
Investigation of the Upper Respiratory Tract of a Male Smoker with Laryngeal Cancer by Inhaling Air Associated with Various Physical Activity Levels





Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
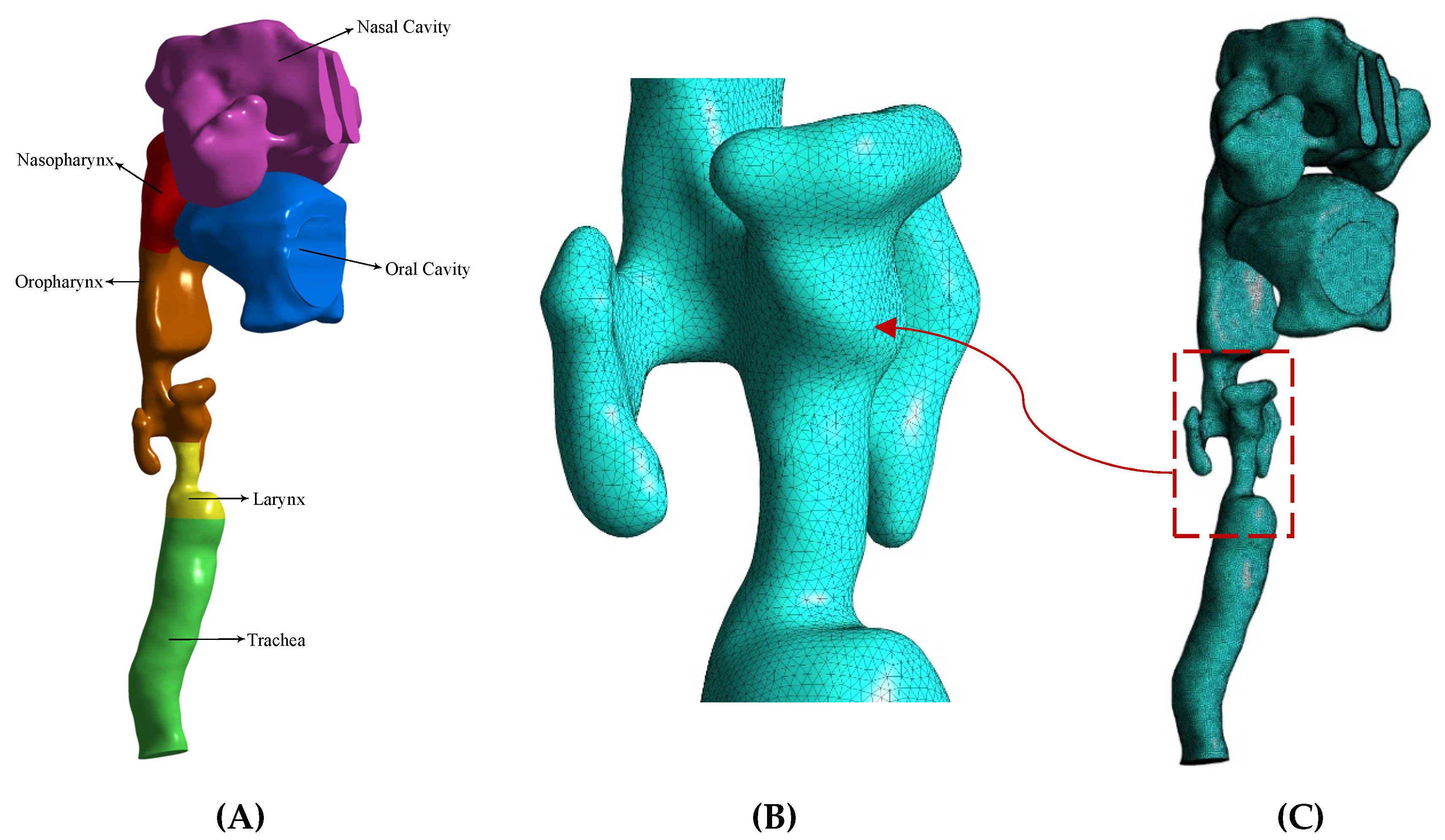
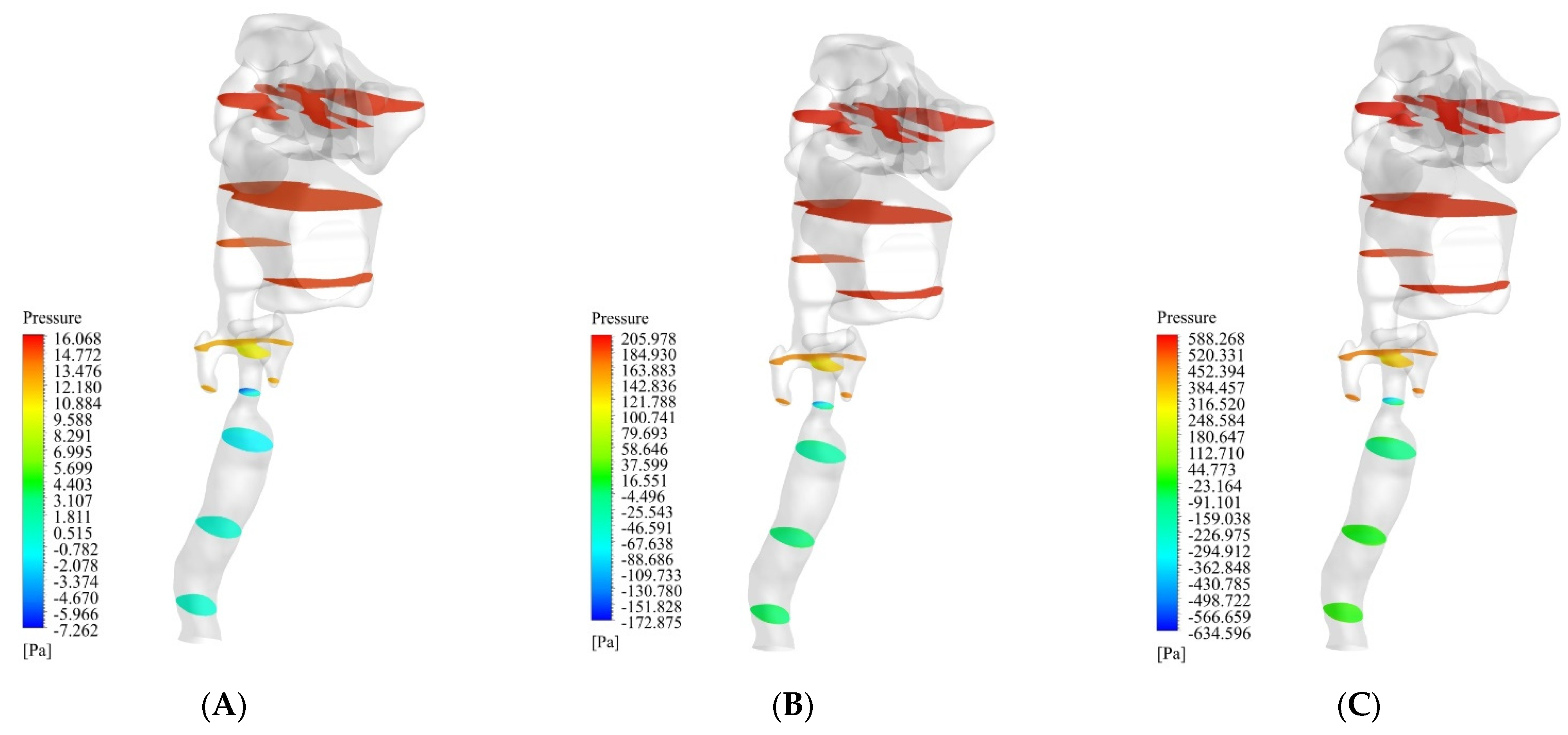
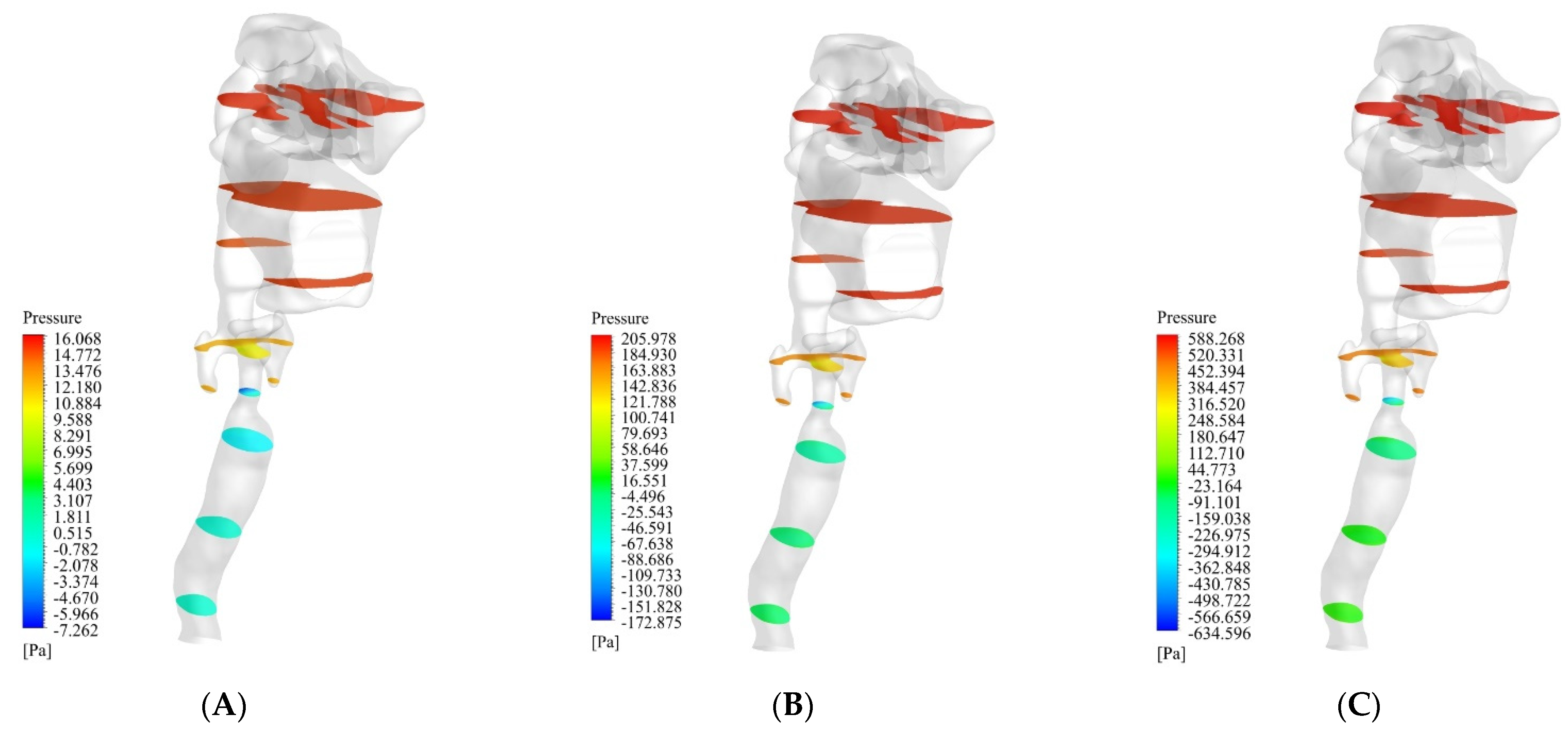
- The pressure in the nasal cavity and nasopharynx region increased sharply due to the narrowing of the airway in the larynx;
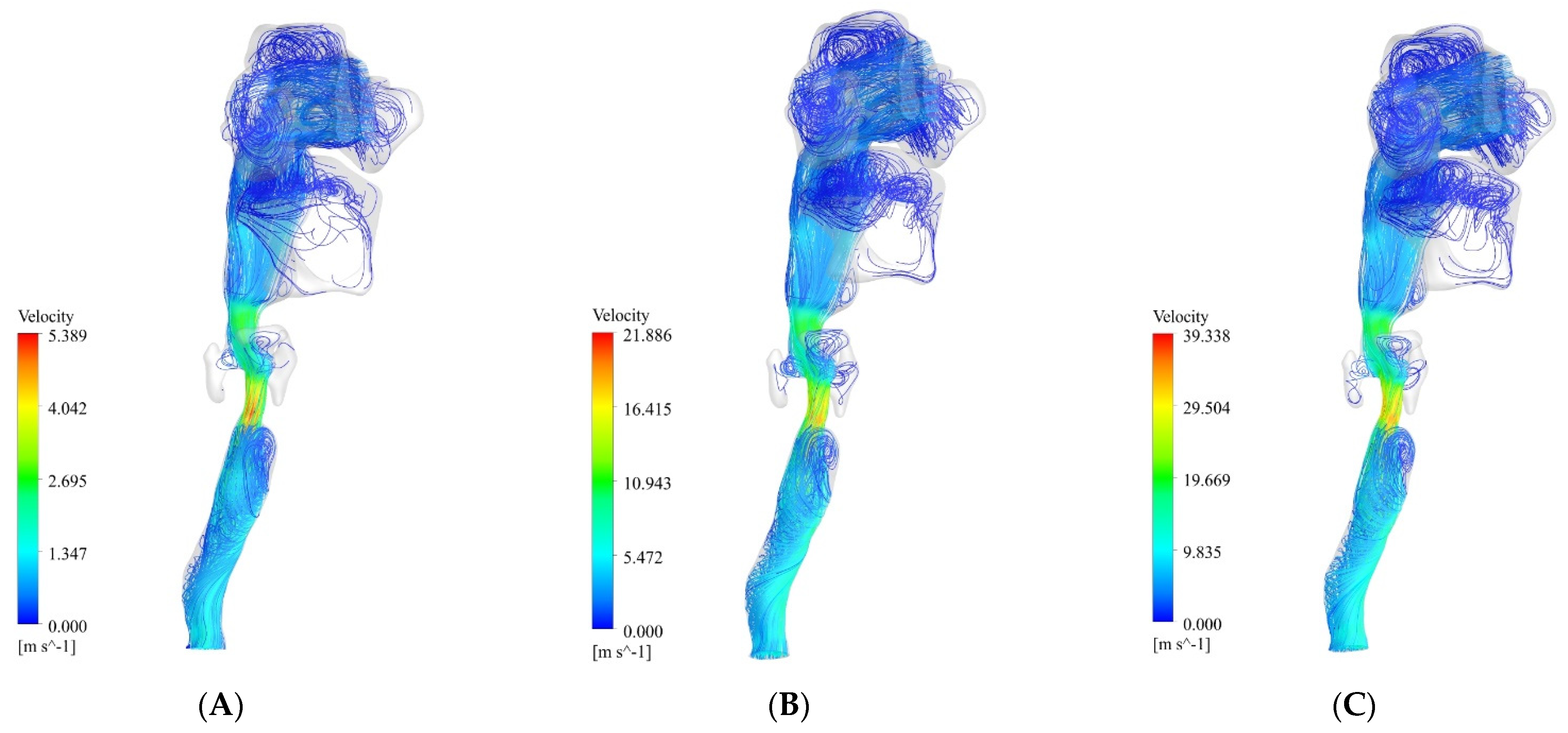
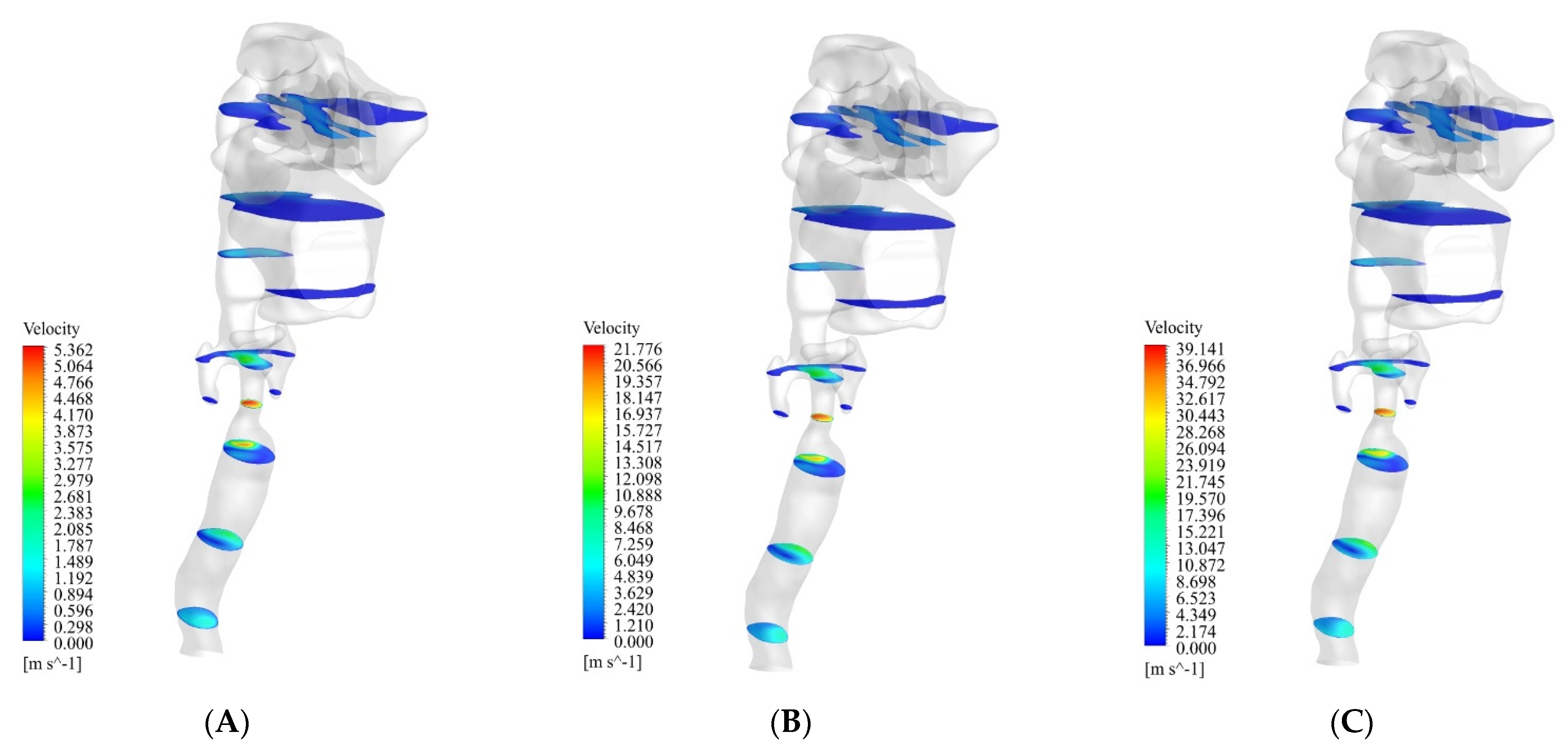
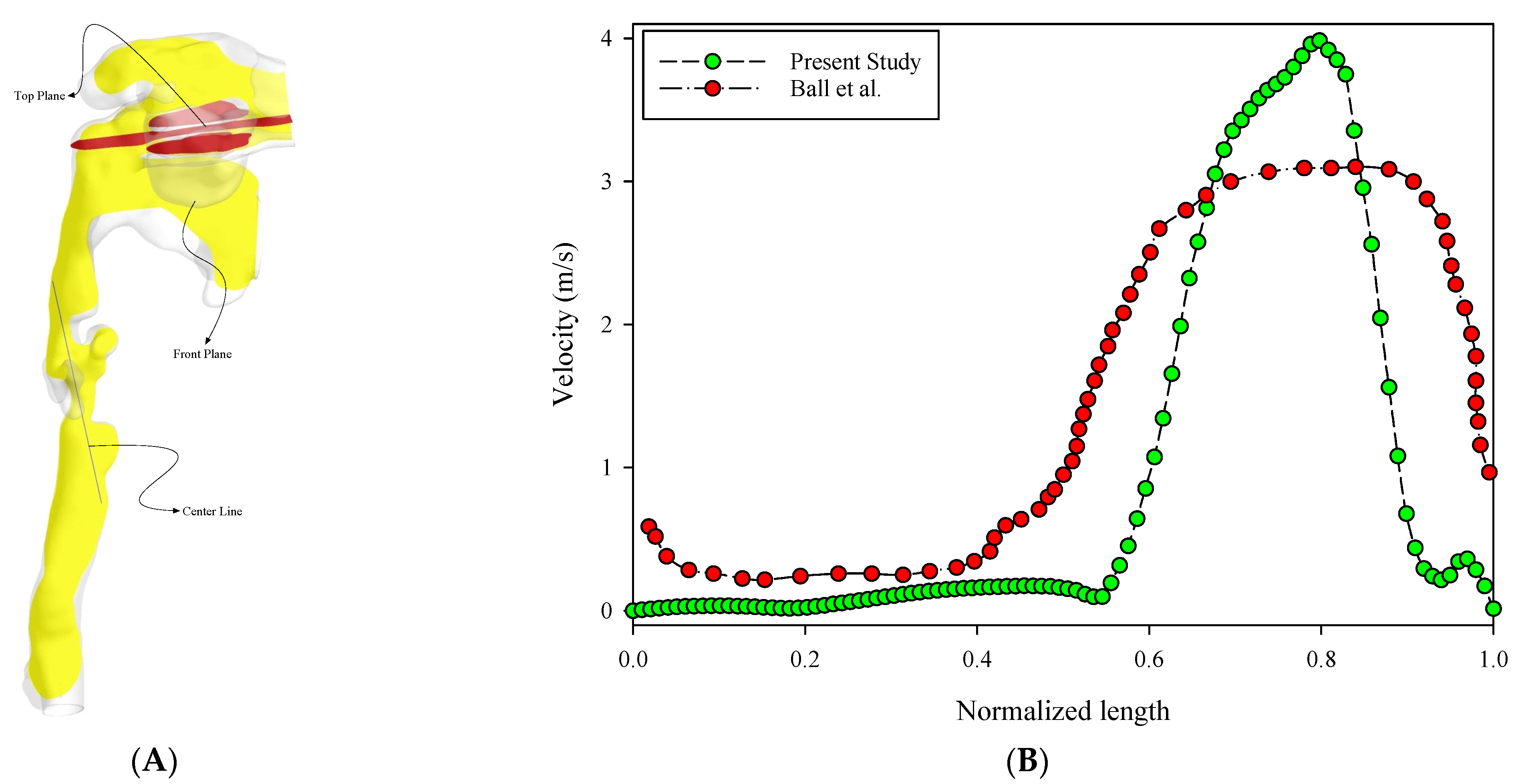
- The maximum velocity occurred in the lower part of the larynx. After this part, the oropharynx showed a significantly higher velocity than the other parts;
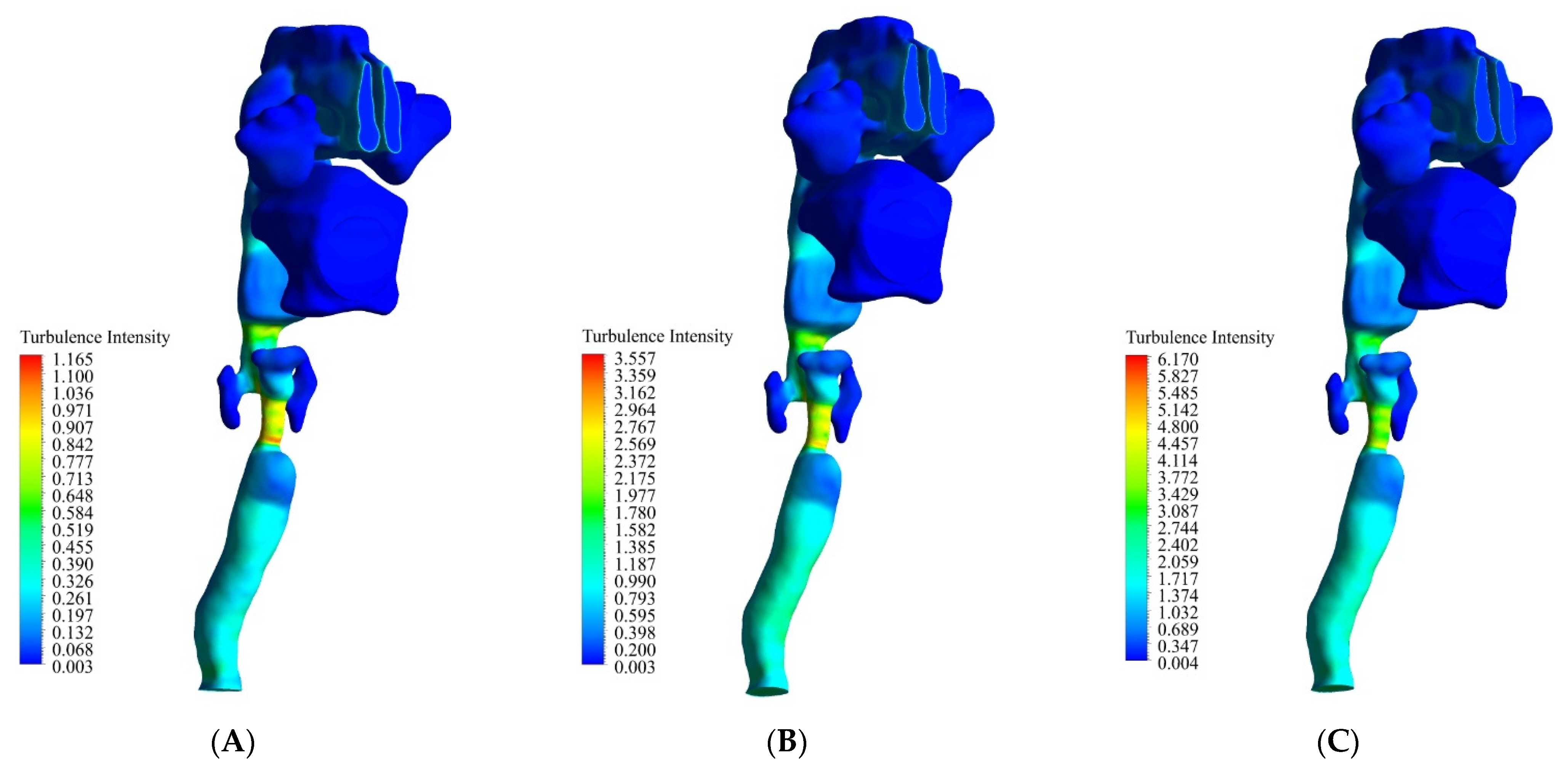
- The maximum turbulence intensity occurred in the larynx. At 13 L/min, 55 L/min, and 100 L/min, the maximum turbulence intensity was 1.1, 3.5, and 6.1, respectively;
- The maximum WSS occurred in the larynx. At 13 L/min, 55 L/min, and 100 L/min, the maximum WSS was 0.62 Pa, 5.4 Pa, and 12.4 Pa, respectively.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ball, C.G.; Uddin, M.; Pollard, A. High resolution turbulence modelling of airflow in an idealized human extra-thoracic airway. Comput. Fluids 2008, 37, 943–964. [Google Scholar] [CrossRef]
- Heenan, A.F.; Matida, E.; Pollard, A.; Finlay, W.H. Experimental measurements and computational modeling of the flow field in an idealized extra-thoracic airway. Exp. Fluids 2003, 35, 70–84. [Google Scholar] [CrossRef]
