
Designing Healing Environments: A Literature Review on the Benefits of Healing Gardens for Children in Healthcare Facilities and the Urgent Need for Policy Implementation



Abstract
1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. Definition of a Healing Garden
3.2. Theories
3.3. The Value of Play and the Impact on Children’s Development
3.4. Policies
3.5. Challenges, Opportunities, and Best Practices
3.6. Research Gaps
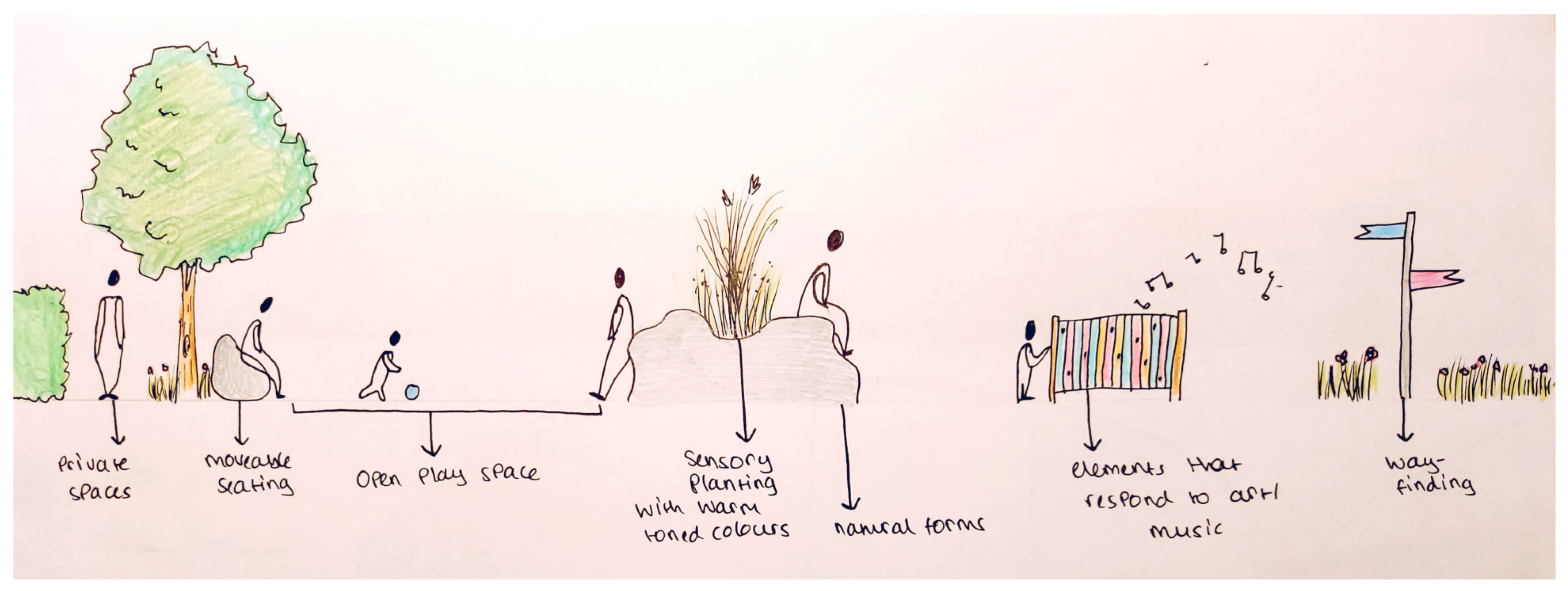
3.7. Design Recommendations
- Open space allowing for flexibility of play [91].
- Signage to location of garden (way finding) with accessible wheelchair-friendly paths [27].
- Sensory planting.
- Natural forms such as biomorphism and biomimicry.
- Elements that correspond to art and music (sculptures).
- Educational boards to explain what a healing garden is.
- Moveable seating.
- Private courtyard derived from the prospect–refuge theory [2].
