Identification of Prion Disease-Related Somatic Mutations in the Prion Protein Gene (PRNP) in Cancer Patients



Abstract
1. Introduction
2. Results
2.1. Previously Reported Prion Disease-Related Mutations
2.2. 48 Somatic Mutations in the PRNP Gene in Cancer Patients
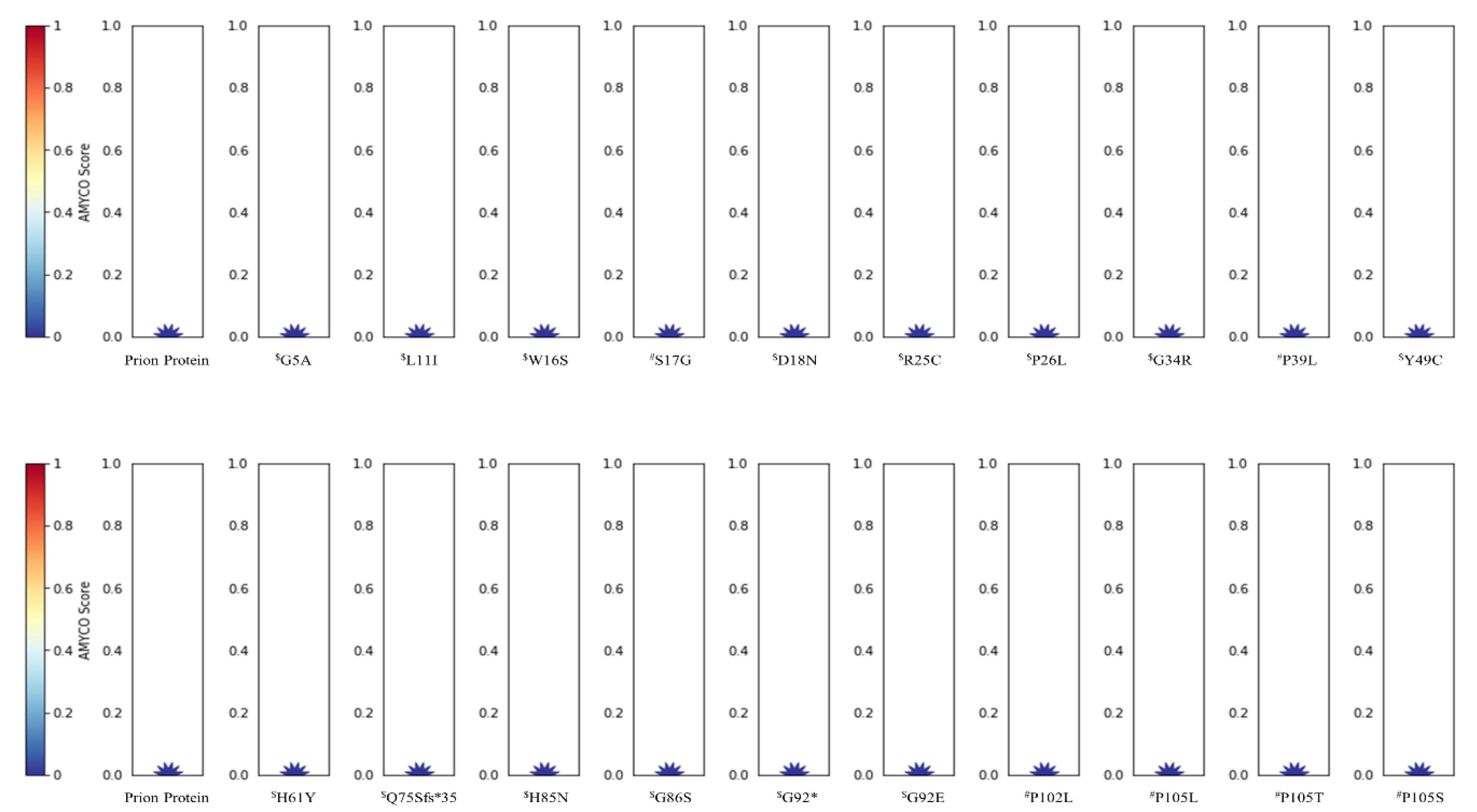
2.3. In Silico Annotation of Mutations in the PRNP Gene
3. Discussion
4. Material and Methods
4.1. Information on the Somatic Mutations in the PRNP Gene in Cancer Patients
4.2. Statistical Analysis
4.3. In Silico Evaluation of Somatic Mutations in the PRNP Gene in Cancer Patients
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| PrPSc | Misfolded prion protein |
| PrPC | Normal prion protein |
| PrP | Prion protein |
| TCGA | The Cancer Genome Atlas |
| BSE | Bovine spongiform encephalopathy |
| CJD | Creutzfeldt–Jakob disease |
| CWD | Chronic wasting disease |
| FFI | Fatal familial insomnia |
| GSS | Gerstmann–Sträussler–Scheinker syndrome |
| PRNP | Prion protein gene |
References
- Prusiner, S.B. Prions. Proc. Natl. Acad. Sci. USA 1998, 95, 13363–13383. [Google Scholar] [CrossRef] [PubMed]
- Prusiner, S.B. The prion diseases. Brain Pathol. 1998, 8, 499–513. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, B.M.; Murdoch, G.K. Genetics of Prion Disease in Cattle. Bioinform. Biol. Insights 2015, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kurt, T.D.; Sigurdson, C.J. Cross-species transmission of CWD prions. Prion 2016, 10, 83–91. [Google Scholar] [CrossRef]
- Greenlee, J.J. Review: Update on Classical and Atypical Scrapie in Sheep and Goats. Vet. Pathol. 2019, 56, 6–16. [Google Scholar] [CrossRef]
- Jeong, B.H.; Kim, Y.S. Genetic studies in human prion diseases. J. Korean Med. Sci. 2014, 29, 623–632. [Google Scholar] [CrossRef]
- Vaccari, G.; Panagiotidis, C.H.; Acin, C.; Peletto, S.; Barillet, F.; Acutis, P.; Bossers, A.; Langeveld, J.; van Keulen, L.; Sklaviadis, T.; et al. State-of-the-art review of goat TSE in the European Union, with special emphasis on PRNP genetics and epidemiology. Vet. Res. 2009, 40, 48. [Google Scholar] [CrossRef]
- Kim, Y.C.; Jeong, B.H. The first report of prion-related protein gene (PRNT) polymorphisms in goat. Acta. Vet. Hung. 2017, 65, 291–300. [Google Scholar] [CrossRef]
- Kim, Y.C.; Jeong, B.H. Bovine spongiform encephalopathy (BSE) associated polymorphisms of the prion-like protein gene (PRND) in Korean dairy cattle and Hanwoo. J. Dairy Res. 2018, 85, 7–11. [Google Scholar] [CrossRef]
- Kim, Y.C.; Jeong, B.H. First report of prion-related protein gene (PRNT) polymorphisms in cattle. Vet. Rec. 2018, 182, 717. [Google Scholar] [CrossRef]
- Kim, Y.C.; Kim, S.K.; Jeong, B.H. Scrapie susceptibility-associated indel polymorphism of shadow of prion protein gene (SPRN) in Korean native black goats. Sci. Rep. 2019, 9, 15261. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Kim, Y.C.; Won, S.Y.; Jeong, B.H. Potential scrapie-associated polymorphisms of the prion protein gene (PRNP) in Korean native black goats. Sci. Rep. 2019, 9, 15293. [Google Scholar] [CrossRef] [PubMed]
- Erickson, R.P. Somatic gene mutation and human disease other than cancer. Mutat. Res. 2003, 543, 125–136. [Google Scholar] [CrossRef]
