
Advancements in State-of-the-Art Ankle Rehabilitation Robotic Devices: A Review of Design, Actuation and Control Strategies



Abstract
1. Introduction
2. Materials and Methods
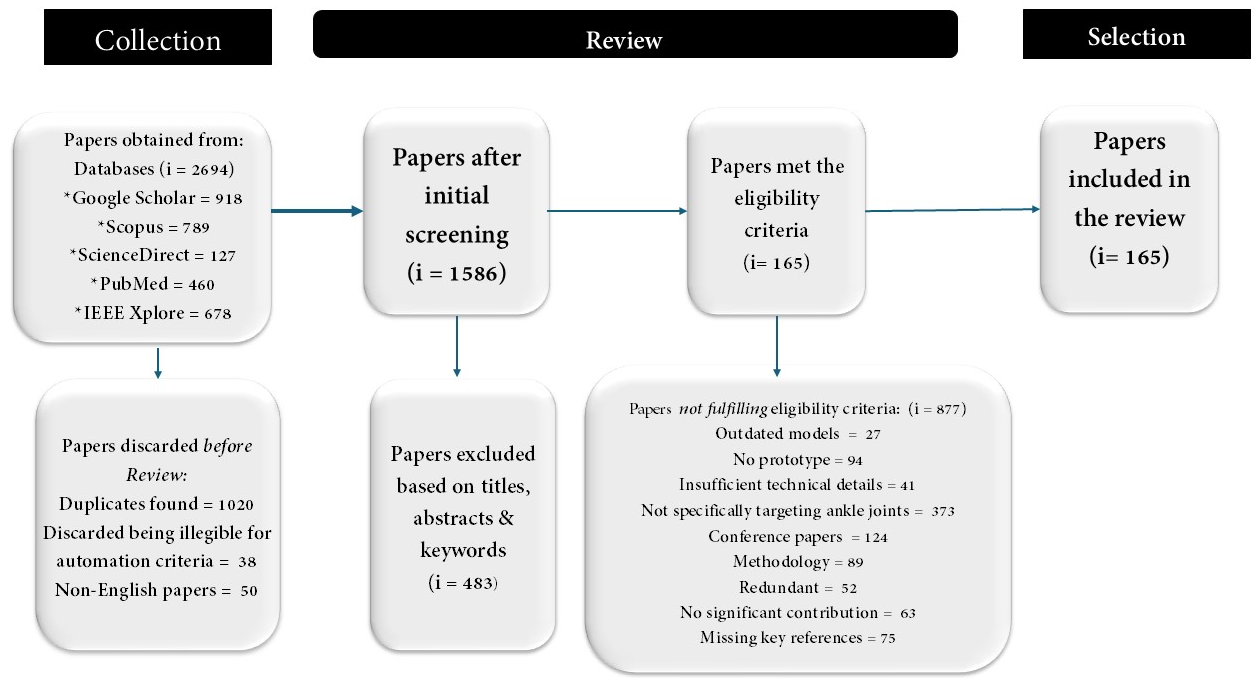
2.1. Methodology
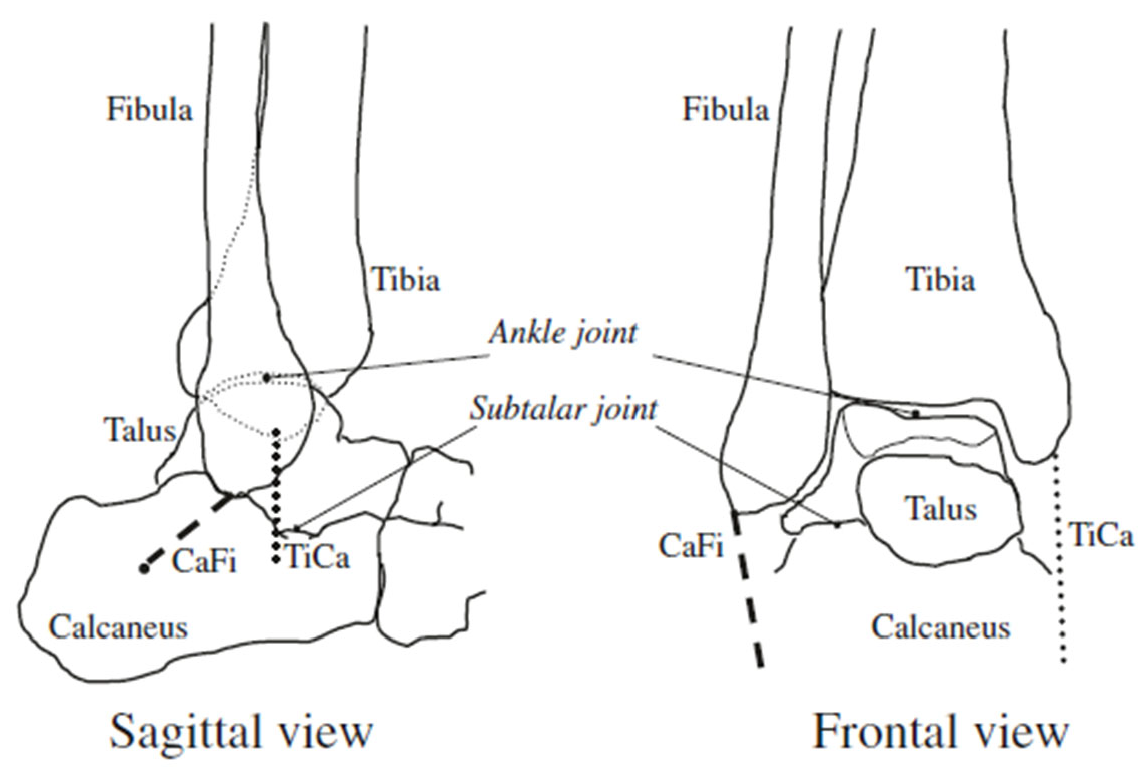
2.2. Anatomy of the Ankle Joint Complex
- Dorsiflexion/Plantarflexion: Motion in the sagittal plane. Motion of the foot upwards and towards the tibia is dorsiflexion. Motion of the foot downwards and far from the tibia is plantarflexion.
- Abduction/Adduction: Motion of the heel around its axis and parallel to the transverse plane. When the forefoot experiences lateral motion, it is abduction, and when it moves medially, it is called adduction.
- Inversion/Eversion: Motion along the anteroposterior axis and parallel to the frontal pale. Medial movement of the plantar surface is inversion, while lateral movement is eversion.
2.3. Ankle Rehabilitation Robots (ARRs) Classification
2.4. Ankle Rehabilitation Robot Design
2.4.1. Mechanical Architecture of Ankle Rehabilitation Robots
2.4.2. Wearable Ankle Rehabilitation Robots
2.4.3. Parallel/Platform-Based Ankle Rehabilitation Robots
2.5. Manufacturing Material
2.5.1. Rigid Ankle Rehabilitation Robots
2.5.2. Soft Ankle Rehabilitation Robots
2.6. Actuation Devices
2.6.1. Pneumatic Air Muscle Actuators
2.6.2. Electric Actuators
2.6.3. Series Elastic Actuators (SEAs)
2.6.4. Other Emerging Actuation Devices
2.7. Control Techniques
2.7.1. Trajectory-Tracking Control Methods
2.7.2. Assist-As-Needed (AAN) Control Methods
2.7.3. Adaptive and Intelligent Control Techniques
3. Results
Experimental Setup Evaluation and Clinical Outcomes
4. Discussion
4.1. Robot Design of Ankle Rehabilitation Robot
4.2. Actuation Methods
4.3. Control Techniques
4.3.1. Trajectory Tracking Controllers
4.3.2. Force and Impedance Controllers
4.3.3. Assist-as-Needed and Adaptive Controllers
4.4. Experimental Setup and Clinical Testing
4.5. Energy Efficiency
4.6. Future Challenges and Recommendations
- Not every patient suffering from ankle joint disorders or neurological diseases has quick and easy access to clinical therapy and experts. In future, ankle rehabilitation robots must be designed keeping in view all kinds of people and their resources. The design and operation of the robot must be simple enough to be used easily by patients in the comfort of their homes. The concept of home rehabilitation using ankle robots is gaining steam due to the potential it offers to improve access and reduce expenses. Worth mentioning, however, is the fact that such devices must be designed with non-professional use in mind, featuring safety features such as compliant actuators, force and position limits, user interfaces, and emergency stops. Remote clinician monitoring and adaptive control systems can further help individualize therapy while ensuring safety. Clinically, home usage is permissible only if the devices are clinically proven, have undergone appropriate regulatory approvals, and are accompanied by explicit guidelines for usage. Without such controls, inappropriate usage, injury, or ineffective therapy can occur. Thus, while promising, home usage needs to be implemented cautiously and within an appropriately monitored environment.