- Kleinstreuer, C.; Zhang, Z. Laminar-to-turbulent fluidparticle flows in a human airway model. Int. J. Multiph. Flow 2003, 29, 271–289. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinstreuer, C.; Donohue, J.; Kim, C. Comparison of micro-and nano-size particle depositions in a human upper airway model. J. Aerosol Sci. 2005, 36, 211–233. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinsteuer, C. Species heat and mass transfer in a human upper airway model. Int. J. Heat Mass Transfer 2003, 45, 55–68. [Google Scholar] [CrossRef]
- Matida, E.; Finlay, W.; Lange, C.; Grgic, B. Improved numerical simulation of aerosol deposition in an idealized mouth–throat. J. Aerosol Sci. 2004, 35, 1–19. [Google Scholar] [CrossRef]
- Stapleton, K.W.; Guentsch, E.; Hoskinson, M.K.; Finlay, W.H. The suitability of k–turbulence modeling for aerosol deposition in the mouth and throat: Acomparison with experiment. J. Aerosol Sci. 2000, 31, 739–749. [Google Scholar] [CrossRef]
- Taylan, M.; Can, O.; Cetincakmak, M.G.; Ozbay, M. Effect of Airway Dynamics on the Development of Larynx Cancer. Laryngoscope 2016, 126, 1136–1142. [Google Scholar] [CrossRef]
- Kaushik, V.; Ghosh, S.; Das, G.; Das, P.K. CFD simulation of core annular flow through sudden contraction and expansion. J. Pet. Sci. Eng. 2012, 86, 153–164. [Google Scholar] [CrossRef]