3.8. Study Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Said, I. Therapeutic Effects of Garden: Preference of Ill Children Towards Garden Over Ward in Malaysian Hospital Environment. J. Teknol. 2003, 38, 55–68. [Google Scholar] [CrossRef]
- Marcus, C.C.; Sachs, N.A. Therapeutic Landscapes: An Evidence-Based Approach to Designing Healing Gardens and Restorative Outdoor Spaces; Wiley: Hoboken, NJ, USA, 2013; ISBN 9781118231913. [Google Scholar]
- Cartwright, M. Medieval Monastery. Available online: https://www.worldhistory.org/Medieval_Monastery/ (accessed on 5 January 2023).
- Whitehouse, S.; Varni, J.W.; Seid, M.; Cooper-Marcus, C.; Ensberg, M.J.; Jacobs, J.R.; Mehlenbeck, R.S. Evaluating a children’s hospital garden environment: Utilization and consumer satisfaction. J. Environ. Psychol. 2001, 21, 301–314. [Google Scholar] [CrossRef]
- Marcus, C.C. Healing Gardens in Hospitals. Des. Heal. 2007, 1, 1–27. [Google Scholar]
- Marcus, C.C.; Barnes, M. Healing Gardens: Therapeutic Benefits and Design Recommendations; Wiley Series in Healthcare and Senior Living Design; Wiley: Hoboken, NJ, USA, 1999; ISBN 9780471192039. [Google Scholar]
- Moorhouse, D. Disease in the Industrial Revolution. Available online: https://schoolshistory.org.uk/topics/british-history/industrial-revolution/disease-industrial-revolution/ (accessed on 5 January 2023).
- Read, E. Children’s Hospice Gardens: Using Nature to Enhance Well-Being; Elizabeth Read: Llangibby, UK, 2019. [Google Scholar]
- Cook, G.C. Henry Currey FRIBA (1820–1900): Leading Victorian hospital architect, and early exponent of the “pavilion principle”. Postgrad. Med. J. 2002, 78, 352–359. [Google Scholar] [CrossRef]
- Florence, N. Notes of Hospitals, 3rd ed.; Longman, Roberts and Green: London, UK, 1863. [Google Scholar]
- Morris, R.E. The Victorian ‘Change of Air’ as medical and social construction. J. Tour. Hist. 2018, 10, 49–65. [Google Scholar] [CrossRef]
- Reeve, A.; Nieberler-Walker, K.; Desha, C. Healing gardens in children’s hospitals: Reflections on benefits, preferences and design from visitors’ books. Urban For. Urban Green. 2017, 26, 48–56. [Google Scholar] [CrossRef]
- Ulrich, R. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef]
- Allahyar, M.; Kazemi, F. Effect of landscape design elements on promoting neuropsychological health of children. Urban For. Urban Green. 2021, 65, 127333. [Google Scholar] [CrossRef]
- Abdelaal, M.S.; Soebarto, V. Biophilia and Salutogenesis as restorative design approaches in healthcare architecture. Archit. Sci. Rev. 2019, 62, 195–205. [Google Scholar] [CrossRef]
- Paraskevopoulou, A.T.; Kamperi, E. Design of hospital healing gardens linked to pre- or post-occupancy research findings. Front. Archit. Res. 2018, 7, 395–414. [Google Scholar] [CrossRef]
- Andreucci, M.B.; Russo, A.; Olszewska-Guizzo, A. Designing Urban Green Blue Infrastructure for Mental Health and Elderly Wellbeing. Sustainability 2019, 11, 6425. [Google Scholar] [CrossRef]
- Jonveaux, T.R.; Batt, M.; Fescharek, R.; Benetos, A.; Trognon, A.; Bah Chuzeville, S.; Pop, A.; Jacob, C.; Yzoard, M.; Demarche, L.; et al. Healing Gardens and Cognitive Behavioral Units in the Management of Alzheimer’s Disease Patients: The Nancy Experience. J. Alzheimers Dis. 2013, 34, 325–338. [Google Scholar] [CrossRef]
- Uwajeh, P.C.; Iyendo, T.O.; Polay, M. Therapeutic gardens as a design approach for optimising the healing environment of patients with Alzheimer’s disease and other dementias: A narrative review. Explore 2019, 15, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Jonveaux, T.R.; Fescharek, R. When Art Meets Gardens: Does It Enhance the Benefits? The Nancy Hypothesis of Care for Persons with Alzheimer’s Disease. J. Alzheimers Dis. 2018, 61, 885–898. [Google Scholar] [CrossRef]
