
Relationship between Wildfire Smoke and Children’s Respiratory Health in the Metropolitan Cities of Central-Chile


 ,
,
Abstract
:1. Introduction
1.1. Wildfires in Chile
1.2. Study Objective
2. Methods
2.1. Study Area
2.2. Study Design and Data
2.3. Statistical Analyses
- -
- The parameter “ “ is the outcome (dependent) variable and corresponds to the monthly number of Health Emergency at time “t” on the period 2010–2013;
- -
- “PM10” is the ambient PM10 concentration in micrograms per cubic meters;
- -
- “Fires” is the monthly number of fires in the studied area;
- -
- “Temp” and Precip” are the ambient temperature (°C) and precipitations (mm/hours), respectively;
- -
- f(t;λ) is a smoothing function;
- -
- “Popt” is the population density;
- -
- “β’s” are the calculated regression parameters, used to estimate Relative Risks.
3. Results
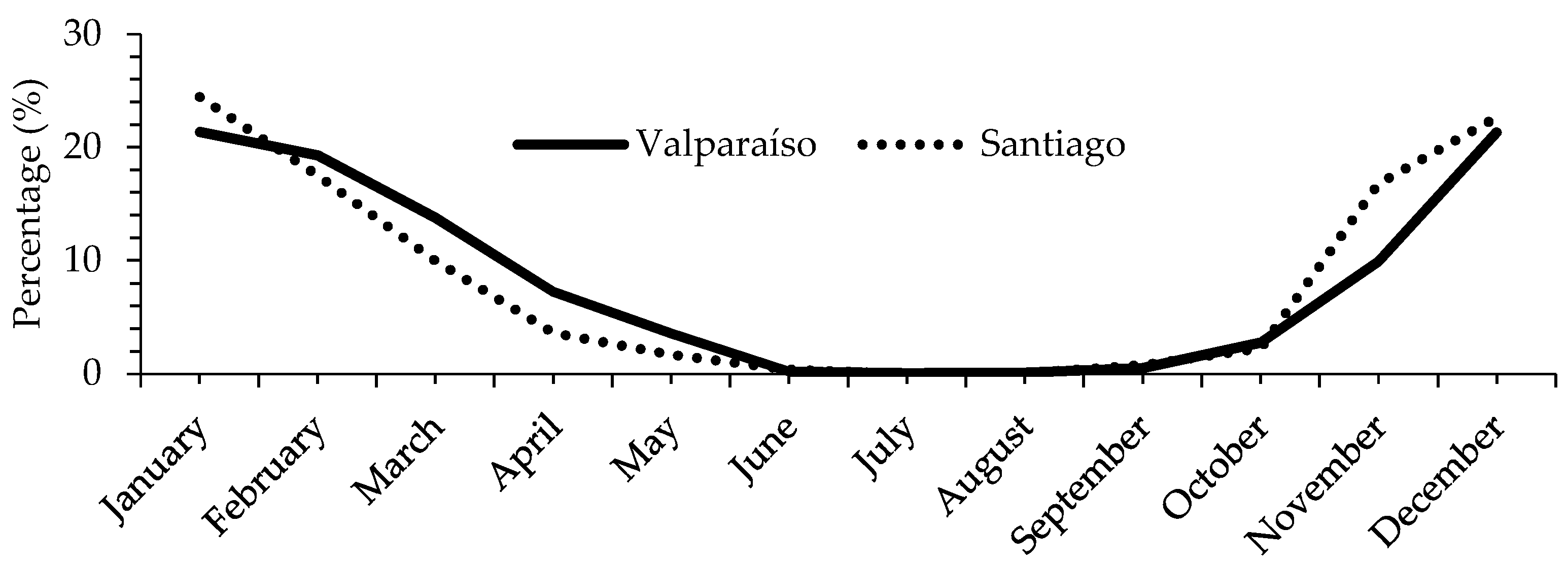
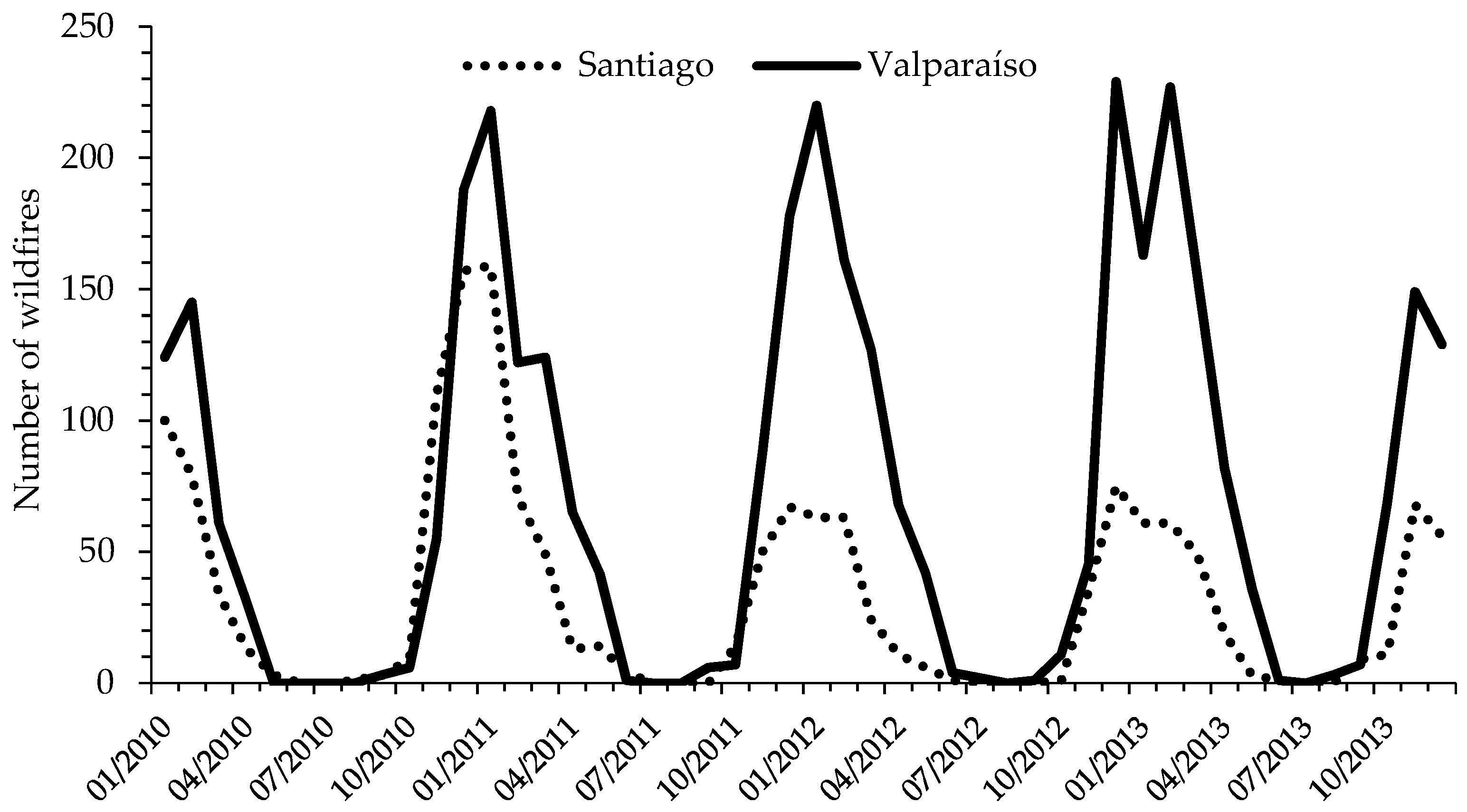
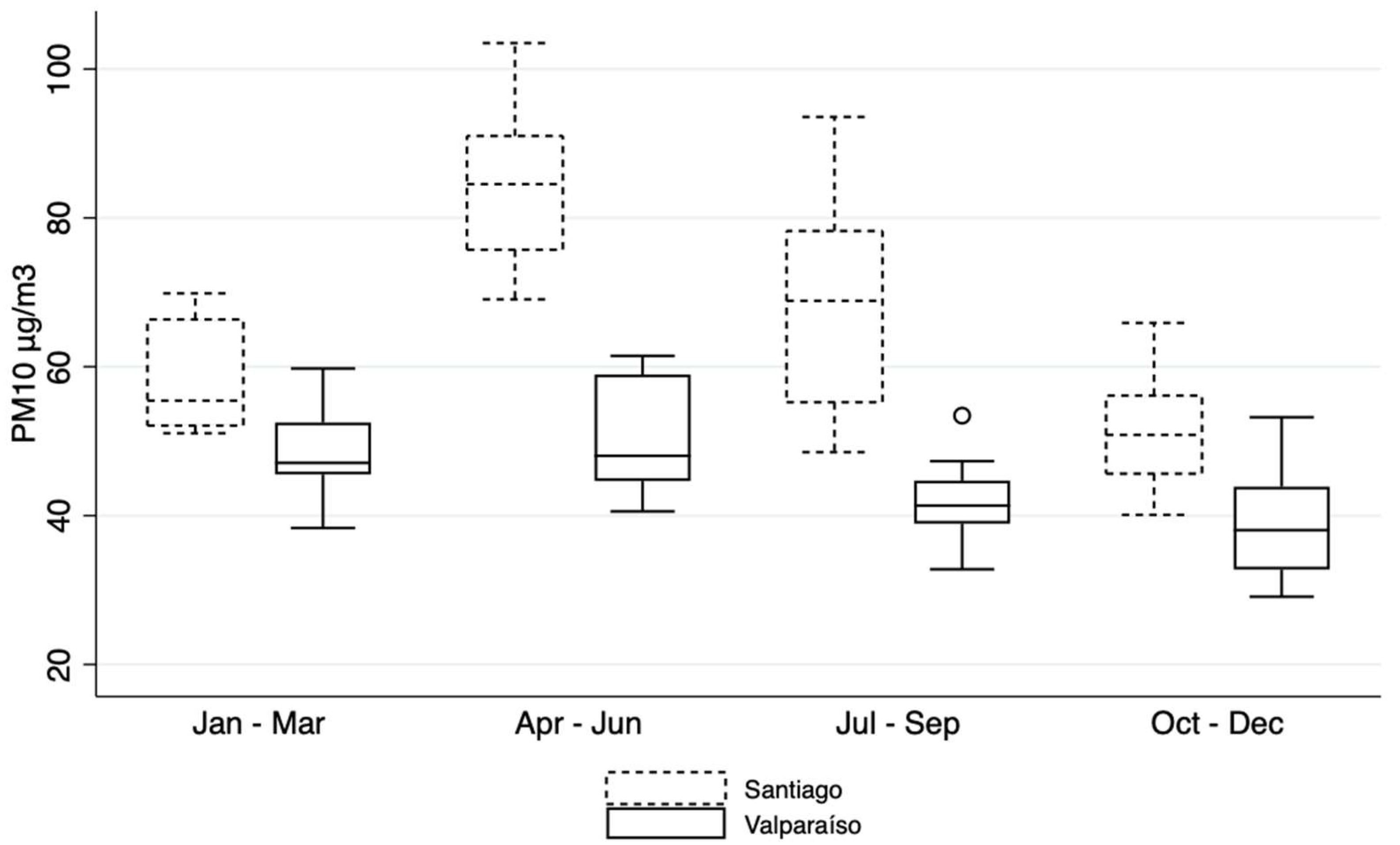
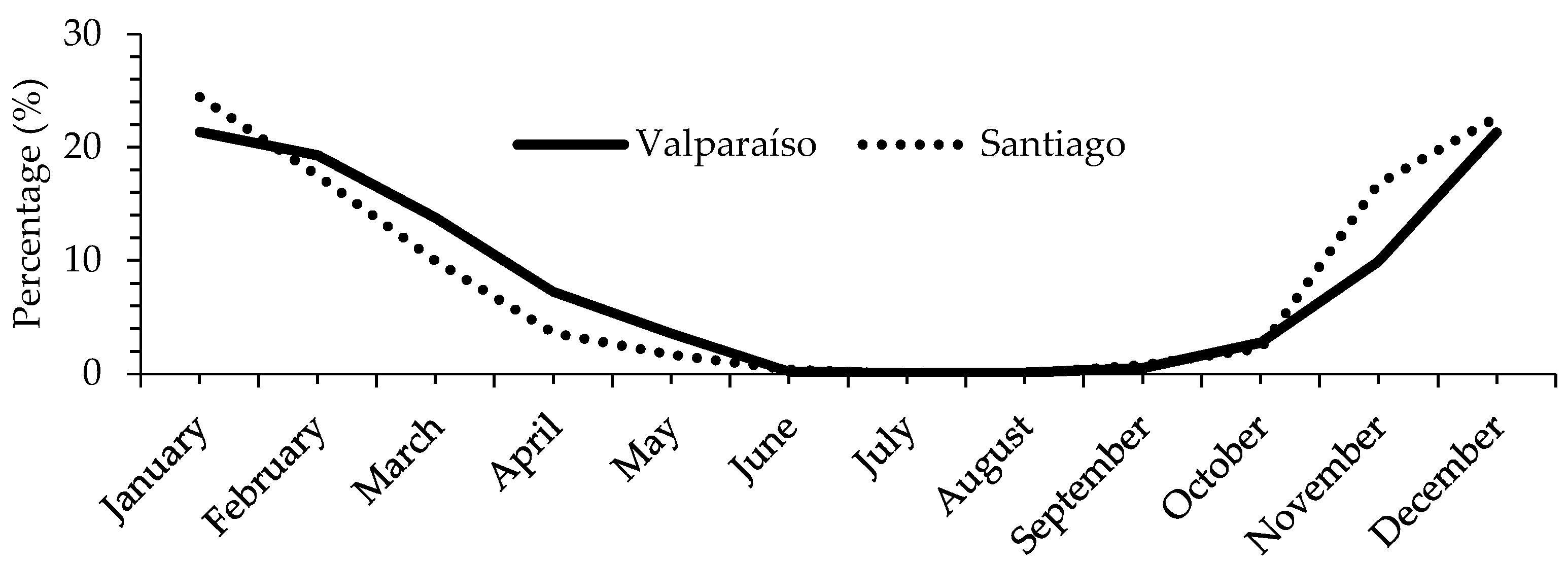
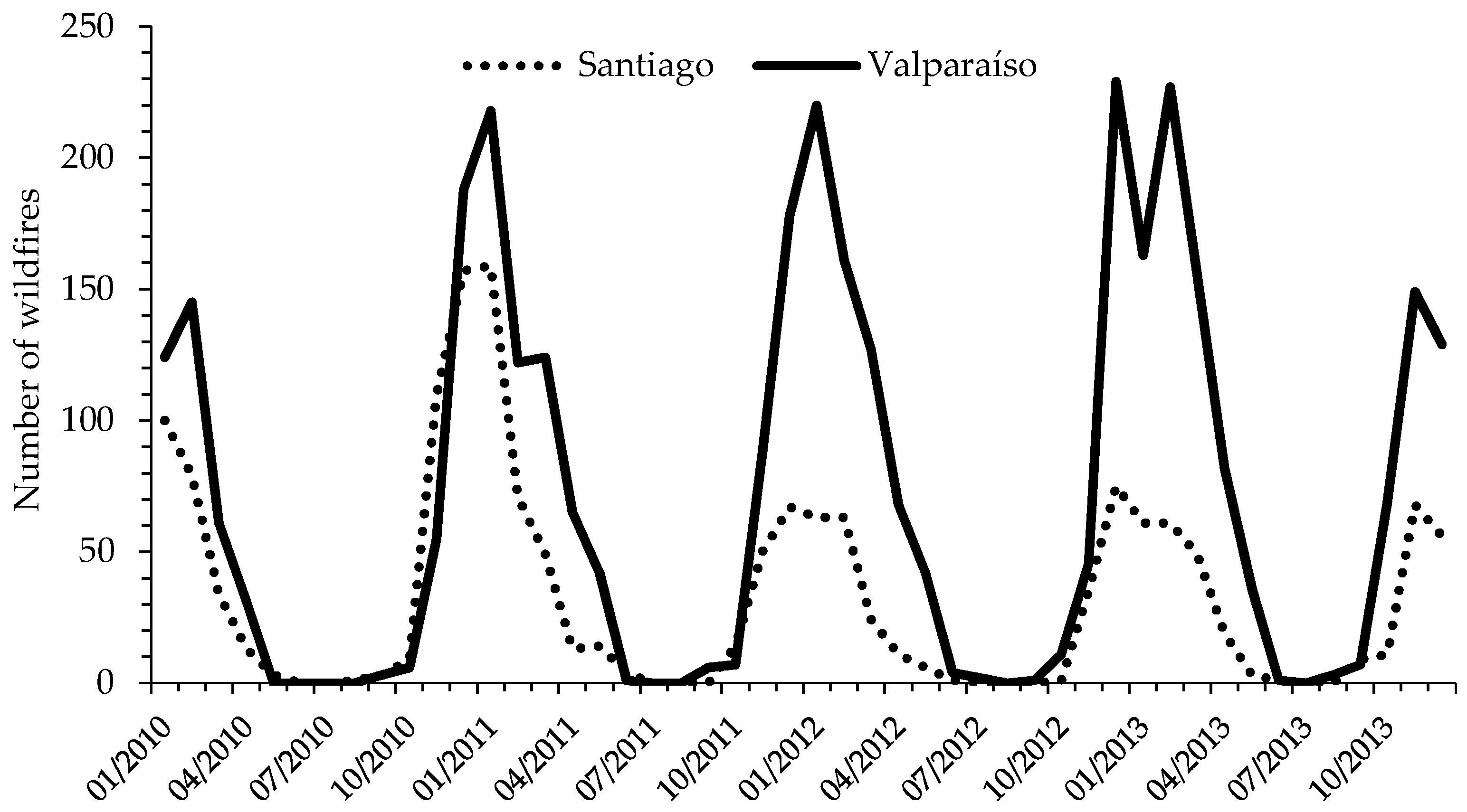
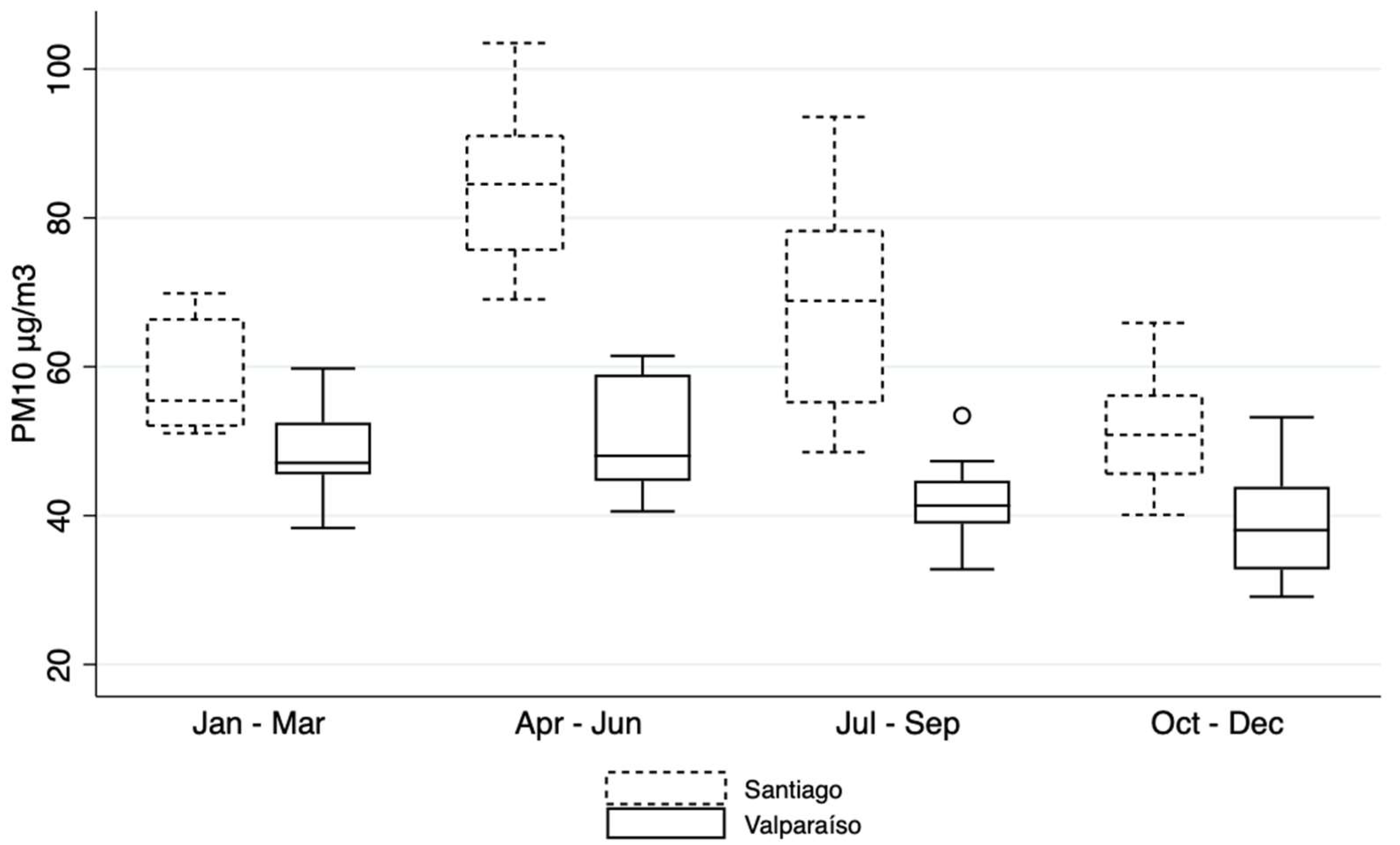
3.1. Ambient Parameters and Wildfires Trend for Santiago and Valparaiso Regions
3.2. Risk Estimation of Respiratory Illness
4. Discussion
4.1. Strengths and Limitations of Our Study
