Abstract
Three-dimensional virtual reality (VR) games incorporating haptic feedback were developed to support upper-limb rehabilitation in individuals with Parkinson’s disease (PD). Three interactive games: fishing, archery, and mining, were designed to simulate resistance, tension, and vibration using a haptic device, thereby encouraging motor tasks such as pulling, lifting, and lateral maneuvers. Both individuals with PD and healthy participants completed structured sessions, with performance measured through task completion time, scores, and movement trajectories, alongside perceived workload via the NASA-TLX. Results showed that higher haptic resistance levels reduced tremor amplitude by up to 10.55% in participants with PD and improved task completion efficiency by an average of 12.4% across games. These findings demonstrate the potential of personalized haptic feedback to stabilize motor control and enhance performance in VR-based rehabilitation. Importantly, individuals with PD demonstrated improved motor control under moderate haptic resistance, indicating the potential of adjustable haptic feedback for tailoring rehabilitation. These findings underscore the value of VR-haptic games as engaging and adaptable rehabilitation tools, supporting personalized interventions for individuals with PD.
1. Introduction
Parkinson’s disease (PD) is a progressive, neurodegenerative disorder characterized by motor symptoms of tremor, bradykinesia, postural instability, and muscular rigidity [1]. Due to these symptoms, individuals with PD are at an increased risk of fall, loss of independence, and reduced quality of life [2]. By 2030, PD is expected to grow to 1,238,000 diagnosed cases in the United States (US) [3]. Individuals with PD often experience difficulties with coordination, control, fluency, and synchrony of upper extremity multijoint movement tasks [4]. Although rehabilitation exercise therapy has been shown to promote improvement in upper extremity motor function, mobility, and bradykinesia in PD [5,6], adherence to therapy can be challenging in this population.
To address these challenges, researchers have increasingly explored technology-enhanced approaches that can make rehabilitation more engaging and adaptive. Recent advances in technology have introduced new possibilities for rehabilitation. Gamification, virtual reality (VR), and haptic feedback systems have been increasingly studied as tools to enhance motivation and engagement in therapeutic programs [7,8,9,10,11]. Yazdnian et al. [7] developed a comprehensive and gamified rehabilitation system for upper-limb impairment treatments, demonstrating improved user engagement through interactive task-based therapy. Khwaja et al. [8] examined personality traits and their relationship to user engagement in digital health interventions, emphasizing the importance of personalization in gamified systems. Schez-Sobrino et al. [9] proposed a distributed gamified platform that automatically assessed physical exercises, enabling continuous remote rehabilitation with real-time feedback and motivation tracking. Hocine et al. [10] implemented adaptive difficulty in serious games for upper-limb rehabilitation, showing that dynamically adjusting challenge levels improved user performance and adherence. Pillai et al. [11] introduced gamification within a mixed-reality environment, reporting that immersive visual feedback enhanced movement range and task repetition during upper-limb exercises.
VR environments, in particular, provide immersive and interactive platforms that allow individuals to practice motor skills in safe, controlled, and stimulating contexts. Unlike conventional therapy, VR can simulate real-life tasks, offer immediate feedback, and adapt dynamically to patient performance. Haptic devices add another layer of interaction by delivering tactile and force feedback, enabling more natural and realistic training of motor functions. Luo et al. [12] demonstrated that somatosensory driving-based games could enhance coordination and limb control through immersive motion-based training. Hamanishi and Rekimoto [13] presented SuppleView, a system that reduces physical movement limitations by visually guiding imitation tasks, thereby supporting rehabilitation of restricted motor ranges. Avola et al. [14] developed a full-body immersive rehabilitation framework using 3D serious games, confirming that interactive VR environments can improve mobility and overall motor function in cost-effective ways.
Several studies have explored how these approaches can improve rehabilitation outcomes. Hocine et al. [10] developed adaptive difficulty mechanisms in serious games that improved upper-limb coordination by tailoring task challenge to user performance. Pillai et al. [11] integrated gamification within mixed-reality environments and reported increased engagement and movement range in upper-limb exercises. Luo et al. [12] demonstrated that immersive VR driving simulations enhanced patient motivation and spatial coordination during stroke rehabilitation. Gutiérrez et al. [15] designed a haptic feedback thimble for post-spinal cord injury rehabilitation, showing that tactile cues can increase immersion and improve user perception of movement control. These findings suggest that haptic force levels and game difficulty are crucial for personalized PD training, potential impact on long-term rehabilitation outcomes. The study demonstrates the potential of integrating haptic feedback and game difficulty in VR games for personalized training, addressing varying tremor severities in PD individuals.
This study addresses these gaps by investigating the role of haptic feedback and gameplay difficulty in VR-based upper-limb rehabilitation for individuals with PD. We hypothesize that increasing levels of haptic resistance in VR rehabilitation games will reduce tremors and improve task performance in individuals with PD, while adjustable gameplay difficulty will allow for more personalized training that accommodates symptom severity. To examine this, we developed and evaluated three VR games, fishing, archery, and mining, that incorporate adjustable haptic feedback designed to elicit motor tasks such as pulling, lifting, and lateral maneuvers. Both healthy participants and individuals diagnosed with PD were recruited to evaluate how varying levels of haptic feedback and difficulty affect motor performance, hand stability, and subjective workload.
The findings of this work contribute to the growing body of research on technology-enhanced rehabilitation in several ways. First, the study demonstrates the feasibility of combining immersive VR environments with customizable haptic feedback for PD rehabilitation. Second, it provides empirical evidence that haptic resistance can stabilize motor performance and reduce tremor severity, with effects varying according to disease severity. Third, it highlights the importance of adaptive gameplay difficulty in creating personalized rehabilitation experiences that are both effective and engaging. Together, these contributions offer new insights into how VR–haptic systems can be designed for individualized rehabilitation and suggest directions for future clinical applications.
The remainder of this paper is organized as follows. Section 2 reviews related work, Section 3 describes the development of the VR–haptic system and methods, Section 4 outlines the experimental procedures, Section 5 presents the results, Section 6 discusses the findings and their implications, and Section 7 concludes the paper.
2. Related Works
In this section, we review prior work on technology-enhanced rehabilitation with a particular emphasis on three domains: (i) the use of gamification elements to improve adherence and motivation in therapy, (ii) the application of virtual and mixed-reality environments to create immersive training experiences, and (iii) the integration of haptic feedback to provide tactile and force-based interaction. The purpose of this review is to identify how these approaches have been applied to upper-limb rehabilitation, to highlight their limitations, and to situate the novelty of our VR–haptic system within this context. Recent systematic reviews highlight the importance of mechanical design, actuation strategies, and clinical evaluation when developing rehabilitation systems [16], underscoring the need for adaptable and user-centered technologies that align with clinical requirements.
The conventional approach to incorporating design elements in rehabilitation exercises typically relies on 2D displays. Yazdnian et al. used detectors to track joint movements, enhancing range of motion through monitor-based games [7]. Khwaja et al. found that personality traits affect engagement in digital interventions, emphasizing the value of adaptive, personalized design [8]. Schez-Sobrino et al. integrated the Microsoft Kinect sensor to monitor movements and reward exercise performance [9]. Hocine et al. developed a 2D serious game using a graphics tablet, finding dynamic difficulty adaptation improved performance the most [10]. More recently, Zhang et al. [17] demonstrated that partial tactile feedback integrated into gamified VR tasks enhanced embodiment and motivation during upper-limb rehabilitation, reinforcing the value of multisensory engagement in game-based therapy. However, the physical detachment of a 2D display may cause frustration and fatigue.