- Jesson, J.; Matheson, L.; Lacey, F.M. Doing Your Systematic Review—Taditional and Systematic Techniques; SAGE Publications Ltd.: London, UK, 2011; Volume 3, ISBN 9781848601543. [Google Scholar]
- Bandara, W.; Furtmueller, E.; Gorbacheva, E.; Miskon, S.; Beekhuyzen, J. Achieving Rigor in Literature Reviews: Insights from Qualitative Data Analysis and Tool-Support. Commun. Assoc. Inf. Syst. 2015, 37, 8. [Google Scholar] [CrossRef]
- Atkinson, L.Z.; Cipriani, A. How to carry out a literature search for a systematic review: A practical guide. BJPsych Adv. 2018, 24, 74–82. [Google Scholar] [CrossRef]
- Vapaa, A.G. Healing Gardens: Creating Places for Restoration, Meditation, and Sanctuary. Master’s Thesis, Virginia Polytechnic Institute and State University, Blacksburg, VA, USA, 2002. [Google Scholar]
- Tyson, M. The Healing Landscape: Therapeutic Outdoor Environments, 1st ed.; McGraw-Hill: London, UK, 1998; ISBN 0070657688 9780070657687. [Google Scholar]
- Krčmářová, J. EO Wilson’s concept of biophilia and the environmental movement in the USA. Internet J. Hist. Geogr. Environ. Hist. 2009, 6, 4–17. [Google Scholar]
- Marcus, C.C.; Barnes, M. Gardens in Healthcare Facilities: Uses, Therapeutic Benefits, and Design Recommendations; The Center for Health Design, Inc.: Concord, CA, USA, 1995. [Google Scholar]
- Hartig, T.; Marcus, C.C. Essay: Healing gardens-places for nature in health care. Lancet 2006, 368, 36–37. [Google Scholar] [CrossRef]
- Louv, R. Last Child in the Woods: Saving Our Children from Nature-Deficit Disorder, 1st ed.; Algonquin Books: Chapell Hill, NC, USA, 2005. [Google Scholar]
- Santer, J.; Griffiths, C.; Goodall, D.L. Free Play in Early Childhood: A Literature Review; National Children’s Bureau: London, UK, 2007; ISBN 9781905818105. [Google Scholar]
- Moore, R.C.; Goltsman, S.M.; Iacofano, D.S. Play for All Guidelines: Planning, Design, and Management of Outdoor Play Settings for All Children, 2nd ed.; MIG Communications: Berkeley, CA, USA, 1992. [Google Scholar]
- Gaminiesfahani, H.; Lozanovska, M.; Tucker, R. A Scoping Review of the Impact on Children of the Built Environment Design Characteristics of Healing Spaces. HERD Health Environ. Res. Des. J. 2020, 13, 98–114. [Google Scholar] [CrossRef]
- Pearson, M.; Gaines, K.; Pati, D.; Colwell, M.; Motheral, L.; Adams, N.G. The Physiological Impact of Window Murals on Pediatric Patients. HERD Health Environ. Res. Des. J. 2019, 12, 116–129. [Google Scholar] [CrossRef]
- Jiang, S. Therapeutic landscapes and healing gardens: A review of Chinese literature in relation to the studies in western countries. Front. Archit. Res. 2014, 3, 141–153. [Google Scholar] [CrossRef]
- Eckerling, M. Guidelines for designing healing gardens. J. Ther. Hortic. 1996, 8, 21–25. [Google Scholar]
- Lei, Y.; Jin, H.; Wang, J. The current status and prospect of healing garden. Chin. Landsc. Archit. 2011, 27, 31–36. [Google Scholar]
- Li, Q.; Tang, X. Quality evaluation index system of healing gardens. J. Shanghai Jiaotong Univ. Agric. Sci. 2012, 30, 58–64. [Google Scholar] [CrossRef]
- Wang, X.; Li, J. Analysis of the healing landscape and its relevant conceptions. J. Beijing Univ. Agric. 2012, 27, 71–73. [Google Scholar]
- Browning, W.D.; Ryan, C.O. Nature Inside—A Biophilic Design Guide; RIBA Publishing: London, UK, 2020; ISBN 9781003033011. [Google Scholar]
- Rogers, K. Biophilia Hypothesis. Available online: https://www.britannica.com/science/biophilia-hypothesis (accessed on 10 March 2023).