- Leija-Salazar, M.; Piette, C.; Proukakis, C. Review: Somatic mutations in neurodegeneration. Neuropathol. Appl. Neurobiol. 2018, 44, 267–285. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Jeong, M.J.; Jeong, B.H. Strong association of regulatory single nucleotide polymorphisms (SNPs) of the IFITM3 gene with influenza H1N1 2009 pandemic virus infection. Cell. Mol. Immunol. 2019, in press. [Google Scholar] [CrossRef]
- Bagyinszky, E.; Giau, V.V.; Youn, Y.C.; An, S.S.A.; Kim, S. Characterization of mutations in PRNP (prion) gene and their possible roles in neurodegenerative diseases. Neuropsychiatr. Dis. Treat. 2018, 14, 2067–2085. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, S.; Mead, S.; Collinge, J. Genetics of prion disease. Top. Curr. Chem. 2011, 305, 1–22. [Google Scholar]
- Nicolas, G.; Veltman, J.A. The role of de novo mutations in adult-onset neurodegenerative disorders. Acta. Neuropathol. 2019, 137, 183–207. [Google Scholar] [CrossRef]
- Alzualde, A.; Moreno, F.; Martinez-Lage, P.; Ferrer, I.; Gorostidi, A.; Otaegui, D.; Blazquez, L.; Atares, B.; Cardoso, S.; Martinez de Pancorbo, M.; et al. Somatic mosaicism in a case of apparently sporadic Creutzfeldt-Jakob disease carrying a de novo D178N mutation in the PRNP gene. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2010, 153B, 1283–1291. [Google Scholar] [CrossRef]
- Dagvadorj, A.; Petersen, R.B.; Lee, H.S.; Cervenakova, L.; Shatunov, A.; Budka, H.; Brown, P.; Gambetti, P.; Goldfarb, L.G. Spontaneous mutations in the prion protein gene causing transmissible spongiform encephalopathy. Ann. Neurol. 2002, 52, 355–359. [Google Scholar] [CrossRef]
- Webb, T.E.; Poulter, M.; Beck, J.; Uphill, J.; Adamson, G.; Campbell, T.; Linehan, J.; Powell, C.; Brandner, S.; Pal, S.; et al. Phenotypic heterogeneity and genetic modification of P102L inherited prion disease in an international series. Brain 2008, 131, 2632–2646. [Google Scholar] [CrossRef]
- Santos, T.G.; Lopes, M.H.; Martins, V.R. Targeting prion protein interactions in cancer. Prion 2015, 9, 165–173. [Google Scholar] [CrossRef]
- Hinton, C.; Antony, H.; Hashimi, S.M.; Munn, A.; Wei, M.Q. Significance of prion and prion-like proteins in cancer development, progression and multi-drug resistance. Curr. Cancer. Drug Targets 2013, 13, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Gorgoulis, V.G.; Halazonetis, T.D. Genomic instability—an evolving hallmark of cancer. Nat. Rev. Mol. Cell. Biol. 2010, 11, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z. Genomic instability and cancer: An introduction. J. Mol. Cell. Biol. 2011, 3, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, K.; Czerwinska, P.; Wiznerowicz, M. The Cancer Genome Atlas (TCGA): An immeasurable source of knowledge. Contemp. Oncol. (Pozn) 2015, 19, A68–A77. [Google Scholar] [CrossRef] [PubMed]
- Adzhubei, I.; Jordan, D.M.; Sunyaev, S.R. Predicting functional effect of human missense mutations using PolyPhen-2. Curr. Protoc. Hum. Genet. 2013, 76, 7–20. [Google Scholar] [CrossRef]
- Choi, Y.; Chan, A.P. PROVEAN web server: A tool to predict the functional effect of amino acid substitutions and indels. Bioinformatics 2015, 31, 2745–2747. [Google Scholar] [CrossRef]
- Iglesias, V.; Conchillo-Sole, O.; Batlle, C.; Ventura, S. AMYCO: Evaluation of mutational impact on prion-like proteins aggregation propensity. BMC Bioinform. 2019, 20, 24. [Google Scholar] [CrossRef]
- Tang, H.; Thomas, P.D. PANTHER-PSEP: Predicting disease-causing genetic variants using position-specific evolutionary preservation. Bioinformatics 2016, 32, 2230–2232. [Google Scholar] [CrossRef]