Prior research has explored using VR or Mixed Reality (MR) to enhance rehabilitation. Pillai et al. used gamified MR tasks for upper limb rehabilitation with the Microsoft HoloLens 2, leading to increased engagement and mobility [11]. Luo et al. found VR was preferred for driving rehabilitation in stroke patients due to its immersion [12]. Hamanishi and Rekimoto’s SuppleView system used visual motion cues to ease physical constraints during imitation, enhancing motor learning and rehabilitation [13]. Avola et al. used the Microsoft Kinect, Oculus Rift S, and LeapMotion to create a personalized VR environment, improving user engagement [14]. Building on these advances, Garcia-Hernandez et al. [18] combined gamified mixed-reality tasks with a robotic exoskeleton, reporting high usability and effective bilateral upper-limb training, which demonstrates the potential of MR-robotic integration for immersive rehabilitation. Despite VR/MR amplifying immersion, the lack of haptic feedback beyond vibration remains a limitation.
Enhancing immersion through haptic devices shows promise. Gutiérrez et al. created VR games with a custom thimble for pressure feedback and vibration, improving immersion [15]. Masmoudi et al. developed a glove for grasp precision with fingertip vibration, enhancing a door-opening game [19]. Chalfant et al. used the Geomagic Touch haptic device to simulate button pressing for PD participant rehabilitation [20]. Bortone et al. used a VR headset and a custom haptic device with electromagnetic servo motors for engaging rehabilitation games, resulting in favorable user engagement [21]. In Parkinson’s-specific rehabilitation, a recent haptic-enhanced mixed-reality system named the Virtual Upper Arm Rehabilitation Simulation (VUARS) demonstrated improved task performance and user experience through adaptive haptic stylus feedback [22], suggesting that tailored tactile cues can enhance both precision and engagement in PD motor training. This deeper evaluation builds upon the foundational findings of Bektic et al. [23], advancing the understanding of how calibrated haptic forces can be personalized to optimize engagement and motor outcomes in PD rehabilitation. While haptic feedback guides movements, its impact on performance and improvement in varying conditions remains unclear.
Among the studies reviewed, only a limited number directly address Parkinson’s disease rehabilitation [19,20], whereas many others focus on post-stroke or general upper-limb impairment [7,11,12,13,14]. This distinction highlights the gap in PD-specific research integrating both adjustable haptic feedback and game difficulty are areas directly addressed by the present study. Further exploration is needed for effective integration into VR games, especially for upper limb rehabilitation. No prior study has demonstrated the effectiveness of integrating haptic force levels and game difficulty into VR games, presenting a new finding for personalized rehabilitation.
3. VR-Haptic Games Development
This section describes the development of the VR-haptic rehabilitation system, including the system architecture, perception study, haptic feedback interface, and game design. The development process followed a structured sequence from hardware and software integration to perceptual calibration and application in three rehabilitation games of fishing, archery, and mining.
3.1. System Architecture
The overall hardware–software configuration is shown in Figure 1. The system was developed on a Dell Alienware PC (Dell Technologies, Round Rock, TX, USA) with Intel® Core™ i5-11400F processor (2.60 GHz) (Intel Corporation, Santa Clara, CA, USA), 32 GB RAM, NVIDIA GeForce RTX 3060 (NVIDIA Corporation, Santa Clara, CA, USA), using Unity game engine (Unity Technologies, San Francisco, CA, USA), using version 2021.3.21f1. Utilizes the Meta Quest 2 VR headset (1832 × 1920, 120 Hz, 92° horizontal FOV, 116° vertical FOV, 503 g) (Meta Platforms, Inc., Menlo Park, CA, USA) and Geomagic Touch haptic device (3 DOF, 431 W × 348 H × 165 D mm, max 3.3 N) (3D Systems, Rock Hill, SC, USA). Integrated into Unity with OpenXR [24] for VR and OpenHaptics [25] for haptics.
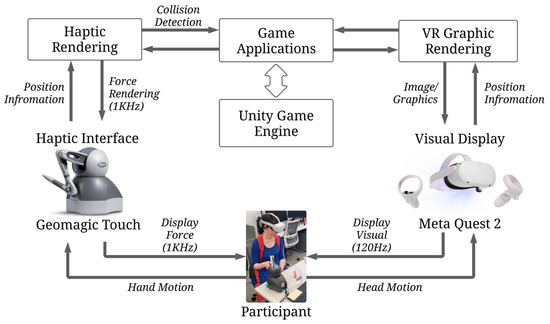
Figure 1.
System architecture diagram that comprises three important components of haptic rendering, VR graphic rendering, and game applications.
The Geomagic Touch was selected because its maximum force output of 3.3 N was sufficient to simulate the range of forces required in our rehabilitation tasks (e.g., fishing resistance, bow tension, rock breaking), while maintaining safe force levels for repeated patient use. Its high positional accuracy (<0.055 mm) allowed precise tracking of subtle upper-limb movements, which was critical for implementing perceptual thresholds from the haptic study. The Meta Quest 2 was chosen due to its combination of lightweight design (503 g), high refresh rate (120 Hz), and wireless capability, reducing participant fatigue and motion sickness while providing high immersion during rehabilitation sessions. Finally, the Alienware PC ensured stable rendering of VR graphics and low-latency force feedback, which was necessary to maintain realism, as delays in haptic feedback can diminish rehabilitation effectiveness. Together, these devices balanced technical performance, participant safety, and usability, making them suitable for both experimental and clinical rehabilitation contexts.
3.2. Development of VR Graphics System
The graphical pipeline in VR rendering within Unity using OpenXR [24] transforms 3D scenes into immersive experiences on devices like the Meta Quest 2. A common technique is raycasting, which traces rays from the viewer’s perspective to determine visible objects and their interaction with light [26]. This involves creating a virtual camera representing the user’s viewpoint, projecting the 3D scene onto the camera’s image plane, and casting rays to determine intersections with objects, calculating light interactions such as shading, reflections, and shadows.
Unity, OpenXR [24], and the Meta Quest 2 specifications enable seamless VR rendering using a premade VR rig in Unity’s scene editor. This setup allows for quick user immersion. The three games used core graphical elements: a premade VR rig, premade assets from the Unity Asset Store, and uniquely created fish silhouettes using Blender. A 3D sign with a world space canvas served as the UI, requiring the user to turn their head to read information.
A pilot study showed that the text on the sign was too small. Initially set to a font size of fifty, the text size was increased to one hundred based on feedback, significantly improving readability for participants.
3.3. Haptic Perception Study
Before implementing haptic feedback into the games, a perception study was conducted to identify human sensitivity thresholds to various haptic stimuli. These thresholds were used to calibrate force feedback levels that would be perceptually distinct yet realistic for rehabilitation tasks. A perception study collected data on human touch feedback, analyzing discrimination thresholds for five haptic feedback types using the adaptive staircase method [27,28,29]: Downward Force, Toward Force, Upward Force, Vibration, and Viscosity.
Total of twenty participants (15 males, 5 females, average age 24, all healthy) were recruited, in accordance with the protocol of the Institutional Review Board (IRB). Participants sat in front of the Geomagic Touch haptic device and wore the Meta Quest 2 VR headset. The order in which participants conducted the five perception tests was randomized using a wheel spinning application, which provides a probability function with a uniform distribution. Participants entered their names, put on the VR headset, grabbed the haptic pen, and selected “Enter.” Upon entering, participants faced a wall of buttons, selectable with the pen to choose the perception study that the examiner told them, based on the randomized order. When entering a test, instructions appeared, and participants could press the start button to begin. All five tests follow a similar structure, presenting haptic feedback stimuli in two sets: one as a reference and the other as a test stimulus controlled by intensity variables. Presentation order randomized per trial; participants choose the stronger stimulus. Test stimulus intensity adjusted based on participant’s response using one-up-one-down (1U1D) adaptive method [27,28,29]. For instance, if the participant’s response was incorrect, the stimulus intensity was increased, and vice versa. Perception tests were conducted in a black empty virtual space with a square changing between red and green for a three-second break between trials. After presenting the two haptic stimuli in each trial, two buttons appeared, asking, “Which was stronger?” Participants then selected ‘A’ or ‘B’ and proceeded to the next trial, as shown in Figure 2. Process repeated until twenty reversals completed for each test, with reference stimulus intensity set to 0.5. For the test stimuli, the first five reversals used a value of 0.2 (max 1 as normalized haptic feedback) for a larger step size to quickly reach the threshold, then 0.05 for smaller step size to increase threshold estimation accuracy. Participant times and answers recorded for each trial. To estimate the discrimination threshold of each haptic feedback test, the standard deviation was used, calculated from the last fifteen reversals. Table 1 summarizes average and standard deviation values from the last fifteen reversals of each test. Estimated discrimination thresholds were used as minimum discriminable intensity values for designing three haptic feedback levels (Haptic Level 1, 2, and 3) in each game application (see Table 2 and Table 3), incorporating five haptic feedback types based on game scenario.
