
A Review of Wrist Rehabilitation Robots and Highlights Needed for New Devices




Abstract
1. Introduction
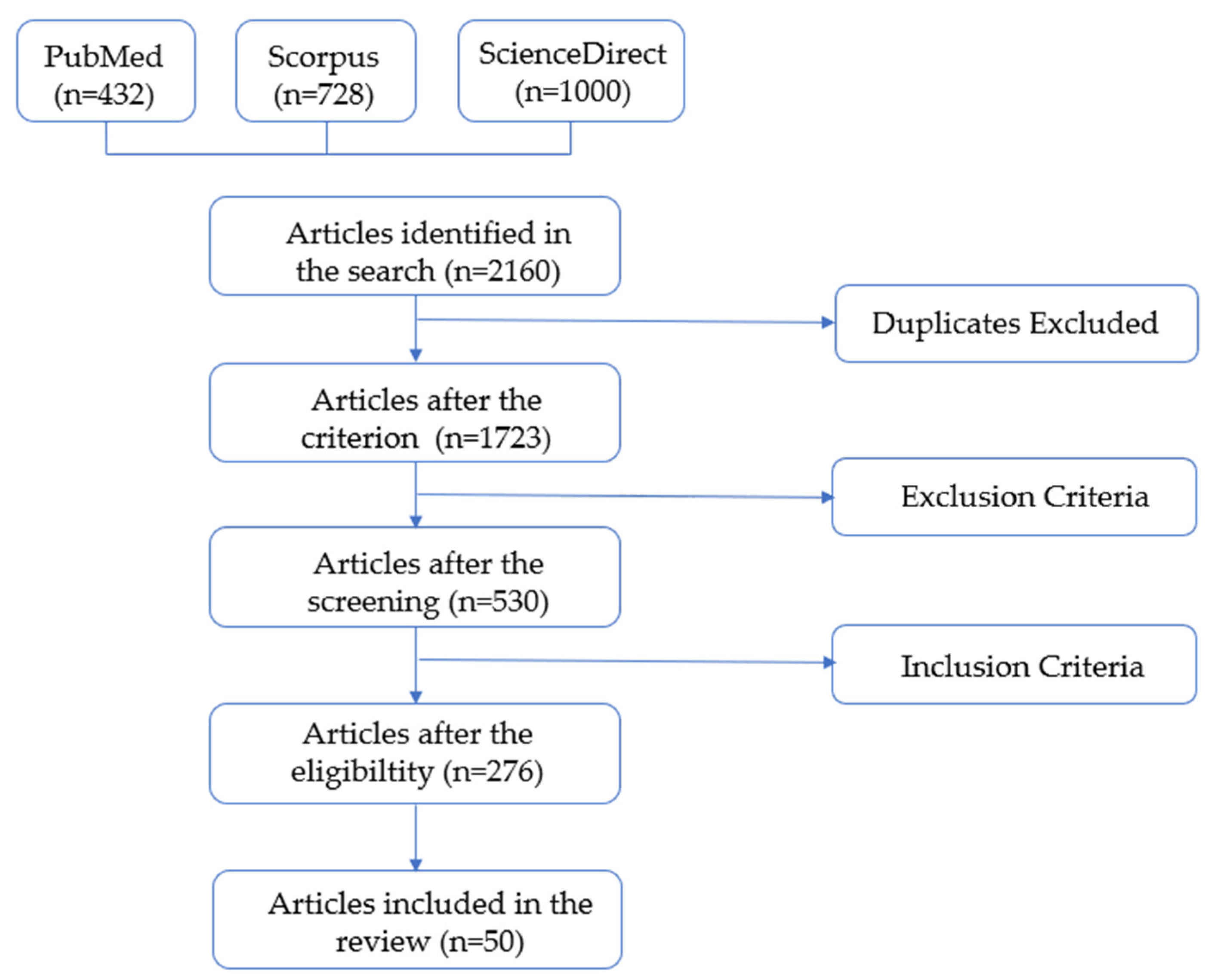
2. Literature Review Search Method
3. Wrist Description
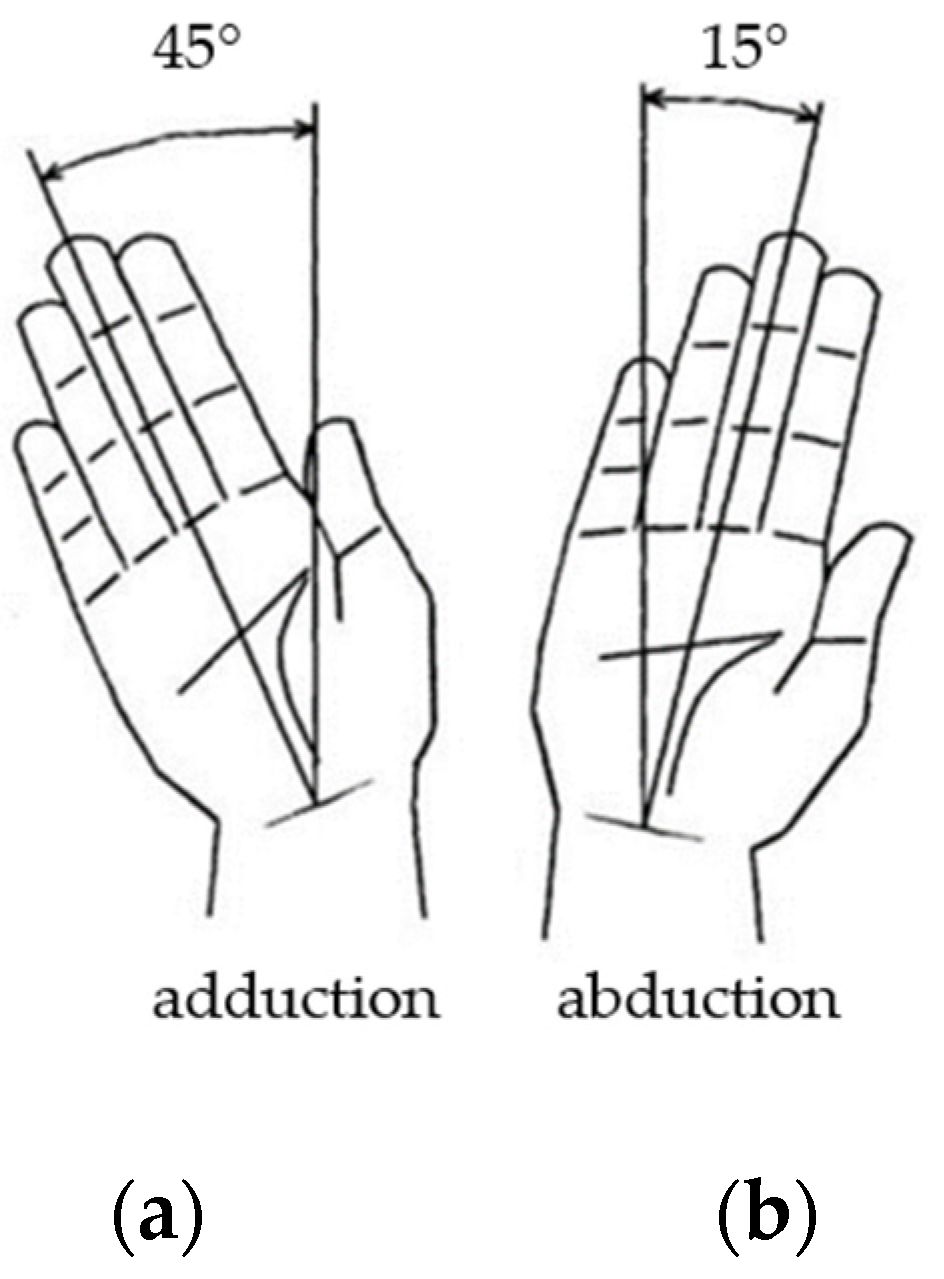
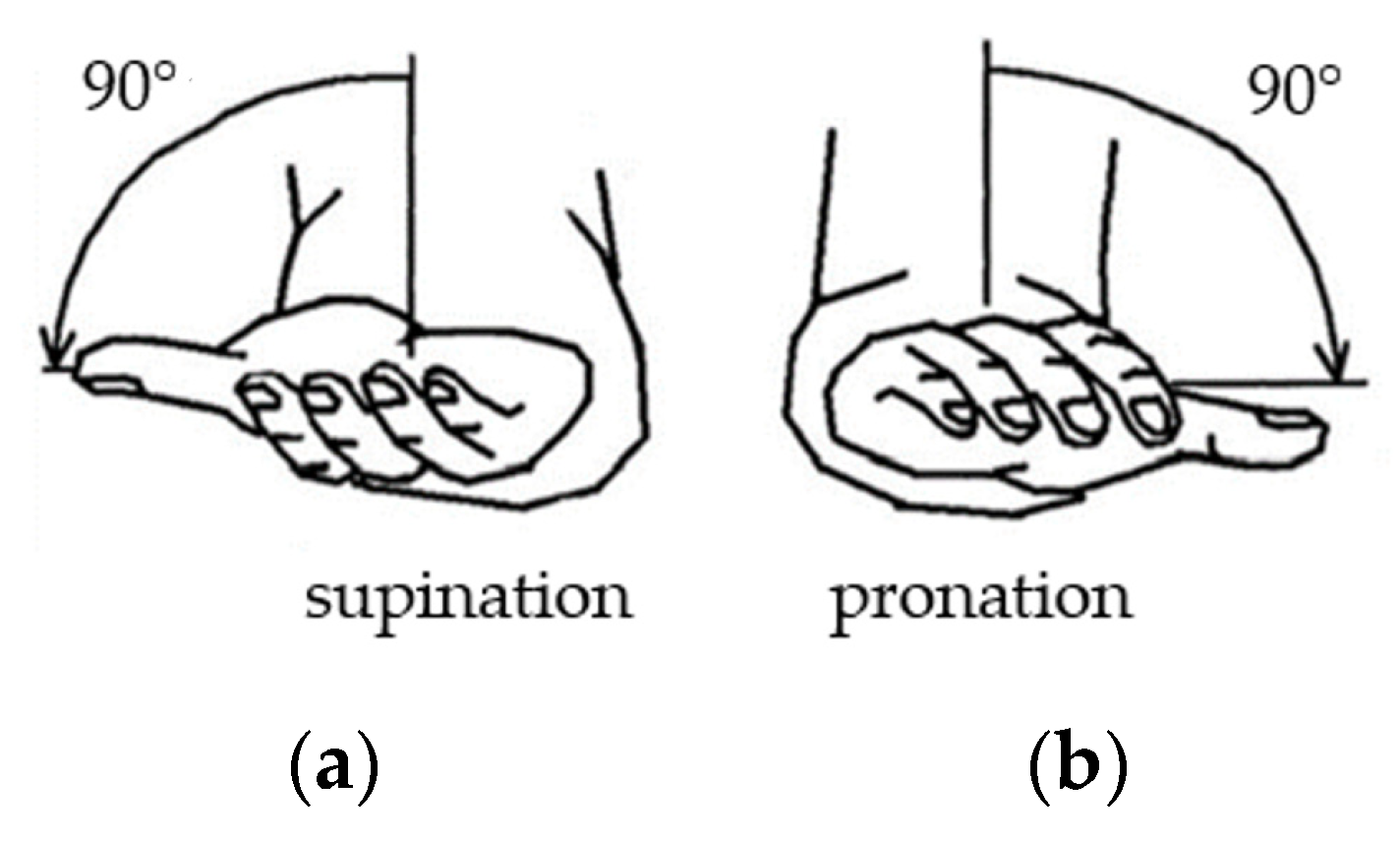
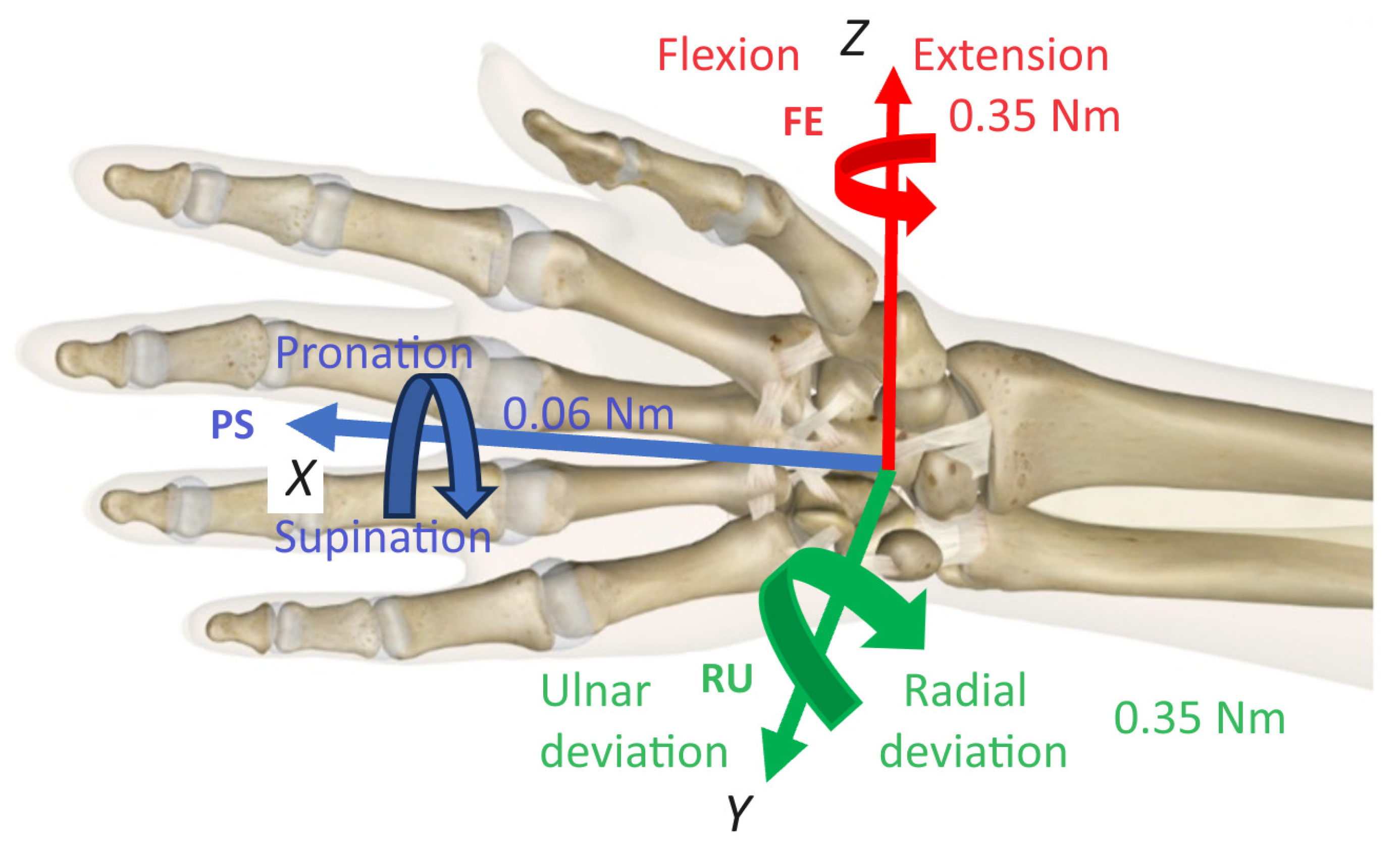
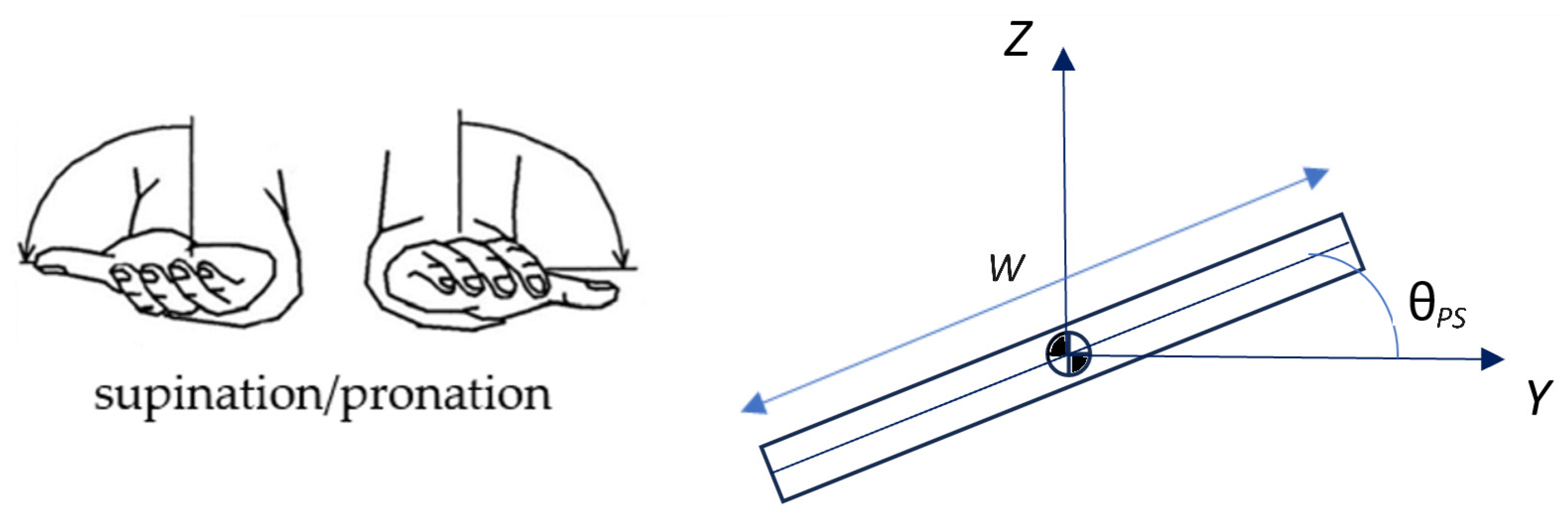
3.1. Wrist Kinematics
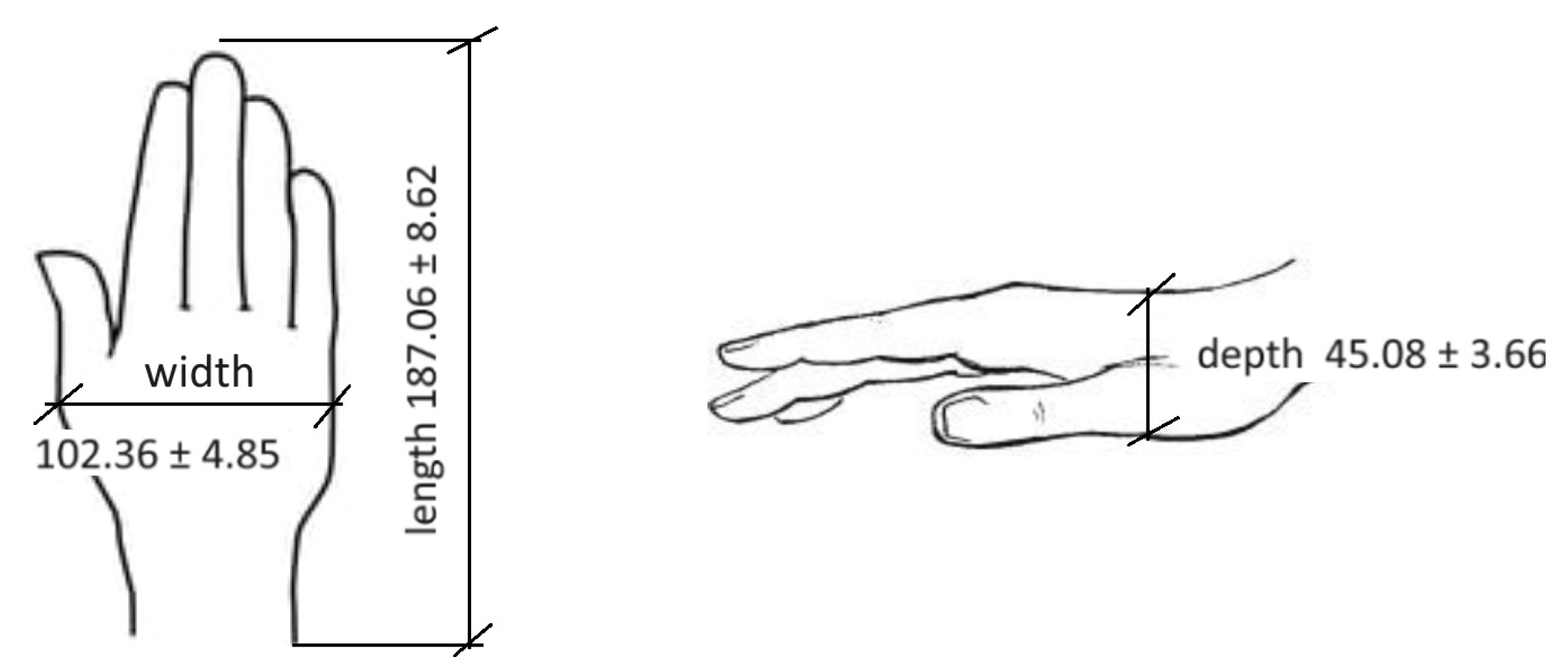
3.2. Wrist Anthropometry and Mathematical Model
4. Wrist Rehabilitation Classification
Wrist Rehabilitation Devices

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device Name | DOF | Structure-Based | Joint | Type of Operation | Control Method | Feedback Signal | Safety | Serious Games and/or AI |
|---|---|---|---|---|---|---|---|---|
| MIT wrist robot [33,34] | 3 | Exoskeleton | Wrist—FE, RU, PS | DC Motors | Impedance Control (AAN) | Load cell, encoders | Not Cited | Serious games No AI |
| Haptic Knob [32,35] | 2 | End-effector (parallelogram mechanism) | Forearm—PS Wrist—FE | DC Motors | Impedance Control | Load cell, encoders | Not Cited | Serious games No AI |
| Open Wrist [36,37,38] | 3 | Exoskeleton (3-RPS (revolute–prismatic–spherical) parallel mechanism) | Wrist—FE, RU, PS | DC Motors | PD Trajectory Tracking | Joint Angles (encoders) and Forces | mechanical stops | No Serious games No AI |
| UHD [39] | 3 | End-effector | Wrist—FE, RU, PS | DC Motors | Impedance Control | Linear Potentiometer | Not Cited | No Serious games No AI |
