
The Influence of the Dominant Leg on Angle Trunk Rotation and Postural Symmetries in Adolescent Male Soccer Players: A Comparative Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Scoliosis Screening
2.4. Statistical Analysis
3. Results
3.1. Descriptive
3.2. Chi-Square
3.3. Mann–Whitney U Test
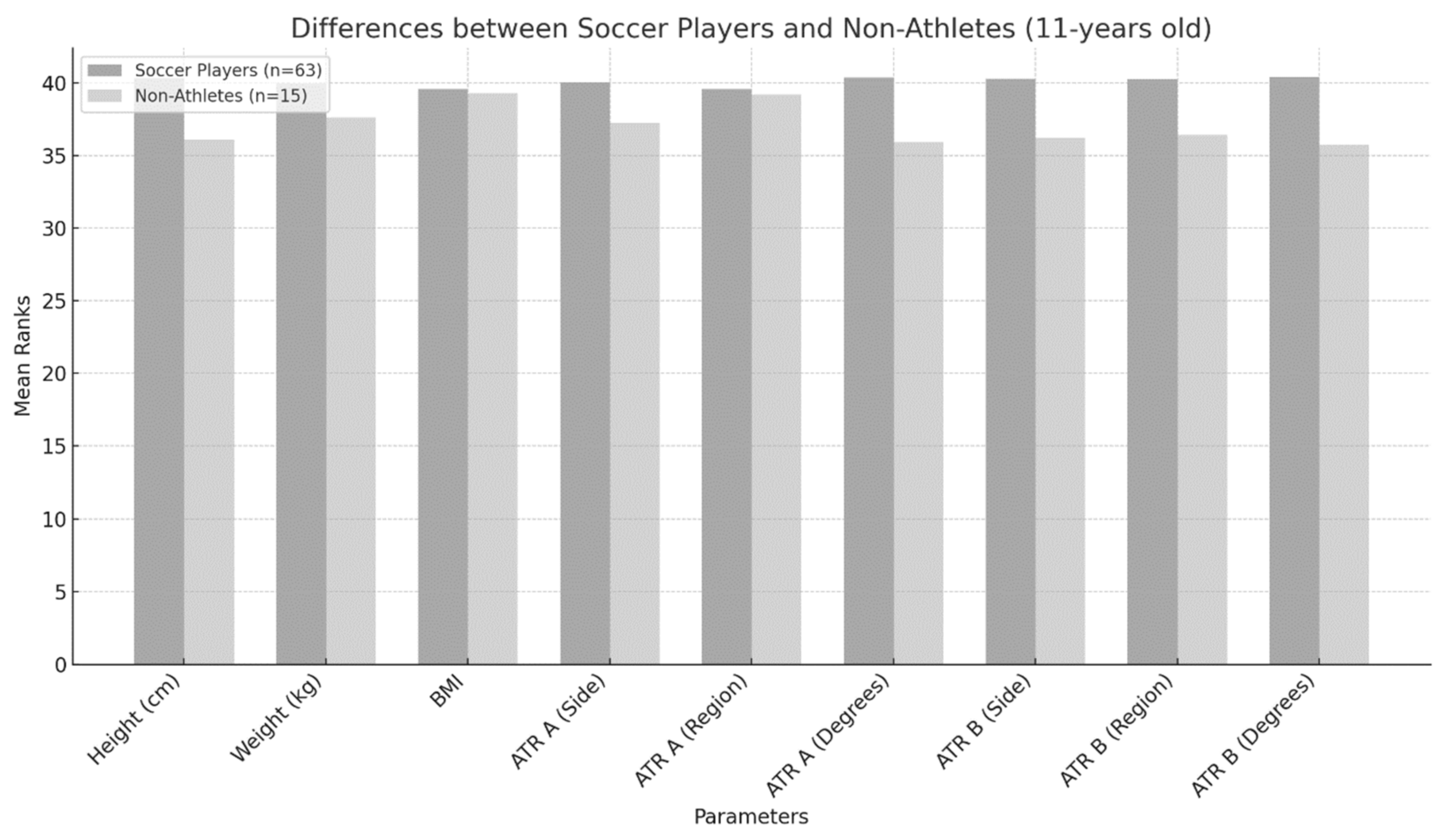
- 11 years of age
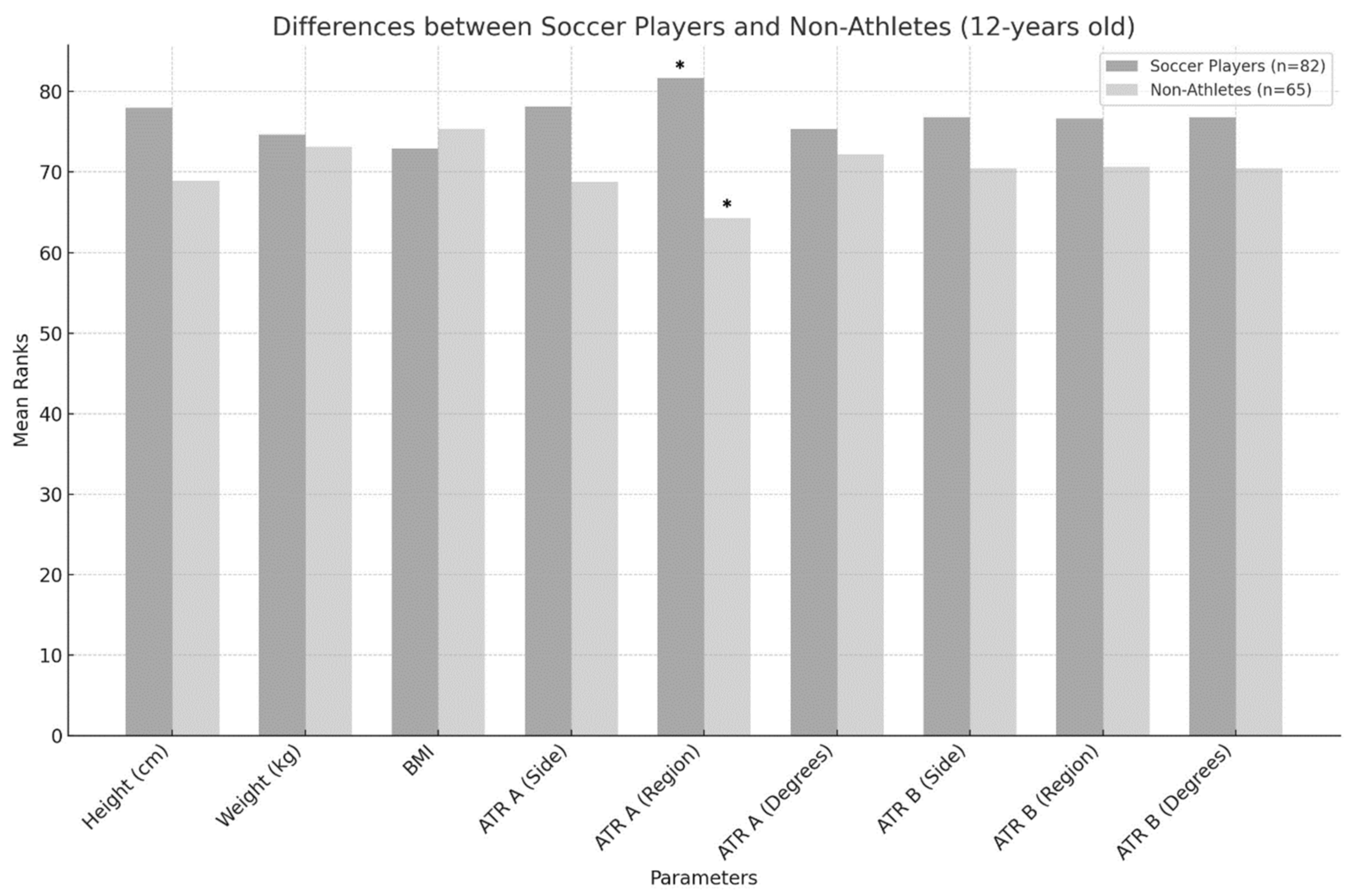
- 12 years of age
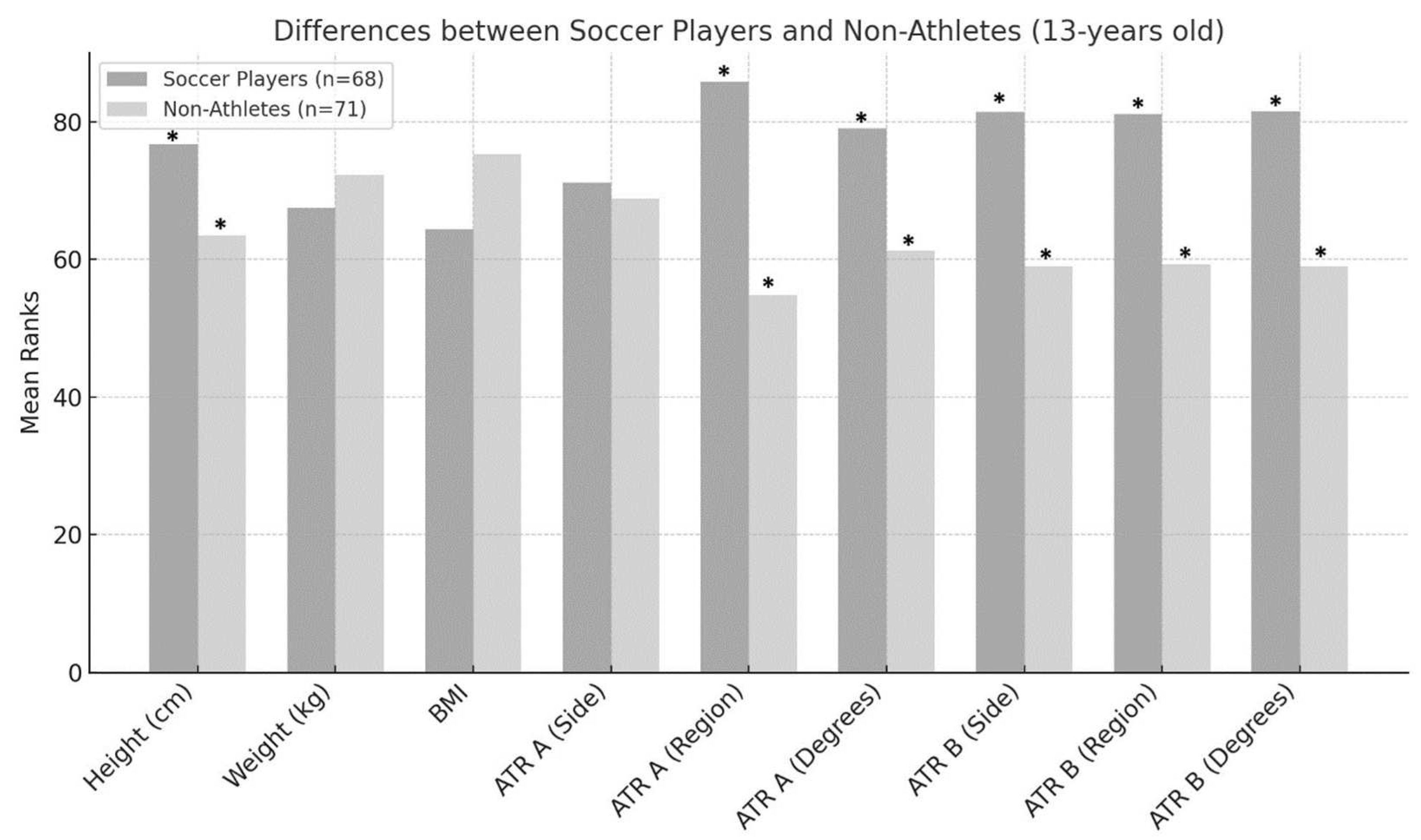
- 13 years of age
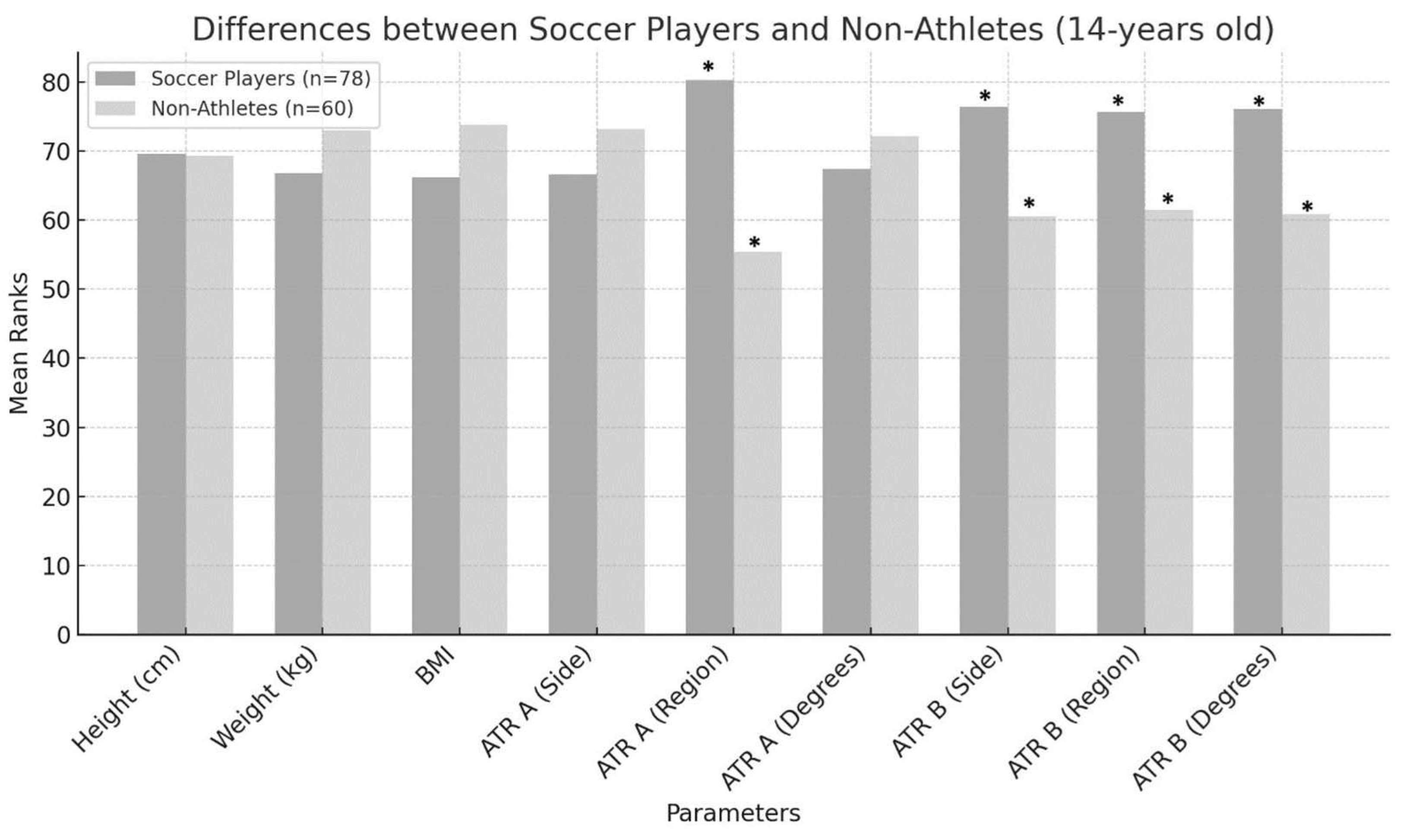
- 14 years of age
4. Discussion
4.1. Laterality
4.2. Differences Between Soccer Players and Non-Athletes per Age Group
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Magee, D.J. Orthopedic Physical Assessment, 6th ed.; Saunders, Elservier Inc.: North York, ON, Canada, 2014. [Google Scholar]
- Ciortea, V.; Ungur, R.; Irsay, L.; Onac, I.; Popa, A.; Popa, D.; Borda, I.M. Classification of scoliosis. Palestrica Third Millenn. Civiliz. Sport 2014, 15, 353–356. [Google Scholar]
- Theodorou, E.; Hadjicharalambous, M.; Tryfonidis, M. School Scoliosis Screening: The Influence of Dominant Limbs and Gender. Adolescents 2024, 4, 62–74. [Google Scholar] [CrossRef]
- Wik, E.H.; Martínez-Silván, D.; Farooq, A.; Cardinale, M.; Johnson, A.; Bahr, R. Skeletal Maturation and Growth Rates Are Related to Bone and Growth Plate Injuries in Adolescent Athletics. Scand. J. Med. Sci. Sports 2020, 30, 894–903. [Google Scholar] [CrossRef] [PubMed]