4.2. Wildfires and Climate Change
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Resnick, A.; Woods, B.; Krapfl, H.; Toth, B. Health outcomes associated with smoke exposure in Albuquerque, New Mexico, during the 2011 Wallow fire. J. Public Health Manag. Pract. JPHMP 2015, 21 (Suppl. 2), S55–S61. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.C.; Mickley, L.J.; Sulprizio, M.P.; Dominici, F.; Yue, X.; Ebisu, K.; Anderson, G.B.; Khan, R.F.A.; Bravo, M.A.; Bell, M.L. Particulate Air Pollution from Wildfires in the Western US under Climate Change. Clim. Chang. 2016, 138, 655–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldizen, F.C.; Sly, P.D.; Knibbs, L.D. Respiratory effects of air pollution on children. Pediatr. Pulmonol. 2016, 51, 94–108. [Google Scholar] [CrossRef]
- Nirel, R.; Maimon, N.; Fireman, E.; Agami, S.; Eyal, A.; Peretz, A. Respiratory hospitalizations of children living near a hazardous industrial site adjusted for prevalent dust: A case-control study. Int. J. Hyg. Environ. Health 2015, 218, 273–279. [Google Scholar] [CrossRef]
- Caamano-Isorna, F.; Figueiras, A.; Sastre, I.; Montes-Martinez, A.; Taracido, M.; Pineiro-Lamas, M. Respiratory and mental health effects of wildfires: An ecological study in Galician municipalities (north-west Spain). Environ. Health A Glob. Access Sci. Source 2011, 10, 48. [Google Scholar] [CrossRef] [Green Version]