| IIT Genova Robot [41] | 3 | Exoskeleton | Wrist—FE, RU, PS | DC Motors | Impedance Control | Load cell, encoders | Not Cited | Serious games No AI |
| SCRIPT Prototype 1 [42] | 1 | Exoskeleton | Wrist—FE | Springs | Not provided | Rotary potentiometer | Not Cited | Serious games No AI |
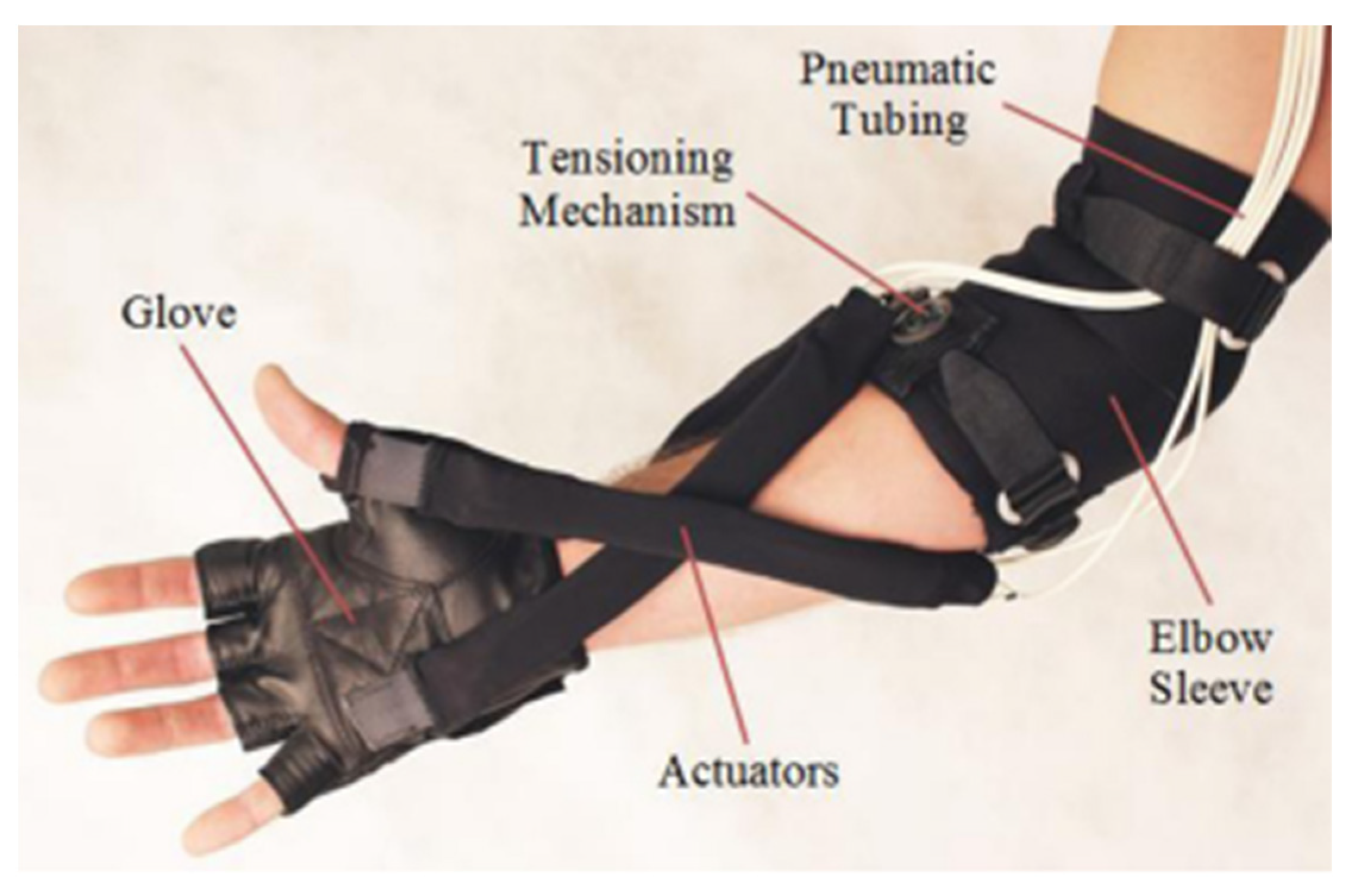
| Harvard University Robot [30] | 2 | Exoskeleton (wearable soft robot) | Wrist—FE, PS | Pneumatic actuator | Not provided | Not provided | Not Cited | No Serious games No AI |
| WRES [43] | 3 | Exoskeleton | Wrist—FE, RU, PS | DC Motors | Not provided | Load cell, encoders | Not Cited | No Serious games No AI |
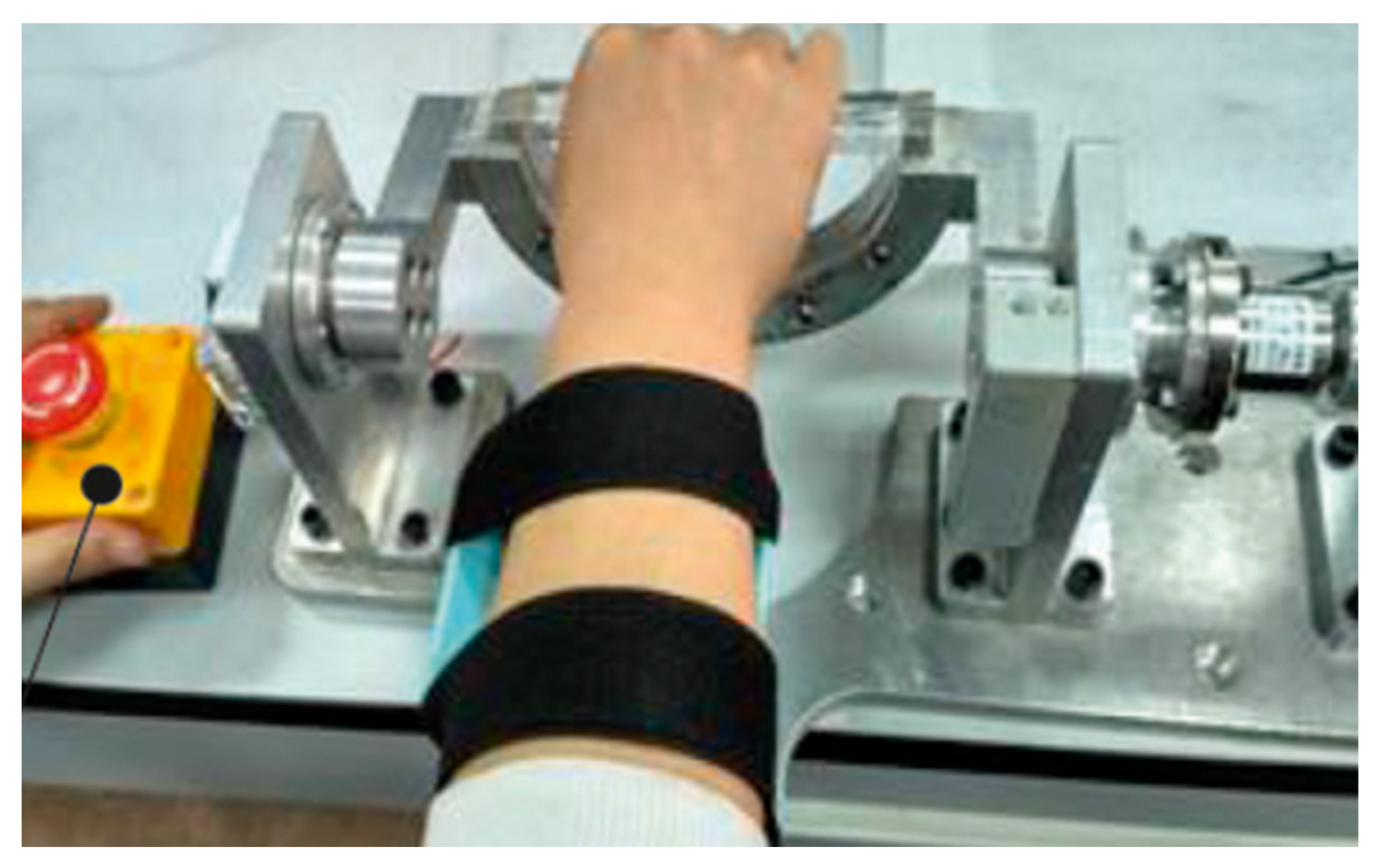
| Kocaeli University [10] | 1 | Exoskeleton | Wrist—FE | DC Motor | Impedance Control | Load cell, encoder | emergency stop | No Serious games No AI |
| CR2-Haptic [44,45] | 1 | End-effector | Wrist—FE, RU, PS | DC Motor | Impedance Control | Current sensor Pulse oximeter Encoder | mechanical stops emergency stop | Serious games No AI |
| Kyushu Robot University [46] | 2 | Exoskeleton | Wrist—FE, RU | Linear Motors | Not provided | Load cell, camera | Not Cited | No Serious games No AI |
| WReD [31] | 1 | End-effector | Wrist—FE | DC Motor | Impedance Control | Torque sensor, encoder | mechanical stops emergency stop | No Serious games No AI |
| Free University Berlin Robot [12] | 1 | End-effector | Wrist—FE | DC Motors | Impedance Control | encoder | Cited | No Serious games No AI |
| UFU wrist robot [24] | 1 | End-effector | Wrist—FE, RU, PS | Servomotor | Impedance Control (AAN) | Torque Sensor | Cited | Serious games No AI |