- Theodorou, E.; Christou, M.; Apostolidis, A.; Tryfonidis, M.; Zaras, N.; Hadjicharalambous, M. The Effect of Spinal Asymmetries on Physical Fitness Parameters in Young Elite Soccer Players. Symmetry 2022, 14, 2497. [Google Scholar] [CrossRef]
- Kendall, F.P.; Kendall, F.P. (Eds.) Muscles: Testing and Function with Posture and Pain, 5th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2005. [Google Scholar]
- Theodorou, E.; Grivas, T.B.; Hadjicharalambous, M. The Influence of the Dominant Leg in Body Asymmetries in Children and Adolescent Male Soccer Players. Pediatr. Rep. 2024, 16, 684–695. [Google Scholar] [CrossRef] [PubMed]
- Asadi, M.; Nourasteh, A.; Daneshmandi, H. Comparison of Spinal Column Curvatures Between Master Football Players and Their Non-Athletes Peers. IJSS 2014, 4, 338–342. [Google Scholar]
- Grabara, M. Analysis of Body Posture Between Young Football Players and Their Untrained Peers. Hum. Mov. 2012, 13, 120–126. [Google Scholar] [CrossRef]
- Theodorou, E.; Tryfonidis, M.; Zaras, N.; Hadjicharalambous, M. Musculoskeletal Asymmetries in Young Soccer Players: 8 Weeks of an Applied Individual Corrective Exercise Intervention Program. Appl. Sci. 2023, 13, 6445. [Google Scholar] [CrossRef]
- Marques, V.B.; Medeiros, T.M.; de Stigger, F.S.; Nakamura, F.Y.; Baroni, B.M. The Functional Movement Screen (FMSTM) in Elite Young Soccer Players Between 14 and 20 Years: Composite Score, Individual-test Scores and Asymmetries. Int. J. Sports Phys. Ther. 2017, 12, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Tamura, A. Body Composition Asymmetry between Dominant and Non-Dominant Arms in Experienced Overhead Throwing Sports Athletes. J. Sports Med. Phys. Fit. 2024, 64, 1071–1078. [Google Scholar] [CrossRef]