- Lin, C.L.; Tawhai, M.H.; McLennan, G.; Hoffman, E.A. Characteristics of the turbulent laryngeal jet and its effect on airflow in the human intra-thoracic airways. Respir. Physiol. Neurobiol. 2007, 157, 295–309. [Google Scholar] [CrossRef] [Green Version]
- Kumar, H.; Spence, C.J.; Tawhai, M.H. Modeling of pharyngeal pressure dur-ing adult nasal high flow therapy. Respir. Physiol. Neurobiol. 2015, 219, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Carrigy, N.B.; Carey, J.P.; Martin, A.R. Simulation of muscle and adipose tissue deformation in the passive human pharynx. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Hiramatsu, H.; Tokashiki, R.; Suzuki, M. Usefulness of three-dimensional computed tomography of the larynx for evaluation of unilateral vocal fold paralysis before and after treatment: Technique and clinical applications. Eur. Arch. Otorhinolaryngol. 2008, 265, 725–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vampola, T.; Horáček, J.; Klepáček, I. Computer simulation of mucosal waves on vibrating human vocal folds. Biocybern. Biomed. Eng. 2016, 36, 451–465. [Google Scholar] [CrossRef]
- Chen, T.; Chodara, A.M.; Sprecher, A.J.; Fang, F.; Song, W.; Tao, C.H. A new method of reconstructing the human laryngeal architecture using micro-MRI. J. Voice 2012, 26, 55–62. [Google Scholar] [CrossRef]
- Zheng, X.; Mittal, R.; Xue, Q.; Bielamowicz, S. Directnumerical simulation of the glottal jet and vocal-fold dynamics in athree-dimensional laryngeal model. J. Acoust. Soc. Am. 2011, 130, 404–415. [Google Scholar] [CrossRef] [Green Version]