| Device Name | Experimental Evaluation | Outcomes |
|---|---|---|
| MIT wrist robot [33,34] | 36 stroke participants | Improvements in motor impairment scales |
| Haptic Knob [32,35] | 15 stroke participants | Significantly improved hand and arm functions |
| Open Wrist [36,37,38] | spinal cord C3-5 level | Improvements in hand function test |
| UHD [39] | 1 stroke participant | Reliable and repeatable performance was achieved |
| IIT Genova Robot [41] | 9 stroke participants | Improvements in motor function and range of motion |
| SCRIPT Prototype 1 [42] | 23 stroke participants | Possibility of using device in home care |
| CR2-Haptic [44,45] | 7 stroke participants | Improvements in motor function and range of motion |
| Free University Berlin Robot [12] | 12 stroke participants | Reduction in spasticity and pain relief |
| UFU wrist robot [24] | 3 stroke and 14 healthy participants | Significant gains in motion amplitudes |
5. Wrist Robot Device Control System
Safety
6. Serious Games and AI in Wrist Rehabilitation Devices
7. Discussion
- ⮚
- Movements: They need to be in the function of the traditional physiotherapeutic concepts and reproduce the rehabilitation protocols. It is desirable that the center of rotation of the device coincides with the rotational axis of the human joint;
- ⮚
- Safety: In addition to robots being developed to be safe to use, with mechanisms to prevent accidents and injuries, the need complies with the IEC 80601-2-78:2020 standard [18];
- ⮚