- Bona, C.C.; Filho, H.T.; Izquierdo, M.; Ferraz, R.M.P.; Marques, M.C. Peak Torque and Muscle Balance in the Knees of Young U-15 and U-17 Soccer Athletes Playing Various Tactical Positions. J. Sports Med. Phys. Fit. 2017, 57, 923–929. [Google Scholar] [CrossRef]
- Corso, M. Developmental Changes in the Youth Athlete: Implications for Movement, Skills Acquisition, Performance and Injuries. J. Can. Chiropr. Assoc. 2018, 62, 150–160. [Google Scholar] [PubMed]
- Rouissi, M.; Chtara, M.; Owen, A.; Chaalali, A.; Chaouachi, A.; Gabbett, T.; Chamari, K. Effect of Leg Dominance on Change of Direction Ability amongst Young Elite Soccer Players. J. Sports Sci. 2016, 34, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Van Dillen, L.R.; Bloom, N.J.; Gombatto, S.P.; Susco, T.M. Hip Rotation Range of Motion in People with and without Low Back Pain Who Participate in Rotation-Related Sports. Phys. Ther. Sport 2008, 9, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Bussey, M.D. Does the Demand for Asymmetric Functional Lower Body Postures in Lateral Sports Relate to Structural Asymmetry of the Pelvis? J. Sci. Med. Sport 2010, 13, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C.; Turner, A.; Read, P. Effects of Inter-Limb Asymmetries on Physical and Sports Performance: A Systematic Review. J. Sports Sci. 2018, 36, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Osiński, W. Antropomotoryka, 2nd ed.; AWF Poznań: Poznań, Poland, 2003. [Google Scholar]