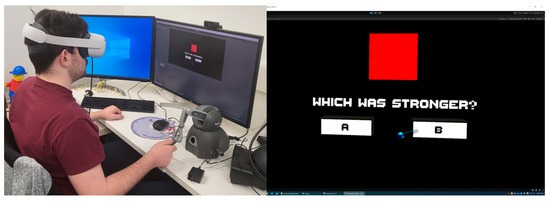
Figure 2.
Illustrates the haptic perception study, which was conducted to determine user sensitivity thresholds for force and friction stimuli. The left image shows the experimental setup, including the participant using the Geomagic Touch device and VR headset. The right panel presents the visual interface displayed in VR, where participants were asked to identify differences in force and friction between the white and red squares on a black background. These stimuli were systematically varied across trials to establish distinct haptic intensity levels used in subsequent gameplay calibration.

Table 1.
Perception Thresholds.
3.4. Design and Integration of Haptic Feedback Interface
The three haptic force levels were derived directly from the perception study (Section 3.3), where discrimination thresholds for multiple haptic feedback types were established using the adaptive staircase (1U1D) method [27,28,29]. These thresholds informed the minimum perceptible change in feedback, which we then scaled to generate three force levels: Level 1 (no force), Level 2 (force values within the perceptible but realistic range, e.g., 0.1–0.35 × 3.3 N), and Level 3 (twice the magnitude of Level 2). Friction and resistance values in the fishing game were determined in the same way, ensuring that they were perceptually distinct yet realistic within the device’s capacity. We note that while these values are sufficient for differentiating feedback levels, future studies could refine the model by incorporating discipline-specific fishing parameters (e.g., rod sensitivity, fish species, tackle type).
Haptic rendering algorithms are essential for creating immersive experiences where users can see and feel virtual environments. These algorithms handle collision detection and responses, providing realistic haptic feedback during virtual interactions. The Geomagic Touch haptic device was selected for its capabilities. In Unity, haptic rendering was managed using OpenHaptics [25]. The first step in haptic rendering is detecting collisions between virtual objects and the haptic device. This involves continuously monitoring their positions and orientations in the virtual environment. Collision detection algorithms determine if the haptic device intersects with any virtual objects. Upon collision detection, haptic responses are generated to simulate tactile feedback. These responses are based on the physical properties of the virtual objects and interactions specified in the games.
To establish the foundation for the fishing rod, bow and arrow, and pickaxe and shovel for the respective games, and to determine how haptic force would be transmitted from the games to the user, the pre-existing haptic device grabber rig was employed. The library’s key functions, including vibration, constant force, tension, friction, viscosity, and pop through, played pivotal roles in this integration. The OpenHaptic [25] offers a variety of scripts to be used and attached to game objects with colliders within the Unity editor scene. This allows those objects to provide haptic feedback instructions to the haptic device. Therefore, capsule colliders are used but not visual rendered. They are moved to the position of the haptic device endpoint when needed to provide feedback and then moved to a position far out of reach for the user to avoid accidental feedback when playing fishing and archery games. This is done because OpenHaptics [25] creates a list of all haptic enabled game objects at the start of runtime when playing the games. However, the script is accessible and can be slightly modified to allow for the list to be recreated later in runtime. This is only implemented within the mining game due to the need for constantly destroying and instantiating game objects.
A perception study, as mentioned previously, was undertaken to explore distinct haptic force levels, employing a discrimination threshold of 0.05 magnitude. The findings yielded three force levels for all of the games but starting with fishing: Level 1 with 0 N, Level 2 representing realistic force values (ranging from 0.1 to 0.35 times 3.3 N for a fishing rod, various-sized fish models, fish tugging, etc.), and Level 3 at twice the magnitude of Level 2, signifying the highest force setting, see Table 2. The viscosity function was used to create the viscous feeling of the lure moving through the water. This is done by moving the capsule collider that contains the functionality to the haptic devices end point position if the lure enters the water surface. The vibration function effectively simulated the nibbling effect of the fish tapping the lure; we achieve this effect similarly to viscosity, but the capsule only stays in position for 0.2 s before returning to a distant location. Constant force and friction were instrumental in mimicking the weight of a caught fish by providing a consistent downward force and introducing stiffness to the movement; this was performed similarly to viscosity. Hooke’s Law, expressed as
was employed to generate the fish-tugging effect through constant force, with F denoting the applied force, k representing the spring constant, and x indicating the amount of extension.
F = −kx,
Table 2.
Fishing Haptic Magnitude Levels.
Table 2.
Fishing Haptic Magnitude Levels.
| Magnitude | Haptic Level 1 | Haptic Level 2 | Haptic Level 3 |
|---|---|---|---|
| Rod Weight | 0 | 0.1 | 0.2 |
| Small Fish Weight | 0 | 0.125 | 0.25 |
| Medium Fish Weight | 0 | 0.155 | 0.31 |
| Large Fish Weight | 0 | 0.175 | 0.35 |
| Shark Weight | 0 | 0.22 | 0.44 |
| Small Fish Friction | 0 | 0.1 | 0.2 |
| Medium Fish Friction | 0 | 0.2 | 0.4 |
| Large Fish Friction | 0 | 0.25 | 0.5 |
| Shark Friction | 0 | 0.3 | 0.6 |
| Fishing Rod Tug | 0 | 0.35 | 0.7 |
| Fish Nibble Vibration | 0 | 306 | 612 |
| Water Viscosity | 0 | 0.1 | 0.2 |
Based on the findings from the perception, three haptic levels were developed for the archery game similarly to the fishing game, see Table 3. The tension function was used to create the bow’s tension and was applied to pull the users hand back to the front of the bow and had a stronger force the farther the device was pulled back. A capsule was used similarly to how other haptic feedback effects were created but unlike the others, never leaves its position to always provide tension feedback to the user. The mining game incorporates the same haptic level structure as the previous two games, as shown in Table 3. For the bounce-off recoil of hitting the rocks, the pop-through force for breaking rocks, and weight of the gems, with Level 3 at twice the magnitude of Level 2, signifying the highest force setting, see Table 3. Constant force and Hook’s Law were used to create the bounce-off effect when hitting rocks by performing a similar method as the fishing tug effect but reversed to push the user’s hand upward with the device. The pop-through functionality of the library was used to allow for the rocks to be touched but needing ample amounts of force to be applied to allow for the pickaxe to break through the rock, this is where the script that OpenHaptics [25] provides that loads in-game objects with the tag ‘touchable’ are loaded into a list needed to be modified since this is only completed during runtime. The modification was to create a function version that allowed me to update the list to remove objects that have been destroyed and add new ones that need to be instantiated; this change was needed to allow for the user to break rocks and have multiple layers of rock underneath that also need breaking, but every rock needs a collider that has haptic feedback for the pop-through that the library offers. The gem weight was created similarly to the fish weight but with only a downward constant force to replicate the feeling of weight on the users’ hands.
Table 3.
Archery and Mining Haptic Magnitude Levels.
Table 3.
Archery and Mining Haptic Magnitude Levels.
| Magnitude | Haptic Level 1 | Haptic Level 2 | Haptic Level 3 |
|---|---|---|---|
| Bow Tension | 0 | 0.25 | 0.5 |
| Bounce Off | 0 | 0.3 | 0.6 |
| Pop through | 0 | 0.3 | 0.6 |
| Gem Weight | 0 | 0.3 | 0.6 |
3.5. Designing Parkinson’s Fishing Rehabilitation Game
All three games use the Meta Quest 2 to enhance immersion, but they differ in haptic devices and game mechanics to focus on various motor tasks.