- Cost: Especially for developing countries, the issue of cost is fundamental for the inclusion of this equipment in wrist rehabilitation procedures. In addition to the cost of the equipment, one must also think about the easy replacement of parts that are widely used commercially and their maintenance, which should preferably be carried out by the users themselves;
- ⮚
- User-friendly device: Wrist robot devices need to be patient-friendly and easy to adjust, allowing for the quick attachment and removal of the patient’s hand/forearm. The equipment also needs to be user-friendly for healthcare professionals, allowing for easy use;
- ⮚
- Adaptability: Wrist robot devices need to adapt to different patients at the anthropometric level and the difficult level. The control systems need to adapt to the needs of patients, and the use of serious games together with AI can potentially enhance the rehabilitation process.
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hussain, S.; Jamwal, P.K.; Van Vliet, P.; Ghayesh, M.H. State-of-the-Art Robotic Devices for Wrist Rehabilitation: Design and Control Aspects. IEEE Trans. Hum.-Mach. Syst. 2020, 50, 361–372. [Google Scholar] [CrossRef]
- Alves, T.; Gonçalves, R.S.; Carbone, G. Quantitative assessment of the progress of post-stroke patients using a new cable-actuated bimanual robot. J. Bionic Eng. 2021, 18, 1331–1343. [Google Scholar] [CrossRef]
- Kabir, R.; Sunny, S.H.; Ahmed, H.U.; Rahman, M.H. Hand Rehabilitation Devices: A Comprehensive Systematic Review. Micromachines 2022, 13, 1033. [Google Scholar] [CrossRef]