- Arienti, C.; Buraschi, R.; Donzelli, S.; Zaina, F.; Pollet, J.; Negrini, S. Trunk Asymmetry Is Associated with Dominance Preference: Results from a Cross-Sectional Study of 1029 Children. Braz. J. Phys. Ther. 2019, 23, 324–328. [Google Scholar]
- Scaturro, D.; de Sire, A.; Terrana, P.; Costantino, C.; Lauricella, L.; Sannasardo, C.E.; Vitale, F.; Mauro, G.L. Adolescent Idiopathic Scoliosis Screening: Could a School-Based Assessment Protocol Be Useful for an Early Diagnosis? J. Back Musculoskelet. Rehabil. 2021, 34, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; De Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT Guidelines: Orthopaedic and Rehabilitation Treatment of Idiopathic Scoliosis during Growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef]
- Rosenthal, R. Meta-Analysis: A Review. Psychosom. Med. 1991, 53, 247–271. [Google Scholar] [PubMed]
- Cohen, J. (Ed.) Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 1988. [Google Scholar]
- Latalski, M.; Danielewicz-Bromberek, A.; Fatyga, M.; Latalska, M.; Kröber, M.; Zwolak, P. Current Insights into the Aetiology of Adolescent Idiopathic Scoliosis. Arch. Orthop. Trauma Surg. 2017, 137, 1327–1333. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, O.; Mazet, C.; Mazet, D.; Hammes, A.; Schmitt, E. Age-Dependency of Posture Parameters in Children and Adolescents. J. Phys. Ther. Sci. 2016, 28, 1607–1610. [Google Scholar] [PubMed]
- Yang, L.; Lu, X.; Yan, B.; Huang, Y. Prevalence of Incorrect Posture among Children and Adolescents: Finding from a Large Population-Based Study in China. iScience 2020, 23, 101043. [Google Scholar] [CrossRef]