- Won, S.Y.; Kim, Y.C.; Kim, K.; Kim, A.D.; Jeong, B.H. The First Report of Polymorphisms and Genetic Features of the prion-like Protein Gene (PRND) in a Prion Disease-Resistant Animal, Dog. Int. J. Mol. Sci. 2019, 20, 1404. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Jeong, B.H. In Silico Evaluation of Acetylation Mimics in the 27 Lysine Residues of Human Tau Protein. Curr. Alzheimer. Res. 2019, 16, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Mead, S.; Poulter, M.; Uphill, J.; Beck, J.; Whitfield, J.; Webb, T.E.; Campbell, T.; Adamson, G.; Deriziotis, P.; Tabrizi, S.J.; et al. Genetic risk factors for variant Creutzfeldt-Jakob disease: A genome-wide association study. Lancet Neurol. 2009, 8, 57–66. [Google Scholar] [CrossRef]
- Mead, S.; Uphill, J.; Beck, J.; Poulter, M.; Campbell, T.; Lowe, J.; Adamson, G.; Hummerich, H.; Klopp, N.; Ruckert, I.M.; et al. Genome-wide association study in multiple human prion diseases suggests genetic risk factors additional to PRNP. Hum. Mol. Genet. 2012, 21, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Minikel, E.V.; Vallabh, S.M.; Lek, M.; Estrada, K.; Samocha, K.E.; Sathirapongsasuti, J.F.; McLean, C.Y.; Tung, J.Y.; Yu, L.P.; Gambetti, P.; et al. Quantifying prion disease penetrance using large population control cohorts. Sci. Transl. Med. 2016, 8, 322ra329. [Google Scholar] [CrossRef]
- Pan, Y.; Zhao, L.; Liang, J.; Liu, J.; Shi, Y.; Liu, N.; Zhang, G.; Jin, H.; Gao, J.; Xie, H.; et al. Cellular prion protein promotes invasion and metastasis of gastric cancer. FASEB J. 2006, 20, 1886–1888. [Google Scholar] [CrossRef]
- Wang, Q.; Qian, J.; Wang, F.; Ma, Z. Cellular prion protein accelerates colorectal cancer metastasis via the Fyn-SP1-SATB1 axis. Oncol. Rep. 2012, 28, 2029–2034. [Google Scholar] [CrossRef]
- Manix, M.; Kalakoti, P.; Henry, M.; Thakur, J.; Menger, R.; Guthikonda, B.; Nanda, A. Creutzfeldt-Jakob disease: Updated diagnostic criteria, treatment algorithm, and the utility of brain biopsy. Neurosurg. Focus 2015, 39, E2. [Google Scholar] [CrossRef]
- Gao, Z.; Peng, M.; Chen, L.; Yang, X.; Li, H.; Shi, R.; Wu, G.; Cai, L.; Song, Q.; Li, C. Prion Protein Protects Cancer Cells against Endoplasmic Reticulum Stress Induced Apoptosis. Virol. Sin. 2019, 34, 222–234. [Google Scholar] [CrossRef]
- Yang, X.; Cheng, Z.; Zhang, L.; Wu, G.; Shi, R.; Gao, Z.; Li, C. Prion Protein Family Contributes to Tumorigenesis via Multiple Pathways. Adv. Exp. Med. Biol. 2017, 1018, 207–224. [Google Scholar]
- Watts, J.C.; Giles, K.; Bourkas, M.E.; Patel, S.; Oehler, A.; Gavidia, M.; Bhardwaj, S.; Lee, J.; Prusiner, S.B. Towards authentic transgenic mouse models of heritable PrP prion diseases. Acta. Neuropathol. 2016, 132, 593–610. [Google Scholar] [CrossRef] [PubMed]
- Sigurdson, C.J.; Joshi-Barr, S.; Bett, C.; Winson, O.; Manco, G.; Schwarz, P.; Rulicke, T.; Nilsson, K.P.; Margalith, I.; Raeber, A.; et al. Spongiform encephalopathy in transgenic mice expressing a point mutation in the beta2-alpha2 loop of the prion protein. J. Neurosci. 2011, 31, 13840–13847. [Google Scholar] [CrossRef]
- Gill, O.N.; Spencer, Y.; Richard-Loendt, A.; Kelly, C.; Brown, D.; Sinka, K.; Andrews, N.; Dabaghian, R.; Simmons, M.; Edwards, P.; et al. Prevalence in Britain of abnormal prion protein in human appendices before and after exposure to the cattle BSE epizootic. Acta Neuropathol. 2020, in press. [Google Scholar] [CrossRef]