- Fareh, R.; Elsabe, A.; Baziyad, M.; Kawser, T.; Brahmi, B.; Rahman, M.H. Will Your Next Therapist Be a Robot?—A Review of the Advancements in Robotic Upper Extremity Rehabilitation. Sensors 2023, 23, 5054. [Google Scholar] [CrossRef]
- Coskunsu, D.K.; Akcay, S.; Ogul, O.E.; Akyol, D.K.; Ozturk, N.; Zileli, F.; Tuzun, B.B.; Krespi, Y. Effects of robotic rehabilitation on recovery of hand functions in acute stroke: A preliminary randomized controlled trial. Acta Neurol. Scand. 2022, 146, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, C.D.; Der-Yeghiaian, L.; Le, V.; Motiwala, R.R.; Cramer, S.C. Robot-based hand motor therapy after stroke. Brain 2008, 131 Pt 2, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Auriat, A.M.; Neva, J.L.; Peters, S.; Ferris, J.K.; Boyd, L.A. A review of transcranial magnetic stimulation and multimodal neuroimaging to characterize post-stroke neuroplasticity. Front. Neurol. 2015, 6, 226. [Google Scholar] [CrossRef]
- Gonçalves, R.S.; Prado, R.A.; Ladeira, G.M.V.; Gasparini, A.L.P. Development of Serious Games for the Rehabilitation of the Human Vertebral Spine for Home Care. Robotics 2023, 12, 58. [Google Scholar] [CrossRef]
- Paiva, T.S.d.; Gonçalves, R.S.; Carbone, G. A Critical Review and Systematic Design Approach for Linkage-Based Gait Rehabilitation Devices. Robotics 2024, 13, 11. [Google Scholar] [CrossRef]
- Mayetin, U.; Kucuk, S. A low cost 3-DOF force sensing unit design for wrist rehabilitation robots. Mechatronics 2021, 78, 102623. [Google Scholar] [CrossRef]