- Reid, C.E.; Brauer, M.; Johnston, F.H.; Jerrett, M.; Balmes, J.R.; Elliott, C.T. Critical Review of Health Impacts of Wildfire Smoke Exposure. Environ. Health Perspect. 2016, 124, 1334–1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaidyanathan, A.; Yip, F.; Garbe, P. Developing an online tool for identifying at-risk populations to wildfire smoke hazards. Sci. Total Environ. 2018, 619-620, 376–383. [Google Scholar] [CrossRef]
- Alman, B.L.; Pfister, G.; Hao, H.; Stowell, J.; Hu, X.; Liu, Y.; Strickland, M.J. The association of wildfire smoke with respiratory and cardiovascular emergency department visits in Colorado in 2012: A case crossover study. Environ. Health A Glob. Access Sci. Source 2016, 15, 64. [Google Scholar] [CrossRef] [Green Version]
- Jayachandran, S. Air quality and early-life mortality evidence from Indonesia’s wildfires. J. Hum. Resour. 2009, 44, 916–954. [Google Scholar] [CrossRef] [Green Version]
- Johnston, F.H.; Purdie, S.; Jalaludin, B.; Martin, K.L.; Henderson, S.B.; Morgan, G.G. Air pollution events from forest fires and emergency department attendances in Sydney, Australia 1996-2007: A case-crossover analysis. Environ. Health A Glob. Access Sci. Source 2014, 13, 105. [Google Scholar] [CrossRef] [Green Version]
