Compliance with Good Manufacturing Practice in the Assessment of Immunomodulation Potential of Clinical Grade Multipotent Mesenchymal Stromal Cells Derived from Wharton’s Jelly


Abstract
1. Introduction
2. Materials and Methods
2.1. Source Tissue, MSC Derivation, and Expansion
2.2. Flow Cytometry
2.3. Lymphocyte Proliferation Assays
2.4. Karyotype
2.5. Risk Analysis
2.5.1. Risk Assessment
2.5.2. Risk Control
2.5.3. Graphical Representation
2.6. Microbiological Testing
2.7. Endotoxin, Mycoplasm and Adventitious Virus Tests
2.8. Statistical Analysis
3. Results
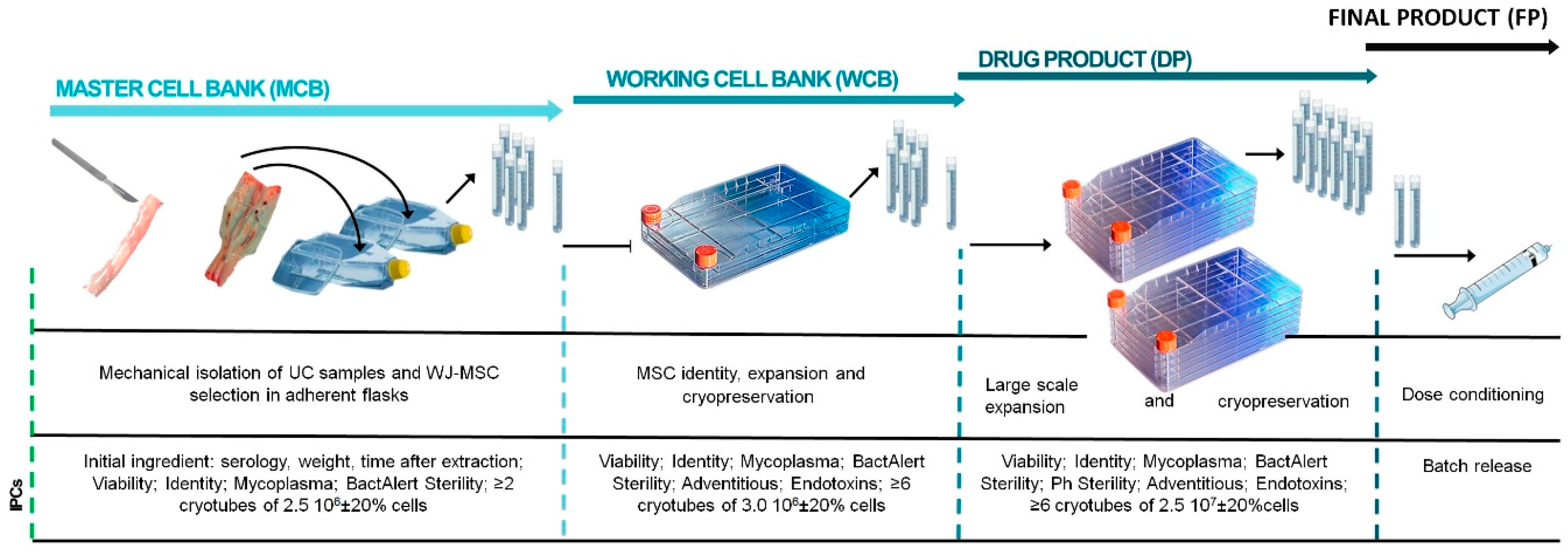
3.1. Bioprocess Design
3.1.1. Master Cell Bank (MCB)
3.1.2. Working Cell Bank (WCB)
3.1.3. Drug Product (DP)
3.1.4. Final Product (FP)
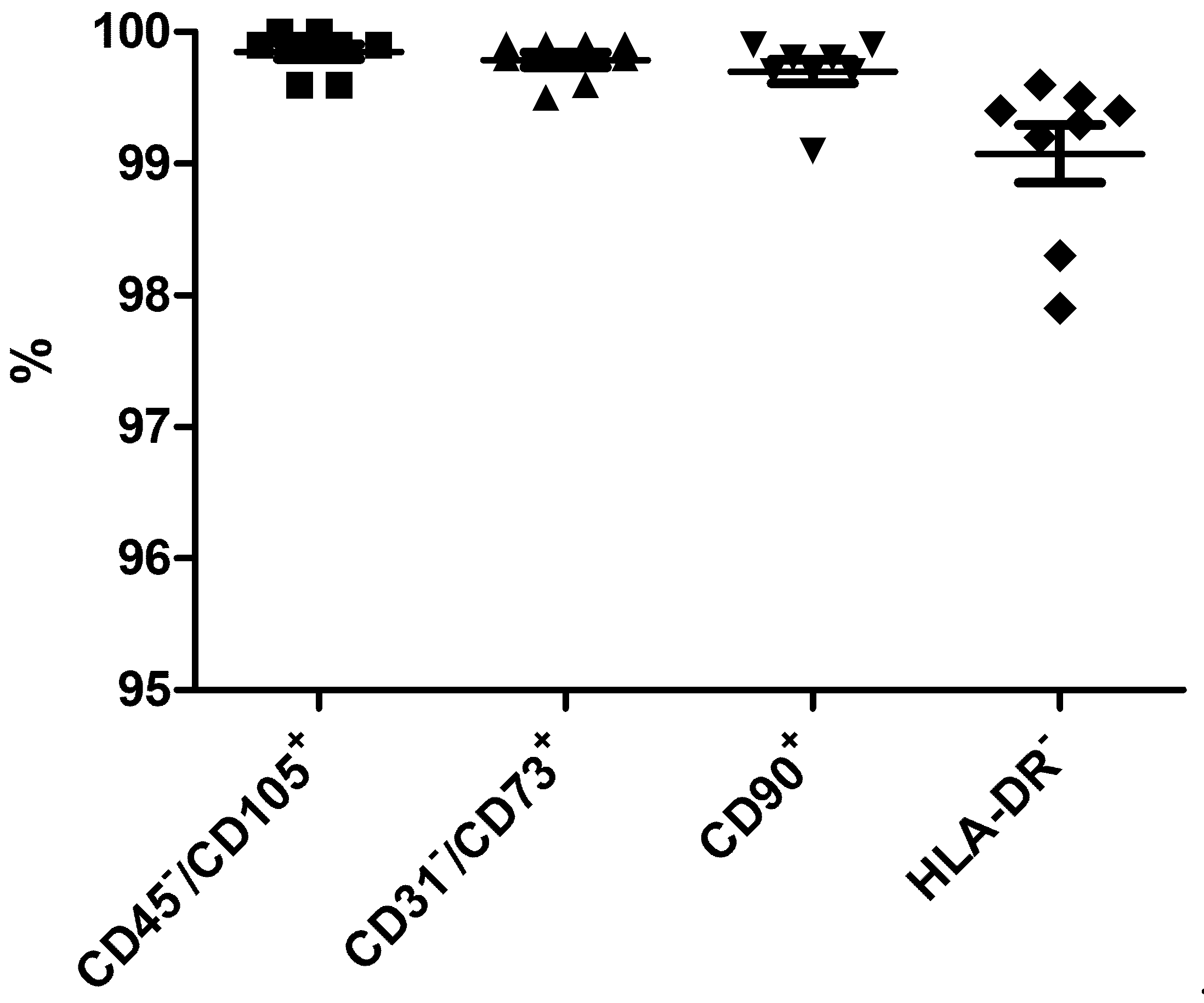
3.2. Identity of WJ-MSCs
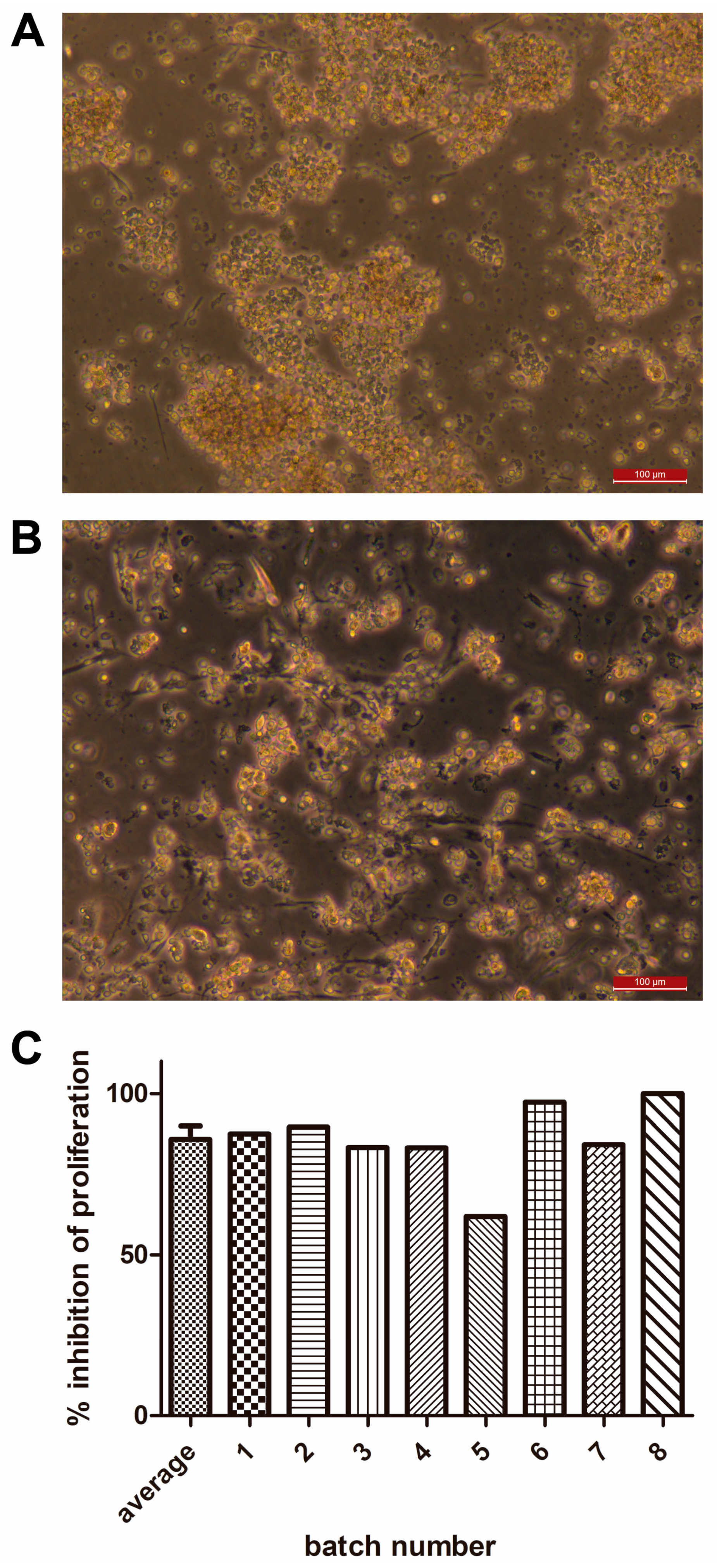
3.3. Potency of WJ-MSCs
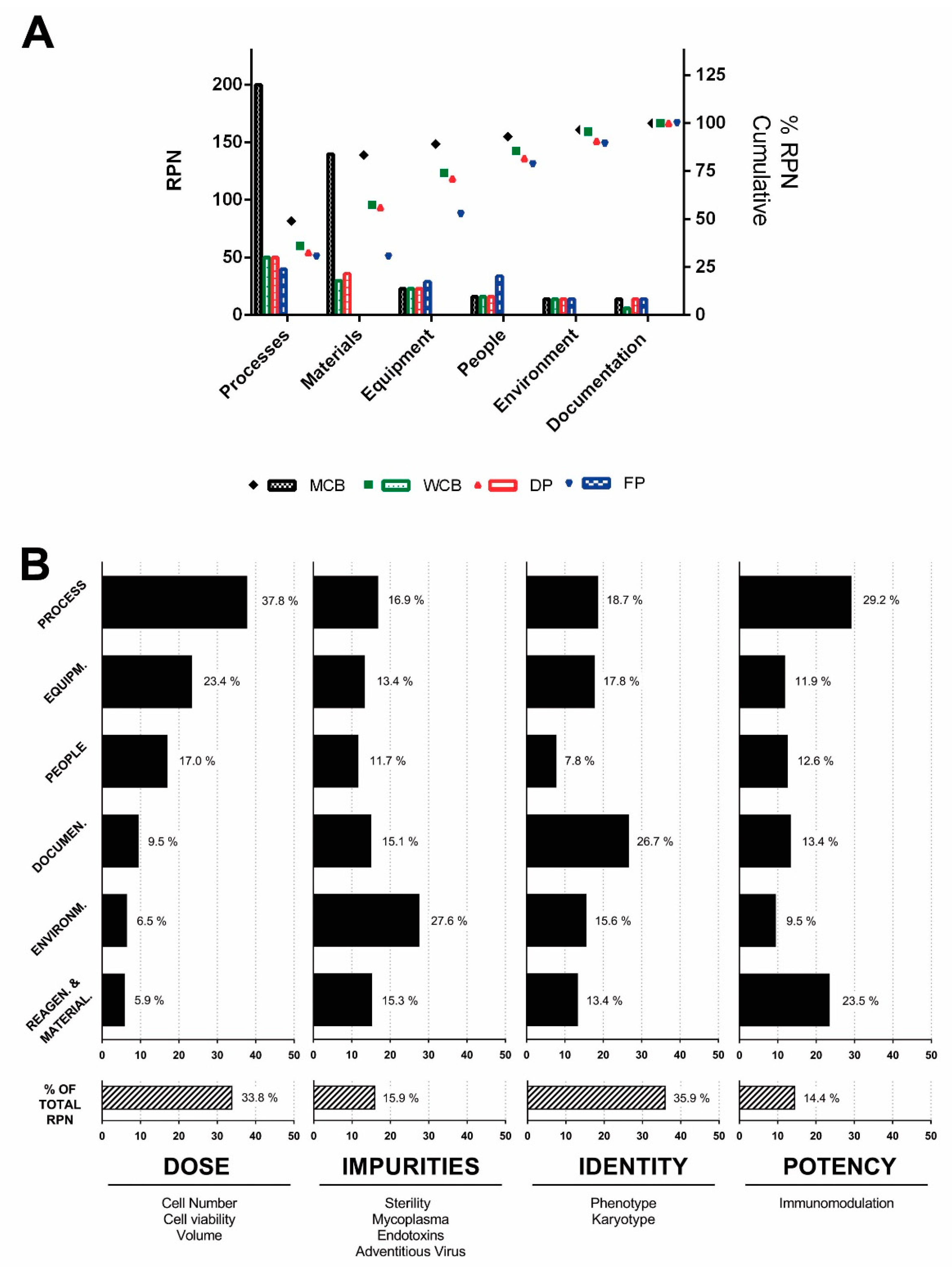
3.4. Risk Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guadix, J.A.; Zugaza, J.L.; Gálvez-Martín, P. Characteristics, applications and prospects of mesenchymal stem cells in cell therapy. Med. Clín. (Barc) 2017, 148, 408–414. [Google Scholar] [CrossRef]