- One of the major challenges faced with ankle orthosis and rehabilitation platforms is their size and weight. It is necessary to design devices with reduced weight and size employing smart materials and nanotechnologies.
- Implementation of artificial intelligence and intelligent control systems to enhance the performance of AAN-based ankle rehabilitation robots.
- In order to regulate the use of ankle rehabilitation devices more commonly, it is recommended that a set of general guidelines should be issued. This will promote the user’s confidence and control resulting in positive impacts on their health.
- Creating opportunities for engineers, clinicians, and researchers to work together in a team in order to design and develop ankle rehabilitative devices that have the potential to cater to real-world needs and demands.
- Multi-DOF capabilities: Advanced robots increasingly support dorsiflexion/plantarflexion, inversion/eversion, and internal/external rotation, essential for natural and adaptable gait patterns.
- Wearability and portability: Lightweight, modular exoskeletons are replacing bulky setups, making these robots viable for use during daily walking or in home-based rehabilitation.
- User-adaptive control: Integration of EMG signals, force sensors, or learning-based control allows real-time customization of assistance based on patient effort or intention.
- Functional task training: Rather than repetitive motion alone, modern systems focus on training users through goal-oriented tasks, e.g., walking on uneven terrain or climbing stairs.
- Remote monitoring and telerehabilitation: With the increasing use of wireless sensors and cloud platforms, therapists can remotely assess progress and adjust therapy protocols.
- Engagement and motivation features: Gamification, biofeedback, and virtual environments are being used to keep users motivated and improve adherence.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Valderrabano, V.; Barg, A.; Paul, J.; Pagenstert, G.; Wiewiorski, M. Foot and Ankle Injuries in Professional Soccer Players. Sport Orthop. Sport Traumatol. Sports Orthop. Traumatol. 2014, 30, 98–105. [Google Scholar] [CrossRef]
- Chinn, L.; Hertel, J. Rehabilitation of Ankle and Foot Injuries in Athletes. Clin. Sports Med. 2010, 29, 157. [Google Scholar] [CrossRef]
- Mattacola, C.G.; Dwyer, M.K. Rehabilitation of the Ankle After Acute Sprain or Chronic Instability. J. Athl. Train. 2002, 37, 413. [Google Scholar] [PubMed]
- De Ridder, R.; Willems, T.; Vanrenterghem, J.; Robinson, M.A.; Palmans, T.; Roosen, P. Multi-Segment Foot Landing Kinematics in Subjects with Chronic Ankle Instability. Clin. Biomech. 2015, 30, 585–592. [Google Scholar] [CrossRef]
- Nolan, K.J.; Yarossi, M.; McLaughlin, P. Changes in Center of Pressure Displacement with the Use of a Foot Drop Stimulator in Individuals with Stroke. Clin. Biomech. 2015, 30, 755–761. [Google Scholar] [CrossRef]
- Alvarez-Perez, M.G.; Garcia-Murillo, M.A.; Cervantes-Sánchez, J.J. Robot-Assisted Ankle Rehabilitation: A Review. Disabil. Rehabil. Assist. Technol. 2020, 15, 394–408. [Google Scholar] [CrossRef]
- Zeng, X.; Zhu, G.; Zhang, M.; Xie, S.Q. Reviewing Clinical Effectiveness of Active Training Strategies of Platform-Based Ankle Rehabilitation Robots. J. Healthc. Eng. 2018, 2018, 2858294. [Google Scholar] [CrossRef]
- Zhang, M.; Zhu, G.; Nandakumar, A.; Gong, S.; Xie, S. A Virtual-Reality Tracking Game for Use in Robot-Assisted Ankle Rehabilitation. In Proceedings of the 2014 IEEE/ASME 10th International Conference on Mechatronic and Embedded Systems and Applications (MESA), Senigallia, Italy, 10–12 September 2014. [Google Scholar] [CrossRef]
- Khalid, Y.M.; Gouwanda, D.; Parasuraman, S. A Review on the Mechanical Design Elements of Ankle Rehabilitation Robot. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2015, 229, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.F.; Hussain, S.; Goecke, R.; Jamwal, P.K. Mechanism Design and Control of Shoulder Rehabilitation Robots: A Review. IEEE Trans. Med. Robot. Bionics 2023, 5, 780–792. [Google Scholar] [CrossRef]
- Li, J.; Zhang, Z.; Tao, C.; Ji, R. A Number Synthesis Method of the Self-Adapting Upper-Limb Rehabilitation Exoskeletons. Int. J. Adv. Robot. Syst. 2017, 14, 1729881417710796. [Google Scholar] [CrossRef]
- Zhu, G.; Zeng, X.; Zhang, M.; Xie, S.; Meng, W.; Huang, X.; Xu, Q. Robot-Assisted Ankle Rehabilitation for the Treatment of Drop Foot: A Case Study. In Proceedings of the 2016 12th IEEE/ASME International Conference on Mechatronic and Embedded Systems and Applications (MESA), Auckland, New Zealand, 29–31 August 2016. [Google Scholar] [CrossRef]
- Blaya, J.A.; Herr, H. Adaptive Control of a Variable-Impedance Ankle-Foot Orthosis to Assist Drop-Foot Gait. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Saglia, J.A.; Tsagarakis, N.G.; Dai, J.S.; Caldwell, D.G. A High-Performance Redundantly Actuated Parallel Mechanism for Ankle Rehabilitation. Int. J. Robot. Res. 2009, 28, 1216–1227. [Google Scholar] [CrossRef]
- Burdea, G.C.; Cioi, D.; Kale, A.; Janes, W.E.; Ross, S.A.; Engsberg, J.R. Robotics and Gaming to Improve Ankle Strength, Motor Control, and Function in Children with Cerebral Palsy—A Case Study Series. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 165–173. [Google Scholar] [CrossRef]
- Hussain, S.; Jamwal, P.K.; Ghayesh, M.H. State-of-the-Art Robotic Devices for Ankle Rehabilitation: Mechanism and Control Review. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2017, 231, 1224–1234. [Google Scholar] [CrossRef] [PubMed]
- Jamwal, P.K.; Hussain, S.; Xie, S.Q. Review on Design and Control Aspects of Ankle Rehabilitation Robots. Disabil. Rehabil. Assist. Technol. 2015, 10, 93–101. [Google Scholar] [CrossRef]
- Hussain, S.; Jamwal, P.K.; Ghayesh, M.H. Single Joint Robotic Orthoses for Gait Rehabilitation: An Educational Technical Review. J. Rehabil. Med. 2016, 48, 333–338. [Google Scholar] [CrossRef]