- Wulf, M.A.; Senatore, A.; Aguzzi, A. The biological function of the cellular prion protein: An update. BMC Biol. 2017, 15, 34. [Google Scholar] [CrossRef] [PubMed]
- Altmeppen, H.C.; Puig, B.; Dohler, F.; Thurm, D.K.; Falker, C.; Krasemann, S.; Glatzel, M. Proteolytic processing of the prion protein in health and disease. Am. J. Neurodegener. Dis. 2012, 1, 15–31. [Google Scholar] [PubMed]
- Rangel, L.P.; Costa, D.C.; Vieira, T.C.; Silva, J.L. The aggregation of mutant p53 produces prion-like properties in cancer. Prion 2014, 8, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Scheckel, C.; Aguzzi, A. Prions, prionoids and protein misfolding disorders. Nat. Rev. Genet. 2018, 19, 405–418. [Google Scholar] [CrossRef]
- Silva, J.L.; Rangel, L.P.; Costa, D.C.; Cordeiro, Y.; De Moura Gallo, C.V. Expanding the prion concept to cancer biology: Dominant-negative effect of aggregates of mutant p53 tumour suppressor. Biosci. Rep. 2013, 33, e00054. [Google Scholar] [CrossRef]
- Morales, R.; Moreno-Gonzalez, I.; Soto, C. Cross-seeding of misfolded proteins: Implications for etiology and pathogenesis of protein misfolding diseases. PLoS Pathog. 2013, 9, e1003537. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Phenotypes | Mutations |
|---|---|
| Creutzfeldt–Jakob Disease (CJD) | G114V, D178N-129V, V180I, T183A, T188K, E196K, E196A, E200K, E200G, V203I, R208H, V210I, E211Q, I215V, M232R, P238S, double octapeptide deletion, and octapeptide insertions |
| Fatal familial insomnia (FFI) | D178N-129M |
| Gerstmann–Sträussler–Scheinker syndrome (GSS) | P102L, P105L, P105T, P105S, A117V, G131V, Y145*, Q160*, V176G, H187R, F198S, D202N, Q212P, Q217R, Y226*, Q227*, and M232T |
| Others | S17G, P39L, Y163*, D167N, D187fs, and R208C |
| Sample ID | Sex | Age | Cancer Type | AJCCMSC | AJCCTSC | Mutation | Mutation Type | Allele Frequency | # Mut |
|---|---|---|---|---|---|---|---|---|---|
| TCGA-4Z-AA7Q-01 | M | 79 | Bladder urothelial carcinoma | M0 | T3A | E146Q | Missense | 0.19 | 222 |
| TCGA-5N-A9KM-01 | F | 73 | Bladder urothelial carcinoma | MX | T4A | M1? | Nonstart | 0.36 | 189 |
| TCGA-IR-A3LK-01 | F | 69 | Cervical squamous cell carcinoma | M0 | T1B2 | G131V | Missense | 0.14 | 1189 |
| TCGA-KN-8428-01 | M | 71 | Chromophobe renal cell carcinoma | NA | T2 | V203I | Missense | 0.20 | 673 |
| TCGA-CK-5916-01 | F | 71 | Colon adenocarcinoma | M0 | T1 | V180I | Missense | 0.25 | 1407 |
| TCGA-EE-A29V-06 | M | 85 | Cutaneous melanoma | M0 | T3B | G92E | Missense | 0.42 | 1012 |
| TCGA-EB-A41A-01 | M | 90 | Cutaneous melanoma | M0 | T4B | L125F | Missense | 0.44 | 1533 |
| TCGA-D3-A2JC-06 | F | 53 | Cutaneous melanoma | M0 | T0 | M166I | Missense | 0.11 | 3148 |
| TCGA-D3-A8GM-06 | M | 73 | Cutaneous melanoma | M0 | T3B | G86S | Missense | 0.09 | 3288 |
| TCGA-YD-A9TA-06 | M | 75 | Cutaneous melanoma | NA | NA | H61Y | Missense | 0.29 | 2782 |
| TCGA-L5-A43J-01 | M | 90 | Esophageal squamous cell carcinoma | MX | T3 | R25C | Missense | 0.20 | 700 |
| TCGA-F7-A624-01 | M | 73 | Head and neck squamous cell carcinoma | M0 | T2 | R208H | Missense | 0.16 | 2744 |
| TCGA-VQ-A91D-01 | M | 70 | Intestinal type stomach adenocarcinoma | M0 | T4B | R208C | Missense | 0.25 | 2140 |
| TCGA-67-3771-01 | F | 77 | Lung adenocarcinoma | M0 | T1 | N173H | Missense | 0.12 | 951 |
| TCGA-44-5644-01 | F | 51 | Lung adenocarcinoma | NA | T2A | G5A | Missense | 0.34 | 908 |