- Vives, J.; Mirabel, C. Multipotent Mesenchymal Stromal Cells From Bone Marrow for Current and Potential Clinical Applications. In Reference Module in Biomedical Sciences; Elsevier BV: Amsterdam, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Cuende, N.; Rasko, J.E.; Koh, M.B.; Dominici, M.; Ikonomou, L. Cell, tissue and gene products with marketing authorization in 2018 worldwide. Cytotherapy 2018, 20, 1401–1413. [Google Scholar] [CrossRef]
- Lalu, M.M.; Mazzarello, S.; Zlepnig, J.; Dong, Y.Y.R.; Montroy, J.; McIntyre, L.; Devereaux, P.J.; Stewart, D.J.; David Mazer, C.; Barron, C.C.; et al. Safety and Efficacy of Adult Stem Cell Therapy for Acute Myocardial Infarction and Ischemic Heart Failure (SafeCell Heart): A Systematic Review and Meta-Analysis. Stem Cells Transl. Med. 2018, 7, 857–866. [Google Scholar] [CrossRef]
- Bianco, P.; Cao, X.; Frenette, P.S.; Mao, J.J.; Robey, P.G.; Simmons, P.J.; Wang, C.-Y. The meaning, the sense and the significance: translating the science of mesenchymal stem cells into medicine. Nat. Med. 2013, 19, 35–42. [Google Scholar] [CrossRef]
