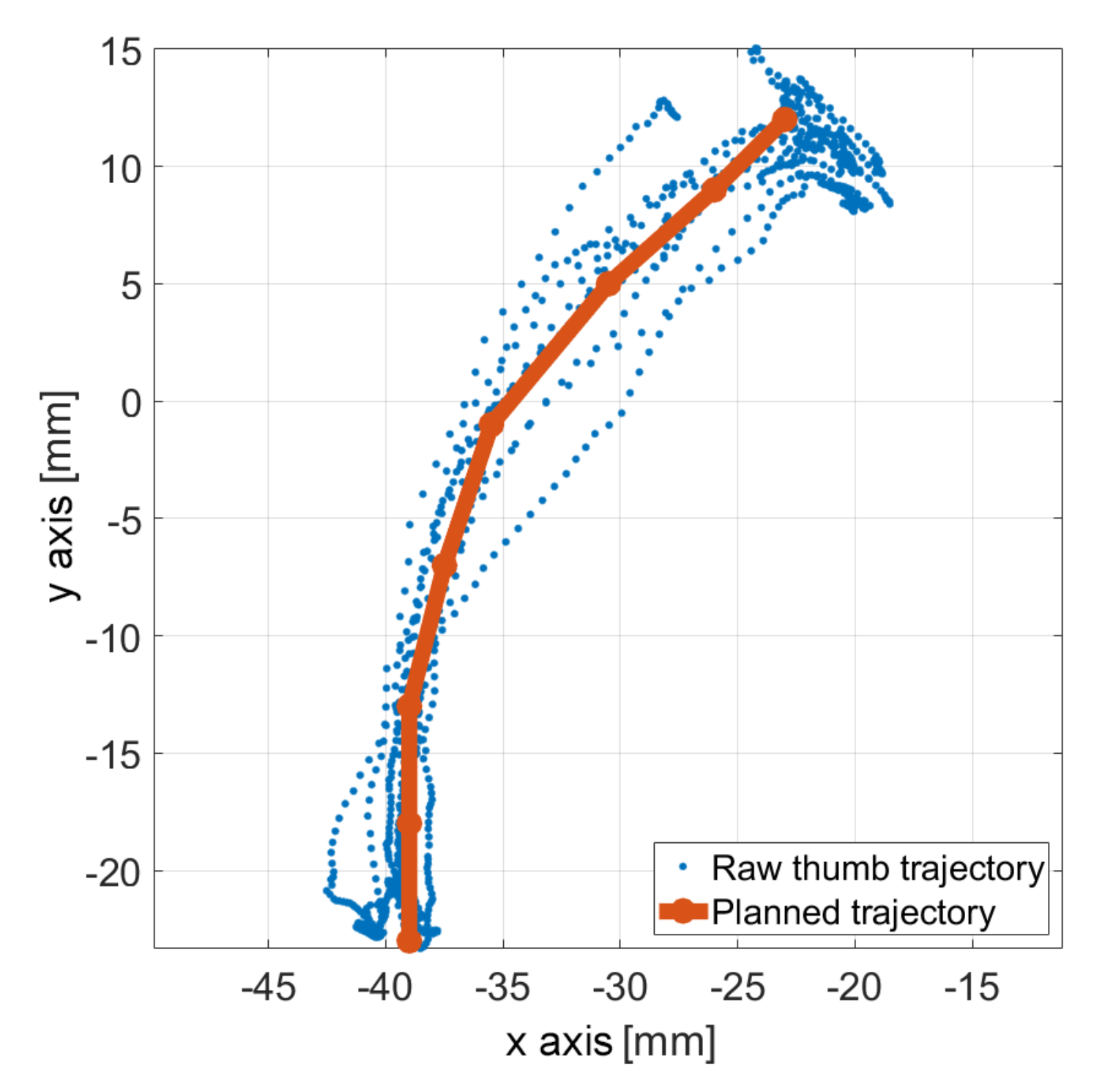
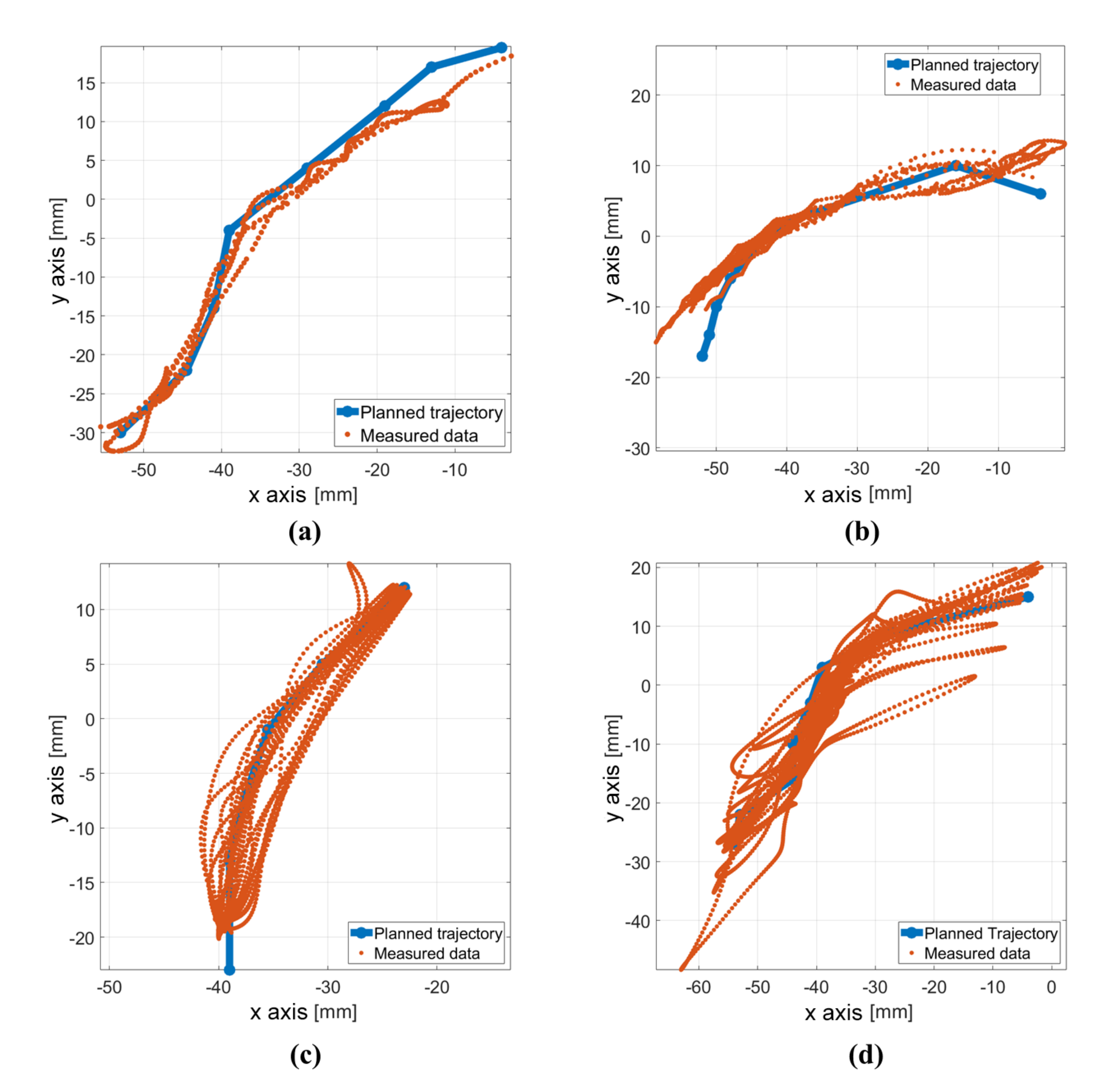
Figure 22 shows the experiment results pertaining to the FE movement of four users which was controlled using the prototype. These experiment data were measured as three-dimensional data using the motion capture system. Because the reachable workspace was located in the
plane, the figures are shown in the
plane. The blue dot and line represent the planned trajectory, which are generated from the thumb trajectory while the users did not have the prototype attached, and the orange dots correspond to the measurement data of the thumb trajectory provided by the prototype. In the figure, the orange dots indicate the difference from the planned trajectory (marked by the blue dots). From the result of
Figure 22, the position of the output link shows that the prototype generates a trajectory that is mostly similar to the planned trajectories. Thus, the prototype is capable of controlling the FE movement.