- Jamwal, P.K.; Hussain, S.; Xie, S.Q. Three-Stage Design Analysis and Multicriteria Optimization of a Parallel Ankle Rehabilitation Robot Using Genetic Algorithm. IEEE Trans. Autom. Sci. Eng. 2015, 12, 1433–1446. [Google Scholar] [CrossRef]
- Gordon, K.E.; Sawicki, G.S.; Ferris, D.P. Mechanical Performance of Artificial Pneumatic Muscles to Power an Ankle–Foot Orthosis. J. Biomech. 2006, 39, 1832–1841. [Google Scholar] [CrossRef]
- Shi, B.; Chen, X.; Yue, Z.; Yin, S.; Weng, Q.; Zhang, X.; Wang, J.; Wen, W. Wearable Ankle Robots in Post-Stroke Rehabilitation of Gait: A Systematic Review. Front. Neurorobot. 2019, 13, 63. [Google Scholar] [CrossRef]
- Jamwal, P.K.; Xie, S.; Aw, K.C. Kinematic Design Optimization of a Parallel Ankle Rehabilitation Robot Using Modified Genetic Algorithm. Robot. Auton. Syst. 2009, 57, 1018–1027. [Google Scholar] [CrossRef]
- Dong, M.; Zhou, Y.; Li, J.; Rong, X.; Fan, W.; Zhou, X.; Kong, Y. State of the Art in Parallel Ankle Rehabilitation Robot: A Systematic Review. J. Neuroeng. Rehabil. 2021, 18, 52. [Google Scholar] [CrossRef]
- Aggogeri, F.; Pellegrini, N.; Adamini, R. Functional Design in Rehabilitation: Modular Mechanisms for Ankle Complex. Appl. Bionics Biomech. 2016, 2016, 9707801. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Davies, T.C.; Xie, S. Effectiveness of Robot-Assisted Therapy on Ankle Rehabilitation—A Systematic Review. J. Neuroeng. Rehabil 2013, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Siegler, S.; Chen, J.; Schneck, C.D. The Three-Dimensional Kinematics and Flexibility Characteristics of the Human Ankle and Subtalar Joints—Part I: Kinematics. J. Biomech. Eng. 1988, 110, 364–373. [Google Scholar] [CrossRef]
- Leardini, A.; O’Connor, J.J.; Giannini, S. Biomechanics of the Natural, Arthritic, and Replaced Human Ankle Joint. J. Foot Ankle Res. 2014, 7, 8. [Google Scholar] [CrossRef]
- Barnett, C.H.; Napier, J.R. The Axis of Rotation at the Ankle Joint in Man. Its Influence upon the Form of the Talus and the Mobility of the Fibula. J. Anat. 1952, 86, 1. [Google Scholar]
- Malosio, M.; Negri, S.P.; Pedrocchi, N.; Vicentini, F.; Caimmi, M.; Molinari Tosatti, L. A Spherical Parallel Three Degrees-of-Freedom Robot for Ankle-Foot Neuro-Rehabilitation. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2012, 2012, 3356–3359. [Google Scholar] [CrossRef]
- Wang, C.; Fang, Y.; Guo, S.; Chen, Y. Design and Kinematical Performance Analysis of a 3-RUS/RRR Redundantly Actuated Parallel Mechanism for Ankle Rehabilitation. J. Mech. Robot. 2013, 5, 041003. [Google Scholar] [CrossRef]
- Girone, M.; Burdea, G.; Bouzit, M.; Popescu, V.; Deutsch, J.E. Stewart Platform-Based System for Ankle Telerehabilitation. Auton. Robot. 2001, 10, 203–212. [Google Scholar] [CrossRef]
- Contreras-Vidal, J.L.; Bhagat, N.A.; Brantley, J.; Cruz-Garza, J.G.; He, Y.; Manley, Q.; Nakagome, S.; Nathan, K.; Tan, S.H.; Zhu, F.; et al. Powered Exoskeletons for Bipedal Locomotion after Spinal Cord Injury. J. Neural Eng. 2016, 13, 031001. [Google Scholar] [CrossRef]
- Ni, M.; Liu, J.; Sun, Z.; Sun, T. Design and Experiment of an Ankle Rehabilitation Robot After Fracture Surgery. J. Mech. Robot. 2024, 16, 121014. [Google Scholar] [CrossRef]
- Pei, Y.; Han, T.; Zallek, C.M.; Liu, T.; Yang, L.; Hsiao-Wecksler, E.T. Design and Clinical Validation of a Robotic Ankle-Foot Simulator with Series Elastic Actuator for Ankle Clonus Assessment Training. IEEE Robot. Autom. Lett. 2021, 6, 3793–3800. [Google Scholar] [CrossRef]
- Nursultan, Z.; Marco, C.; Balbayev, G. A Portable Robotic System for Ankle Joint Rehabilitation. Electronics 2023, 12, 4271. [Google Scholar] [CrossRef]
- Takahashi, K.Z.; Lewek, M.D.; Sawicki, G.S. A Neuromechanics-Based Powered Ankle Exoskeleton to Assist Walking Post-Stroke: A Feasibility Study. J. Neuroeng. Rehabil. 2015, 12, 23. [Google Scholar] [CrossRef]
- Yeung, L.F.; Ockenfeld, C.; Pang, M.K.; Wai, H.W.; Soo, O.Y.; Li, S.W.; Tong, K.Y. Randomized Controlled Trial of Robot-Assisted Gait Training with Dorsiflexion Assistance on Chronic Stroke Patients Wearing Ankle-Foot-Orthosis. J. Neuroeng. Rehabil. 2018, 15, 51. [Google Scholar] [CrossRef]
- Sawicki, G.S.; Ferris, D.P. A Pneumatically Powered Knee-Ankle-Foot Orthosis (KAFO) with Myoelectric Activation and Inhibition. J. Neuroeng. Rehabil. 2009, 6, 23. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, C.; Long, J.J.; Sun, T.; Duan, L.; Zhang, X.; Zhang, B.; Shen, Y.; Shang, W.; Lin, Z.; et al. Development of a New Robotic Ankle Rehabilitation Platform for Hemiplegic Patients after Stroke. J. Healthc. Eng. 2018, 2018, 3867243. [Google Scholar] [CrossRef]
- Doroftei, I.; Cazacu, C.M.; Alaci, S. Design and Experimental Testing of an Ankle Rehabilitation Robot. Actuators 2023, 12, 238. [Google Scholar] [CrossRef]
- Wang, C.; Sun, Z.; Wei, J.; Xia, J.; Duan, L.; Cai, W.; Liu, Q.; Long, J.; Wang, Y. Systemic Design of an NARR for Hemiplegic Survivors. J. Eng. 2019, 2019, 522–529. [Google Scholar] [CrossRef]
- Zhang, M.; Mcdaid, A.; Veale, A.J.; Peng, Y.; Xie, S.Q. Adaptive Trajectory Tracking Control of a Parallel Ankle Rehabilitation Robot with Joint-Space Force Distribution. IEEE Access 2019, 7, 85812–85820. [Google Scholar] [CrossRef]
- Meng, W.; Zhu, C.; Liu, H.; Liu, Q.; Xie, S. Soft Ankle-Foot Exoskeleton for Rehabilitation: A Systematic Review of Actuation, Sensing, Mechanical Design, and Control Strategy. IEEE Trans. Med. Robot. Bionics 2024, 6, 384–398. [Google Scholar] [CrossRef]
- Miao, Q.; Zhang, M.; Wang, C.; Li, H. Towards Optimal Platform-Based Robot Design for Ankle Rehabilitation: The State of the Art and Future Prospects. J. Healthc. Eng. 2018, 2018, 1534247. [Google Scholar] [CrossRef] [PubMed]