The fishing rod features a red lure on twelve white hinged cylinders, with a spring force of 1 and a damper of 15. The lure floats realistically on a Unity plane underwater, allowing gentle collisions and settling below the surface. A viscosity capsule activates when the lure is submerged. The lure attracts fish silhouettes of various sizes (small, medium, large, and shark) by enlarging a spherical trigger collider to ten times its original size. Fish silhouettes enter bait mode on collision but move randomly within a pond radius using Unity’s navmesh agent when not in bait mode. Silhouettes entering the lure’s trigger space are added to a list. A random fish is then selected from this list, and its movement position is set to the lure’s position. The haptic device vibrates upon a silhouette reaching and then backing from the lure, incrementing a catch counter for the fish. This process repeats until either the fish exits the trigger collider due to player movement, thus exiting bait mode and being removed from the list, or until the catch counter reaches a required threshold for it to be counted as caught. To signal the participant to pull the fish out of the water and start the motor task of pulling up, as depicted in Figure 3a, the tug effect activates, the silhouette is removed, and a fish model is instantiated below the lure, following its position. The fish model mirrors the size of the silhouette caught by checking its name through a switch statement, determining which fish models to instantiate to follow the lure. The fish model is equipped only with a rigid body and a trigger box collider and interacts only with the bucket tagged as ‘bucket’, or upon touching the water after the user presses the button on the haptic device to release the fish. This prevents the fish from following the lure and activates its rigid body, allowing it to descend until it reaches the water, after which the model is removed. Haptic feedback from Table 2 used throughout: vibration for fish nibbling, tug force upon initial hooking, varied weights and frictions simulating the rod’s resistance when fish are hooked, water viscosity simulated when lure submerged. Points within the game are primarily earned by colliding the caught fish with the bucket. This triggers a check of the fish’s name to determine its size within a switch statement, which then determines the points awarded to the player. The bucket then randomly relocates to a predefined position on the left or right. A new silhouette appears whenever the max number of fish is not in the pond. Multiple small fish are possible, but only one of the other sizes can be present and the spawn rate is set to every 2.5 s. The game ends when ten fish are caught and deposited in the bucket. The in-game sign UI features a fish caught counter, which increases and updates with each successful capture. The game offers three difficulty levels: easy, normal, and hard. Easy level: Max of five fish in the pond with a swimming radius that allows for individual fish to be singled out and caught. Normal level: Max of ten fish in the pond with a smaller swim radius, making it more challenging to single out fish for capture. Hard level: Fifteen fish max in the pond, reduced swim radius for greater challenge in singling out fish, leading to more catches and releases.
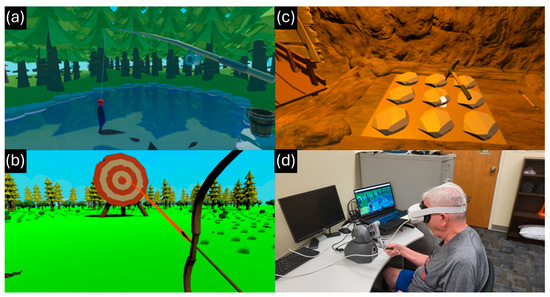
Figure 3.
Illustrates the three VR rehabilitation games: (a) fishing, showing the user pulling a hooked fish with resistance feedback; (b) archery, depicting bow tension during aiming; and (c) mining, where the user applies force to break rocks and collect gems. Panel (d) shows a participant interacting with the fishing game while using the haptic device and Meta Quest 2 headset. These examples highlight how different motor tasks are elicited in immersive VR-haptic environments.
3.6. Designing Parkinson’s Archery Rehabilitation Game
The bow and arrow match the device pen rotation. The bow animation mirrors pen pulling by disabling the mesh renderer from a premade haptic grabber rig by OpenHaptics [25]. Distance from the bow handle is converted to a 0–17 range to determine the animation frame. A red line fades near the target to aid aiming, using a line renderer that increases transparency and shows the arrow’s trajectory (Figure 3b). Users feel tension as they pull back. Pressing the haptic device button instantiates an arrow and applies forward force to its rigid body, propelling it along the indicator path. To reload, the user moves the pen to the bow’s tip, triggering a new arrow and a visual cue for readiness. The objective is to achieve the highest score with 15 arrows. The target has five sections: Center (100 points), next ring (75), following ring (50), then 25, and outer ring (15); misses score 0 points. Unity’s trigger system assigns respective point values upon arrow entry. The remaining arrow counter updates upon contact, and the game ends when the counter reaches zero. The game has three difficulty levels: easy, normal, and hard. Easy: the target is close and centered. Normal: the target is half the size and moves left to right. Hard: the target is smaller, moves in a rectangular pattern, and is obstructed by three trees.
3.7. Designing Parkinson’s Mining Rehabilitation Game
The user enters a mine setting, equipped with a pickaxe to break rocks and unearth randomly placed gems by applying sufficient force. Rocks are arranged in a grid pattern, with gems randomly placed beneath them (Figure 3c). Each rock has a break threshold; surpassing it destroys the rock, potentially revealing a gem. Gems are not placed adjacent to each other, except diagonally, checked by four trigger box colliders. When a gem is revealed, the user can continue searching or swap the pickaxe for a shovel on the right. Swapping tools involves the current tool entering the trigger collider of the unselected tool, disabling its model, and enabling the new tool’s model. Only the shovel can pick up gems by entering the gem’s trigger collider, moving the gem model to the shovel as its child. The cart functions like the fishing game’s bucket, holding gems as its child. Score is based on broken rocks and time, with 500 points deducted per minute. The game ends when all the gems are collected. It offers easy (3 × 3 grid, 3 gems, one hit per rock), normal (4 × 4 grid, 6 gems, two hits per rock with color changes), and hard (5 × 5 grid, 9 gems, three rock layers to break) difficulties.
4. Experiment
An evaluation study measured the usability of the VR-haptic game system using quantitative and qualitative data. We also assessed users’ performance at different haptic force levels to understand the impact on hand-motor rehabilitation for individuals with PD. These results aimed to identify improvement areas and determine the system’s effectiveness based on variable haptic feedback and difficulty levels. The study involved two experiments with two groups: a healthy group (N = 20) for baseline data and a PD group (N = 6) to see if PD severity affects performance and usability. This section details the experiments for both groups, starting with the healthy group and then the PD group.
4.1. Apparatus
For the experiments, we used the Meta Quest 2 VR headset and Geomagic Touch haptic device. A laptop with an Intel® Core™ i7-11800H processor, 16 GB of RAM, and an NVIDIA GeForce RTX 3070 GPU was chosen for its portability.
4.2. Participants
Twenty-six participants were recruited for this study. Among them, twenty were healthy individuals (eleven males, nine females, average age 26.35) with no upper limb impairments. Additionally, six individuals diagnosed with PD (three males, three females, average age 71.17) volunteered to participate in the study.
The PD group had motor function assessments conducted using the Unified Parkinson’s Disease Rating Scale (UPDRS) III, a clinical scale [30]. These assessments were recorded on video and subsequently evaluated and scored by an impartial assessor. Cutoff points for UPDRS severity levels, as outlined in [30], were employed. The severity categories were defined as mild (32 and below), moderate (33–58), and severe (59 and above). Among the PD participants, one individual scored 34, falling into the moderate category. The remaining five participants, with scores ranging from 17 to 29, were classified in the mild category based on UPDRS scores, see Table 4 for more details. Due to the exploratory nature of this study and recruitment constraints, six individuals with PD volunteered. Most participants were classified as mild on the UPDRS-III [30], with one moderate case. Although the participant sample size was limited (N = 6), the study yielded 108 trial samples (6 PD participants × 3 games × 6 trials), providing sufficient data for statistical analysis. Nonetheless, we acknowledge that these findings offer preliminary insights into the feasibility of integrating haptic VR games for upper-limb rehabilitation in PD.