- Wilson, E.O. Biophilia; Harvard University Press: Cambridge, UK, 1986. [Google Scholar]
- Montgomery, J. Nature as Healer and Teacher—The Importance of Reconnecting Children to the Earth for Physical and Emotional Wellbeing; City University of Seattle: Seattle, WA, USA, 2015. [Google Scholar]
- Russo, A.; Andreucci, M.B. Raising Healthy Children: Promoting the Multiple Benefits of Green Open Spaces through Biophilic Design. Sustainability 2023, 15, 1982. [Google Scholar] [CrossRef]
- Zhong, W.; Schröder, T.; Bekkering, J. Biophilic design in architecture and its contributions to health, well-being, and sustainability: A critical review. Front. Archit. Res. 2022, 11, 114–141. [Google Scholar] [CrossRef]
- Kellert, S.R.; Heerwagen, J.; Mador, M. Biophilic Design: The Theory, Science, and Practice of Bringing Buildings to Life; Wiley: Hoboken, NJ, USA, 2008; ISBN 9780470163344 0470163348. [Google Scholar]
- Sadick, A.-M.; Kamardeen, I. Enhancing employees’ performance and well-being with nature exposure embedded office workplace design. J. Build. Eng. 2020, 32, 101789. [Google Scholar] [CrossRef]
- Dankner, S. Using Positive Visual Distractions and Color in Healthcare Settings to Reduce Patient Stress & Increase Patient Satisfaction. Available online: https://www.c-sgroup.com/-/media/files/literature/awp/flyers/sally_dankner_white_paper.ashx (accessed on 14 March 2023).
- Lacy, M.L. The Power of Colour to Heal the Environment; Rainbow Bridge: London, UK, 1996; ISBN 0952870002 9780952870005. [Google Scholar]
- Park, J.G. Color Perception in Pediatric Patient Room Design: Healthy Children vs. Pediatric Patients. HERD Health Environ. Res. Des. J. 2009, 2, 6–28. [Google Scholar] [CrossRef] [PubMed]
- Kellert, S.R.; Calabrese, E.F. The Practice of Biophilic Design; Biophilic Design: 2015. Available online: www.biophilic-design.com (accessed on 14 March 2023).
- Biomimicry Institute. What Is Biomimicry? Available online: https://biomimicry.org/what-is-biomimicry/ (accessed on 14 March 2023).
- Tate Biomorphic—Art Term. Available online: https://www.tate.org.uk/art/art-terms/b/biomorphic (accessed on 10 March 2023).
- Soderlund, J.; Newman, P. Biophilic architecture: A review of the rationale and outcomes. AIMS Environ. Sci. 2015, 2, 950–969. [Google Scholar] [CrossRef]
- Bloemsma, L.D.; Wijga, A.H.; Klompmaker, J.O.; Hoek, G.; Janssen, N.A.H.; Oldenwening, M.; Koppelman, G.H.; Lebret, E.; Brunekreef, B.; Gehring, U. Green space, air pollution, traffic noise and saliva cortisol in children. Environ. Epidemiol. 2021, 5, e141. [Google Scholar] [CrossRef]
- Harari, Y.N. Sapiens: A Brief History of Humankind; Harvill Secker: London, UK, 2014; ISBN 1846558239. [Google Scholar]
- Kellert, S.R.; Wilson, E.O. The Biophilia Hypothesis; Island Press: Washington DC, WA, USA, 1993; Volume 4. [Google Scholar]
- Sternberg, E.M. Healing Spaces: The Science of Place and Well-Being, 1st ed.; Belknap Press of Harvard University Press: Cambridge, UK, 2010; ISBN 9780674057487. [Google Scholar]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989; ISBN 0-521-34139-6/0-521-34939-7. [Google Scholar]
- Shackell, A.; Walter, R. Greenspace Design for Health and Well-Being; Forestry Commission: Edinburgh, Scotland, 2012; ISBN 9780855388539. [Google Scholar]
- Holmes, D. The Landscape Spaces of Nelson Mandela Children’s Hospital. Available online: https://worldlandscapearchitect.com/the-landscape-spaces-of-nelson-mandela-childrens-hospital/?v=79cba1185463#.YyR6uXbMJPY (accessed on 14 March 2023).