- Minkes-Weiland, S.; Reinders-Messelink, H.A.; Boonstra, A.M.; van der Woude, L.H.; Den Otter, R. Effects of Asymmetrical Support on Lower Limb Muscle Activity during Lokomat Guided Gait in Persons with a Chronic Stroke: An Explorative Study. Eur. J. Phys. Rehabil. Med. 2022, 58, 693. [Google Scholar] [CrossRef]
- Esquenazi, A.; Talaty, M.; Packel, A.; Saulino, M. The ReWalk Powered Exoskeleton to Restore Ambulatory Function to Individuals with Thoracic-Level Motor-Complete Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2012, 91, 911–921. [Google Scholar] [CrossRef]
- Kolakowsky-Hayner, S.A. Safety and Feasibility of Using the EksoTM Bionic Exoskeleton to Aid Ambulation after Spinal Cord Injury. J. Spine 2013. [Google Scholar] [CrossRef]
- Sankai, Y. HAL: Hybrid Assistive Limb Based on Cybernics. Springer Tracts Adv. Robot. 2010, 66, 25–34. [Google Scholar] [CrossRef]
- Li, X.; Zhang, X.; Li, X.; Long, J.; Li, J.; Xu, L.; Chen, G.; Ye, J. BEAR-H: An Intelligent Bilateral Exoskeletal Assistive Robot for Smart Rehabilitation. IEEE Robot. Autom. Mag. 2022, 29, 34–46. [Google Scholar] [CrossRef]
- Schmidt, H.; Hesse, S.; Bernhardt, R.; Krüger, J. Haptic Walker—A Novel Haptic Foot Device. ACM Trans. Appl. Percept. 2005, 2, 166–180. [Google Scholar] [CrossRef]
- Salih, R.K.; Aboud, W.S. Smart Robotic Exoskeleton: Constructing Using 3D Printer Technique for Ankle-Foot Rehabilitation. J. Robot. Control (JRC) 2023, 4, 537–547. [Google Scholar] [CrossRef]
- Li, J.; Zuo, S.; Zhang, L.; Dong, M.; Zhang, Z.; Tao, C.; Ji, R. Mechanical Design and Performance Analysis of a Novel Parallel Robot for Ankle Rehabilitation. J. Mech. Robot. 2020, 12, 051007. [Google Scholar] [CrossRef]
- Chung, J.; Heimgartner, R.; Oneill, C.T.; Phipps, N.S.; Walsh, C.J. ExoBoot, a Soft Inflatable Robotic Boot to Assist Ankle during Walking: Design, Characterization and Preliminary Tests. In Proceedings of the 2018 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob), Enschede, The Netherlands, 26–29 August 2018; pp. 509–516. [Google Scholar] [CrossRef]
- Meijneke, C.; Van Oort, G.; Sluiter, V.; Van Asseldonk, E.; Tagliamonte, N.L.; Tamburella, F.; Pisotta, I.; Masciullo, M.; Arquilla, M.; Molinari, M.; et al. Symbitron Exoskeleton: Design, Control, and Evaluation of a Modular Exoskeleton for Incomplete and Complete Spinal Cord Injured Individuals. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Galiana, I.; Asbeck, A.T.; De Rossi, S.M.M.; Bae, J.; Santos, T.R.T.; De Araujo, V.L.; Lee, S.; Holt, K.G.; Walsh, C. Biomechanical and Physiological Evaluation of Multi-Joint Assistance With Soft Exosuits. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 119–130. [Google Scholar] [CrossRef]
- Park, Y.L.; Chen, B.R.; Pérez-Arancibia, N.O.; Young, D.; Stirling, L.; Wood, R.J.; Goldfield, E.C.; Nagpal, R. Design and Control of a Bio-Inspired Soft Wearable Robotic Device for Ankle-Foot Rehabilitation. Bioinspiration Biomim. 2014, 9, 016007. [Google Scholar] [CrossRef] [PubMed]
- Hau, C.T.; Gouwanda, D.; Gopalai, A.A.; Low, C.Y.; Hanapiah, F.A. Gamification and Control of Nitinol Based Ankle Rehabilitation Robot. Biomimetics 2021, 6, 53. [Google Scholar] [CrossRef]
- Nematollahi, M.; Baghbaderani, K.S.; Amerinatanzi, A.; Zamanian, H.; Elahinia, M. Application of NiTi in Assistive and Rehabilitation Devices: A Review. Bioengineering 2019, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- Hillesheim, L.F.; Ventura, V.N.S.; Ponce, D.A.S. Soft Robot Development: Air Muscle for Rehabilitation Robotic Application. Acad. Soc. J. 2019, 3, 256–260. [Google Scholar] [CrossRef]
- Xie, S.Q.; Jamwal, P.K. An Iterative Fuzzy Controller for Pneumatic Muscle Driven Rehabilitation Robot. Expert Syst. Appl. 2011, 38, 8128–8137. [Google Scholar] [CrossRef]
- Klute, G.K.; Czerniecki, J.M.; Hannaford, B. Artificial Muscles: Actuators for Biorobotic Systems. Int. J. Robot. Res. 2002, 21, 295–309. [Google Scholar] [CrossRef]
- Ferris, D.P.; Gordon, K.E.; Sawicki, G.S.; Peethambaran, A. An Improved Powered Ankle–Foot Orthosis Using Proportional Myoelectric Control. Gait Posture 2006, 23, 425–428. [Google Scholar] [CrossRef]
- Grazi, L.; Crea, S.; Parri, A.; Lova, R.M.; Micera, S.; Vitiello, N. Gastrocnemius Myoelectric Control of a Robotic Hip Exoskeleton Can Reduce the User’s Lower-Limb Muscle Activities at Push Off. Front. Neurosci. 2018, 12, 71. [Google Scholar] [CrossRef]
- Liu, Q.; Zuo, J.; Zhu, C.; Meng, W.; Ai, Q.; Xie, S.Q. Design and Hierarchical Force-Position Control of Redundant Pneumatic Muscles-Cable-Driven Ankle Rehabilitation Robot. IEEE Robot. Autom. Lett. 2022, 7, 502–509. [Google Scholar] [CrossRef]
- Ward, J.; Sugar, T.; Boehler, A.; Standeven, J.; Engsberg, J.R. Stroke Survivors’ Gait Adaptations to a Powered Ankle Foot Orthosis. Adv. Robot. 2011, 25, 1879–1901. [Google Scholar] [CrossRef]
- Zhong, J.; He, D.; Zhao, C.; Zhu, Y.; Zhang, Q. An Rehabilitation Robot Driven by Pneumatic Artificial Muscles. J. Mech. Med. Biol. 2020, 20, 2040008. [Google Scholar] [CrossRef]
- Thalman, C.; Debeurre, M.P.; Lee, H. Entrainment during Human Locomotion Using a Soft Wearable Ankle Robot. IEEE Robot. Autom. Lett. 2021, 6, 4265–4272. [Google Scholar] [CrossRef]
- Głowiński, S.; Ptak, M. A Kinematic Model of a Humanoid Lower Limb Exoskeleton with Pneumatic Actuators. Acta Bioeng. Biomech. 2022, 24, 145–157. [Google Scholar] [CrossRef]
- Hiura, M.; Furukawa, D.; Satoh, T.; Saito, N. Examination of Stiffness Control Performance of Ankle Joint Rehabilitation Machine Using Highly Durable Straight Fiber Type Pneumatic Artificial Muscle. J. Robot. Soc. Jpn. 2022, 40, 936–939. [Google Scholar] [CrossRef]
- Takahashi, Y.; Okada, K.; Noda, T.; Teramae, T.; Nakamura, T.; Haruyama, K.; Okuyama, K.; Tsujimoto, K.; Mizuno, K.; Morimoto, J.; et al. Robotized Knee-Ankle-Foot Orthosis-Assisted Gait Training on Genu Recurvatum during Gait in Patients with Chronic Stroke: A Feasibility Study and Case Report. J. Clin. Med. 2023, 12, 415. [Google Scholar] [CrossRef]