Table 4.
PD Participants UPDRS III Scores.
4.3. Procedure
All participants provided informed consent approved by the Institutional Review Board (IRB) of Kent State University approved this study with an approval number of IRB 632. The experimental setup varied haptic intensity across three levels: Level 1 with no haptic, Level 2 standard, and Level 3 double of Level 2, while keeping difficulty consistent. Gameplay difficulty also varied across three levels: easy, normal, and hard, with a consistent haptic level. Participants grasped the device and initiated the experiment by pressing a pen button, entering a virtual waiting room as the experimenter six trials per game (two per level, three haptic and three difficulty conditions). The order of conditions (haptic level or game difficulty) was randomly selected using a wheel application.
Participants began with a practice mode specific to each game. In fishing, they focused on catching and pulling up fish. In archery, they focused on pulling and aiming the arrow. In mining, they broke rocks to find gems and collected them with a shovel. After practice, participants completed six trials for each game. In fishing, the task was to catch and deposit ten fish in a bucket (Figure 3d). In archery, the goal was to hit targets with fifteen arrows. In mining, the objective was to find and collect all gems hidden under rocks by pushing downward and maneuvering the gems. After finishing one game, another was selected randomly. The process was repeated for the other unselected condition.
We recorded hand motion trajectories, scores, completion times, and practice durations for all three games. After completing all trials for both conditions, participants completed the NASA Task Load Index (TLX) [31] to provide feedback on their subjective workload experience.
5. Results
Here are the findings from the three VR-haptic game tasks (fishing, archery, mining), focusing on haptic conditions and gameplay difficulty. We compare healthy participants with those with PD. Quantitative outcomes include movement trajectories, completion times, and scores for haptic level and gameplay difficulty conditions. Qualitative insights are based on participants’ NASA TLX responses and associated questions. Prior to conducting statistical analysis, the assumptions of ANOVA were assessed to ensure the validity of the results. Normality was evaluated using the Shapiro–Wilk test, while Levene’s test was used to verify homogeneity of variance. The independence of observations was maintained by study design. Assumption checks confirmed that the data met ANOVA requirements, and where violations were detected, appropriate corrective measures, such as data transformation or the use of non-parametric alternatives, were considered.
5.1. Hand Movement Trajectories
Throughout the trials, hand movements were recorded and compared between healthy participants and those with PD. Trajectories for healthy participants were averaged for each haptic level, with force levels varying from 0 N in Level 1 to realistic values in Level 2 (0.1 to 0.35 × 3.3 N) and double the magnitude in Level 3. The trajectory path data indicates a discernible trend during the haptic level trials for the fishing game: as the haptic level increased, hand movements became more compact and ‘T’-shaped for both healthy and PD participants. Notably, at Level 1, the healthy group exhibited more of a ‘V’ shape, while the PD group displayed a more scattered pattern. Participants with PD, particularly those experiencing pronounced tremors, demonstrated smoother and more controlled movements when aided by a higher level of haptic feedback. The trend was confirmed by lower MSE values at higher haptic levels. The hand tremors were significantly reduced by haptic force levels, with the average reduction for PD participants in the mild category being 0.801%. The most significant result was shown by PD participant 4, whose tremors were reduced by 10.55% in MSE. The haptic trials for the archery game revealed that higher haptic levels led to narrower and straighter hand movements, see Figure 4b. Both healthy and PD groups showed this effect, but it was more greatly noticed with the PD group due to the help in stabilizing hand movements and trajectory by the increased haptic force, narrowing user movements, and providing more resistance when attempting to exit that path. The MSE results indicated that as force increased during the arrow-pulling task (Table 1), both healthy and PD participants displayed more compact motions. The mining game haptic trials presented a trend of increased vertical movement distance for both groups as the haptic level rose, with more concise and directed hits to specific areas also noted due to the increase in haptic level, as seen in Figure 4c. The healthy group showed a clear increase in downward motion frequency with higher haptic levels, unlike the PD group, which required only one or two hits to break the rocks as the haptic level rose.
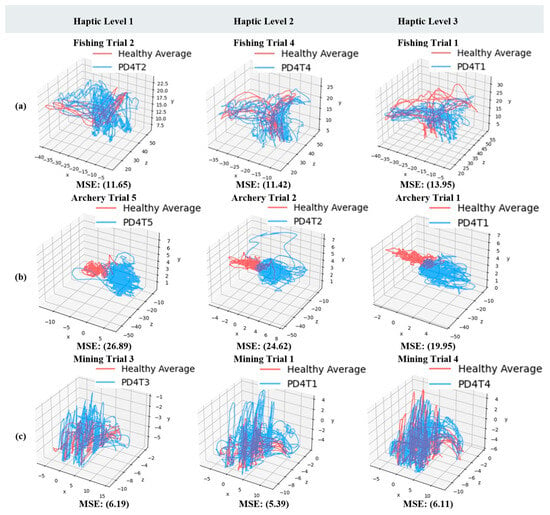
Figure 4.
Comparison of hand motion trajectories for a PD participant (PD4, UPDRS 29, blue) versus the average path of healthy participants (red) in each game with varying haptic force levels. The mean squared error (MSE) quantifies the PD participant’s deviation from the healthy average. (a) Fishing game trajectories showing reduced path dispersion as haptic force increases. (b) Archery game trajectories demonstrating narrower and more stable hand movement with greater haptic resistance. (c) Mining game trajectories illustrating increased vertical control and reduced variability under higher haptic levels. Minor trajectory overlaps between the red and blue lines occurs due to 3D path convergence and does not affect interpretation or clarity of results.
These findings support our hypothesis that increasing haptic force levels reduce tremors and stabilize hand movements in PD participants by providing additional resistance that constrains erratic trajectories.
5.2. Game Scores
Scores for the three games were categorized by haptic level and gameplay difficulty. In the haptic level trials, with constant normal gameplay difficulty, feedback varied: level 1 (no feedback), level 2 (intermediate), and level 3 (double level 2). The analysis compared differences across mild PD, moderate PD, and healthy groups, as shown in Figure 5.
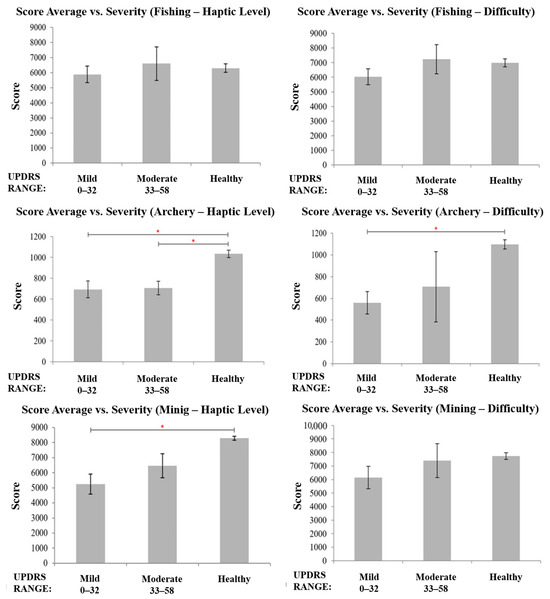
Figure 5.
(Left) Comparison of mean scores across UPDRS severity levels and healthy participants for all haptic level trial scores in the three games with normal gameplay difficulty. (Right) Mean scores for all gameplay difficulty trials among UPDRS severity levels and healthy participants with haptic level fixed at 2. Asterisks (*) indicate statistically significant differences identified using one-way ANOVA (p < 0.05). Note: The “Moderate (33–58)” category includes one participant (N = 1); results should be interpreted accordingly.