- Souter-Brown, G. Landscape and Urban Design for Health and Well-Being: Using Healing, Sensory and Therapeutic Gardens; Routledge: Oxfordshire, UK, 2015; ISBN 0415843529. [Google Scholar]
- Stigsdotter, U.; Grahn, P. What makes a garden a healing garden? J. Ther. Hortic. 2002, 13, 60–69. [Google Scholar]
- Gesler, W.M. Healing Places; G—Reference, Information and Interdisciplinary Subjects Series; Rowman & Littlefield: Lanham, MD, USA, 2003; ISBN 9780742519565. [Google Scholar]
- Han, K.-T.; Ruan, L.-W.; Liao, L.-S. Effects of Indoor Plants on Human Functions: A Systematic Review with Meta-Analyses. Int. J. Environ. Res. Public Health 2022, 19, 7454. [Google Scholar] [CrossRef]
- Heft, H. Affordances and the perception of landscape: An inquiry into environmental perception and aesthetics. In Innovative Approaches to Researching Landscape and Health: Open Space: People Space 2; Ward-Thompson, C., Aspinall, P., Bell, S., Eds.; Routledge: Abingdon, UK, 2010. [Google Scholar]
- Gibson, J.J. The Ecological Approach to Visual Perception; Psychology Press: New York, NY, USA, 2014; ISBN 9781315740218. [Google Scholar]
- Gordon-Rawlings, T.; Russo, A. Exploring the effects of the COVID-19 pandemic on people’s relationships with gardens. Emot. Sp. Soc. 2023, 46, 100936. [Google Scholar] [CrossRef]
- Golembiewski, J.A. Salutogenic Architecture in Healthcare Settings. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Espnes, G.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 267–276. ISBN 9783319046006. [Google Scholar]
- Rynor, B. Beautifying hospitals: A tough sell. Can. Med. Assoc. J. 2010, 182, E633–E634. [Google Scholar] [CrossRef] [PubMed]
- Bento, G.; Dias, G. The importance of outdoor play for young children’s healthy development. Porto Biomed. J. 2017, 2, 157–160. [Google Scholar] [CrossRef]
- Almon, J. Improving Children’s Health through Play: Exploring Issues and Recommendations; Alliance for Childhood and US Play Coalition: College Park, MD, USA, 2018. [Google Scholar]
- Panksepp, J. Can PLAY diminish ADHD and facilitate the construction of the social brain? J. Can. Acad. Child Adolesc. Psychiatry 2007, 16, 57–66. [Google Scholar] [PubMed]
- Hillman, C.H.; Pontifex, M.B.; Raine, L.B.; Castelli, D.M.; Hall, E.E.; Kramer, A.F. The effect of acute treadmill walking on cognitive control and academic achievement in preadolescent children. Neuroscience 2009, 159, 1044–1054. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children. Med. Sci. Sport. Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef] [PubMed]
- Ulset, V.; Vitaro, F.; Brendgen, M.; Bekkhus, M.; Borge, A.I.H. Time spent outdoors during preschool: Links with children’s cognitive and behavioral development. J. Environ. Psychol. 2017, 52, 69–80. [Google Scholar] [CrossRef]
- Koukourikos, K.; Tzeha, L.; Pantelidou, P.; Tsaloglidou, A. The Importance of Play During Hospitalization of Children. Mater. Socio Med. 2015, 27, 438. [Google Scholar] [CrossRef]
- Parizi, M.K. Children’s Healing Garden V2.00. Available online: https://worldarchitecture.org/architecture-projects/hvghe/children-s-healing-garden-v2-00-project-pages.html (accessed on 5 January 2023).
