Focused Ultrasound-Induced Cavitation Sensitizes Cancer Cells to Radiation Therapy and Hyperthermia


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Tumor Cell Lines and Cell Culturing
2.2. FUS In Vitro System
2.3. Cavitation Dose Measurement with a Fiber-Optic Hydrophone (FOH)
2.4. Cavitation Dose Measurement with Terephthalic Acid (TA)
2.5. FUS Treatment of Cancer Cells
2.6. HT Treatment with Water Bath
2.7. RT with X-ray In Vitro
2.8. Combination Treatment Protocol of Cancer Cells
2.9. Clonogenic Assay
2.10. WST-1 Assay
2.11. Invasion Assay
2.12. Detection of Sonoporation by Cell Staining with Propidium Iodide (PI)
2.13. Statistical Analysis
3. Results
3.1. Cavitation Occurs at a Certain Level of Intensity
3.2. Short High-Intensity Cavitation-Inducing FUS Shots (FUS-Cav) Are Effective to Radiosensitize Tumor Cells
3.3. Short High-Intensity FUS-Induced Cavitation Shots (FUS-Cav) Increase the Effect of HT
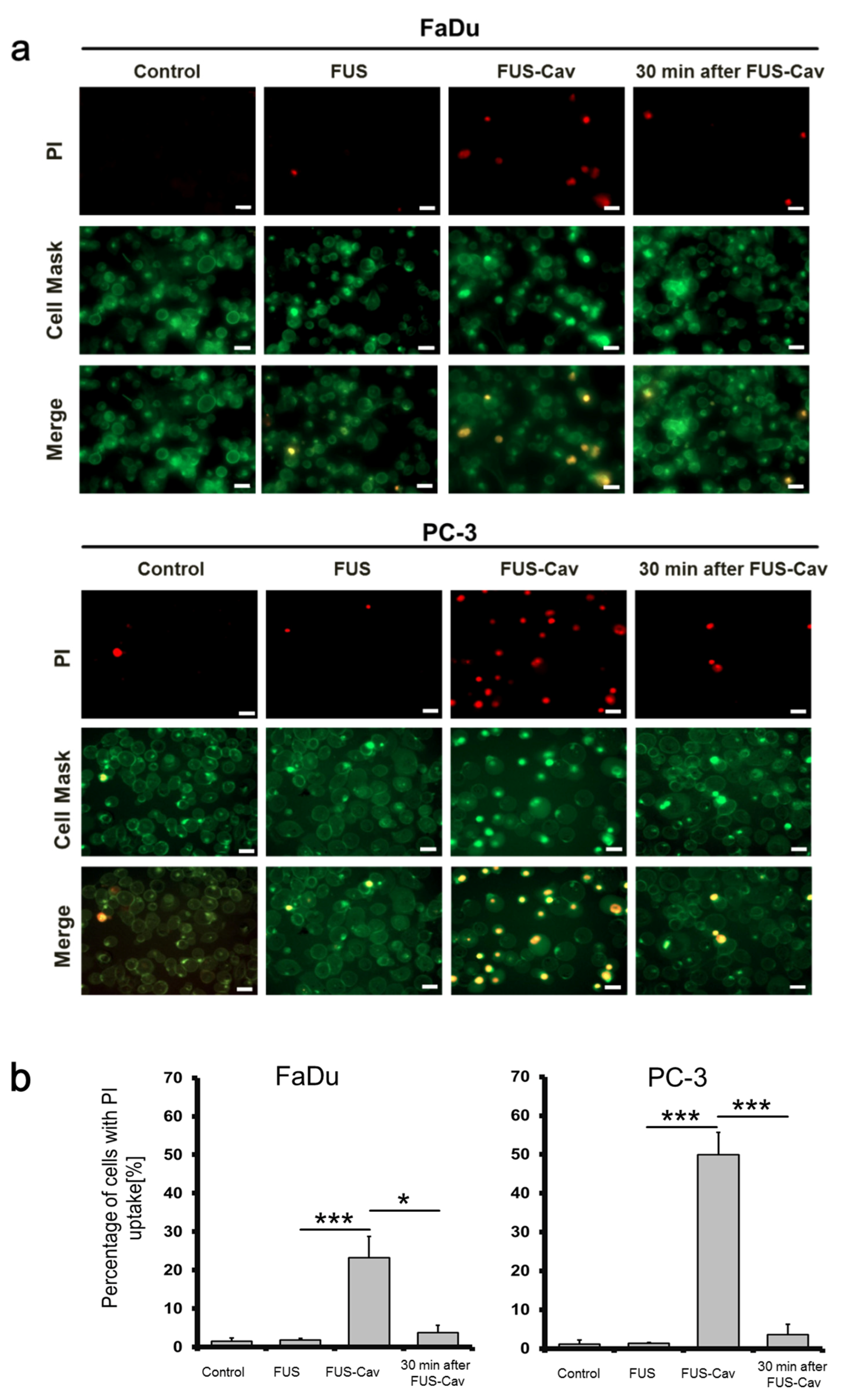
3.4. FUS-Cav Treatment Immediately Induced Sonoporation Effect
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| FUS | Focused ultrasound |
| RT | Radiation therapy |
| HT | Hyperthermia |
| FUS-Cav | FUS shot with cavitation |
| HIFU | High-intensity focused ultrasound |
| MR | Magnetic resonance |
| BBB | Blood–brain barrier |
| PCD | Passive cavitation detector |
| TA | Terephthalate acid |
| FOH | Fiber-optic hydrophone |
| DMEM | Dulbecco’s Modified Eagle’s Medium |
| HEPES | 4-(2- Hydroxyethyl)-piperazine- 1- ethanesulfonic acid |
| MEM | Minimum Essential Medium |
| FBS | Fetal bovine serum |
| PBS | Phosphate-buffered saline |
| EDTA | Ethylenediaminetetraacetic acid |
| FFT | Fast Fourier transformation |
| RMS | Root-mean-square |
| SF | Survival fraction |
| PI | Propidium iodide |
| SD | Standard deviation |
| SEM | Standard error of the mean |
References
- Siedek, F.; Yeo, S.Y.; Heijman, E.; Grinstein, O.; Bratke, G.; Heneweer, C.; Puesken, M.; Persigehl, T.; Maintz, D.; Grüll, H. Magnetic Resonance-Guided High-Intensity Focused Ultrasound (MR-HIFU): Technical Background and Overview of Current Clinical Applications (Part 1). RöFo—Fortschr. Geb. Röntgenstrahlen Bildgeb. Verfahr. 2019, 191, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Bour, P.; Ozenne, V.; Marquet, F.; De Senneville, B.D.; Dumont, E.; Quesson, B. Real-time 3D ultrasound based motion tracking for the treatment of mobile organs with MR-guided high-intensity focused ultrasound. Int. J. Hyperth. 2018, 34, 1225–1235. [Google Scholar] [CrossRef] [PubMed]
- Elming, P.B.; Sørensen, B.S.; Oei, A.L.; Franken, N.A.; Crezee, J.; Overgaard, J.; Horsman, M.R. Hyperthermia: The Optimal Treatment to Overcome Radiation Resistant Hypoxia. Cancers 2019, 11, 60. [Google Scholar] [CrossRef] [PubMed]
- Roti, J.L.R. Introduction: Radiosensitization by hyperthermia. Int. J. Hyperth. 2004, 20, 109–114. [Google Scholar] [CrossRef]