- Nombela-Arrieta, C.; Ritz, J.; Silberstein, L.E. The elusive nature and function of mesenchymal stem cells. Nat. Rev. Mol. Cell Boil. 2011, 12, 126–131. [Google Scholar] [CrossRef]
- Galipeau, J.; Sensébé, L. Mesenchymal Stromal Cells: Clinical Challenges and Therapeutic Opportunities. Cell Stem Cell 2018, 22, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Galipeau, J.; Krampera, M.; Barrett, J.; Dazzi, F.; Deans, R.J.; DeBruijn, J.; Dominici, M.; Fibbe, W.E.; Gee, A.P.; Gimble, J.M.; et al. International Society for Cellular Therapy perspective on immune functional assays for mesenchymal stromal cells as potency release criterion for advanced phase clinical trials. Cytotherapy 2016, 18, 151–159. [Google Scholar] [CrossRef]
- Del Mazo-Barbara, A.; Nieto, V.; Mirabel, C.; Reyes, B.; García-López, J.; Oliver-Vila, I.; Vives, J. Streamlining the qualification of computerized systems in GxP-compliant academic cell therapy facilities. Cytotherapy 2016, 18, 1237–1239. [Google Scholar] [CrossRef]
- Oliver-Vila, I.; Coca, M.I.; Grau-Vorster, M.; Pujals-Fonts, N.; Caminal, M.; Casamayor-Genescà, A.; Ortega, I.; Reales, L.; Pla, A.; Blanco, M.; et al. Evaluation of a cell-banking strategy for the production of clinical grade mesenchymal stromal cells from Wharton’s jelly. Cytotherapy 2016, 18, 25–35. [Google Scholar] [CrossRef]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Oliver-Vila, I.; Ramírez-Moncayo, C.; Grau-Vorster, M.; Marín-Gallén, S.; Caminal, M.; Vives, J. Optimisation of a potency assay for the assessment of immunomodulative potential of clinical grade multipotent mesenchymal stromal cells. Cytotechnology 2018, 70, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Codinach, M.; Blanco, M.; Ortega, I.; Lloret, M.; Reales, L.; Coca, M.I.; Torrents, S.; Doral, M.; Oliver-Vila, I.; Requena-Montero, M.; et al. Design and validation of a consistent and reproducible manufacture process for the production of clinical-grade bone marrow–derived multipotent mesenchymal stromal cells. Cytotherapy 2016, 18, 1197–1208. [Google Scholar] [CrossRef] [PubMed]
- Mirabel, C.; Nieto, V.; Reyes, B.; García-López, J.; Oliver-Vila, I.; Del Mazo-Barbara, A.; Vives, J. Qualification of computerized monitoring systems in a cell therapy facility compliant with the good manufacturing practices. Regen. Med. 2016, 11, 521–528. [Google Scholar]