- Stokes, I.A.F. Analysis and Simulation of Progressive Adolescent Scoliosis by Biomechanical Growth Modulation. Eur. Spine J. 2007, 16, 1621–1628. [Google Scholar] [PubMed]
- Mahrová, A.; Hráský, P.; Zahálka, F.; Požárek, P. The Effect of Two Types of Stretching on Flexibility in Selected Joints in Youth Soccer Players. Acta Gymnica 2014, 44, 23–32. [Google Scholar]
- Xing, L.; Popik, S. A Systematic Review of the Impact of Sports on Body Posture in Adolescents. J. Med. Imaging Health Inform. 2020, 10, 1159–1164. [Google Scholar]
- Lourenço, J.F.D.S.; De Sousa, J.L.M.A.; Soares, D.P.; Gonçalves-Lopes, S.C. Postural Analysis of Male Football Athletes from Different Age Levels of Training. Eur. J. Med. Health Sci. 2021, 3, 100–105. [Google Scholar] [CrossRef]
- Barczyk-Pawelec, K.; Rubajczyk, K.; Stefańska, M.; Pawik, Ł.; Dziubek, W. Characteristics of Body Posture in the Sagittal Plane in 8–13-Year-Old Male Athletes Practicing Soccer. Symmetry 2022, 14, 210. [Google Scholar] [CrossRef]
- Kalata, M.; Maly, T.; Hank, M.; Michalek, J.; Bujnovsky, D.; Kunzmann, E.; Zahalka, F. Unilateral and Bilateral Strength Asymmetry among Young Elite Athletes of Various Sports. Medicina 2020, 56, 683. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sub-Groups | Height (cm) | Weight (kg) | ATR-A (°) | ATR-B (°) | |
|---|---|---|---|---|---|
| Soccer Players (n = 291) | 11 yrs (n = 63) | 147 ± 6 | 41.5 ± 7.8 | 2 ± 3 | 0 ± 0 |
| 12 yrs (n = 82) | 153 ± 11 | 47.1 ± 9.6 | 2 ± 1 | 0 ± 0 | |