- Borràs, J.; Thomas, F.; Torras, C. New Geometric Approaches to the Analysis and Design of Stewart-Gough Platforms. IEEE/ASME Trans. Mechatron. 2014, 19, 445–455. [Google Scholar] [CrossRef]
- Yoon, J.; Ryu, J.; Lim, K.B. Reconfigurable Ankle Rehabilitation Robot for Various Exercises. J. Robot. Syst. 2006, 22, S15–S33. [Google Scholar] [CrossRef]
- Jamwal, P.K.; Hussain, S.; Ghayesh, M.H.; Rogozina, S.V. Impedance Control of an Intrinsically Compliant Parallel Ankle Rehabilitation Robot. IEEE Trans. Ind. Electron. 2016, 63, 3638–3647. [Google Scholar] [CrossRef]
- Ai, Q.; Zhu, C.; Zuo, J.; Meng, W.; Liu, Q.; Xie, S.Q.; Yang, M. Disturbance-Estimated Adaptive Backstepping Sliding Mode Control of a Pneumatic Muscles-Driven Ankle Rehabilitation Robot. Sensors 2018, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, W.; Liu, H.; Zhang, J.; Liu, S. Conceptual Design and Dimensional Synthesis of a Novel Parallel Mechanism for Lower-Limb Rehabilitation. Robotica 2019, 37, 469–480. [Google Scholar] [CrossRef]
- Xie, S.; Ren, G.; Xiong, J.; Lu, Y. A Trajectory Tracking Control of a Robot Actuated with Pneumatic Artificial Muscles Based on Hysteresis Compensation. IEEE Access 2020, 8, 80964–80977. [Google Scholar] [CrossRef]
- Chi, H.; Su, H.; Liang, W.; Ren, Q. Control of a Rehabilitation Robotic Device Driven by Antagonistic Soft Actuators. Actuators 2021, 10, 123. [Google Scholar] [CrossRef]
- Qian, K.; Li, Z.; Zhang, Z.; Li, G.; Xie, S.Q. Data-Driven Adaptive Iterative Learning Control of a Compliant Rehabilitation Robot for Repetitive Ankle Training. IEEE Robot. Autom. Lett. 2023, 8, 656–663. [Google Scholar] [CrossRef]
- Michmizos, K.P.; Rossi, S.; Castelli, E.; Cappa, P.; Krebs, H.I. Robot-Aided Neurorehabilitation: A Pediatric Robot for Ankle Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 1056–1067. [Google Scholar] [CrossRef]
- Ren, Y.; Wu, Y.N.; Yang, C.Y.; Xu, T.; Harvey, R.L.; Zhang, L.Q. Developing a Wearable Ankle Rehabilitation Robotic Device for In-Bed Acute Stroke Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 589–596. [Google Scholar] [CrossRef]
- Kamarudin, M.N.; Md Rozali, S.; Rozali, S.M.; Lin, T.Y.; Amran, A.C.; Kamarudin, M.N. Development of a Wearable Ankle Rehabilitation Device for Patient with Calf Muscles Flexibility Problems. J. Fundam Appl. Sci. 2018, 10, 365–376. [Google Scholar]
- Liu, J.; Xiong, C.; Fu, C. An Ankle Exoskeleton Using a Lightweight Motor to Create High Power Assistance for Push-Off. J. Mech. Robot. 2019, 11, 041001. [Google Scholar] [CrossRef]
- Khazoom, C.; Veronneau, C.; Bigue, J.P.L.; Grenier, J.; Girard, A.; Plante, J.S. Design and Control of a Multifunctional Ankle Exoskeleton Powered by Magnetorheological Actuators to Assist Walking, Jumping, and Landing. IEEE Robot. Autom. Lett. 2019, 4, 3083–3090. [Google Scholar] [CrossRef]
- Durandau, G.; Farina, D.; Asín-Prieto, G.; Dimbwadyo-Terrer, I.; Lerma-Lara, S.; Pons, J.L.; Moreno, J.C.; Sartori, M. Voluntary Control of Wearable Robotic Exoskeletons by Patients with Paresis via Neuromechanical Modeling. J. Neuroeng. Rehabil. 2019, 16, 91. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.M.; Pei, X.; Hou, T.G.; Fan, Y.B.; Yang, X.; Herr, H.M.; Yang, X.-B. An Untethered Cable-Driven Ankle Exoskeleton with Plantarflexion-Dorsiflexion Bidirectional Movement Assistance. Front. Inf. Technol. Electron. Eng. 2020, 21, 723–739. [Google Scholar] [CrossRef]
- Kim, H.K.; Seong, S.; Park, J.; Kim, J.; Park, J.; Park, W. Subjective Evaluation of the Effect of Exoskeleton Robots for Rehabilitation Training. IEEE Access 2021, 9, 130554–130561. [Google Scholar] [CrossRef]
- Setiawan, R.; Sabar, S.; Madi, M. Design of An Active Power Ankle-Foot Orthosis with Myoelectric Control for Drop-Foot Rehabilitation. Int. J. Electr. Energy Power Syst. Eng. 2021, 4, 139–144. [Google Scholar] [CrossRef]
- Sarmiento Ramos, J.L.; Suárez Galvis, J.C.; Grisales Muñoz, V. Exoskeleton for Ankle Joint Flexion/Extension Rehabilitation. ITECKNE 2022, 19, 104–112. [Google Scholar] [CrossRef]
- Chen, J.; Han, J.; Zhang, J. Design and Evaluation of a Mobile Ankle Exoskeleton With Switchable Actuation Configurations. IEEE/ASME Trans. Mechatron. 2022, 27, 1846–1853. [Google Scholar] [CrossRef]
- Vallés, M.; Cazalilla, J.; Valera, Á.; Mata, V.; Page, Á.; DIáz-Rodríguez, M. A 3-PRS Parallel Manipulator for Ankle Rehabilitation: Towards a Low-Cost Robotic Rehabilitation. Robotica 2017, 35, 1939–1957. [Google Scholar] [CrossRef]
- Rastegarpanah, A.; Saadat, M.; Borboni, A. Parallel Robot for Lower Limb Rehabilitation Exercises. Appl. Bionics Biomech. 2016, 2016, 8584735. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Sun, Y.; Wang, N.; Gao, F.; Wei, K.; Wang, Q. Robot-Assisted Rehabilitation of Ankle Plantar Flexors Spasticity: A 3month Study with Proprioceptive Neuromuscular Facilitation. Front. Neurorobot. 2016, 10, 217222. [Google Scholar] [CrossRef]
- Ayas, M.S.; Altas, I.H. Fuzzy Logic Based Adaptive Admittance Control of a Redundantly Actuated Ankle Rehabilitation Robot. Control Eng. Pract. 2017, 59, 44–54. [Google Scholar] [CrossRef]
- Du, Y.; Li, R.; Li, D.; Bai, S. An Ankle Rehabilitation Robot Based on 3-RRS Spherical Parallel Mechanism. Adv. Mech. Eng. 2017, 9, 1687814017718112. [Google Scholar] [CrossRef]
- Ayas, M.S.; Altas, I.H. Designing and Implementing a Plug-in Type Repetitive Controller for a Redundantly Actuated Ankle Rehabilitation Robot. Proc. Inst. Mech. Eng. Part I J. Syst. Control Eng. 2018, 232, 592–607. [Google Scholar] [CrossRef]
- Liao, Z.; Yao, L.; Lu, Z.; Zhang, J. Screw Theory Based Mathematical Modeling and Kinematic Analysis of a Novel Ankle Rehabilitation Robot with a Constrained 3-PSP Mechanism Topology. Int. J. Intell. Robot. Appl. 2018, 2, 351–360. [Google Scholar] [CrossRef]