- Reid, C.E.; Jerrett, M.; Tager, I.B.; Petersen, M.L.; Mann, J.K.; Balmes, J.R. Differential respiratory health effects from the 2008 northern California wildfires: A spatiotemporal approach. Environ. Res. 2016, 150, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Wettstein, Z.S.; Hoshiko, S.; Fahimi, J.; Harrison, R.J.; Cascio, W.E.; Rappold, A.G. Cardiovascular and Cerebrovascular Emergency Department Visits Associated With Wildfire Smoke Exposure in California in 2015. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, C.; Tesfaigzi, Y.; Bassein, J.A.; Miller, L.A. Wildfire smoke exposure and human health: Significant gaps in research for a growing public health issue. Environ. Toxicol. Pharmacol. 2017, 55, 186–195. [Google Scholar] [CrossRef]
- Cuchiara, G.C.; Rappenglück, B.; Rubio, M.A.; Lissi, E.; Gramsch, E.; Garreaud, R.D. Modeling study of biomass burning plumes and their impact on urban air quality; a case study of Santiago de Chile. Atmos. Environ. 2017, 166, 79–91. [Google Scholar] [CrossRef]
- Rubio, M.A.; Lissi, E.; Jorquera, H.; Salinas, E.; Castro, J.; Cadiz, M. Carbon monoxide concentrations in Santiago City at street levels and their vertical gradient. Environ. Monit. Assess. 2008, 140, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Úbeda, X.; Sarricolea, P. Wildfires in Chile: A review. Glob. Planet. Chang. 2016, 146, 152–161. [Google Scholar] [CrossRef]
- de la Barrera, F.; Barraza, F.; Favier, P.; Ruiz, V.; Quense, J. Megafires in Chile 2017: Monitoring multiscale environmental impacts of burned ecosystems. Sci. Total Environ. 2018, 637–638, 1526–1536. [Google Scholar] [CrossRef] [PubMed]
- Gómez-González, S.; González, M.E.; Paula, S.; Díaz-Hormazábal, I.; Lara, A.; Delgado-Baquerizo, M. Temperature and agriculture are largely associated with fire activity in Central Chile across different temporal periods. For. Ecol. Manag. 2019, 433, 535–543. [Google Scholar] [CrossRef]
- Bowman, D.; Moreira-Munoz, A.; Kolden, C.A.; Chavez, R.O.; Munoz, A.A.; Salinas, F.; Gonzalez-Reyes, A.; Rocco, R.; de la Barrera, F.; Williamson, G.J.; et al. Human-environmental drivers and impacts of the globally extreme 2017 Chilean fires. Ambio 2019, 48, 350–362. [Google Scholar] [CrossRef]