| 13 yrs (n = 68) | 163 ± 15 | 54.1 ± 11.8 | 3 ± 2 | 0 ± 3 | |
| 14 yrs (n = 78) | 168 ± 12 | 58.5 ± 11.2 | 3 ± 2 | 0 ± 2 | |
| Non-Athletes (n = 211) | 11 yrs (n = 15) | 146 ± 7 | 40.7 ± 10.7 | 2 ± 2 | 0 ± 0 |
| 12 yrs (n = 65) | 152 ± 8 | 44.4 ± 14.4 | 2 ± 3 | 0 ± 0 | |
| 13 yrs (n = 71) | 159 ± 10 | 53.9 ± 20.9 | 2 ± 2 | 0 ± 0 | |
| 14 yrs (n = 60) | 168 ± 7 | 59.2 ± 55.6 | 3 ± 2 | 0 ± 0 |
| Soccer Players—Age Categories | |||||
|---|---|---|---|---|---|
| ATR-A | 11 years old | 12 years old | 13 years old | 14 years old | Total |
| 0–2 degrees | 50.8% (n = 32) | 54.9% (n = 45) | 41.2% (n = 28) | 42.3% (n = 33) | 47.4% (n = 138) |
| 3–5 degrees | 42.9% (n = 27) | 43.9% (n = 36) | 51.5% (n = 35) | 51.3% (n = 40) | 47.4% (n = 138) |
| ≥6 degrees | 6.3% (n = 4) | 1.2% (n = 1) | 7.3% (n = 5) | 6.4% (n = 5) | 5.2% (n = 15) |
| Total | 100% (n = 63) | 100% (n = 82) | 100% (n = 68) | 100% (n = 78) | 100% (n = 291) |
| ATR-B | 11 years old | 12 years old | 13 years old | 14 years old | Total |
| 0–2 degrees | 88.55% (n = 52) | 89% (n = 73) | 70.6% (n = 48) | 82% (n = 64) | 81.4% (n = 237) |
| 3–5 degrees | 17.5% (n = 11) | 10.1% (n = 9) | 29.4% (n = 20) | 16.7% (n = 13) | 18.2% (n = 53) |
| ≥6 degrees | 0% (n = 0) | 0% (n = 0) | 0% (n = 0) | 1.3% (n = 1) | 0.3% (n = 1) |
| Total | 100% (n = 63) | 100% (n = 82) | 100% (n = 68) | 100% (n = 78) | 100% (n = 291) |
| Non-Athletes—Age Categories | |||||
|---|---|---|---|---|---|
| ATR-A | 11 years old | 12 years old | 13 years old | 14 years old | Total |
| 0–2 degrees | 60% (n = 9) | 50.8% (n = 33) | 53.9% (n = 39) | 43.3% (n = 26) | 50.7% (n = 107) |