- Wang, L.; Chang, Y.; Zhu, H. Internal Model Control and Experimental Study of Ankle Rehabilitation Robot. Robotica 2020, 38, 940–956. [Google Scholar] [CrossRef]
- Dong, M.; Fan, W.; Li, J.; Zhou, X.; Rong, X.; Kong, Y.; Zhou, Y. A New Ankle Robotic System Enabling Whole-Stage Compliance Rehabilitation Training. IEEE/ASME Trans. Mechatron. 2021, 26, 1490–1500. [Google Scholar] [CrossRef]
- Qu, S.; Li, R.; Yao, W.; Ma, C.; Guo, Z. Structure Design, Kinematics Analysis, and Effect Evaluation of a Novel Ankle Rehabilitation Robot. Appl. Sci. 2023, 13, 6109. [Google Scholar] [CrossRef]
- Veneman, J.F.; Ekkelenkamp, R.; Kruidhof, R.; Van Der Helm, F.C.T.; Van Der Kooij, H. A Series Elastic- and Bowden-Cable-Based Actuation System for Use as Torque Actuator in Exoskeleton-Type Robots. Int. J. Robot. Res. 2006, 25, 261–281. [Google Scholar] [CrossRef]
- Kim, J.; Hwang, S.; Sohn, R.; Lee, Y.; Kim, Y. Development of an Active Ankle Foot Orthosis to Prevent Foot Drop and Toe Drag in Hemiplegic Patients: A Preliminary Study. Appl. Bionics Biomech. 2011, 8, 377–384. [Google Scholar] [CrossRef]
- Chen, G.; Yu, H. A Portable Powered Knee-Ankle- Foot Orthosis. J. Med. Devices Trans. ASME 2014, 8, 020927. [Google Scholar] [CrossRef]
- Chen, G.; Qi, P.; Guo, Z.; Yu, H. Mechanical Design and Evaluation of a Compact Portable Knee-Ankle-Foot Robot for Gait Rehabilitation. Mech. Mach. Theory 2016, 103, 51–64. [Google Scholar] [CrossRef]
- Erdogan, A.; Celebi, B.; Satici, A.C.; Patoglu, V. Assist On-Ankle: A Reconfigurable Ankle Exoskeleton with Series-Elastic Actuation. Auton. Robot. 2017, 41, 743–758. [Google Scholar] [CrossRef]
- Guo, K.; Zhao, S.; Liu, Y.; Liu, B.; Yang, H. Wearable Ankle Rehabilitation Device Based on Novel Series Elastic Actuator. DEStech Trans. Eng. Technol. Res. 2019. [Google Scholar] [CrossRef]
- Noel, M.; Fortin, K.; Bouyer, L.J. Using an Electrohydraulic Ankle Foot Orthosis to Study Modifications in Feedforward Control during Locomotor Adaptation to Force Fields Applied in Stance. J. Neuroeng. Rehabil. 2009, 6, 16. [Google Scholar] [CrossRef]
- Blanchette, A.K.; Noël, M.; Richards, C.L.; Nadeau, S.; Bouyer, L.J. Modifications in Ankle Dorsiflexor Activation by Applying a Torque Perturbation during Walking in Persons Post-Stroke: A Case Series. J. Neuroeng. Rehabil. 2014, 11, 98. [Google Scholar] [CrossRef]
- Ficanha, E.M.; Ribeiro, G.A.; Dallali, H.; Rastgaar, M. Design and Preliminary Evaluation of a Two DOFs Cable-Driven Ankle-Foot Prosthesis with Active Dorsiflexion-Plantarflexion and Inversion-Eversion. Front. Bioeng. Biotechnol. 2016, 4, 170293. [Google Scholar] [CrossRef]
- Baser, O.; Kizilhan, H. Mechanical Design and Preliminary Tests of VS-AnkleExo. J. Braz. Soc. Mech. Sci. Eng. 2018, 40, 442. [Google Scholar] [CrossRef]
- Low, F.Z.; Lim, J.H.; Yeow, C.H. Design, Characterisation and Evaluation of a Soft Robotic Sock Device on Healthy Subjects for Assisted Ankle Rehabilitation. J. Med. Eng. Technol. 2018, 42, 26–34. [Google Scholar] [CrossRef]
- Xu, J.; Li, Y.; Xu, L.; Peng, C.; Chen, S.; Liu, J.; Xu, C.; Cheng, G.; Xu, H.; Liu, Y.; et al. A Multi-Mode Rehabilitation Robot with Magnetorheological Actuators Based on Human Motion Intention Estimation. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 2216–2228. [Google Scholar] [CrossRef]
- Baser, O.; Kizilhan, H.; Kilic, E. Employing Variable Impedance (Stiffness/Damping) Hybrid Actuators on Lower Limb Exoskeleton Robots for Stable and Safe Walking Trajectory Tracking. J. Mech. Sci. Technol. 2020, 34, 2597–2607. [Google Scholar] [CrossRef]
- Kim, B.; Jeong, U.; Kang, B.B.; Cho, K.J. Slider-Tendon Linear Actuator with Under-Actuation and Fast-Connection for Soft Wearable Robots. IEEE/ASME Trans. Mechatron. 2021, 26, 2932–2943. [Google Scholar] [CrossRef]
- Gonzalez-Vazquez, A.; Garcia, L.; Kilby, J. Paediatric Ankle Rehabilitation System Based on Twisted and Coiled Polymer Actuators. Smart Mater. Struct. 2024, 33, 075009. [Google Scholar] [CrossRef]
- Bharadwaj, K.; Sugar, T.G.; Koeneman, J.B.; Koeneman, E.J. Design of a Robotic Gait Trainer Using Spring over Muscle Actuators for Ankle Stroke Rehabilitation. J. Biomech. Eng. 2005, 127, 1009–1013. [Google Scholar] [CrossRef]
- Malcolm, P.; Derave, W.; Galle, S.; De Clercq, D. A Simple Exoskeleton That Assists Plantarflexion Can Reduce the Metabolic Cost of Human Walking. PLoS ONE 2013, 8, e56137. [Google Scholar] [CrossRef]
- Shorter, K.A.; Kogler, G.F.; Loth, E.; Durfee, W.K.; Hsiao-Wecksler, E.T. A Portable Powered Ankle-Foot Orthosis for Rehabilitation. J. Rehabil. Res. Dev. 2011, 48, 459–472. [Google Scholar] [CrossRef]
- Jamwal, P.K.; Xie, S.Q.; Hussain, S.; Parsons, J.G. An Adaptive Wearable Parallel Robot for the Treatment of Ankle Injuries. IEEE/ASME Trans. Mechatron. 2014, 19, 64–75. [Google Scholar] [CrossRef]
- Pérez-San Lázaro, R.; Salgado, I.; Chairez, I. Adaptive Sliding-Mode Controller of a Lower Limb Mobile Exoskeleton for Active Rehabilitation. ISA Trans. 2021, 109, 218–228. [Google Scholar] [CrossRef]
- Shushtari, M.; Nasiri, R.; Arami, A. Online Reference Trajectory Adaptation: A Personalized Control Strategy for Lower Limb Exoskeletons. IEEE Robot. Autom. Lett. 2022, 7, 128–134. [Google Scholar] [CrossRef]
- Duc, D.; Phuoc, P.; Tuy, T.; Dong, V.; Dinh Phung, P.; Ngai, Q. Research Control for Ankle Joint Rehabilitation Device. J. Mech. Eng. Sci. 2022, 16, 8743–8753. [Google Scholar] [CrossRef]
- Fang, Q.; Xu, T.; Zheng, T.; Cai, H.; Zhao, J.; Zhu, Y. A Rehabilitation Training Interactive Method for Lower Limb Exoskeleton Robot. Math. Probl. Eng. 2022, 2022, 2429832. [Google Scholar] [CrossRef]
- Meng, W.; Xie, S.Q.; Liu, Q.; Lu, C.Z.; Ai, Q. Robust Iterative Feedback Tuning Control of a Compliant Rehabilitation Robot for Repetitive Ankle Training. IEEE/ASME Trans. Mechatron. 2017, 22, 173–184. [Google Scholar] [CrossRef]