Scores in the fishing game were based on fish size, with larger fish earning more points. A one-way ANOVA comparing the haptic level trial scores among mild PD, moderate PD, and healthy groups showed no significant difference (F(2, 75) = 0.35, p = 0.71). For the archery game, accuracy determined scores, and a one-way ANOVA revealed a significant difference (F(2, 75) = 13.25, p < 0.001). T-tests indicated lower scores for both PD groups compared to the healthy group, with no significant difference between the PD groups. In the mining game, scores depended on the number of rocks broken and time to collect gems, starting at 10,000 points and decreasing based on hits and time. A one-way ANOVA showed significant differences among the groups (F(2, 75) = 21.8, p < 0.001). Post hoc T-tests revealed that the mild PD group scored lower than the healthy group, but no significant differences were found between mild and moderate PD or between moderate PD and healthy groups.
The gameplay difficulty was constant at haptic level 2 and varied across three games: fishing, archery, and mining. In fishing, difficulty increased with more fish and a smaller swim radius. In archery, it depended on target positioning, size, and movement. Mining difficulty was determined by grid size, number of gems, and layers. A one-way ANOVA showed no significant effect of PD severity on fishing game scores (F(2, 75) = 1.17, p = 0.31). Archery scores varied significantly by severity (F(2, 75) = 11.49, p < 0.001), with lower scores for mild PD compared to healthy controls. No significant differences were found between mild and moderate PD, or between moderate PD and healthy groups. In the mining game, no significant differences were observed across severity levels (F(2, 75) = 1.53, p = 0.22).
These results partially support our hypothesis. While haptic feedback improved motor control, the influence on overall scores was more modest, suggesting that tremor reduction does not always translate into immediate performance gains, particularly when gameplay difficulty increases.
5.3. Completion Times
The completion times for the three games are categorized by haptic and difficulty levels. First, the completion times under varying haptic levels are presented, using the same task requirements and setup as for the haptic level score results.
Participants’ completion times in the haptic fishing game were averaged, and a one-way ANOVA was conducted to examine the impact of PD severity on average completion times. The analysis compared differences across mild PD, moderate PD, and healthy groups, as depicted in Figure 6. Notably, there was a statistically significant difference in averaged completion times among the severity types at the p < 0.05 level for the three groups, with F(2, 75) = 34.33 and p < 0.001. Post hoc T-Test results revealed that both the mild PD group and the moderate PD group exhibited significantly higher completion times compared to the healthy group. However, no significant difference in completion times was observed between the mild and moderate PD groups. The completion times for the archery game haptic trials were averaged and analyzed using a one-way ANOVA to examine the impact of PD severity on completion time averages. Comparisons we made with mild PD, moderate PD, and healthy groups. There was a statistically significant difference in averaged completion times among the severity types at the p < 0.05 level for the three groups, as shown in Figure 6, with F(2, 75) = 5.02 and p = 0.009. Subsequent T-Test results revealed that the moderate PD group showed significantly higher completion times compared to the mild PD group. However, no significant difference in completion times was observed between the mild PD and healthy groups, as well as moderate PD and healthy groups. The completion times for the mining game haptic levels were averaged, and a one-way ANOVA was used to explore how PD severity affects these averages. Variations were examined among mild PD, moderate PD, and healthy groups. A statistically significant difference in averaged completion times among the severity types was observed at the p < 0.05 level for the three groups, as depicted in Figure 6, with F(2, 75) = 25.07 and p < 0.001. Subsequent T-Test results indicated that the mild PD group exhibited significantly longer completion times compared to the healthy group. However, no significant differences in completion times were observed between the mild and moderate PD groups and the moderate PD and healthy groups.
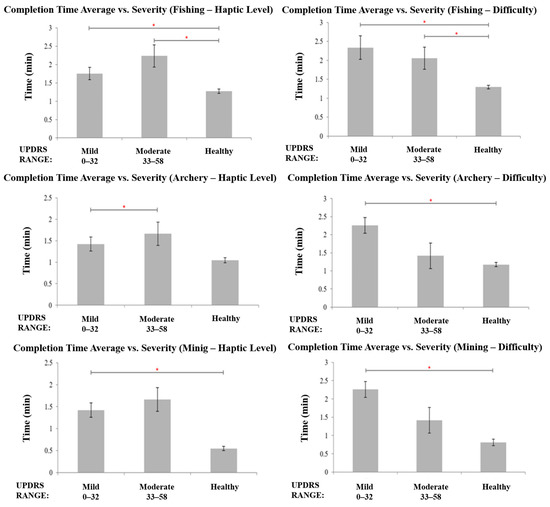
Figure 6.
(Left) Average completion times for haptic level trials among UPDRS severity levels and healthy participants in the three games with normal gameplay difficulty. (Right) Mean completion times for gameplay difficulty trials across UPDRS severity levels and healthy participants in the three games with haptic level fixed at 2. Asterisks (*) indicate statistically significant differences identified using one-way ANOVA (p < 0.05). Note: The “Moderate (33–58)” bar represents data from a single participant with moderate PD severity.
Game difficulty settings matched those for score results. Haptic level remained constant at level 2, as in the previous section. Completion times for fishing game difficulty were averaged, and a one-way ANOVA explored PD severity effects on completion times. Statistically significant differences were found among severity types at the p < 0.05 level for the three groups, as shown in Figure 6, with F(2, 75) = 14.94 and p < 0.001. Subsequent T-Test results revealed that both the mild PD group and the moderate PD group exhibited significantly higher completion times compared to the healthy group. However, no significant difference in completion times was observed between the mild and moderate PD groups. Participants’ completion times in the difficulty archery game were averaged, and a one-way ANOVA was conducted to investigate the influence of PD severity on these averages. Assessments were made among mild PD, moderate PD, and healthy groups, as depicted in Figure 6. Importantly, there was a statistically significant disparity in the averaged completion times among the severity categories at the p < 0.05 level for the three groups, with F(2, 75) = 17.04 and p < 0.001. Subsequent T-Test results indicated that the mild PD group displayed significantly longer completion times compared to the healthy group. However, no significant differences in completion times were observed between the mild and moderate PD groups and the moderate PD and healthy groups. The completion times of the mining game difficulty trials were averaged and underwent analysis using a one-way ANOVA to assess how PD severity influences average completion times. Comparisons were conducted among mild PD, moderate PD, and healthy groups. A statistically significant difference in averaged completion times among the severity categories was evident at the p < 0.05 level for the three groups, as depicted in Figure 6, with F(2, 75) = 15.4 and p < 0.001. Subsequent T-Test results indicated that the mild PD group exhibited significantly longer completion times compared to the healthy group. However, no significant differences in completion times were observed between the mild and moderate PD groups, as well as between the moderate PD and healthy groups.
This trend aligns with our hypothesis that gameplay difficulty interacts with symptom severity. Although haptic resistance improved stability, higher difficulty levels prolonged task completion, particularly for PD participants, highlighting the importance of personalization.
5.4. Qualitative Data
Figure 7 shows mean ratings across six categories evaluating the PD group’s system experience in all three games, rated from 0 to 21. The categories are mental, physical, and temporal demand, performance, effort, and frustration. The total workload averages these categories for the PD group, with a similar calculation for the healthy group. PD participants gave positive feedback, while healthy participants found the system slightly more user-friendly. Both groups reported low mental and physical demands, with some frustration and effort noted. Overall, participants were satisfied with their performance. Minor complaints from some PD participants, such as “arm stress, needed finger stretches” (PD2), likely arose from completing all games in one session. PD5 suggested, “Enjoyable experience overall. Could be a leisure activity with more time,” a sentiment echoed by both healthy and PD participants.
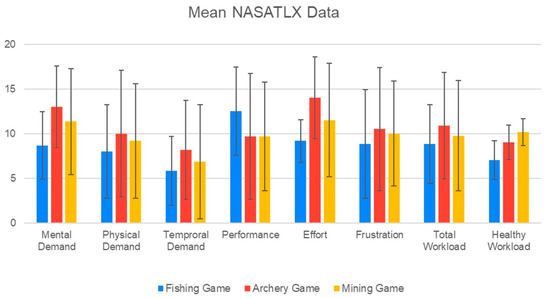
Figure 7.
NASA TLX data for the PD group with a comparison of overall workload of the healthy participants for all three games at the end.