- Heilmayr, R.; Echeverria, C.; Fuentes, R.; Lambin, E.F. A plantation-dominated forest transition in Chile. Appl. Geogr. 2016, 75, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Kousky, C. Impacts of natural disasters on children. Future Child. 2016, 26, 73–92. [Google Scholar] [CrossRef]
- INE. Productos Estadísticos, Demográficas y Vitales; INE: Santiago, Chile, 2019. [Google Scholar]
- Montoya-Tangarife, C.; de la Barrera, F.; Salazar, A.; Inostroza, L. Monitoring the effects of land cover change on the supply of ecosystem services in an urban region: A study of Santiago-Valparaiso, Chile. PLoS ONE 2017, 12, e0188117. [Google Scholar] [CrossRef] [PubMed]
- Garreaud, R.D.; Vuille, M.; Compagnucci, R.; Marengo, J. Present-day south american climate. Palaeogeogr. Palaeoclimatol. Palaeoecol. 2009, 281, 180–195. [Google Scholar] [CrossRef]
- Boisier, J.P.; Rondanelli, R.; Garreaud, R.D.; Muñoz, F. Anthropogenic and natural contributions to the Southeast Pacific precipitation decline and recent megadrought in central Chile. Geophys. Res. Lett. 2016, 43, 413–421. [Google Scholar] [CrossRef] [Green Version]
- (CR)2 Center for Climate and Resilience Research. Report to the Nation. The 2010–2015 Mega-Drought: A Lesson for the Future. November 2015. Available online: https://www.cr2.cl/eng/wp-content/uploads/2020/07/Mega-drought-Report.pdf (accessed on 30 July 2019).