- Gonçalves, A.C.B.; Siqueira, A.A.G. State of the art in robotic rehabilitation of lower limbs of people with stroke. Essays and Sciences: Biological, Agrarian and Health Sciences. Anhanguera Educ. Ltda 2014, 17, 109–129. [Google Scholar]
- Hesse, S.; Schulte-Tigges, G.; Konrad, M.; Bardeleben, A.; Werner, C. Robot-assisted arm trainer for the passive and active practice of bilateral forearm and wrist movements in hemiparetic subjects. Arch. Phys. Med. Rehabil. 2003, 84, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, L.A.O.; Gonçalves, R.S. Development of a new body weight support system for gait rehabilitation. Robotics 2023, 41, 1275–1294. [Google Scholar] [CrossRef]
- Rose, C.G.; Pezent, E.; Kann, C.K.; Deshpande, A.D.; O’Malley, M.K. Evaluation of wrist movement with robotic devices. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1585–1595. [Google Scholar] [CrossRef] [PubMed]
- Yue, Z.; Zhang, X.; Wang, J. Hand Rehabilitation Robotics on Poststroke Motor Recovery. Behav. Neurol. 2017, 2017, 3908135. [Google Scholar] [CrossRef] [PubMed]
- Payedimarri, A.B.; Ratti, M.; Rescinito, R.; Vanhaecht, K.; Panella, M. Effectiveness of platform-based robot-assisted rehabilitation for musculoskeletal or neurological injuries: A systematic review. Bioengineering 2022, 9, 129. [Google Scholar] [CrossRef] [PubMed]
- Kapandji, I.A. The Physiology of the Joints, Volume I, Upper Limb, 2nd ed.; S. & E. Livingstone Ltd.: Edinburgh, UK, 1970. [Google Scholar] [CrossRef]
- IEC 80601-2-78:2020; Medical Electrical Equipment. IEC: Geneva, Switzerland, 2020.