- Huo, W.; Arnez-Paniagua, V.; Ding, G.; Amirat, Y.; Mohammed, S. Adaptive Proxy-Based Controller of an Active Ankle Foot Orthosis to Assist Lower Limb Movements of Paretic Patients. Robotica 2019, 37, 2147–2164. [Google Scholar] [CrossRef]
- Chen, G.; Mao, Z.; Zhou, H.; Yang, P. Design and Control Strategy of 3-Prismatic-Revolute-Spherical Ankle Rehabilitation Robot. Aust. J. Mech. Eng. 2023, 21, 1079–1092. [Google Scholar] [CrossRef]
- Forrester, L.W.; Roy, A.; Krebs, H.I.; Macko, R.F. Ankle Training with a Robotic Device Improves Hemiparetic Gait after a Stroke. Neurorehabilit. Neural repair 2011, 25, 369–377. [Google Scholar] [CrossRef]
- Forrester, L.W.; Roy, A.; Goodman, R.N.; Rietschel, J.; Barton, J.E.; Krebs, H.I.; Macko, R.F. Clinical Application of a Modular Ankle Robot for Stroke Rehabilitation. NeuroRehabilitation 2013, 33, 85–97. [Google Scholar] [CrossRef]
- Roy, A.; Krebs, H.I.; Williams, D.J.; Bever, C.T.; Forrester, L.W.; Macko, R.M.; Hogan, N. Robot-Aided Neurorehabilitation: A Novel Robot for Ankle Rehabilitation. IEEE Trans. Robot. 2009, 25, 569–582. [Google Scholar] [CrossRef]
- Koller, J.R.; Jacobs, D.A.; Ferris, D.P.; Remy, C.D. Learning to Walk with an Adaptive Gain Proportional Myoelectric Controller for a Robotic Ankle Exoskeleton. J. Neuroeng. Rehabil. 2015, 12, 97. [Google Scholar] [CrossRef]
- Galle, S.; Malcolm, P.; Derave, W.; De Clercq, D. Enhancing Performance during Inclined Loaded Walking with a Powered Ankle-Foot Exoskeleton. Eur. J. Appl. Physiol. 2014, 114, 2341–2351. [Google Scholar] [CrossRef]
- Pérez-Ibarra, J.C.; Siqueira, A.A.G.; Silva-Couto, M.A.; De Russo, T.L.; Krebs, H.I. Adaptive Impedance Control Applied to Robot-Aided Neuro-Rehabilitation of the Ankle. IEEE Robot. Autom. Lett. 2019, 4, 185–192. [Google Scholar] [CrossRef]
- Yin, K.; Xiang, K.; Pang, M.; Chen, J.; Anderson, P.; Yang, L. Personalised Control of Robotic Ankle Exoskeleton Through Experience-Based Adaptive Fuzzy Inference. IEEE Access 2019, 7, 72221–72233. [Google Scholar] [CrossRef]
- Ao, D.; Song, R.; Gao, J. Movement Performance of Human-Robot Cooperation Control Based on EMG-Driven Hill-Type and Proportional Models for an Ankle Power-Assist Exoskeleton Robot. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Gasparri, G.M.; Luque, J.; Lerner, Z.F. Proportional Joint-Moment Control for Instantaneously Adaptive Ankle Exoskeleton Assistance. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 751–759. [Google Scholar] [CrossRef]
- Choi, H.; Park, Y.J.; Seo, K.; Lee, J.; Lee, S.E.; Shim, Y. A Multifunctional Ankle Exoskeleton for Mobility Enhancement of Gait-Impaired Individuals and Seniors. IEEE Robot. Autom. Lett. 2018, 3, 411–418. [Google Scholar] [CrossRef]
- Galle, S.; Malcolm, P.; Collins, S.H.; De Clercq, D. Reducing the Metabolic Cost of Walking with an Ankle Exoskeleton: Interaction between Actuation Timing and Power. J. Neuroeng. Rehabil. 2017, 14, 35. [Google Scholar] [CrossRef]
- Zhang, Y.; Nolan, K.J.; Zanotto, D. Oscillator-Based Transparent Control of an Active/Semiactive Ankle-Foot Orthosis. IEEE Robot. Autom. Lett. 2019, 4, 247–253. [Google Scholar] [CrossRef]
- Siviy, C.; Bae, J.; Baker, L.; Porciuncula, F.; Baker, T.; Ellis, T.D.; Awad, L.N.; Walsh, C.J. Offline Assistance Optimization of a Soft Exosuit for Augmenting Ankle Power of Stroke Survivors during Walking. IEEE Robot. Autom. Lett. 2020, 5, 828–835. [Google Scholar] [CrossRef]
- Zhuang, Y.; Leng, Y.; Zhou, J.; Song, R.; Li, L.; Su, S.W. Voluntary Control of an Ankle Joint Exoskeleton by Able-Bodied Individuals and Stroke Survivors Using EMG-Based Admittance Control Scheme. IEEE Trans. Biomed. Eng. 2021, 68, 695–705. [Google Scholar] [CrossRef]
- Lopes, J.M.; Figueiredo, J.; Pinheiro, C.; Reis, L.P.; Santos, C.P. Biomechanical Assessment of Adapting Trajectory and Human-Robot Interaction Stiffness in Impedance-Controlled Ankle Orthosis. J. Intell. Robot. Syst. Theory Appl. 2021, 102, 76. [Google Scholar] [CrossRef]
- Zhang, Q.; Fragnito, N.; Bao, X.; Sharma, N. A Deep Learning Method to Predict Ankle Joint Moment during Walking at Different Speeds with Ultrasound Imaging: A Framework for Assistive Devices Control. Wearable Technol. 2022, 3, e20. [Google Scholar] [CrossRef]
- Zhang, Q.; Lambeth, K.; Sun, Z.; Dodson, A.; Bao, X.; Sharma, N. Evaluation of a Fused Sonomyography and Electromyography-Based Control on a Cable-Driven Ankle Exoskeleton. IEEE Trans. Robot. 2023, 39, 2183–2302. [Google Scholar] [CrossRef]
- Saglia, J.A.; Tsagarakis, N.G.; Dai, J.S.; Caldwell, D.G. Control Strategies for Patient-Assisted Training Using the Ankle Rehabilitation Robot (ARBOT). IEEE/ASME Trans. Mechatron. 2013, 18, 1799–1808. [Google Scholar] [CrossRef]
- Hogan, N. Impedance Control: An Approach to Manipulation: Part I—Theory. J. Dyn. Syst. Meas. Control 1985, 107, 1–7. [Google Scholar] [CrossRef]
- Zhang, M.; Xie, S.Q.; Li, X.; Zhu, G.; Meng, W.; Huang, X.; Veale, A.J. Adaptive Patient-Cooperative Control of a Compliant Ankle Rehabilitation Robot (CARR) with Enhanced Training Safety. IEEE Trans. Ind. Electron. 2017, 65, 1398–1407. [Google Scholar] [CrossRef]
- Zhang, M.; Cao, J.; Zhu, G.; Miao, Q.; Zeng, X.; Xie, S.Q. Reconfigurable Workspace and Torque Capacity of a Compliant Ankle Rehabilitation Robot (CARR). Robot. Auton. Syst. 2017, 98, 213–221. [Google Scholar] [CrossRef]
- Abu-Dakka, F.J.; Valera, A.; Escalera, J.A.; Abderrahim, M.; Page, A.; Mata, V. Passive Exercise Adaptation for Ankle Rehabilitation Based on Learning Control Framework. Sensors 2020, 20, 6215. [Google Scholar] [CrossRef]
- Bo, A.P.L.; Casas, L.; Cucho-Padin, G.; Hayashibe, M.; Elias, D. Control Strategies for Gait Tele-Rehabilitation System Based on Parallel Robotics. Appl. Sci. 2021, 11, 11095. [Google Scholar] [CrossRef]