- Muñoz, R.C.; Undurraga, A.A. Daytime mixed layer over the Santiago Basin: Description of two years of observations with a lidar ceilometer. J. Appl. Meteorol. Climatol. 2010, 49, 1728–1741. [Google Scholar] [CrossRef]
- Barraza, F.; Jorquera, H.; Heyer, J.; Palma, W.; Edwards, A.M.; Munoz, M.; Valdivia, G.; Montoya, L.D. Short-term dynamics of indoor and outdoor endotoxin exposure: Case of Santiago, Chile, 2012. Environ. Int. 2016, 92–93, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, S.; Dales, R.E.; Gultekin, T.; Vidal, C.B.; Farnendaz, M.; Rubio, M.A.; Oyola, P. Components of particulate air pollution and emergency department visits in Chile. Arch. Environ. Occup. Health 2009, 64, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, S.; Dales, R.E.; Vidal, C.B. Air pollution and mortality in Chile: Susceptibility among the elderly. Environ. Health Perspect. 2007, 115, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Dales, R.E.; Cakmak, S.; Vidal, C.B.; Rubio, M.A. Air pollution and hospitalization for acute complications of diabetes in Chile. Environ. Int. 2012, 46, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dales, R.E.; Cakmak, S.; Vidal, C.B. Air pollution and hospitalization for venous thromboembolic disease in Chile. J. Thromb. Haemost. JTH 2010, 8, 669–674. [Google Scholar] [CrossRef]
- Díaz-Robles, L.; Cortés, S.; Vergara-Fernández, A.; Ortega, J.C. Short term health effects of particulate matter: A comparison between wood smoke and multi-source polluted urban areas in Chile. Aerosol Air Qual. Res 2015, 15, 306–318. [Google Scholar] [CrossRef] [Green Version]
- Pino, P.; Walter, T.; Oyarzun, M.; Villegas, R.; Romieu, I. Fine particulate matter and wheezing illnesses in the first year of life. Epidemiol. Camb. Mass. 2004, 15, 702–708. [Google Scholar] [CrossRef] [PubMed]
- CONAF. Resumen Nacional de Ocurrencia Por Provincias y Comunas; CONAF: Santiago, Chile, 2019. [Google Scholar]
- Wood, S.N. Stable and efficient multiple smoothing parameter estimation for generalized additive models. J. Am. Stat. Association. 2004, 99, 673–686. [Google Scholar] [CrossRef] [Green Version]
- Rutllant, J.; Garreaud, R. Episodes of Strong Flow down the Western Slope of the Subtropical Andes. Mon. Weather Rev. 2004, 132, 611–622. [Google Scholar] [CrossRef] [Green Version]
- Delfino, R.J.; Brummel, S.; Wu, J.; Stern, H.; Ostro, B.; Lipsett, M.; Winer, A.; Street, D.H.; Zhang, L.; Tjoa, T.; et al. The relationship of respiratory and cardiovascular hospital admissions to the southern California wildfires of 2003. Occup. Environ. Med. 2009, 66, 189–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunzli, N.; Avol, E.; Wu, J.; Gauderman, W.J.; Rappaport, E.; Millstein, J.; Bennion, J.; McConnell, R.; Gilliland, F.D.; Berhane, K.; et al. Health effects of the 2003 Southern California wildfires on children. Am. J. Respir. Crit. Care Med. 2006, 174, 1221–1228. [Google Scholar] [CrossRef] [Green Version]
- Black, C.; Gerriets, J.E.; Fontaine, J.H.; Harper, R.W.; Kenyon, N.J.; Tablin, F.; Schelegle, E.S.; Miller, L.A. Early Life Wildfire Smoke Exposure Is Associated with Immune Dysregulation and Lung Function Decrements in Adolescence. Am. J. Respir. Cell Mol. Biol. 2017, 56, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.R.G.; Agyapong, V.; Greenshaw, A.J.; Cribben, I.; Brett-MacLean, P.; Drolet, J.; McDonald-Harker, C.; Omeje, J.; Mankowsi, M.; Noble, S.; et al. After the Fort McMurray wildfire there are significant increases in mental health symptoms in grade 7–12 students compared to controls. BMC Psychiatry 2019, 19, 18. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.C.; Pereira, G.; Uhl, S.A.; Bravo, M.A.; Bell, M.L. A systematic review of the physical health impacts from non-occupational exposure to wildfire smoke. Environ. Res. 2015, 136, 120–132. [Google Scholar] [CrossRef] [Green Version]