- Peeken, J.C.; Vaupel, P.; Combs, S.E. Integrating Hyperthermia into Modern Radiation Oncology: What Evidence Is Necessary? Front. Oncol. 2017, 7, 7. [Google Scholar] [CrossRef]
- Baronzio, G.; Parmar, G.; Ballerini, M.; Szasz, A.; Cassutti, V. A Brief Overview of Hyperthermia in Cancer Treatment. J. Integr. Oncol. 2014, 3. [Google Scholar] [CrossRef]
- Phenix, C.P.; Togtema, M.; Pichardo, S.; Zehbe, I.; Curiel, L. High intensity focused ultrasound technology, its scope and applications in therapy and drug delivery. J. Pharm. Pharm. Sci. 2014, 17, 136–153. [Google Scholar] [CrossRef]
- Bull, V.; Civale, J.; Rivens, I.; Ter Haar, G. A Comparison of Acoustic Cavitation Detection Thresholds Measured with Piezo-electric and Fiber-optic Hydrophone Sensors. Ultrasound Med. Biol. 2013, 39, 2406–2421. [Google Scholar] [CrossRef]
- Prentice, P.; Cuschieri, A.; Dholakia, K.; Prausnitz, M.; Campbell, P. Membrane disruption by optically controlled microbubble cavitation. Nat. Phys. 2005, 1, 107–110. [Google Scholar] [CrossRef]
- Collis, J.; Manasseh, R.; Liovic, P.; Tho, P.; Ooi, A.; Petkovic-Duran, K.; Zhu, Y. Cavitation microstreaming and stress fields created by microbubbles. Ultrasonics 2010, 50, 273–279. [Google Scholar] [CrossRef]
- Coussios, C.C.; Roy, R.A. Applications of Acoustics and Cavitation to Noninvasive Therapy and Drug Delivery. Annu. Rev. Fluid Mech. 2008, 40, 395–420. [Google Scholar] [CrossRef]
- Gourevich, D.; Volovick, A.; Dogadkin, O.; Wang, L.; Mulvana, H.; Medan, Y.; Melzer, A.; Cochran, S. In Vitro Investigation of the Individual Contributions of Ultrasound-Induced Stable and Inertial Cavitation in Targeted Drug Delivery. Ultrasound Med. Biol. 2015, 41, 1853–1864. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, A.; Liu, M.; Ojha, T.; Storm, G.; Kiessling, F.; Lammers, T.G.G.M. Ultrasound-mediated drug delivery to the brain: Principles, progress and prospects. Drug Discov. Today Technol. 2016, 20, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, A.; Sapozhnikov, O.; Bailey, M.; Crum, L.; Xu, Z.; Fowlkes, B.; Cain, C.; Khokhlova, V. Disintegration of Tissue Using High Intensity Focused Ultrasound: Two Approaches That Utilize Shock Waves. Acoust. Today 2012, 8, 24. [Google Scholar] [CrossRef]
- Chaplin, V.; Caskey, C.F. Multi-focal HIFU reduces cavitation in mild-hyperthermia. J. Ther. Ultrasound 2017, 5, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bian, S.N.; Seth, A.; Daly, D.; Carlisle, R.; Stride, E. A multimodal instrument for real-time in situ study of ultrasound and cavitation mediated drug delivery. Rev. Sci. Instrum. 2017, 88, 034302. [Google Scholar] [CrossRef] [PubMed]
- Gerold, B.; Kotopoulis, S.; McDougall, C.; McGloin, D.; Postema, M.; Prentice, P. Laser-nucleated acoustic cavitation in focused ultrasound. Rev. Sci. Instrum. 2011, 82, 044902. [Google Scholar] [CrossRef]