| TCGA-69-A59K-01 | F | 60 | Lung adenocarcinoma | M0 | T3 | G119R | Missense | 0.21 | 438 |
| TCGA-17-Z023-01 | NA | NA | Lung adenocarcinoma | NA | NA | Y49C | Missense | 0.23 | 362 |
| TCGA-17-Z026-01 | NA | NA | Lung adenocarcinoma | NA | NA | E211Q | Missense | 0.19 | 873 |
| TCGA-22-5489-01 | M | 64 | Lung squamous cell carcinoma | M0 | T1B | Y145C | Missense | 0.21 | 227 |
| TCGA-63-A5MM-01 | F | 69 | Lung squamous cell carcinoma | M0 | T2 | H177N | Missense | 0.23 | 1070 |
| TCGA-NC-A5HH-01 | M | 53 | Lung squamous cell carcinoma | M0 | T1 | W16S | Missense | 0.27 | 314 |
| TCGA-G7-6790-01 | M | 57 | Papillary renal cell carcinoma | MX | T1A | Q217K | Missense | 0.09 | 71 |
| TCGA-F9-A97G-01 | M | 79 | Papillary renal cell carcinoma | M0 | T3 | V252L | Missense | 0.20 | 62 |
| TCGA-AG-A002-01 | M | 35 | Rectal adenocarcinoma | M0 | T2 | P26L | Missense | 0.45 | 11,438 |
| TCGA-B0-5713-01 | F | 75 | Renal clear cell carcinoma | M0 | T3B | E221G | Missense | 0.30 | 97 |
| TCGA-25-1313-01 | F | 62 | Serous ovarian cancer | NA | NA | G131R | Missense | 0.37 | 179 |
| TCGA-VQ-A8PO-01 | M | 74 | Signet ring cell carcinoma of the stomach | M0 | T4A | M129T | Missense | 0.23 | 751 |
| TCGA-BR-6452-01 | F | 78 | Stomach adenocarcinoma | M0 | T3 | I244F | Missense | 0.19 | 5050 |
| TCGA-CG-5717-01 | M | 58 | Stomach adenocarcinoma | M0 | T2B | R151C | Missense | 0.34 | 117 |
| TCGA-CG-5723-01 | M | 83 | Stomach adenocarcinoma | M0 | T2 | V209M | Missense | 0.08 | 1606 |
| TCGA-VQ-A8PP-01 | M | 76 | Tubular stomach adenocarcinoma | M0 | T4 | K104E | Missense | 0.36 | 1328 |
| TCGA-DX-AB2Z-01 | F | 87 | Undifferentiated pleomorphic sarcoma | NA | NA | R148H | Missense | 0.11 | 69 |
| TCGA-N7-A4Y0-01 | F | 65 | Uterine carcinosarcoma | NA | NA | C214G | Missense | 0.64 | 709 |
| TCGA-ND-A4WC-01 | NA | NA | Uterine carcinosarcoma | NA | NA | H85N | Missense | 0.20 | 3669 |
| TCGA-B5-A0JY-01 | F | 50 | Uterine endometrioid carcinoma | NA | NA | K204N | Missense | 0.34 | 9713 |
| TCGA-D1-A17Q-01 | F | 54 | Uterine endometrioid carcinoma | NA | NA | D167N | Missense | 0.40 | 5945 |
| TCGA-AP-A1DV-01 | F | 59 | Uterine endometrioid carcinoma | NA | NA | R25C | Missense | 0.52 | 12,071 |
| TCGA-FI-A2D5-01 | F | 56 | Uterine endometrioid carcinoma | NA | NA | D202N | Missense | 0.38 | 13,874 |
| TCGA-AJ-A3EL-01 | F | 47 | Uterine endometrioid carcinoma | NA | NA | L11I | Missense | 0.40 | 7391 |
| TCGA-AP-A0LT-01 | F | 57 | Uterine endometrioid carcinoma | NA | NA | E196Rfs*10 | Frame shift del | 0.28 | 638 |
| TCGA-AP-A1DV-01 | F | 59 | Uterine endometrioid carcinoma | NA | NA | Y218C | Missense | 0.42 | 12,071 |
| TCGA-AX-A3FT-01 | F | 64 | Uterine endometrioid carcinoma | NA | NA | Q75Sfs*35 | Frame shift del | 0.23 | 1281 |
| TCGA-B5-A1MX-01 | F | 47 | Uterine endometrioid carcinoma | NA | NA | G92* | Nonsense | 0.33 | 5699 |
| TCGA-BG-A222-01 | F | 49 | Uterine endometrioid carcinoma | NA | NA | G34R | Missense | 0.45 | 4276 |
| TCGA-DF-A2KU-01 | F | NA | Uterine endometrioid carcinoma | NA | NA | S230L | Missense | 0.30 | 10,058 |
| TCGA-EO-A22R- | F | 56 | Uterine endometrioid carcinoma | NA | NA | S230L | Missense | 0.30 | 12,783 |
| TCGA-EY-A1GK-01 | F | 74 | Uterine endometrioid carcinoma | NA | NA | G35Afs*75 | Frame shift del | 0.30 | 841 |
| TCGA-A5-A0G2-01 | F | 57 | Uterine serous carcinoma | NA | NA | D18N | Missense | 0.18 | 25,730 |