- Al-Mayahi, W.; Al-Fahaam, H. A Brief Review of Rehabilitation Wearable Robots for the Upper and Lower Limbs. Int. J. Emerg. Trends Eng. Res. 2023, 11, 291–306. [Google Scholar] [CrossRef]
- Liu, C.; Lu, J.; Yang, H.; Guo, K. Current State of Robotics in Hand Rehabilitation after Stroke: A Systematic Review. Appl. Sci. 2022, 12, 4540. [Google Scholar] [CrossRef]
- Chu, C.Y.; Patterson, R.M. Soft robotic devices for hand rehabilitation and assistance: A narrative review. J. Neuroeng. Rehabil. 2018, 15, 9. [Google Scholar] [CrossRef]
- Abarca, V.E.; Elias, D.A. A Review of Parallel Robots: Rehabilitation, Assistance, and Humanoid Applications for Neck, Shoulder, Wrist, Hip, and Ankle Joints. Robotics 2023, 12, 131. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, R.S.; Brito, L.S.F.; Moraes, L.P.; Carbone, G.; Ceccarelli, M. A fairly simple mechatronic device to train the movement of the human wrist. Int. J. Adv. Robot. Syst. 2020, 17, 1–15. [Google Scholar] [CrossRef]
- Pheasant, S.; Haslegrave, C.M. Bodyspace: Anthropometry, Ergonomics, and Work Design, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar] [CrossRef]
- Chandra, A.; Chandna, P.; Deswal, S. Hand anthropometric survey of male industrial workers of Haryana state (India). Int. J. Ind. Syst. Eng. 2011, 9, 163–182. [Google Scholar]
- Su, Y.-Y.; Yu, Y.-L.; Lin, C.-H.; Lan, C.-C. A compact wrist rehabilitation robot with accurate force/stiffness control and misalignment adaptation. Int. J. Intell. Robot. Appl. 2019, 3, 45–58. [Google Scholar] [CrossRef]
- Sarmiento Ramos, J.L.; Anaya Rojas, M.F. Modelling, design, and construction of a wrist rehabilitation exoskeleton. Sci. Tech. 2022, 27, 177–185. [Google Scholar] [CrossRef]
- Diehl, E. The Engineering Dynamics Course Compananion: Rigid Bodies: Kinematics and Kinetics; Morgan&Claypool: San Rafael, CA, USA, 2021; ISBN 1681739321. [Google Scholar]
- Bartlett, N.W.; Lyau, V.; Raiford, W.A.; Holland, D.; Gafford, J.B.; Ellis, T.D.; Walsh, C.J. A soft robotic orthosis for wrist rehabilitation. J. Med. Devices 2015, 9, 030918. [Google Scholar] [CrossRef]
- Xu, D.; Zhang, M.; Xu, H.; Fu, J.; Li, X.; Xie, S.Q. Interactive compliance control of a wrist rehabilitation (WReD) device with enhanced training safety. J. Healthc. Eng. 2019, 2019, 6537848. [Google Scholar] [CrossRef]
- Lambercy, O.; Dovat, L.; Yun, H.; Wee, S.K.; Kuah, C.W.; Chua, K.S.; Gassert, R.; Milner, T.E.; Teo, C.L.; Burdet, E. Effects of a robot-assisted grasping and pronation/supination training on chronic stroke: A pilot study. J. Neuroeng. Rehabil. 2011, 8, 63. [Google Scholar] [CrossRef]
- Krebs, H.I.; Volpe, B.T.; Williams, D.; Celestino, J.; Charles, S.K.; Lynch, D.; Hogan, N. Robot-Assisted Neurorehabilitation: A Robot for Wrist Rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 327–335. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Durand, S.; Rohan, C.P.; Hamilton, T.; Skalli, W.; Krebs, H.I. Passive Wrist Stiffness: The Influence of Handedness. IEEE Trans. Biomed. Eng. 2019, 66, 656–665. [Google Scholar] [CrossRef]
- Lambercy, O.; Dovat, L.; Gassert, R.; Burdet, E.; Teo, C.L.; Milner, T. A haptic knob for rehabilitation of hand function. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Kadivar, Z.; Sullivan, J.L.; Eng, D.P.; Pehlivan, A.U.; Malley, M.K.O.; Yozbatiran, N.; Berliner, J.D.O.; Boake, C.; Francisco, G.E. Rice Wrist Robotic Device for Upper Limb Training: Feasibility Study and Case Report of Two Quadriplegic Persons with Spinal Cord Injury. Int. J. Biol. Eng. 2012, 2, 27–38. [Google Scholar] [CrossRef]
- Pehlivan, A.U.; Sergi, F.; Erwin, A.; Yozbatiran, N.; Francisco, G.E.; O’Malley, M.K. Design and validation of the RiceWrist-S exoskeleton for robotic rehabilitation after incomplete spinal cord injury. Robotica 2014, 32, 1415–1431. [Google Scholar] [CrossRef]
- Perry, J.C.; Rosen, J.; Burns, S. Upper-Limb Powered Exoskeleton Design. IEEE/ASME Trans. Mechatron. 2007, 12, 408–417. [Google Scholar] [CrossRef]
- Oblak, J.; Cikajlo, I.; Matjacić, Z. Universal haptic unit: A robot for rehabilitation of arms and wrists. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Kang, S.H.; Park, H.S.; Wu, Y.N.; Zhang, L.Q. Developing a multi-joint upper limb exoskeleton robot for diagnosis, therapy, and outcome evaluation in neurorehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Squeri, V.; Masia, L.; Giannoni, P.; Sandini, G.; Morasso, P. Wrist rehabilitation in chronic stroke patients by means of adaptive, progressive robot-aided therapy. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Amirabdollahian, F.; Ates, S.; Basteris, A.; Cesario, A.; Buurke, J.; Hermens, H.; Hofs, D.; Johansson, E.; Mountain, G.; Nasr, N.; et al. Design, development and implantation of a hand/wrist exoskeleton for home rehabilitation after stroke—SCRIPT project. Robotica 2014, 32, 1331–1346. [Google Scholar] [CrossRef]