| 3–5 degrees | 33.3% (n = 5) | 46.1% (n = 30) | 44.7% (n = 31) | 46.7% (n = 28) | 44.5% (n = 94) |
| ≥ 6 degrees | 6.7% (n = 1) | 3.1% (n = 2) | 1.4% (n = 1) | 10% (n = 6) | 4.7% (n = 10) |
| Total | 100% (n = 15) | 100% (n = 65) | 100% (n = 71) | 100% (n = 60) | 100% (n = 211) |
| ATR-B | 11 years old | 12 years old | 13 years old | 14 years old | Total |
| 0–2 degrees | 100% (n = 15) | 96.9% (n = 63) | 98.6% (n = 70) | 93.3% (n = 56) | 96.7% (n = 204) |
| 3–5 degrees | 0% (n = 0) | 3.1% (n = 2) | 1.4% (n = 1) | 6.7% (n = 4) | 3.3% (n = 7) |
| Total | 100% (n = 15) | 100% (n = 65) | 100% (n = 71) | 100% (n = 60) | 100% (n = 211) |
| Soccer Players—DL | |||||
|---|---|---|---|---|---|
| ATR (A) Side | Right | Left | Both | Total | |
| None | 14.5% (n = 34) | 17.8% (n = 8) | 33.3% (n = 4) | 15.8% (n = 46) | |
| Right | 21.4% (n = 50) | 57.8% (n = 26) | 25% (n = 3) | 27.1% (n = 79) | |
| Left | 64.1% (n = 150) | 24.4% (n = 11) | 41.7% (n = 5) | 57% (n = 166) | |
| Total | 100% (n = 234) | 100% (n = 45) | 100% (n = 12) | 100% (n = 291) | |
| ATR (B) Side | Right | Left | Both | Total | |
| None | 73.9% (n = 173) | 80% (n = 36) | 91.7% (n = 11) | 75.6% (n = 220) | |
| Right | 5.6% (n = 13) | 11.1% (n = 5) | 0% (n = 0) | 6.2% (n = 18) | |
| Left | 20.5% (n = 48) | 8.9% (n = 4) | 8.3% (n = 1) | 18.2% (n = 53) | |
| Total | 100% (n = 234) | 100% (n = 45) | 100% (n = 12) | 100% (n = 291) | |
| Non-Athletes—DL | ||||
|---|---|---|---|---|
| ATR (A) Side | Right | Left | Total | |
| None | 18.3% (n = 34) | 12% (n = 3) | 17.5% (n = 37) | |