- Frost, J.L. Lessons from Disasters: Play, Work, and the Creative Arts. Child. Educ. 2005, 82, 2–8. [Google Scholar] [CrossRef]
- Tremblay, M.; Gray, C.; Babcock, S.; Barnes, J.; Bradstreet, C.; Carr, D.; Chabot, G.; Choquette, L.; Chorney, D.; Collyer, C.; et al. Position Statement on Active Outdoor Play. Int. J. Environ. Res. Public Health 2015, 12, 6475–6505. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.-Y.; Herwig, J.E.; Shelley, M. Preschoolers’ Play Behaviors with Peers in Classroom and Playground Settings. J. Res. Child. Educ. 2001, 15, 149–163. [Google Scholar] [CrossRef]
- Hartle, L. Effects of Additional Materials on Preschool Children’s Outdoor Play Behaviors. J. Res. Child. Educ. 1996, 11, 68–81. [Google Scholar] [CrossRef]
- Cullen, J. Preschool children’s use and perceptions of outdoor play areas. Early Child Dev. Care 1993, 89, 45–56. [Google Scholar] [CrossRef]
- Schofield, E. How the Van Campenvaart Playground Is Breaking Boundries. Available online: https://land8.com/how-the-van-campenvaart-playground-is-breaking-boundries/ (accessed on 5 January 2023).
- Woolley, H.; Lowe, A. Exploring the Relationship between Design Approach and Play Value of Outdoor Play Spaces. Landsc. Res. 2013, 38, 53–74. [Google Scholar] [CrossRef]
- Jiang, S. Positive Distractions and Play in the Public Spaces of Pediatric Healthcare Environments: A Literature Review. HERD Health Environ. Res. Des. J. 2020, 13, 171–197. [Google Scholar] [CrossRef]
- Corsano, P.; Majorano, M.; Vignola, V.; Guidotti, L.; Izzi, G. The waiting room as a relational space: Young patients and their families’ experience in a day hospital. Child. Care. Health Dev. 2015, 41, 1066–1073. [Google Scholar] [CrossRef]
- Little Journey Limited. The Power of Play in Healthcare. Available online: https://www.littlejourney.health/news/power-of-play-in-healthcare (accessed on 13 April 2023).
- Starlight Children’s Foundation. The Importance of Play in Hospital 2021; Starlight Children’s Foundation: London, UK, 2021. [Google Scholar]
- Halim Babbu, A.; Haque, M. A framework for the design of pediatric healthcare environment using the Delphi technique. Ain Shams Eng. J. 2023, 14, 101975. [Google Scholar] [CrossRef]
- Plan Inclusive Play Area. PiPA (Plan Inclusive Play Area): The Complete Checklist; Inclusive Play: Loanhead, UK, 2015. [Google Scholar]
- Scottish Government. Out to Play—Creating Outdoor Play Experiences for Children: Practical Guidance. Available online: https://www.gov.scot/publications/out-play-practical-guidance-creating-outdoor-play-experiences-children/pages/9/ (accessed on 5 January 2023).
- British Lung Foundation. Toxic Air at the Door of the NHS—British Lung Foundation. Available online: https://www.blf.org.uk/take-action/campaign/nhs-toxic-air-report (accessed on 5 January 2023).
- Diener, A.; Mudu, P. How can vegetation protect us from air pollution? A critical review on green spaces’ mitigation abilities for air-borne particles from a public health perspective—With implications for urban planning. Sci. Total Environ. 2021, 796, 148605. [Google Scholar] [CrossRef] [PubMed]
- Global Action Plan. Great Ormond Street Hospital’s Clean Air Journey. Available online: https://www.actionforcleanair.org.uk/health/clean-air-hospital-framework/gosh-clean-air-hospital (accessed on 5 January 2023).