- Buongiorno, D.; Sotgiu, E.; Leonardis, D.; Marcheschi, S.; Solazzi, M.; Frisoli, A. WRES: A new 3 DoF WRist ExoSkeleton with tendon-oriented differential transmission for neuro-rehabilitation and teleoperation. IEEE Robot. Autom. Lett. 2018, 3, 2152–2159. [Google Scholar] [CrossRef]
- Khor, K.X.; Chin, P.J.H.; Yeong, C.F.; Su, E.L.M.; Narayanan, A.L.T.; Rahman, H.A.; Khan, Q.I. Portable, reconfigurable wrist robot improves hand function for post-stroke individuals. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1864–1873. [Google Scholar] [CrossRef] [PubMed]
- Khor, K.X.; Chin, P.J.H.; Hisyam, A.R.; Yeong, C.F.; Narayanan, A.L.T.; Su, E.L.M. Development of CR2-haptic: A compact and portable rehabilitation robot for wrist and forearm training. In Proceedings of the 2014 IEEE Conference on Biomedical Engineering and Sciences (IECBES), Kuala Lumpur, Malaysia, 8–10 December 2014; pp. 424–429. [Google Scholar]
- Higuma, T.; Kiguchi, K.; Arata, J. Low-profile two-degree-of-freedom wrist exoskeleton device using multiple spring blades. IEEE Robot. Autom. Lett. 2018, 3, 305–311. [Google Scholar] [CrossRef]
- Mayetin, U.; Kucuk, S. Design and Experimental Evaluation of a Low Cost, Portable, 3-DOF Wrist Rehabilitation Robot with High Physical Human–Robot Interaction. J. Intell. Robot. Syst. 2022, 106, 65. [Google Scholar] [CrossRef]
- Pitzalis, R.F.; Park, D.; Caldwell, D.G.; Berselli, G.; Ortiz, J. State of the Art in Wearable Wrist Exoskeletons Part I: Background Needs and Design Requirements. Machines 2023, 11, 458. [Google Scholar] [CrossRef]
- Alves, T.; Gonçalves, R.S.; Carbone, G. Serious Games Strategies with Cable-Driven Robots for Bimanual Rehabilitation: A Randomized Controlled Trial with Post-Stroke Patients. Front. Robot. AI 2022, 9, 739088. [Google Scholar] [CrossRef] [PubMed]
- Andrade, K.O.; Fernandes, G.; Martins, J.; Roma, V.; Joaquim, R.C.; Caurin, G.A.P. Rehabilitation Robotics and Serious Games: An Early Architecture for Concurrent Players. In Proceedings of the IEEE Biosignals and Biorobotics Conference (BRC), 2013 ISSNIP (BRC2013), Rio de Janeiro, Brazil, 18–20 February 2013; pp. 1, 6, 18–20. [Google Scholar]
- Gu, Y.; Xu, Y.; Shen, Y.; Huang, H.; Liu, T.; Jin, L.; Ren, H.; Wang, J. A Review of Hand Function Rehabilitation Systems Based on Hand Motion Recognition Devices and Artificial Intelligence. Brain Sci. 2022, 12, 1079. [Google Scholar] [CrossRef] [PubMed]
- Vasconcelos, G.B.O. Use of Artificial Intelligence Techniques for the Development of Serious Games Applied to Robotic Structure for Human wrist Rehabilitation; 2023. 74 f. Final Paper (Graduation in Mechatronics Engineering); Federal University of Uberlândia: Uberlândia, Brazil, 2023. [Google Scholar]
- Rafiq, A.; Kadir, T.A.A.; Ihsan, S.N. A Review of Artificial Intelligence in Serious Game for Public Health. J. Phys. Conf. Ser. 2021, 1830, 012001. [Google Scholar] [CrossRef]
- Tolks, D.; Schmidt, J.J.; Kuhn, S. The Role of AI in Serious Games and Gamification for Health: Scoping Review. JMIR Serious Games 2024, 12, e48258. [Google Scholar] [CrossRef] [PubMed]
- Pitzalis, R.F.; Park, D.; Caldwell, D.G.; Berselli, G.; Ortiz, J. State of the Art in Wearable Wrist Exoskeletons Part II: A Review of Commercial and Research Devices. Machines 2024, 12, 21. [Google Scholar] [CrossRef]
- Vatan, H.M.F.; Nefti-Meziani, S.; Davis, S.; Saffari, Z.; El-Hussieny, H. A review: A Comprehensive Review of Soft and Rigid Wearable Rehabilitation and Assistive Devices with a Focus on the Shoulder Joint. J. Intell. Robot. Syst. 2021, 102, 9. [Google Scholar] [CrossRef]





| Parameter | Value | Unites |
|---|---|---|
| Hand mass [m] | 0.006·M | [kg] |
| Hand length [L] | 0.108·H | [m] |
| Proximal center of gravity [I] | 0.506·L | [m] |
| Radius of gyration of hand [k] | 0.297·L | [m] |
| Gravity [g] | 9.81 | [m/s2] |
| Moment of inertia of hand [J] | m·k2 | [kg·m2] |
| Damping coefficient [b] | 0.1 | [N·m·s] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, G.F.; Gonçalves, R.S.; Carbone, G. A Review of Wrist Rehabilitation Robots and Highlights Needed for New Devices. Machines 2024, 12, 315. https://doi.org/10.3390/machines12050315
Garcia GF, Gonçalves RS, Carbone G. A Review of Wrist Rehabilitation Robots and Highlights Needed for New Devices. Machines. 2024; 12(5):315. https://doi.org/10.3390/machines12050315
Chicago/Turabian StyleGarcia, Gabriella Faina, Rogério Sales Gonçalves, and Giuseppe Carbone. 2024. "A Review of Wrist Rehabilitation Robots and Highlights Needed for New Devices" Machines 12, no. 5: 315. https://doi.org/10.3390/machines12050315
APA StyleGarcia, G. F., Gonçalves, R. S., & Carbone, G. (2024). A Review of Wrist Rehabilitation Robots and Highlights Needed for New Devices. Machines, 12(5), 315. https://doi.org/10.3390/machines12050315