6. Discussion
Overall, the results support our hypothesis that haptic resistance can reduce tremors and improve motor stability in PD participants. Higher haptic levels constrained hand trajectories and promoted smoother movements, while difficulty adjustments influenced engagement and frustration levels. These outcomes reinforce the idea that combining haptic feedback with adaptive gameplay difficulty is essential for tailoring rehabilitation to individual needs. By validating the efficacy of VR-haptic rehabilitation and different avenues for future research with implications for optimizing rehabilitation outcomes and enhancing patient engagement by analyzing hand trajectory, game scores, and completion time data.
The hand trajectory data indicated the influence of haptics on the movement patterns of both healthy and PD participants. Increased force levels mitigated symptoms in the PD group, leading to more distinct pulling up and left or right motor task movements, suggesting the potential to regulate and stabilize the movements of the individuals with PD and reduce tremor symptoms, this was especially demonstrated by PD4 with a reduction of 10.55%. Analyzing the scores revealed subtle distinctions between severity levels Although higher haptic levels improved motor control and reduced tremor amplitude, this did not always correspond to higher game scores, particularly in the fishing and mining games. This may be due to differences in task sensitivity with archery requiring fine precision and benefiting more directly from tremor stabilization, while fishing and mining emphasized task completion over precision, making small improvements in control less reflected in scores. The completion times demonstrated an anticipated impact on performance, affirming that haptic feedback not only yielded a quicker response time but also provided valuable assistance. This directly supports the hypothesis by showing that haptic resistance not only stabilizes movements but also enhances task efficiency in many cases.
Overall, participants from both groups expressed enjoyment and found the fishing game to be entertaining and engaging, especially with the PD group. The allure of haptic feedback and the serene environment of the fishing game, particularly the tugging sensation and the sense of weight from the fish, were appreciated by both groups. The increase in difficulty showed some frustration with some participants, due to the inability to capture fish as easily and quickly but others enjoyed the more methodical and patient approach needed with the higher difficulties. Having a similar feeling and essence as in fishing in real life needs patience and opportunity. The archery game also showed great favorability by the participants, but more so from the healthy group. The appeal of being able to feel the increased tension as the bow is pulled back was especially an enjoyment. Many also liked the increase in difficulty introducing moving target and mentioned that it was a natural increase in difficulty from the stationary target and how it reminded them of other arcade and carnival shotting games. The mining game had both groups share the how they liked the puzzle elements of finding the gems and the need to use force to break though the rocks, but both did mention feeling fatigue with the higher haptic levels and especially when mixed with the higher gameplay difficulty levels needing more rocks to be broken resulting it needing to do more repeated hammer swinging motions. Despite overall satisfaction with their performance, participants faced occasional frustration attributed to technological challenges and an unfamiliar gaming environment. The system’s ability to adjust haptic feedback levels and gameplay difficulty in real-time allows for personalized rehabilitation that cater to the diverse needs and ranged capabilities of individuals with PD, encouraging improved involvement and effectiveness of rehabilitation and represents a significant contribution to the field, offering promising avenues for future research and clinical applications in PD management.
Our findings align with previous studies that reported the benefits of VR and gamified rehabilitation in improving engagement and motor control [11,14,15], and extend them by demonstrating that calibrated haptic force levels can provide measurable tremor reduction in PD participants. Unlike prior work such as Hocine et al. [10], which focused on adaptive difficulty in 2D games, our results show that integrating haptic feedback into immersive VR produces additional stabilization effects. Similarly, while Bortone et al. [22] and Gutiérrez et al. [15] incorporated custom haptic devices, their studies did not examine multi-level force scaling or gameplay difficulty, which our results suggest are critical for personalization. Prior VR studies in PD have shown improvements in balance, gait, and motor performance, particularly when gamification elements are included [6,19]. However, most did not incorporate adjustable haptic resistance as a design parameter. Our study adds to this literature by systematically calibrating haptic levels based on perceptual thresholds and integrating them with varying gameplay difficulties across multiple VR tasks. This dual adaptation framework distinguishes our work and provides a foundation for personalized rehabilitation strategies.
There are certain limitations to this study, which also suggest directions for future work. First, the participant sample was limited, with most PD participants falling into the mild category on the UPDRS, and only one participant classified as moderate. As such, the generalizability of our findings to individuals with severe PD remains limited. The findings should be interpreted as preliminary, warranting confirmation in larger, more diverse participants. Second, while we observed significant reductions in tremors and improvements in stability, these effects did not consistently translate to performance gains under higher gameplay difficulties. Future studies should recruit a broader range of participants across UPDRS severity levels to evaluate whether the benefits of haptic resistance scale consistently with disease progression. In addition to the limited PD sample size, this study was conducted in a single-session, cross-sectional design, which restricts understanding of long-term rehabilitation effects. Future longitudinal studies are needed to evaluate sustained improvements and adaptability over repeated use.
While the present study assessed short-term usability and performance, repeated exposure to VR-haptic rehabilitation games may provide cumulative benefits. Longitudinal use could reinforce motor learning, increase patient adherence, and potentially translate to functional improvements in daily activities. Future trials should adopt repeated-session designs over weeks or months to evaluate durability of effects and potential clinical gains.
7. Conclusions
In summary, this study confirmed our hypothesis that integrating haptic resistance into VR rehabilitation games can reduce tremors and improve task performance in individuals with PD. Higher haptic force levels stabilized motor movements, while gameplay difficulty shaped performance outcomes in ways that emphasize the need for personalized approaches. The study highlights improvements in usability for both healthy and PD participants, and the impact of varying haptic feedback on performance. The experimental phase evaluated the VR-haptic game system’s efficacy across different user groups and conditions. By engaging both healthy individuals and those with PD, the study examined the effects of haptic feedback and game difficulty on motor performance and user experience. Data on trajectories, scores, completion times, and subjective feedback provided valuable insights into the system’s efficacy and user preferences. The results confirmed that increased haptic resistance can reduce tremor amplitude by up to 10.55% and improve task efficiency by over 12% in PD participants. Adjustable game difficulty further enables individualized training to match symptom severity. Findings underscore the importance of haptic force in reducing tremors and customizing training, potentially impacting long-term rehabilitation. Game difficulty contributes to personalized training, dependent on severity. The study demonstrates the potential of integrating haptic feedback and game difficulty into VR games for personalized training for PD. Future research should explore the long-term rehabilitation effects of repeated VR–haptic gaming on hand–motor functions in PD and the potential integration of biofeedback for adaptive difficulty adjustment in clinical settings.