- Canney, M.S.; Khokhlova, V.A.; Bessonova, O.V.; Bailey, M.R.; Crum, L.A. Shock-Induced Heating and Millisecond Boiling in Gels and Tissue Due to High Intensity Focused Ultrasound. Ultrasound Med. Biol. 2010, 36, 250–267. [Google Scholar] [CrossRef]
- Jensen, C.R.; Ritchie, R.; Gyongy, M.; Collin, J.R.T.; Leslie, T.A.; Coussios, C.C. Spatiotemporal Monitoring of High-Intensity Focused Ultrasound Therapy with Passive Acoustic Mapping. Radiology 2012, 262, 252–261. [Google Scholar] [CrossRef]
- Zhang, S.; Yin, L.; Fang, N. Focusing Ultrasound with an Acoustic Metamaterial Network. Phys. Rev. Lett. 2009, 102, 194301. [Google Scholar] [CrossRef]
- Villeneuve, L.; Alberti, L.; Steghens, J.; Lancelin, J.; Mestas, J.-L. Assay of hydroxyl radicals generated by focused ultrasound. Ultrason. Sonochem. 2009, 16, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Lai, P.; Tarapacki, C.; Tran, W.T.; El Kaffas, A.; Lee, J.; Hupple, C.; Iradji, S.; Giles, A.; Al-Mahrouki, A.; Czarnota, G.J. Breast tumor response to ultrasound mediated excitation of microbubbles and radiation therapy in vivo. Oncoscience 2016, 3, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Bobeica, M.; Unger, M.; Bednarz, A.; Gerold, B.; Patties, I.; Melzer, A.; Landgraf, L. Focused ultrasound radiosensitize human cancer cells by enhancement of DNA damage. 2020; Submitted. [Google Scholar]
- Barati, A.H.; Mokhtari-Dizaji, M.; Mozdarani, H.; Bathaie, Z.; Hassan, Z.M. Effect of exposure parameters on cavitation induced by low-level dual-frequency ultrasound. Ultrason. Sonochem. 2007, 14, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Bezjak, A.; Paulus, R.; Gaspar, L.E.; Timmerman, R.D.; Straube, W.L.; Ryan, W.F.; Garces, Y.I.; Pu, A.T.; Singh, A.K.; Videtic, G.M.; et al. Safety and Efficacy of a Five-Fraction Stereotactic Body Radiotherapy Schedule for Centrally Located Non–Small-Cell Lung Cancer: NRG Oncology/RTOG 0813 Trial. J. Clin. Oncol. 2019, 37, 1316–1325. [Google Scholar] [CrossRef] [PubMed]
- Le, Q.-T.; Loo, B.W.; Ho, A.; Cotrutz, C.; Koong, A.C.; Wakelee, H.; Kee, S.T.; Constantinescu, D.; Whyte, R.I.; Donington, J. Results of a Phase I Dose-Escalation Study Using Single-Fraction Stereotactic Radiotherapy for Lung Tumors. J. Thorac. Oncol. 2006, 1, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Franken, N.; Rodermond, H.M.; Stap, J.; Haveman, J.; Van Bree, C. Clonogenic assay of cells in vitro. Nat. Protoc. 2006, 1, 2315–2319. [Google Scholar] [CrossRef]
- Patties, I.; Kallendrusch, S.; Böhme, L.; Kendzia, E.; Oppermann, H.; Gaunitz, F.; Kortmann, R.-D.; Glasow, A. The Chk1 inhibitor SAR-020106 sensitizes human glioblastoma cells to irradiation, to temozolomide, and to decitabine treatment. J. Exp. Clin. Cancer Res. 2019, 38, 420. [Google Scholar] [CrossRef]
- Shaw, L.M. Tumor Cell Invasion Assays. Cell Migration 2004, 294, 97–106. [Google Scholar] [CrossRef]