- Mace, B.L.; Bell, P.A.; Loomis, R.J. Aesthetic, affective, and cognitive effects of noise on natural landscape assessment. Soc. Nat. Resour. 1999, 12, 225–242. [Google Scholar] [CrossRef]
- Ow, L.F.; Ghosh, S. Urban cities and road traffic noise: Reduction through vegetation. Appl. Acoust. 2017, 120, 15–20. [Google Scholar] [CrossRef]
- United Nations. General Assembly Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Russo, A.; Cirella, G.T. Urban Sustainability: Integrating Ecology in City Design and Planning. In Sustainable Human—Nature Relations: Environmental Scholarship, Economic Evaluation, Urban Strategies; Cirella, G.T., Ed.; Springer: Singapore, 2020; pp. 187–204. ISBN 978-981-15-3049-4. [Google Scholar]
- Russo, A.; Escobedo, F.J.; Cirella, G.T.; Zerbe, S. Edible green infrastructure: An approach and review of provisioning ecosystem services and disservices in urban environments. Agric. Ecosyst. Environ. 2017, 242, 53–66. [Google Scholar] [CrossRef]
- O’Neill, C. The Healing Gardens of Makahikilua: The Landscape as a Healer. J. Ther. Hortic. 1996, 8, 92–96. [Google Scholar]
- The Edible Healing Garden Edible Healing Garden. Available online: https://www.ediblehealinggarden.org/about (accessed on 13 April 2023).
- Packard, E. It’s Fun, but Does It Make You Smarter? Available online: https://www.apa.org/monitor/nov07/itsfun (accessed on 5 January 2023).
- Play Gloucestershire. Play Nurture Plus Handbook; Play Gloucestershire: Gloucester, UK, 2022. [Google Scholar]
- Zosh, J.M.; Hirsh-Pasek, K.; Hopkins, E.J.; Jensen, H.; Liu, C.; Neale, D.; Solis, S.L.; Whitebread, D. Accessing the Inaccessible: Redefining Play as a Spectrum. Front. Psychol. 2018, 9, 1124. [Google Scholar] [CrossRef]
- ASLA HONOR AWARD—The Crown Sky Garden: Ann & Robert H. Lurie Children’s Hospital of Chicago. Available online: https://www.asla.org/2013awards/374.html (accessed on 10 January 2023).
- Forman, A.D. Healing by Design. N. Engl. J. Med. 1996, 334, 334–336. [Google Scholar] [CrossRef]
- Laursen, J.; Danielsen, A.; Rosenberg, J. Effects of environmental design on patient outcome: A systematic review. Health Environ. Res. Des. J. 2014, 7, 108–119. [Google Scholar] [CrossRef]
- Public Health England. Improving Access to Greenspace. A New Review for 2020; Public Health England: London, UK, 2020. [Google Scholar]
- Unmüßig, B. Monetizing Nature: Taking Precaution on a Slippery Slope. Available online: https://greattransition.org/publication/monetizing-nature-taking-precaution-on-a-slippery-slope (accessed on 14 March 2023).
- Olds, A.R. Nature as healer. Child. Environ. Q. 1989, 6, 27–32. [Google Scholar]
- Natural England. ‘Nature Nearby’ Accessible Natural Greenspace Guidance; Natural England: Peterborough, UK, 2010. [Google Scholar]
- Greater Cambridge Shared. Planning Planning Application Documents. Available online: https://applications.greatercambridgeplanning.org/online-applications/applicationDetails.do?activeTab=documents&keyVal=R08MBZDXKLB00 (accessed on 14 March 2023).
- Cordoza, M.; Ulrich, R.S.; Manulik, B.J.; Gardiner, S.K.; Fitzpatrick, P.S.; Hazen, T.M.; Mirka, A.; Perkins, R.S. Impact of Nurses Taking Daily Work Breaks in a Hospital Garden on Burnout. Am. J. Crit. Care 2018, 27, 508–512. [Google Scholar] [CrossRef]
- Grahn, P.; Pálsdóttir, A.M.; Ottosson, J.; Jonsdottir, I.H. Longer Nature-Based Rehabilitation May Contribute to a Faster Return to Work in Patients with Reactions to Severe Stress and/or Depression. Int. J. Environ. Res. Public Health 2017, 14, 1310. [Google Scholar] [CrossRef]
- Stigsdotter, U.A.; Grahn, P. Experiencing a Garden: A Healing Garden for People Suffering from Burnout Diseases. J. Ther. Hortic. 2003, 14, 38–48. [Google Scholar]
- Gerlach-Spriggs, N.; Healy, V.J. Rehabilitation and Gardens: The Legacy of Dr. Howard A. Rusk. SiteLINES J. Place 2019, 15, 15–19. [Google Scholar]
- Healthcare Design. Rusk Children’s PlayGarden for Interactive Therapeutic Play at the Rusk Institute of Rehabilitation Medicine, NYU Medical Center—New York, NY. Available online: https://healthcaredesignmagazine.com/trends/architecture/rusk-childrens-playgarden-interactive-therapeutic-play-rusk-institute-rehabilitation-medicin/ (accessed on 6 April 2023).