| Right | 25.3% (n = 47) | 40% (n = 10) | 27% (n = 57) | |
| Left | 56.4% (n = 105) | 48% (n = 12) | 55% (n = 117) | |
| Total | 100% (n = 186) | 100% (n = 25) | 100% (n = 211) | |
| ATR (B) Side | Right | Left | Total | |
| None | 95.7% (n = 178) | 84% (n = 21) | 94.3% (n = 199) | |
| Right | 1.1% (n = 2) | 8% (n = 2) | 1.9% (n = 4) | |
| Left | 3.2% (n = 6) | 8% (n = 2) | 3.8% (n = 8) | |
| Total | 100% (n = 186) | 100% (n = 25) | 100% (n = 211) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theodorou, E.; Chalari, E.; Hadjicharalambous, M. The Influence of the Dominant Leg on Angle Trunk Rotation and Postural Symmetries in Adolescent Male Soccer Players: A Comparative Study. Symmetry 2025, 17, 94. https://doi.org/10.3390/sym17010094
Theodorou E, Chalari E, Hadjicharalambous M. The Influence of the Dominant Leg on Angle Trunk Rotation and Postural Symmetries in Adolescent Male Soccer Players: A Comparative Study. Symmetry. 2025; 17(1):94. https://doi.org/10.3390/sym17010094
Chicago/Turabian StyleTheodorou, Eleni, Eleanna Chalari, and Marios Hadjicharalambous. 2025. "The Influence of the Dominant Leg on Angle Trunk Rotation and Postural Symmetries in Adolescent Male Soccer Players: A Comparative Study" Symmetry 17, no. 1: 94. https://doi.org/10.3390/sym17010094
APA StyleTheodorou, E., Chalari, E., & Hadjicharalambous, M. (2025). The Influence of the Dominant Leg on Angle Trunk Rotation and Postural Symmetries in Adolescent Male Soccer Players: A Comparative Study. Symmetry, 17(1), 94. https://doi.org/10.3390/sym17010094