- Švec, J.G.; Schutte, H.K. Kymographic imaging of laryngeal vibrations. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 458–465. [Google Scholar] [CrossRef]
- Zhang, Z.; Neubauer, J.; Berry, D.A. Aerodynamically and acoustically driven modes of vibration in a physical model of the vocal folds. J. Acoust. Soc. Am. 2006, 120, 2841–2849. [Google Scholar] [CrossRef]
- Murray, P.R.; Thomson, S.L. Vibratory responses of synthetic, self-oscillating vocal fold models. J. Acoust. Soc. Am. 2012, 132, 3428–3438. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Wang, X.; Krane, M.; Zhang, L.T. FullyCoupled Aeroelastic Simulation with Fluid Compressibility-for Application to Vocal Fold Vibration. Comput. Methods Appl. Mech. Eng. 2016, 315, 584–606. [Google Scholar] [CrossRef] [Green Version]
- Gemci, T.; Ponyavin, V.; Chen, Y.; Chen, H. Collins Computational model of airflow in upper 17 generations of human respiratory tract. J. Biomech. 2008, 41, 2047–2054. [Google Scholar] [CrossRef] [PubMed]
- Pollard, A.; Secretain, F.; Milne, B. Air and blood fluid dynamics: At the interface between engineering and medicine. J. Phys. Conf. Ser. 2014, 530, 012005. [Google Scholar] [CrossRef] [Green Version]
- U.S. EPA. Exposure Factors Handbook 2011 Edition (Final Report); EPA/600/R-09/052F; U.S. Environmental Protection Agency: Washington, DC, USA, 2011.