- Brown, D.F.; Xie, S.Q. Effectiveness of Intelligent Control Strategies in Robot-Assisted Rehabilitation-A Systematic Review. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 1828–1840. [Google Scholar] [CrossRef]
- Xie, Z.; Qian, K.; Li, Z.; Zhao, Y.; Zhang, J.; Kong, X.; Chakrabarty, S.; Zhang, Z.; Xie, S.Q. Progressive Learning Based Assist-as-Needed Control for Ankle Rehabilitation. IEEE Trans. Cogn. Dev. Syst. 2024, 17, 328–339. [Google Scholar] [CrossRef]
- Zhang, H.; Liao, Y.; Zhu, C.; Meng, W.; Liu, Q.; Xie, S.Q. VR-Aided Ankle Rehabilitation Decision-Making Based on Convolutional Gated Recurrent Neural Network. Sensors 2024, 24, 6998. [Google Scholar] [CrossRef]
- Zhang, P.; Zhang, J.; Zhang, Z. Design of RBFNN-Based Adaptive Sliding Mode Control Strategy for Active Rehabilitation Robot. IEEE Access 2020, 8, 155538–155547. [Google Scholar] [CrossRef]
- Koller, J.R.; Remy, C.D.; Ferris, D.P. Biomechanics and Energetics of Walking in Powered Ankle Exoskeletons Using Myoelectric Control versus Mechanically Intrinsic Control. J. Neuroeng. Rehabil. 2018, 15, 42. [Google Scholar] [CrossRef]
- Yeung, L.F.; Lau, C.C.Y.; Lai, C.W.K.; Soo, Y.O.Y.; Chan, M.L.; Tong, R.K.Y. Effects of Wearable Ankle Robotics for Stair and Over-Ground Training on Sub-Acute Stroke: A Randomized Controlled Trial. J. Neuroeng. Rehabil. 2021, 18, 19. [Google Scholar] [CrossRef] [PubMed]
- van Silfhout, L.; Hosman, A.J.F.; van de Meent, H.; Bartels, R.H.M.A.; Edwards, M.J.R. Design Recommendations for Exoskeletons: Perspectives of Individuals with Spinal Cord Injury. J. Spinal Cord Med. 2023, 46, 256. [Google Scholar] [CrossRef]
- Kumar, S.; Zwall, M.R.; Bolivar-Nieto, E.A.; Gregg, R.D.; Gans, N. Extremum Seeking Control for Stiffness Auto-Tuning of a Quasi-Passive Ankle Exoskeleton. IEEE Robot. Autom. Lett. 2020, 5, 4604–4611. [Google Scholar] [CrossRef]
- Moltedo, M.; Baček, T.; Serrien, B.; Langlois, K.; Vanderborght, B.; Lefeber, D.; Rodriguez-Guerrero, C. Walking with a Powered Ankle-Foot Orthosis: The Effects of Actuation Timing and Stiffness Level on Healthy Users. J. Neuroeng. Rehabil. 2020, 17, 98. [Google Scholar] [CrossRef]
- Khan, N.A.; Goyal, T.; Hussain, F.; Jamwal, P.K.; Hussain, S. Transformer-Based Approach for Predicting Transactive Energy in Neurorehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 33, 46–57. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Axis | Movement | Range of Motion (Degrees) |
|---|---|---|
| Transverse | Plantarflexion | 37.6–45.8 |
| Dorsiflexion | 20.3–29.8 | |
| Anteroposterior | Inversion | 14.5–22.0 |
| Eversion | 10.0–17.0 | |
| Vertical | Adduction | 22.0–36.0 |
| Abduction | 15.4–25.4 |
| Reference | Name | DOFs * | Actuator | Control Technique | Experimental Evaluation |
|---|---|---|---|---|---|
| [56] | Bio-Inspired AFO * | 2 | PMA * | Linear Time-Invariant | Healthy Participants |
| [79] | PediAnklebot | 3 | Motor | Impedance Control | CP Patients * |
| [133] | Sun Yat-Sen University Robot | 1 | Motor | EMG-based ANN Control * | Healthy Participants |
| [137] | SAFE * | 1 | SEA * | ANN Control | Healthy Participants |
| [135] | Samsung Robot | 2 | Motor | Assistance Force Control | Healthy Participant |
| [104] | AssistOn- Ankle | 2 | SEA | Force/Impedance | Healthy Participant |
| [34] | Ankle–Foot Simulator | 1 | SEA | Cascaded + Impedance | Clinicians |
| [138] | Soft Exosuit | 1 | Motor | Force/Admittance Control | Stroke Patients |
| [121] | Ankle Robot | 1 | Linear | PD Control * | Not mentioned |
| [131] | AnkleBot | 2 | Motor | Impedance Control | Stroke Patients |
| [134] | Ankle Exoskeleton | 2 | Motor | Proportional Joint-Moment | CP&PD Patients * |
| [36] | Ankle Exoskeleton | 1 | PMA | EMG Control | Stroke Patients |
| [153] | Ankle Exoskeleton | 1 | PMA | EMG Control Finite state Control | Healthy Participant |
| [80] | In-bed Rehabilitation Robot | 1 | Motor | Force Control | Stroke Patients |
| Reference | Name | DOFs | Actuator | Control Technique | Experimental Evaluation | Number of Participants |
|---|---|---|---|---|---|---|
| [73] | PARR * | 3 | PMA * | Position Control + 3 Impedance Control | Healthy Participants | 10 |
| [93] | Ankle Robot | 2 | Motor | Fuzzy Logic Control | Not specified | - |
| [74] | ARR * | 2 | PM * | ABS-SMC * | Healthy Participants | 05 |
| [41] | NARR * | 3 | Motor | PID/Position Control * | Healthy Participants | 01 |
| [98] | 2-UPS/RRR ARR * | 3 | Motor | Admittance Control | Healthy Participants | 05 |
| [148] | PARR | 6 | Hydraulic | FGTM + TTM + SSM * | Healthy Participants | 01 |
| [118] | PARR | 2 | PMA | Adaptive Fuzzy Logic Control | Healthy Participants | 01 |
| [123] | PARR | 3 | PMA | IFT Control * | Healthy Participants | 04 |
| [95] | ARR | 2 | Linear | PID + RC-PID * | Not specified | - |
| [42] | CARR * | 3 | PMA | Admittance Control | Stroke Patients | 01 |
| [131] | ICPAR * | 3 | PMA | Adaptive Impedance Control | Stroke Patients | 04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalsoom, A.; Shah, M.F.; Farooq, M.U. Advancements in State-of-the-Art Ankle Rehabilitation Robotic Devices: A Review of Design, Actuation and Control Strategies. Machines 2025, 13, 429. https://doi.org/10.3390/machines13050429
Kalsoom A, Shah MF, Farooq MU. Advancements in State-of-the-Art Ankle Rehabilitation Robotic Devices: A Review of Design, Actuation and Control Strategies. Machines. 2025; 13(5):429. https://doi.org/10.3390/machines13050429
Chicago/Turabian StyleKalsoom, Asna, Muhammad Faizan Shah, and Muhammad Umer Farooq. 2025. "Advancements in State-of-the-Art Ankle Rehabilitation Robotic Devices: A Review of Design, Actuation and Control Strategies" Machines 13, no. 5: 429. https://doi.org/10.3390/machines13050429
APA StyleKalsoom, A., Shah, M. F., & Farooq, M. U. (2025). Advancements in State-of-the-Art Ankle Rehabilitation Robotic Devices: A Review of Design, Actuation and Control Strategies. Machines, 13(5), 429. https://doi.org/10.3390/machines13050429