| Characteristics | All Cancer Patients | Subgroup 1 | Subgroup 2 | |
|---|---|---|---|---|
| Number of patients | 10,953 | 47 | 8 | |
| % compared to all cancer patients | - | 0.43% | 0.07% | |
| % compared to subgroup 1 | - | - | 17.02% | |
| Number of samples | 10,967 | 48 | 8 | |
| % compared to all cancer patients | 0.44% | 0.07% | ||
| % compared to subgroup 1 | - | - | 16.67% | |
| Diagnosis age (mean ± SD) | 59.1 ± 14.5 | 66 ± 12.8 | 66.3 ± 7.8 | |
| p-value compared to all cancer patients | 0.000742 | 0.093018 | ||
| p-value compared to subgroup 1 | - | - | 0.477389 | |
| Sex, N (%) | Male | 4866 (44.4%) | 18 (37.5%) | 3 (37.5%) |
| Female | 5315 (48.5%) | 27 (56.2%) | 4 (50.0%) | |
| NA | 772 (7.0%) | 3 (6.3%) | 1 (12.5%) | |
| Total | 10,953 | 48 | 8 | |
| p-value compared to all cancer patients | - | 0.30 | 0.79 | |
| p-value compared to subgroup 1 | - | - | 0.89 | |
| Mutation count | <100 | 6798 (67.3%) | 4 (8.3%) | 0 (0%) |
| 100 ≤ x < 200 | 1516 (15.0%) | 2 (4.2%) | 0 (0%) | |
| 200 ≤ x < 280 | 455 (4.5%) | 2 (4.2%) | 0 (0%) | |
| >280 | 1328 (13.2%) | 40 (83.3%) | 8 (100%) | |
| Total | 10,097 (100%) | 48 | 8 | |
| p-value compared to all cancer patients | - | <0.00001 | 2.3 × 10−11 | |
| p-value compared to subgroup 1 | - | - | 0.67 | |
| Cancer type, N (%) | Invasive breast carcinoma | 1084 (9.9%) | 0 (0%) | 0 (0%) |
| Non-small cell lung cancer | 1053 (9.6%) | 8 (16.7%) | 1 (12.5%) | |
| Colorectal adenocarcinoma | 594 (5.4%) | 2 (4.2%) | 1 (12.5%) | |
| Glioblastoma | 592 (5.4%) | 0 (0%) | 0 (0%) | |
| Endometrial carcinoma | 586 (5.3%) | 16 (33.3%) | 2 (25.0%) | |
| Ovarian epithelial tumor | 585 (5.3%) | 1 (2.1%) | 0 | |
| Head and neck squamous cell carcinoma | 523 (4.8%) | 1 (2.1%) | 1 (12.5%) | |
| Esophagogastric adenocarcinoma | 514 (4.7%) | 5 (10.4%) | 1 (12.5%) | |
| Diffuse glioma | 513 (4.7%) | 0 (0%) | 0 (0%) | |
| Renal clear cell carcinoma | 512 (4.7%) | 1 (2.1%) | 0 (0%) | |
| Well-differentiated thyroid | 500 (4.6%) | 0 (0%) | 0 (0%) | |
| Prostate adenocarcinoma | 494 (4.5%) | 0 (0%) | 0 (0%) | |
| Melanoma | 448 (4.1%) | 5 (10.4%) | 0 (0%) | |
| Bladder urothelial carcinoma | 411 (3.7%) | 2 (4.2%) | 0 (0%) | |
| Hepatocellular carcinoma | 369 (3.4%) | 0 (0%) | 0 (0%) | |
| Renal non-clear cell carcinoma | 348 (3.2%) | 3 (6.3%) | 1 (12.5%) | |
| Sarcoma | 255 (2.3%) | 1 (2.1%) | 0 (0%) | |
| Cervical squamous cell carcinoma | 251 (2.3%) | 1 (2.1%) | 1 (12.5%) | |
| Leukemia | 200 (1.8%) | 0 (0%) | 0 (0%) | |
| Pancreatic adenocarcinoma | 184 (1.7%) | 0 (0%) | 0 (0%) | |
| Pheochromocytoma | 147 (1.3%) | 0 (0%) | 0 (0%) | |
| Thymic epithelial tumor | 123 (1.1%) | 0 (0%) | 0 (0%) | |
| Esophageal squamous cell carcinoma | 95 (0.9%) | 1 (2.1%) | 0 (0%) | |
| Adrenocortical carcinoma | 92 (0.8%) | 0 (0%) | 0 (0%) | |
| Pleural mesothelioma | 87 (0.8%) | 0 (0%) | 0 (0%) | |
| Non-seminomatous germ cell tumor | 86 (0.8%) | 0 (0%) | 0 (0%) | |
| Ocular melanoma | 80 (0.7%) | 0 (0%) | 0 (0%) | |
| Seminoma | 63 (0.6%) | 0 (0%) | 0 (0%) | |
| Mature B-cell neoplasms | 48 (0.4%) | 0 (0%) | 0 (0%) | |
| Cervical adenocarcinoma | 46 (0.4%) | 0 (0%) | 0 (0%) | |
| Cholangiocarcinoma | 36 (0.3%) | 0 (0%) | 0 (0%) | |
| Miscellaneous neuroepithelial tumor | 31 (0.3%) | 0 (0%) | 0 (0%) | |
| Undifferentiated stomach adenocarcinoma | 13 (0.1%) | 1 (2.1%) | 0 (0%) | |
| Fibrolamellar carcinoma | 3 (<0.1%) | 0 (0%) | 0 (0%) | |
| Encapsulated glioma | 1 (<0.1%) | 0 (0%) | 0 (0%) | |