- Herrera, A.M.; Cavada Ch, G.; Mañalich, M.J. Pediatric asthma hospitalization in Chile: 2001–2014. Rev. Chil. Pediatr. 2017, 88, 602–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moya Olivares, A.; Villarroel Del Pino, L.; Fierro Tolosa, L.; Foncea Fierro, C.; Caussade Larraín, S. Spirometric values in healthy preschool children. Rev. Chil. Pediatr. 2019, 90, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Sapunar, J.; Aguilar-Farías, N.; Navarro, J.; Araneda, G.; Chandía-Poblete, D.; Manríquez, V.; Brito, R.; Cerda, Á. High prevalence of dyslipidemia and high atherogenic index of plasma in children and adolescents. Rev. Med. Chile 2018, 146, 1112–1122. [Google Scholar] [CrossRef] [Green Version]
- Faustini, A.; Alessandrini, E.R.; Pey, J.; Perez, N.; Samoli, E.; Querol, X.; Cadum, E.; Perrino, C.; Ostro, B.; Ranzi, A.; et al. Short-term effects of particulate matter on mortality during forest fires in Southern Europe: Results of the MED-PARTICLES Project. Occup. Environ. Med. 2015, 72, 323–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oyarzún, M. Contaminación aérea y sus efectos en la salud. Rev. Chil. Enferm. Respir. 2010, 26, 16–25. [Google Scholar] [CrossRef] [Green Version]
- D’Amato, G.; Holgate, S.T.; Pawankar, R.; Ledford, D.K.; Cecchi, L.; Al-Ahmad, M.; Al-Enezi, F.; Al-Muhsen, S.; Ansotegui, I.; Baena-Cagnani, C.E.; et al. Meteorological conditions, climate change, new emerging factors, and asthma and related allergic disorders. A statement of the World Allergy Organization. World Allergy Organ. J. 2015, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Valparaíso Region | Santiago Region | |||
|---|---|---|---|---|
| Median | IQR | Median | IQR | |
| Concentration PM10 in summer (μg/m3) | 46.9 | 9.2 | 55.5 | 13.6 |
| Concentration PM10 in winter (μg/m3) | 42.9 | 7.2 | 74.0 | 20.8 |
| Temperature in summer (°C) | 18.3 | 1.1 | 20.4 | 2.0 |
| Temperature in winter (°C) | 12.8 | 1.1 | 8.9 | 2.3 |
| Precipitation in summer (mm/station) | 21.3 | 23.0 | 0.0 | 0.0 |
| Precipitation in winter (mm/station) | 75.5 | 43.1 | 79.1 | 101.5 |
| Population at risk <1 year (Number) | 23,580 | 100,202 | ||
| Population at risk 1 to 4 years (Number) | 93,111 | 397,375 | ||
| Population at risk 5 to 14 years (Number) | 239,915 | 964,422 | ||
| Valparaiso | Santiago | ||||
|---|---|---|---|---|---|
| Emergency Diagnosis | Age Stratum * | RR | 95% CI | RR | 95% CI |
| Bronchitis (J20-21) | <1 | 0.997 | 0.996–0.998 | 1.007 | 1.007–1.008 |
| 1 to 4 | 0.984 | 0.983–0.984 | 0.992 | 0.992–0.993 | |
| 5 to 14 | 0.977 | 0.977–0.978 | 0.978 | 0.978–0.979 | |
| Chronic lower respiratory disease (J40-46) | <1 | 0.994 | 0.994–0.995 | 1.012 | 1.012–1.013 |
| 1 to 4 | 0.985 | 0.985–0.985 | 0.996 | 0.996–0.996 | |
| 5 to 14 | 0.972 | 0.972–0.973 | 0.980 | 0.979–0.980 | |
| Acute upper respiratory infection (J00-J06) | <1 | 0.990 | 0.990–0.990 | 0.988 | 0.988–0.988 |
| 1 to 4 | 0.985 | 0.985–0.985 | 0.984 | 0.983–0.984 | |
| 5 to 14 | 0.980 | 0.980–0.980 | 0.981 | 0.981–0.981 | |
| Pneumonia (J12-18) | <1 | 1.000 | 0.999–1.001 | 1.026 | 1.026–1.027 |
| 1 to 4 | 0.990 | 0.989–0.990 | 1.016 | 1.015–1.016 | |
| 5 to 14 | 0.992 | 0.991–0.993 | 0.999 | 0.999–1.000 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciciretti, R.; Barraza, F.; De la Barrera, F.; Urquieta, L.; Cortes, S. Relationship between Wildfire Smoke and Children’s Respiratory Health in the Metropolitan Cities of Central-Chile. Atmosphere 2022, 13, 58. https://doi.org/10.3390/atmos13010058
Ciciretti R, Barraza F, De la Barrera F, Urquieta L, Cortes S. Relationship between Wildfire Smoke and Children’s Respiratory Health in the Metropolitan Cities of Central-Chile. Atmosphere. 2022; 13(1):58. https://doi.org/10.3390/atmos13010058
Chicago/Turabian StyleCiciretti, Rebecca, Francisco Barraza, Francisco De la Barrera, Lorna Urquieta, and Sandra Cortes. 2022. "Relationship between Wildfire Smoke and Children’s Respiratory Health in the Metropolitan Cities of Central-Chile" Atmosphere 13, no. 1: 58. https://doi.org/10.3390/atmos13010058
APA StyleCiciretti, R., Barraza, F., De la Barrera, F., Urquieta, L., & Cortes, S. (2022). Relationship between Wildfire Smoke and Children’s Respiratory Health in the Metropolitan Cities of Central-Chile. Atmosphere, 13(1), 58. https://doi.org/10.3390/atmos13010058