- Beni, H.M.; Mortazavi, H.; Aghaei, F.; Kamalipour, S. Experimental tracking and numerical mapping of novel coronavirus micro-droplet deposition through nasal inhalation in the human respiratory system. Biomech. Model. Mechanobiol. 2021, 20, 1087–1100. [Google Scholar] [CrossRef] [PubMed]
- Hamed, M.; Beni, H.M.; Aghaei, F.; Sajadian, H. SARS-CoV-2 droplet deposition path and its effects on the human upperairway in the oral inhalation. Comput. Methods Programs Biomed. 2020, 200, 105843. [Google Scholar]
- Alaodolehei, K.B.; Jafarian, A.; Sheikhani, H.; Beni, H.M. Performance enhancement of an achalasia automatic detection system using ensemble empirical mode decomposition denoising method. J. Med. Biol. Eng. 2020, 40, 179–188. [Google Scholar] [CrossRef]
- Beni, H.M.; Mortazavi, H. Mathematical modeling of the solar regenerative heat exchanger under turbulent oscillating flow: Applications of renewable and sustainable energy and artificial heart. Results Eng. 2022, 13, 100321. [Google Scholar] [CrossRef]
- Mortazavi, H.; Beni, H.M.; Islam, M.S. Thermal/fluid characteristics of the inline stacked plain-weave screen as solar-powered Stirling engine heat regenerators. IET Renew. Power Gener. 2022, 16, 956–965. [Google Scholar] [CrossRef]
- Mortazavi, H.; Beni, H.M.; Islam, M.S. Front Cover: Thermal/fluid characteristics of the inline stacked plain-weave screen as solar-powered Stirling engine heat regenerators. IET Renew. Power Gener. 2022, 16, i. [Google Scholar] [CrossRef]