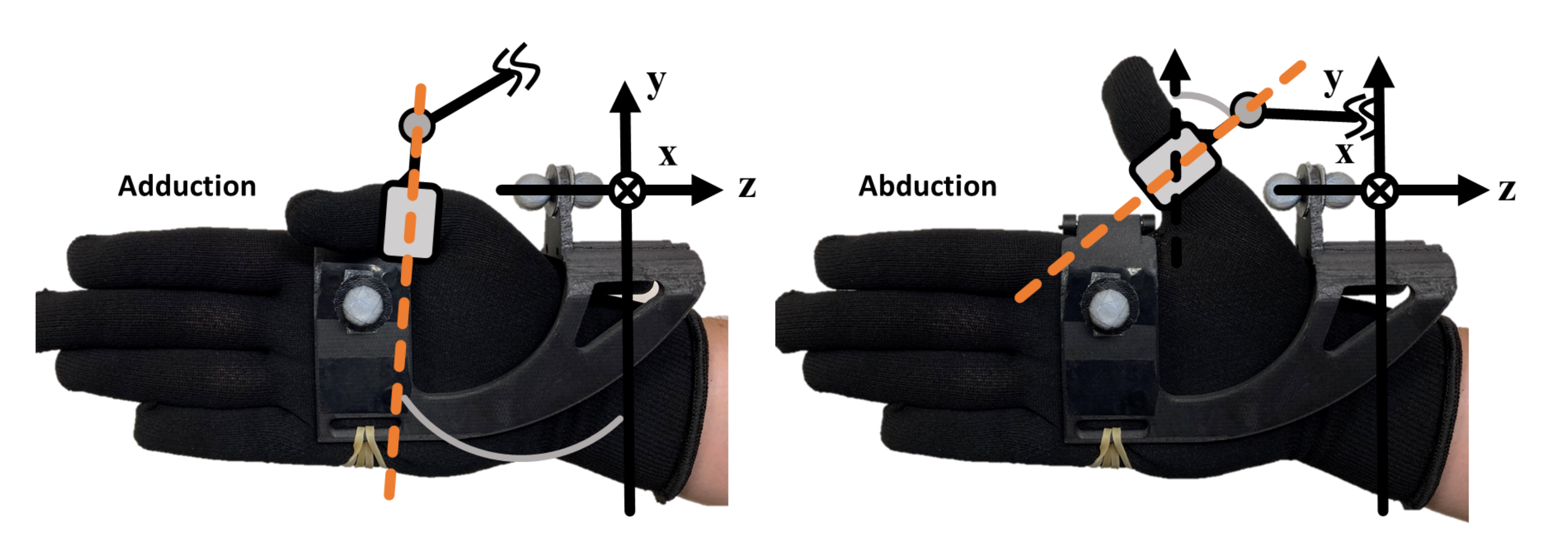
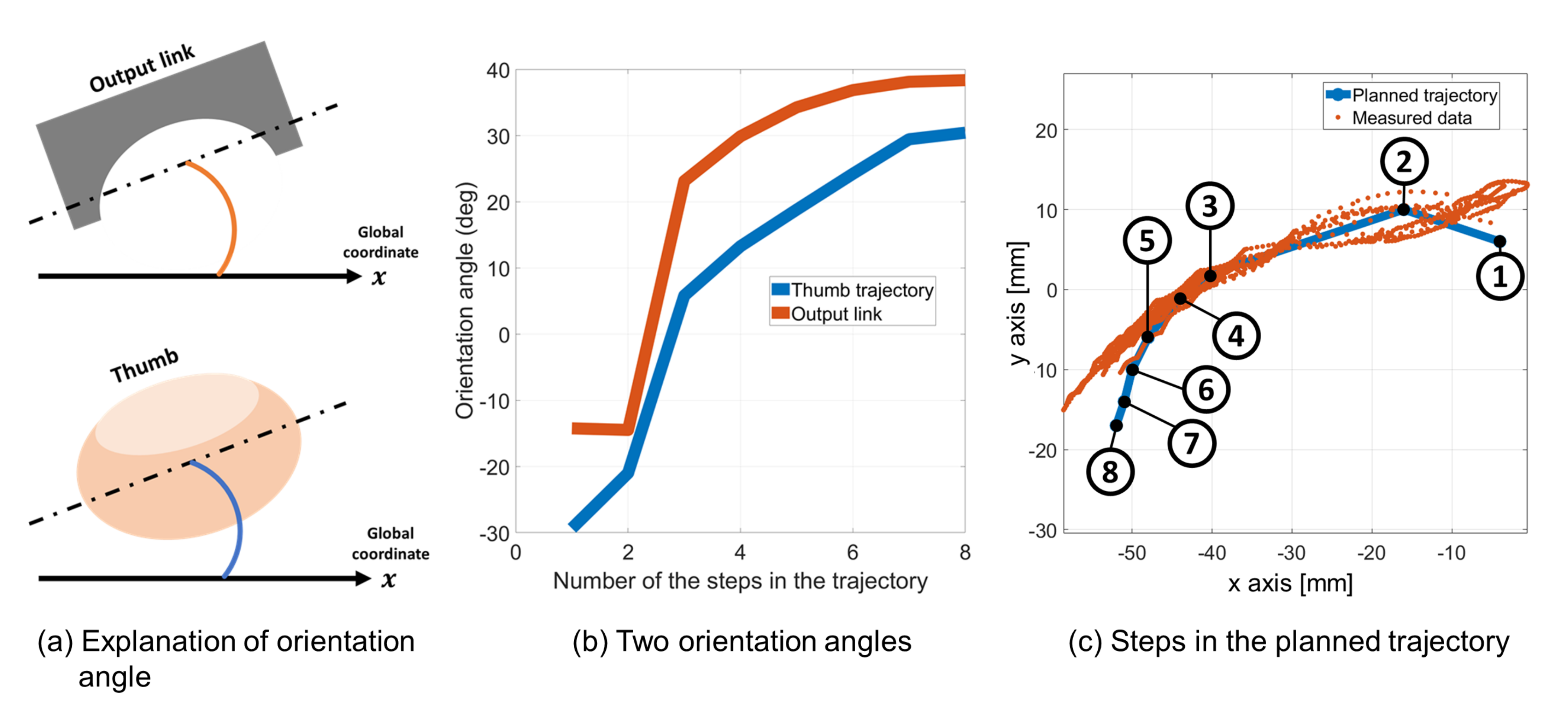
To confirm the FE movement in detail, the orientation angles around the
z axis in the
plane of thumb and output link were compared (this angle is not
).
Figure 23a shows the explanation of the two angles, and
Figure 23b shows the two angles: the blue line is the thumb orientation angle, and orange is the output link orientation angle. Those two data were not simultaneously measured, but the patterns of the movements and the trajectories are largely the same. From the result of
Figure 23, we know that relative motion, which is the sliding motion between hand tissue and bone, between the two angles exists. Therefore, we estimate that the relative motions occur between the output link and the base part. Because of the effects of the relative motion, the tip of the trajectory of the experiment is not expected to match well with the planned trajectory in the practical experiment shown in
Figure 22. To improve the accuracy of the generated trajectory, the relative motion should be reduced, which will be done in future work.
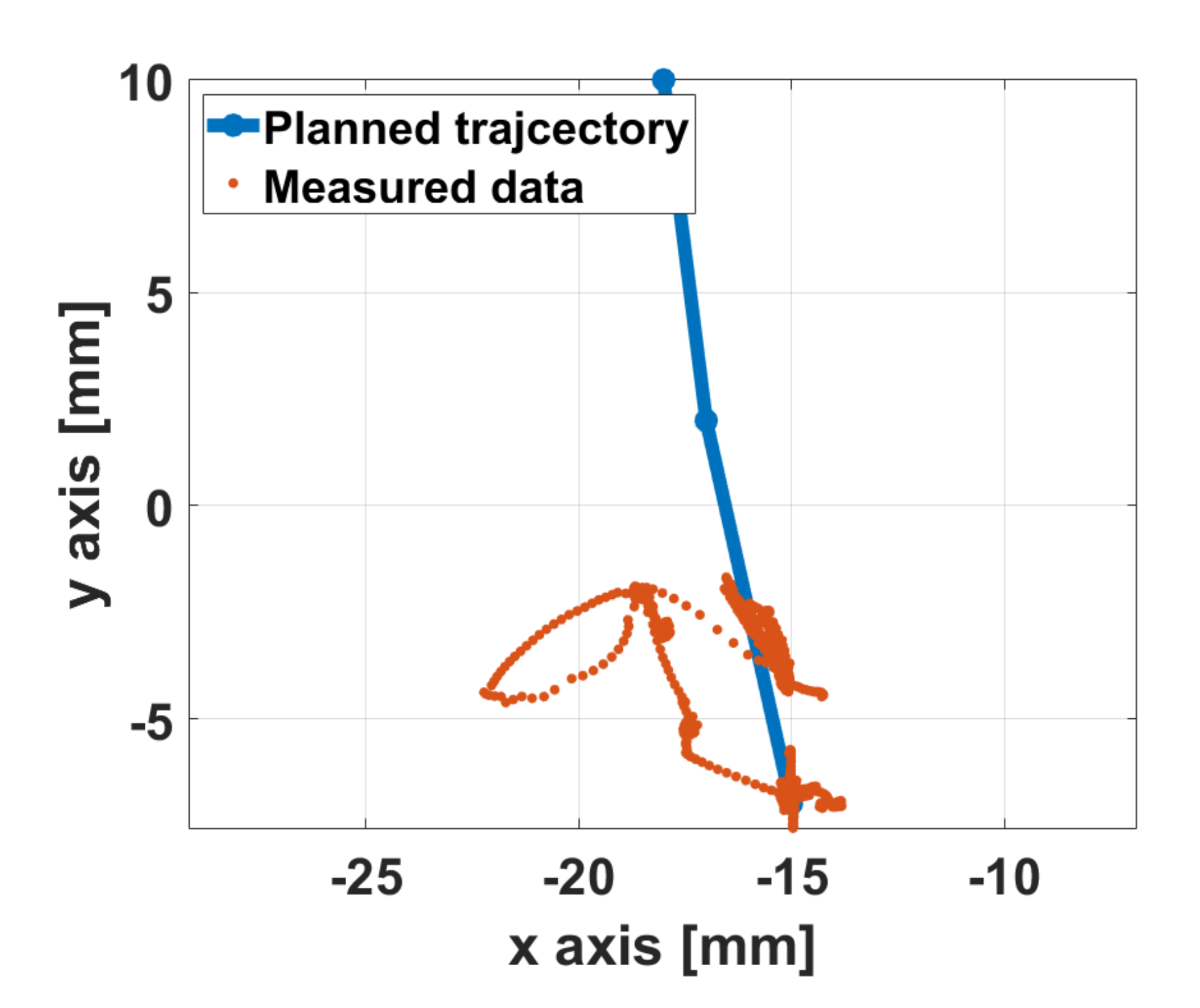