| Total | 10,967 | 48 | 8 | |
| p-value compared to all cancer patients | - | 6 × 10−12 | 0.96 | |
| p-value compared to subgroup 1 | - | - | NA |
| Mutations | PolyPhen-2 | PANTHER | PROVEAN | |||
|---|---|---|---|---|---|---|
| Score | Prediction | Preservation Time | Prediction | Score | Prediction | |
| $ G5A | 0.729 | Possibly damaging | 176 | Probably benign | −1.238 | Neutral |
| $ L11I | 0.161 | Benign | 176 | Probably benign | −0.306 | Neutral |
| $ W16S | 0.546 | Possibly damaging | 176 | Probably benign | −1.237 | Neutral |
| # S17G | 0.528 | Possibly damaging | 176 | Probably benign | −0.239 | Neutral |
| $ D18N | 1.000 | Probably damaging | 176 | Probably benign | −0.104 | Neutral |
| $ R25C | 1.000 | Probably damaging | 176 | Probably benign | −1.801 | Neutral |
| $ P26L | 0.995 | Probably damaging | 324 | Possibly damaging | −3.263 | Deleterious |
| $ G34R | 1.000 | Probably damaging | 220 | Possibly damaging | −3.889 | Deleterious |
| # P39L | 1.000 | Probably damaging | 361 | Possibly damaging | −4.000 | Deleterious |
| $ Y49C | 1.000 | Probably damaging | 176 | Probably benign | −2.222 | Neutral |
| $ H61Y | 0.975 | Probably damaging | 176 | Probably benign | −1.021 | Neutral |
| $ H85N | 0.975 | Probably damaging | 176 | Probably benign | −0.833 | Neutral |
| $ G86S | 1.000 | Probably damaging | 324 | Possibly damaging | −0.995 | Neutral |
| $ G92E | 1.000 | Probably damaging | 176 | Probably benign | −1.253 | Neutral |
| # P102L | 1.000 | Probably damaging | 361 | Possibly damaging | −3.392 | Deleterious |
| # P105L | 1.000 | Probably damaging | 324 | Possibly damaging | −3.271 | Deleterious |
| # P105T | 0.998 | Probably damaging | 324 | Possibly damaging | −2.333 | Neutral |
| # P105S | 0.997 | Probably damaging | 324 | Possibly damaging | −1.496 | Neutral |
| $ K104E | 0.974 | Probably damaging | 324 | Possibly damaging | −1.208 | Neutral |
| # G114V | 1.000 | Probably damaging | 220 | Possibly damaging | −2.540 | Deleterious |
| # A117V | 0.999 | Probably damaging | 176 | Probably benign | −1.263 | Neutral |
| $ G119R | 1.000 | Probably damaging | 361 | Possibly damaging | −2.586 | Deleterious |
| $ L125F | 1.000 | Probably damaging | 324 | Possibly damaging | −0.398 | Neutral |
| $ M129T | 0.181 | Benign | 324 | Possibly damaging | −1.156 | Neutral |
| $ G131R | 1.000 | Probably damaging | 361 | Possibly damaging | −2.451 | Neutral |
| #,$ G131V | 1.000 | Probably damaging | 361 | Possibly damaging | −2.879 | Deleterious |
| $ Y145C | 0.997 | Probably damaging | 220 | Possibly damaging | −1.742 | Neutral |
| $ E146Q | 0.992 | Probably damaging | 361 | Possibly damaging | −0.985 | Neutral |
| $ R148H | 1.000 | Probably damaging | 361 | Possibly damaging | −1.735 | Neutral |
| $ R151C | 0.009 | Benign | 220 | Possibly damaging | −2.016 | Neutral |
| $ M166I | 0.000 | Benign | 30 | Probably benign | 0.254 | Neutral |
| #,$ D167N | 0.001 | Benign | 220 | Possibly damaging | −0.631 | Neutral |
| $ N173H | 0.952 | Probably damaging | 176 | Probably benign | −1.573 | Neutral |
| # V176G | 0.998 | Probably damaging | 361 | Possibly damaging | −2.253 | Neutral |
| $ H177N | 0.313 | Benign | 220 | Possibly damaging | −0.455 | Neutral |
| # D178N-129M | 1.000 | Probably damaging | 361 | Possibly damaging | −1.531 | Neutral |
| # D178N-129V | 1.000 | Probably damaging | 361 | Possibly damaging | −1.451 | Neutral |