- Mortazavi, H.; Beni, H.M.; Islam, M. S Biomedical and Biophysical Limits to Mathematical Modeling of Pulmonary System Mechanics: A Scoping Review on Aerosol and Drug Delivery. Biomech. Model. Mechanobiol. 2021, 21, 79–87. [Google Scholar]
- Islam, M.S.; Larpruenrudee, P.; Saha, S.C.; Pourmehran, O.; Paul, A.R.; Gemci, T.; Collins, R.; Paul, G.; Gu, Y. How severe acute respiratory syndrome coronavirus-2 aerosol propagates through the age-specific upper airways. J Phys. Fluids 2021, 33, 081911. [Google Scholar] [CrossRef]
- Islam, M.; Larpruenrudee, P.; Hossain, S.; Rahimi-Gorji, M.; Gu, Y.; Saha, S.; Paul, G. Polydisperse Aerosol Transport and Deposition in Upper Airways of Age-Specific Lung. J. Int. J. Environ. Res. Public Health 2021, 18, 6239. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Larpruenrudee, P.; Paul, A.R.; Paul, G.; Gemci, T.; Gu, Y.; Saha, S.C. SARS CoV-2 aerosol: How far it can travel to the lower airways? J. Phys. Fluids 2021, 33, 061903. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Saha, S.C.; Sauret, E.; Ong, H.; Young, P.; Gu, Y. Application, Euler–Lagrange approach to investigate respiratory anatomical shape effects on aerosol particle transport and deposition. J. Toxicol. Res. 2019, 3, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Gu, Q.; Qi, S.; Yue, Y.; Shen, J.; Zhang, B.; Sun, W.; Qian, W.; Islam, M.S.; Saha, S.C.; Wu, J. Structural and functional alterations of the tracheobronchial tree after left upper pulmonary lobectomy for lung cancer. BioMed. Eng. Online 2019, 18, 105. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, A.; Islam, M.S.; Saha, S.C. Targeted drug delivery of magnetic nano-particle in the specific lung region. J. Comput. 2020, 8, 10. [Google Scholar] [CrossRef] [Green Version]
- Hendryx, M.; Islam, M.S.; Dong, G.-H.; Paul, G.; Health, P. Air Pollution Emissions 2008–2018 from Australian Coal Mining: Implications for Public and Occupational Health. J. Int. J. Environ. Res. 2020, 17, 1570. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Raghav, V.; Padhmashali, V.; Paul, G.; Islam, M.S.; Saha, S.C. Airflow and Particle Transport Prediction through Stenosis Airways. Int. J. Environ. Res. Public Health 2020, 17, 1119. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Saha, S.C.; Sauret, E.; Gu, Y.; Ristovski, Z. Numerical investigation of aerosol particle transport and deposition in realistic lung airway. In Proceedings of the International Conference on Computational Methods, Auckland, New Zealand, 14–17 July 2015; Scientech Publisher LLC: Berkeley, CA, USA, 2015. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grid Parameters | Average Velocity (m/s) | ||||
|---|---|---|---|---|---|
| Element Size (m) | Nodes | Elements | Top Plane | Front Plane | Center Line |
| 0.004 | 51,652 | 197,214 | 0.21077 | 0.90562 | 2.40075 |
| 0.003 | 62,219 | 243,683 | 0.21978 | 0.85532 | 2.58929 |