- Wang, Y.; Bai, W.-K.; Shen, E.; Hu, B. Sonoporation by low-frequency and low-power ultrasound enhances chemotherapeutic efficacy in prostate cancer cells in vitro. Oncol. Lett. 2013, 6, 495–498. [Google Scholar] [CrossRef]
- Zhu, L.; Altman, M.B.; Laszlo, A.; Straube, W.; Zoberi, I.; Hallahan, D.E.; Chen, H. Ultrasound Hyperthermia Technology for Radiosensitization. Ultrasound Med. Biol. 2019, 45, 1025–1043. [Google Scholar] [CrossRef]
- Dalecki, D. Mechanical Bioeffects of Ultrasound. Annu. Rev. Biomed. Eng. 2004, 6, 229–248. [Google Scholar] [CrossRef] [PubMed]
- Ali, E.A.; Bordacahar, B.; Mestas, J.-L.; Batteux, F.; Lafon, C.; Camus, M.; Prat, F. Ultrasonic cavitation induces necrosis and impairs growth in three-dimensional models of pancreatic ductal adenocarcinoma. PLoS ONE 2018, 13, e0209094. [Google Scholar] [CrossRef]
- Bani, D.; Li, A.Q.; Freschi, G.; Russo, G.L. Histological and Ultrastructural Effects of Ultrasound-induced Cavitation on Human Skin Adipose Tissue. Plast. Reconstr. Surg. Glob. Open 2013, 1, e41. [Google Scholar] [CrossRef] [PubMed]
- Paliwal, S.; Mitragotri, S. Ultrasound-induced cavitation: Applications in drug and gene delivery. Expert Opin. Drug Deliv. 2006, 3, 713–726. [Google Scholar] [CrossRef] [PubMed]
- Kutty, S.; Liu, N.; Zhou, J.; Xiao, Y.; Wu, J.; Danford, D.A.; Lof, J.; Xie, F.; Porter, T.R. Ultrasound-Induced Microbubble Cavitation for the Treatment of Catheterization-Induced Vasospasm. JACC Basic Transl. Sci. 2017, 2, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Ter Haar, G. Heat and sound: Focused ultrasound in the clinic. Int. J. Hyperth. 2015, 31, 223–224. [Google Scholar] [CrossRef] [PubMed]
- Koulakis, J.P.; Rouch, J.; Huynh, N.; Dubrovsky, G.; Dunn, J.C.; Putterman, S. Interstitial Matrix Prevents Therapeutic Ultrasound From Causing Inertial Cavitation in Tumescent Subcutaneous Tissue. Ultrasound Med. Biol. 2018, 44, 177–186. [Google Scholar] [CrossRef]
- Coussios, C.C.; Farny, C.H.; Ter Haar, G.; Roy, R. Role of acoustic cavitation in the delivery and monitoring of cancer treatment by high-intensity focused ultrasound (HIFU). Int. J. Hyperth. 2007, 23, 105–120. [Google Scholar] [CrossRef]
- Yoshizawa, S.; Ikeda, T.; Ito, A.; Ota, R.; Takagi, S.; Matsumoto, Y. High intensity focused ultrasound lithotripsy with cavitating microbubbles. Med. Biol. Eng. Comput. 2009, 47, 851–860. [Google Scholar] [CrossRef]
- Snipstad, S.; Sulheim, E.; Davies, C.D.L.; Moonen, C.; Storm, G.; Kiessling, F.; Schmid, R.; Lammers, T. Sonopermeation to improve drug delivery to tumors: From fundamental understanding to clinical translation. Expert Opin. Drug Deliv. 2018, 15, 1249–1261. [Google Scholar] [CrossRef]
- Lipsman, N.; Meng, Y.; Bethune, A.J.; Huang, Y.; Lam, B.; Masellis, M.; Herrmann, N.; Heyn, C.; Aubert, I.; Boutet, A.; et al. Blood–brain barrier opening in Alzheimer’s disease using MR-guided focused ultrasound. Nat. Commun. 2018, 9, 1–8. [Google Scholar] [CrossRef]