| #,$ V180I | 0.009 | Benign | 220 | Possibly damaging | −0.11 | Neutral |
| # T183A | 0.978 | Probably damaging | 324 | Possibly damaging | −1.785 | Neutral |
| # H187R | 0.989 | Probably damaging | 220 | Possibly damaging | −2.607 | Deleterious |
| # T188K | 0.996 | Probably damaging | 324 | Possibly damaging | −0.550 | Neutral |
| # E196K | 0.624 | Possibly damaging | 220 | Possibly damaging | −0.641 | Neutral |
| # E196A | 0.472 | Possibly damaging | 220 | Possibly damaging | −1.206 | Neutral |
| # F198S | 0.994 | Probably damaging | 220 | Possibly damaging | −0.792 | Neutral |
| # E200K | 0.995 | Probably damaging | 361 | Possibly damaging | −1.478 | Neutral |
| # E200G | 0.994 | Probably damaging | 361 | Possibly damaging | −3.245 | Deleterious |
| #,$ D202N | 1.000 | Probably damaging | 220 | Possibly damaging | −1.118 | Neutral |
| #,$ V203I | 0.001 | Benign | 176 | Probably benign | −0.004 | Neutral |
| $ K204N | 0.898 | Possibly damaging | 220 | Possibly damaging | −1.815 | Neutral |
| #,$ R208C | 1.000 | Probably damaging | 220 | Possibly damaging | −2.324 | Neutral |
| #,$ R208H | 0.999 | Probably damaging | 220 | Possibly damaging | −0.855 | Neutral |
| $ V209M | 0.613 | Possibly damaging | 324 | Possibly damaging | −1.03 | Neutral |
| # V210I | 0.803 | Possibly damaging | 220 | Possibly damaging | 0.039 | Neutral |
| #,$ E211Q | 0.992 | Probably damaging | 220 | Possibly damaging | −0.36 | Neutral |
| # Q212P | 0.930 | Possibly damaging | 220 | Possibly damaging | −1.665 | Neutral |
| $ C214G | 0.975 | Probably damaging | 361 | Possibly damaging | −4.402 | Deleterious |
| # I215V | 0.000 | Benign | 220 | Possibly damaging | −0.099 | Neutral |
| # Q217R | 0.961 | Probably damaging | 220 | Possibly damaging | −1.306 | Neutral |
| $ Q217K | 0.942 | Probably damaging | 220 | Possibly damaging | −1.186 | Neutral |
| $ Y218C | 1.000 | Probably damaging | 361 | Possibly damaging | −3.626 | Deleterious |
| $ E221G | 0.651 | Possibly damaging | 220 | Possibly damaging | −1.244 | Neutral |
| $ S230L | 0.947 | Possibly damaging | 97 | Probably benign | −1.372 | Neutral |
| # M232R | 0.082 | Benign | 91 | Probably benign | −1.167 | Neutral |
| # M232T | 0.000 | Benign | 91 | Probably benign | −0.825 | Neutral |
| # P238S | 1.000 | Probably damaging | 361 | Possibly damaging | −1.189 | Neutral |
| $ I244F | 0.001 | Benign | 176 | Probably benign | −0.939 | Neutral |
| $ V252L | 0.990 | Probably damaging | 176 | Probably benign | −0.411 | Neutral |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-C.; Won, S.-Y.; Jeong, B.-H. Identification of Prion Disease-Related Somatic Mutations in the Prion Protein Gene (PRNP) in Cancer Patients. Cells 2020, 9, 1480. https://doi.org/10.3390/cells9061480
Kim Y-C, Won S-Y, Jeong B-H. Identification of Prion Disease-Related Somatic Mutations in the Prion Protein Gene (PRNP) in Cancer Patients. Cells. 2020; 9(6):1480. https://doi.org/10.3390/cells9061480
Chicago/Turabian StyleKim, Yong-Chan, Sae-Young Won, and Byung-Hoon Jeong. 2020. "Identification of Prion Disease-Related Somatic Mutations in the Prion Protein Gene (PRNP) in Cancer Patients" Cells 9, no. 6: 1480. https://doi.org/10.3390/cells9061480
APA StyleKim, Y.-C., Won, S.-Y., & Jeong, B.-H. (2020). Identification of Prion Disease-Related Somatic Mutations in the Prion Protein Gene (PRNP) in Cancer Patients. Cells, 9(6), 1480. https://doi.org/10.3390/cells9061480