| 0.002 | 225,436 | 659,933 | 0.21905 | 0.74990 | 2.72969 |
| 0.001 | 1,111,962 | 3,502,459 | 0.19995 | 0.68605 | 2.79816 |
| 0.0009 | 1,416,506 | 4,557,811 | 0.20061 | 0.68600 | 2.79471 |
| 0.0007 | 2,672,912 | 8,853,902 | 0.20332 | 0.65686 | 2.80306 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mortazavy Beni, H.; Mortazavi, H.; Tashvighi, E.; Islam, M.S. Investigation of the Upper Respiratory Tract of a Male Smoker with Laryngeal Cancer by Inhaling Air Associated with Various Physical Activity Levels. Atmosphere 2022, 13, 717. https://doi.org/10.3390/atmos13050717
Mortazavy Beni H, Mortazavi H, Tashvighi E, Islam MS. Investigation of the Upper Respiratory Tract of a Male Smoker with Laryngeal Cancer by Inhaling Air Associated with Various Physical Activity Levels. Atmosphere. 2022; 13(5):717. https://doi.org/10.3390/atmos13050717
Chicago/Turabian StyleMortazavy Beni, Hamidreza, Hamed Mortazavi, Ebrahim Tashvighi, and Mohammad S. Islam. 2022. "Investigation of the Upper Respiratory Tract of a Male Smoker with Laryngeal Cancer by Inhaling Air Associated with Various Physical Activity Levels" Atmosphere 13, no. 5: 717. https://doi.org/10.3390/atmos13050717
APA StyleMortazavy Beni, H., Mortazavi, H., Tashvighi, E., & Islam, M. S. (2022). Investigation of the Upper Respiratory Tract of a Male Smoker with Laryngeal Cancer by Inhaling Air Associated with Various Physical Activity Levels. Atmosphere, 13(5), 717. https://doi.org/10.3390/atmos13050717