- Hwang, J.H.; Tu, J.; Brayman, A.A.; Matula, T.J.; Crum, L.A. Correlation between inertial cavitation dose and endothelial cell damage in vivo. Ultrasound Med. Biol. 2006, 32, 1611–1619. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.W.; Everbach, E.C.; Cox, C.; Knapp, R.R.; A Brayman, A.; A Sherman, T. A comparison of the hemolytic potential of Optison and Albunex in whole human blood in vitro: Acoustic pressure, ultrasound frequency, donor and passive cavitation detection considerations. Ultrasound Med. Biol. 2001, 27, 709–721. [Google Scholar] [CrossRef]
- Wu, S.-Y.; Tung, Y.-S.; Marquet, F.; Downs, M.E.; Sanchez, C.S.; Chen, C.C.; Ferrera, V.; Konofagou, E. Transcranial cavitation detection in primates during blood-brain barrier opening-a performance assessment study. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2014, 61, 966–978. [Google Scholar] [CrossRef] [PubMed]
- Brüningk, S.; Rivens, I.; Mouratidis, P.; Ter Haar, G. Focused Ultrasound-Mediated Hyperthermia in Vitro: An Experimental Arrangement for Treating Cells under Tissue-Mimicking Conditions. Ultrasound Med. Biol. 2019, 45, 3290–3297. [Google Scholar] [CrossRef]
- Robertson, J.; Becker, S. Influence of Acoustic Reflection on the Inertial Cavitation Dose in a Franz Diffusion Cell. Ultrasound Med. Biol. 2018, 44, 1100–1109. [Google Scholar] [CrossRef] [PubMed]
- Tempel, N.V.D.; Laffeber, C.; Odijk, H.; Van Cappellen, W.A.; Van Rhoon, G.C.; Franckena, M.; Kanaar, R. The effect of thermal dose on hyperthermia-mediated inhibition of DNA repair through homologous recombination. Oncotarget 2017, 8, 44593–44604. [Google Scholar] [CrossRef]
- Kwok, S.J.J.; El Kaffas, A.; Lai, P.; Al Mahrouki, A.; Lee, J.; Iradji, S.; Tran, W.T.; Giles, A.; Czarnota, G.J. Ultrasound-Mediated Microbubble Enhancement of Radiation Therapy Studied Using Three-Dimensional High-Frequency Power Doppler Ultrasound. Ultrasound Med. Biol. 2013, 39, 1983–1990. [Google Scholar] [CrossRef]
- Izadifar, Z.; Babyn, P.; Chapman, D. Mechanical and Biological Effects of Ultrasound: A Review of Present Knowledge. Ultrasound Med. Biol. 2017, 43, 1085–1104. [Google Scholar] [CrossRef]
- Daecher, A.; Stanczak, M.; Liu, J.-B.; Zhang, J.; Du, S.; Forsberg, F.; Leeper, D.B.; Eisenbrey, J.R. Localized microbubble cavitation-based antivascular therapy for improving HCC treatment response to radiotherapy. Cancer Lett. 2017, 411, 100–105. [Google Scholar] [CrossRef]
- Ganci, F.; Sacconi, A.; Manciocco, V.; Spriano, G.; Fontemaggi, G.; Carlini, P.; Blandino, G. Radioresistance in Head and Neck Squamous Cell Carcinoma — Possible Molecular Markers for Local Recurrence and New Putative Therapeutic Strategies. Contemp. Issues Head Neck Cancer Manag. 2015, 37, 763–770. [Google Scholar] [CrossRef]