- St. Louis Children’s Hospital. Outdoor Gardens. Available online: https://www.stlouischildrens.org/visit-us/hospital-amenities/play-and-activities/outdoor-gardens (accessed on 6 April 2023).
- The Forest Bathing Institute Science and Research. Available online: https://tfb.institute/scientific-research/ (accessed on 5 January 2023).
- Pasha, S. Barriers to Garden Visitation in Children’s Hospitals. HERD Health Environ. Res. Des. J. 2013, 6, 76–96. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.C. The Future of Healing Gardens. HERD Health Environ. Res. Des. J. 2016, 9, 172–174. [Google Scholar] [CrossRef] [PubMed]
- Dosen, A.S.; Ostwald, M.J. Prospect and Refuge Theory: Constructing a Critical Definition for Architecture and Design. Int. J. Des. Soc. 2013, 6, 9–24. [Google Scholar] [CrossRef]
- Appleton, J. The Experience of Landscape, 1st ed.; John Wiley and Sons: London, UK; New York, NY, USA, 1975. [Google Scholar]
- Stigsdotter, U. Landscape Architecture and Health: Evidence-Based Health-Promoting Design and Planning. Ph.D. Thesis, Swedish University of Agricultural Sciences, Uppsala, Sweden, 2005. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Definition | Key Points | Reference |
|---|---|---|
| “the healing environment is based on…the body, mind and spirit working together” | Aimed to enhance people’s health and wellbeing | Tyson, 1998 [25] |
| “it is important to recognise that ‘healing’ is not synonymous with ‘cure’” instead it “facilitates stress reduction” | Focuses on stress reduction | Marcus, 2007 [5] |
| A garden should have “green vegetation, flowers and water” | Healing gardens should be reduced down to physical design aspects | Ulrich, quoted in Marcus and Barnes, 1999 [6] (p. 30) |
| “to a variety of garden features that have in common a consistent tendency to foster restoration from stress and have other positive influences on patients, visitors and staff” | There should be restoration and benefit the health and wellbeing of users | Marcus and Barnes, 1999 [6] (p. 30) |
| “a garden in a healing setting aimed to make people feel better” | Feeling better | Eckerling, 1996 [34,35] |
| “the places where horticultural therapy activities happen” | Horticulture therapy activities | Wang and Li, 2012 [34,38] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Din, S.K.-J.; Russo, A.; Liversedge, J. Designing Healing Environments: A Literature Review on the Benefits of Healing Gardens for Children in Healthcare Facilities and the Urgent Need for Policy Implementation. Land 2023, 12, 971. https://doi.org/10.3390/land12050971
Din SK-J, Russo A, Liversedge J. Designing Healing Environments: A Literature Review on the Benefits of Healing Gardens for Children in Healthcare Facilities and the Urgent Need for Policy Implementation. Land. 2023; 12(5):971. https://doi.org/10.3390/land12050971
Chicago/Turabian StyleDin, Shereen Khatoon-Jaan, Alessio Russo, and Jamie Liversedge. 2023. "Designing Healing Environments: A Literature Review on the Benefits of Healing Gardens for Children in Healthcare Facilities and the Urgent Need for Policy Implementation" Land 12, no. 5: 971. https://doi.org/10.3390/land12050971
APA StyleDin, S. K.-J., Russo, A., & Liversedge, J. (2023). Designing Healing Environments: A Literature Review on the Benefits of Healing Gardens for Children in Healthcare Facilities and the Urgent Need for Policy Implementation. Land, 12(5), 971. https://doi.org/10.3390/land12050971