Figure 24 shows the results for the AA movement. The measured data are significantly smaller compared to the planned trajectory data. From this result, it is expected that the motion transmission from the actuator was not well done or the actuator did not work well. This means that the prototype moved in a small range and its behavior included vibratory motion.
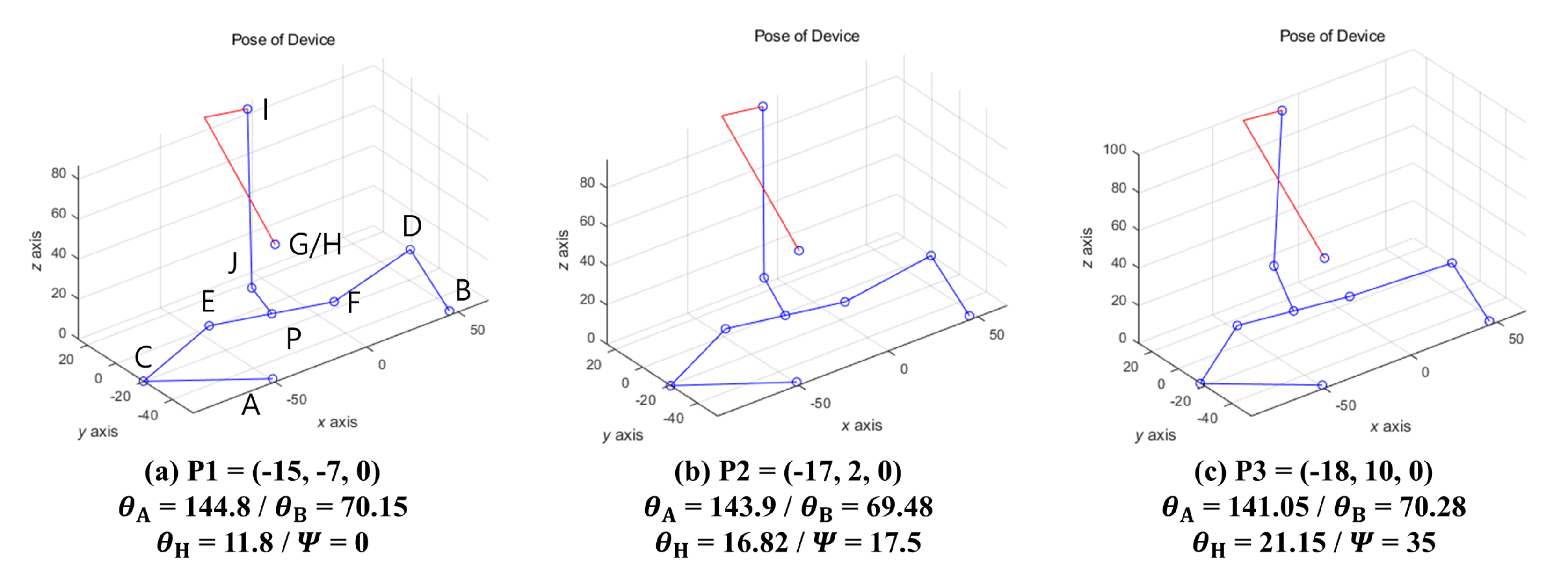
Figure 25 shows the simulation results for the planned trajectories of the above-mentioned example. The different sub-figures show the configuration of the mechanism when
P is assigned with respect to the planned trajectory shown in
Figure 24. It can be noted that actuation joint A does not change considerably from (a) to (c). This experimental result is expected due to the lack of torque.
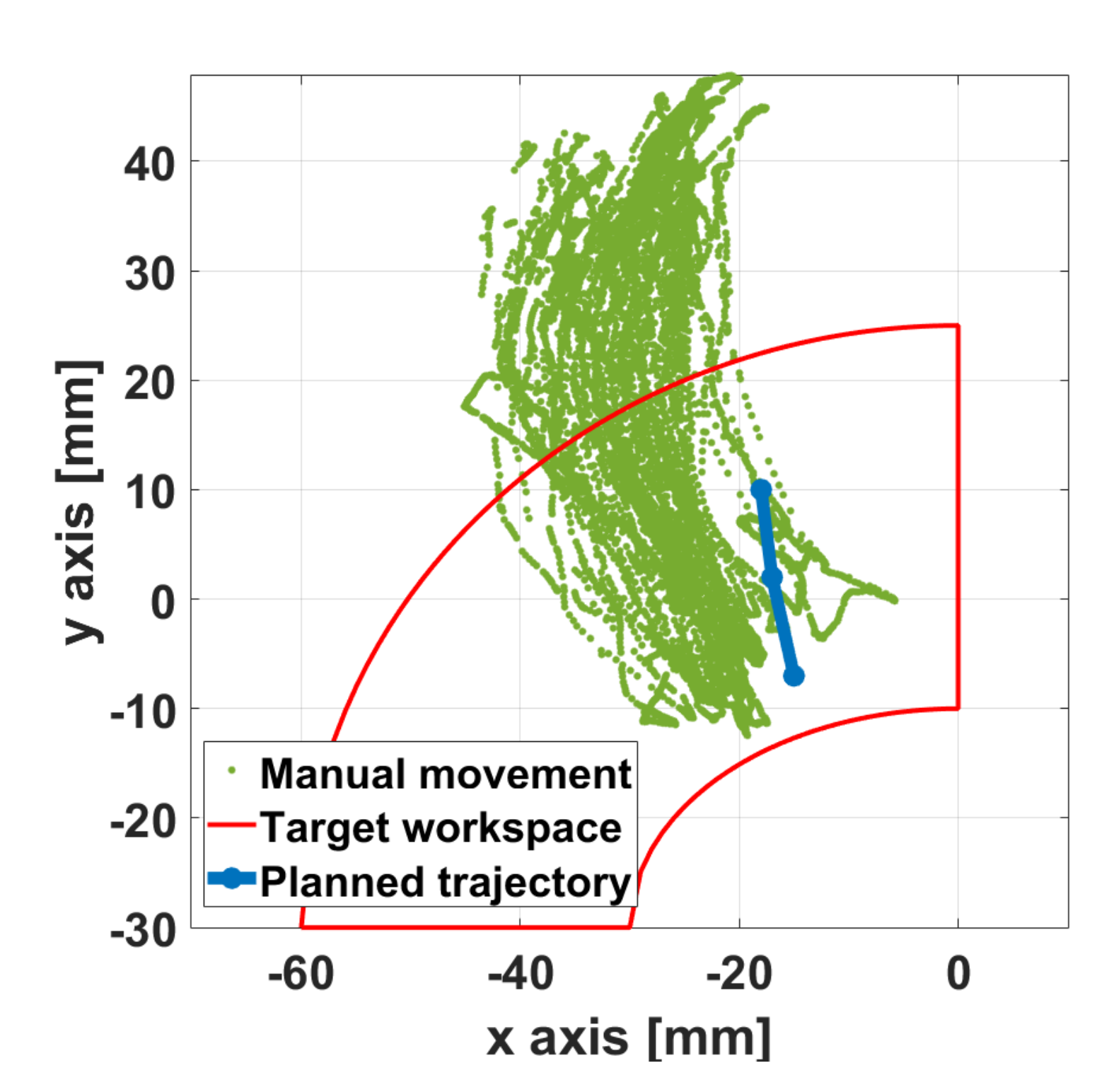
Because of the lack of actuator torque in the experiment of AA movement, a manual movement, which provides assistance to the actuators by hand without electric power, was carried out. This was a simple test done to confirm the prototype performance when the actuators have enough torque. When AA movement was performed, the result, the target workspace, and the planned trajectory are shown in