- Toraya-Brown, S.; Fiering, S.N. Local tumour hyperthermia as immunotherapy for metastatic cancer. Int. J. Hyperth. 2014, 30, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.A.; Wu, S.-K.; Li, Z.; Goertz, D.E.; Hynynen, K. Microbubble-assisted MRI-guided focused ultrasound for hyperthermia at reduced power levels. Int. J. Hyperth. 2018, 35, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Nofiele, J.I.T.; Karshafian, R.; Furukawa, M.; Al Mahrouki, A.; Giles, A.; Wong, C.S.; Czarnota, G.J. Ultrasound-Activated Microbubble Cancer Therapy: Ceramide Production Leading to Enhanced Radiation Effect in vitro. Technol. Cancer Res. Treat. 2013, 12, 53–60. [Google Scholar] [CrossRef]
- Ray, S.; Kassan, A.; Busija, A.R.; Rangamani, P.; Patel, H.H. The plasma membrane as a capacitor for energy and metabolism. Am. J. Physiol. Physiol. 2016, 310, C181–C192. [Google Scholar] [CrossRef]
- Van Wamel, A.; Kooiman, K.; Harteveld, M.; Emmer, M.; Cate, F.J.T.; Versluis, M.; De Jong, N. Vibrating microbubbles poking individual cells: Drug transfer into cells via sonoporation. J. Control. Release 2006, 112, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Kumon, R.E.; Cui, J.; Deng, C.X. The Size of Sonoporation Pores on the Cell Membrane. Ultrasound Med. Biol. 2009, 35, 1756–1760. [Google Scholar] [CrossRef]
- Miller, D.L.; Dou, C. Induction of Apoptosis in Sonoporation and Ultrasonic Gene Transfer. Ultrasound Med. Biol. 2009, 35, 144–154. [Google Scholar] [CrossRef]
- Zhong, W.; Sit, W.H.; Wan, J.M.; Yu, A.C. Sonoporation Induces Apoptosis and Cell Cycle Arrest in Human Promyelocytic Leukemia Cells. Ultrasound Med. Biol. 2011, 37, 2149–2159. [Google Scholar] [CrossRef]
- Yang, F.; Gu, N.; Chen, D.; Xi, X.; Zhang, D.; Li, Y.; Wu, J. Experimental study on cell self-sealing during sonoporation. J. Control. Release 2008, 131, 205–210. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, S.; Zhang, X.; Unger, M.; Patties, I.; Melzer, A.; Landgraf, L. Focused Ultrasound-Induced Cavitation Sensitizes Cancer Cells to Radiation Therapy and Hyperthermia. Cells 2020, 9, 2595. https://doi.org/10.3390/cells9122595
Hu S, Zhang X, Unger M, Patties I, Melzer A, Landgraf L. Focused Ultrasound-Induced Cavitation Sensitizes Cancer Cells to Radiation Therapy and Hyperthermia. Cells. 2020; 9(12):2595. https://doi.org/10.3390/cells9122595
Chicago/Turabian StyleHu, Shaonan, Xinrui Zhang, Michael Unger, Ina Patties, Andreas Melzer, and Lisa Landgraf. 2020. "Focused Ultrasound-Induced Cavitation Sensitizes Cancer Cells to Radiation Therapy and Hyperthermia" Cells 9, no. 12: 2595. https://doi.org/10.3390/cells9122595
APA StyleHu, S., Zhang, X., Unger, M., Patties, I., Melzer, A., & Landgraf, L. (2020). Focused Ultrasound-Induced Cavitation Sensitizes Cancer Cells to Radiation Therapy and Hyperthermia. Cells, 9(12), 2595. https://doi.org/10.3390/cells9122595