Author Contributions
Conceptualization, M.B. and K.K.; methodology, M.B., A.L.R. and K.K.; software development, M.B.; validation, M.B., A.L.R. and K.K.; data collection, M.B. and B.E.S.; data analysis, M.B., A.L.R., B.E.S. and K.K.; resources, K.K.; writing—original draft preparation, M.B. and B.E.S.; writing—review and editing, A.L.R. and K.K.; supervision, K.K.; project administration, K.K. and A.L.R.; funding acquisition, K.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to ongoing participant use in a longitudinal protocol. However, anonymized datasets may be made available upon reasonable request to the corresponding author once the ongoing study concludes.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| VR | Virtual Reality |
| PD | Parkinson’s Disease |
| US | United States |
| VUARS | Virtual Upper Arm Rehabilitation Simulation |
| 1U1D | one-up-one-down |
| UPDRS | Unified Parkinson’s Disease Rating Scale |
| IRB | Institutional Review Board |
| TLX | Task Load Index |
References
- Dickson, D.W. Neuropathology of Parkinson disease. Park. Relat. Disord. 2018, 46, S30–S33. [Google Scholar] [CrossRef] [PubMed]
- Bjornestad, A.; Tysnes, O.B.; Larsen, J.P.; Alves, G. Loss of independence in early Parkinson disease: A 5-year population-based incident cohort study. Neurology 2016, 87, 1599–1606. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.; Beck, J.C.; Bower, J.H.; Roberts, E.; Ritz, B.; Ross, G.W.; Abbott, R.D.; Savica, R.; Van Den Eeden, S.K.; Willis, A.W.; et al. Prevalence of Parkinson’s disease across North America. npj Park. Dis. 2018, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Seidler, R.D.; Alberts, J.L.; Stelmach, G.E. Multijoint movement control in Parkinson’s disease. Exp. Brain Res. 2001, 140, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Ridgel, A.L.; Ault, D.L. High-cadence cycling promotes sustained improvement in bradykinesia, rigidity, and mobility in individuals with mild–moderate Parkinson’s disease. Park. Dis. 2019, 2019, 4076862. [Google Scholar] [CrossRef] [PubMed]
- Ridgel, A.L.; Phillips, R.S.; Walter, B.L.; Discenzo, F.M.; Loparo, K.A. Dynamic high-cadence cycling improves motor symptoms in Parkinson’s disease. Front. Neurol. 2015, 6, 194. [Google Scholar] [CrossRef] [PubMed]
- Yazdnian, V.; Delavari, A.; Moradi, H.; Shams, S.; Teymouri, M.; Rezaei, A. Comprehensive and gamified rehabilitation system for upper-limb impairment treatments. In Proceedings of the 2022 10th RSI International Conference on Robotics and Mechatronics (ICRoM), Tehran, Iran, 15–17 November 2022; pp. 445–452. [Google Scholar]
- Khwaja, M.; Pieritz, S.; Faisal, A.A.; Matic, A. Personality and engagement with digital mental health interventions. In Proceedings of the 29th ACM Conference on User Modeling, Adaptation and Personalization (UMAP ’21), Utrecht, The Netherlands, 21–25 June 2021; pp. 235–239. [Google Scholar]
- Schez-Sobrino, S.; Vallejo, D.; Monekosso, D.N.; Glez-Morcillo, C.; Remagnino, P. A distributed gamified system based on automatic assessment of physical exercises to promote remote physical rehabilitation. IEEE Access 2020, 8, 91424–91434. [Google Scholar] [CrossRef]
- Hocine, N.; Gouaïch, A.; Cerri, S.A.; Mottet, D.; Froger, J.; Laffont, I. Adaptation in serious games for upper-limb rehabilitation: An approach to improve training outcomes. User Model. User-Adapt. Interact. 2015, 25, 65–98. [Google Scholar] [CrossRef]
- Pillai, A.; Sunny, M.S.H.; Shahria, M.T.; Banik, N.; Rahman, M.H. Gamification of upper limb rehabilitation in mixed-reality environment. Appl. Sci. 2022, 12, 12260. [Google Scholar] [CrossRef]
- Luo, T.; Cai, N.; Li, Z.; Pan, Z.; Yuan, Q. VR-DLR: A serious game of somatosensory driving applied to limb rehabilitation training. In Entertainment Computing—ICEC 2020, Proceedings of the 19th IFIP TC 14 International Conference, Xi’an, China, 10–13 November 2020; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2020; Volume 12523, pp. 51–64. [Google Scholar]
- Hamanishi, N.; Rekimoto, J. SuppleView: Decreasing physical limitations on the movement imitation with viewing motions in the video. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 1521–1523. [Google Scholar]
- Avola, D.; Cinque, L.; Foresti, G.L.; Marini, M.R. An interactive and low-cost full body rehabilitation framework based on 3D immersive serious games. J. Biomed. Inform. 2019, 89, 81–100. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, Á.; Farella, N.; Gil-Agudo, Á.; de los Reyes Guzmán, A. Virtual reality environment with haptic feedback thimble for post spinal cord injury upper-limb rehabilitation. Appl. Sci. 2021, 11, 2476. [Google Scholar] [CrossRef]
- Sarajchi, M.; Al-Hares, M.K.; Sirlantzis, K. Wearable lower-limb exoskeleton for children with cerebral palsy: A systematic review of mechanical design, actuation type, control strategy, and clinical evaluation. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 2695–2720. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Huang, M.; Chen, Y.; Liao, K.-L.; Shi, J.; Liang, H.-N.; Yang, R. Touchmark: Partial tactile feedback design for upper limb rehabilitation in virtual reality. IEEE Trans. Vis. Comput. Graph. 2024, 30, 7430–7440. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Hernandez, N.; Buccelli, S.; De Angelis, A.; Taglione, E.; Laffranchi, M.; De Michieli, L. Assessment of gamified mixed reality environments for upper limb robotic rehabilitation: Pilot study on healthy adults. Virtual Real. 2024, 28, 164. [Google Scholar] [CrossRef]
- Masmoudi, M.; Zenati, N.; Benbelkacem, S.; Hadjadj, Z.; Djekoune, O.; Guerroudji, M.A.; Izountar, Y. Low-cost haptic glove for grasp precision improvement in virtual reality-based post-stroke hand rehabilitation. In Proceedings of the 2021 International Conference on Artificial Intelligence for Cyber Security Systems and Privacy (AI-CSP), Batna, Algeria, 6–7 November 2021; pp. 1–3. [Google Scholar]
- Chalfant, B.; Ridgel, A.; Kim, K. An initial study of virtual button pressing with haptic feedback for the rehabilitation of Parkinson’s disease. In Proceedings of the 2021 4th International Conference on BioSMART, Paris, France, 7–9 December 2021; pp. 1–4. [Google Scholar]
- Bortone, I.; Leonardis, D.; Solazzi, M.; Procopio, C.; Crecchi, A.; Bonfiglio, L.; Frisoli, A. Integration of serious games and wearable haptic interfaces for neurorehabilitation of children with movement disorders: A feasibility study. In Proceedings of the 2017 ICORR, London, UK, 17–20 July 2017; pp. 1094–1099. [Google Scholar]
- Mahmood, N.; Anello, A.; Kim, J.W.; Kim, K.; Smith, B.E.; Ridgel, A.L. Haptic-Enhanced Mixed Reality for Upper Limb Rehabilitation in Parkinson’s Disease. In Proceedings of the 46th Annual International Conference of the IEEE EMBC, Orlando, FL, USA, 15–19 July 2024; IEEE: Piscataway, NJ, USA, 2024; pp. 1–5. [Google Scholar]
- Bektic, M.; Smith, B.E.; Ridgel, A.L.; Kim, K. Virtual reality game with haptic feedback for upper limb rehabilitation in Parkinson’s disease. In Proceedings of the 46th Annual International Conference of the IEEE EMBC, Orlando, FL, USA, 15–19 July 2024; IEEE: Piscataway, NJ, USA, 2024; p. 3090. [Google Scholar]
- The Khronos Group. OpenXR Plugin for Unity. Available online: https://www.khronos.org/openxr/ (accessed on 27 June 2024).
- 3D Systems. OpenHaptics Plugin for Unity. Available online: https://www.3dsystems.com/haptics-devices/openhaptics (accessed on 27 June 2024).
- Unity Technologies. Raycasting for Unity. Available online: https://docs.unity3d.com/2021.3/Documentation/Manual/Raycasters.html (accessed on 27 June 2024).
- Leek, M.R. Adaptive procedures in psychophysical research. Percept. Psychophys. 2001, 63, 1279–1292. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Barni, M.; Tan, H.Z. Roughness-adaptive 3-D watermarking based on masking effect of surface roughness. IEEE Trans. Inf. Forensics Secur. 2010, 5, 721–733. [Google Scholar] [CrossRef][Green Version]
- Kang, Z.; Kim, K. Multimodal perception study on virtual 3D curved textures with vision and touch for interactive multimedia systems. Multimed. Tools Appl. 2018, 77, 2209–2223. [Google Scholar] [CrossRef]
- Skorvanek, M.; Martinez-Martin, P.; Kovacs, N.; Rodriguez-Violante, M.; Corvol, J.C.; Taba, P.; Stebbins, G.T. Differences in MDS-UPDRS scores based on Hoehn and Yahr stage and disease duration. Mov. Disord. Clin. Pract. 2017, 4, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.G. NASA-task load index (NASA-TLX); 20 years later. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2006, 50, 904–908. [Google Scholar] [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).