Figure 26. The green dots indicate the output link position of the measured data wherein the prototype was moved by assisting the actuator by hand. Because this data was obtained while moving the actuator by hand, it does not perfectly follow the planned trajectory. From this result, it can be seen that the measured data of the manual movement has a larger trajectory, and it protrudes from the range of the target workspace. Therefore, if the actuator is capable of enough torque output, the prototype is expected to be capable of controlling AA movement. As for future work, additional analysis of the required torque while considering the weight of the prototype for application of the thumb rehabilitation will be carried out.
5. Discussion and Conclusions
In this paper, the geometrical design, prototyping, and user test of the proposed mechanism were described to be adapted for application in thumb rehabilitation therapy. The proposed mechanism is a hybrid type, which combines the exoskeleton and the end-effector type mechanisms. The structural characteristics allow the thumb CMC joint’s complexity to not be considered in the mechanism design. The design requirements were determined such that the thumb rehabilitation’s proposed mechanism can be adapted to the anatomical and kinesiological information. The thumb trajectory was measured using an optical motion capture system to determine the target workspace. Two design candidates, which had different actuator placements, were considered in order to avoid collisions between the mechanism and hand. The sizes of the three workspaces (target workspace, the workspace of candidate 1, and the workspace of candidate 2) were compared while keeping the two candidates’ design variables the same. Because candidate 2 was found to have a wider workspace than candidate 1 while being able to cover the target workspace, candidate 2 was selected as a suitable design. Based on these considerations, a prototype was manufactured. To prove the suitability and performance of the mechanism for application in thumb rehabilitation, user tests were carried out. User testing was performed using the prototype on volunteers. The input data were determined from the results of the trajectory planning method. Two target movements were provided: FE and AA.
The user experiment with the prototype was carried out to verify the effectiveness of the prototype for the thumb rehabilitation therapy. In the experiment, two target movements were provided: FE and AA. The results for the FE movement were largely satisfactory following the planned trajectory. Because the tip of trajectories did not match with the input trajectory well, the relative motion between the thumb and output link was compared. The results showed that a relative motion exists in both ends of the trajectory and it causes a small effect on the control accuracy of the prototype. On the other hand, the AA movement cases were not satisfactory. To investigate these, a manual moving test of the prototype using the AA movement was done by assisting the actuators by hand. Through this test, it was shown that the range of the output trajectory was longer than the planned one, and it could cover the target workspace. Thus, the prototype has the potential to perform the AA movement. To sum up these findings, the prototype has the possibility to adapt for thumb rehabilitation though the prototype used in this paper has some limitations. To improve the proposed mechanism for thumb rehabilitation, actuation selection will be necessary by performing static analysis on the prototype. Future work on the mechanism design while considering the design factors calculated from the static analysis will be carried out.































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}