- Mirabel, C.; Puente-Massaguer, E.; Del Mazo-Barbara, A.; Reyes, B.; Morton, P.; Gòdia, F.; Vives, J. Stability enhancement of clinical grade multipotent mesenchymal stromal cell-based products. J. Transl. Med. 2018, 16, 291. [Google Scholar] [CrossRef]
- Marquez-Curtis, L.A.; Janowska-Wieczorek, A.; McGann, L.E.; Elliott, J.A. Mesenchymal stromal cells derived from various tissues: Biological, clinical and cryopreservation aspects. Cryobiology 2015, 71, 181–197. [Google Scholar] [CrossRef] [PubMed]
- El Omar, R.; Beroud, J.; Stoltz, J.-F.; Menu, P.; Velot, E.; Decot, V. Umbilical Cord Mesenchymal Stem Cells: The New Gold Standard for Mesenchymal Stem Cell-Based Therapies? Tissue Eng. Part B Rev. 2014, 20, 523–544. [Google Scholar] [CrossRef] [PubMed]
- Thirumala, S.; Goebel, W.S.; Woods, E.J. Clinical grade adult stem cell banking. Organogenesis 2009, 5, 143–154. [Google Scholar] [CrossRef]
- Mattar, P.; Bieback, K. Comparing the Immunomodulatory Properties of Bone Marrow, Adipose Tissue, and Birth-Associated Tissue Mesenchymal Stromal Cells. Front. Immunol. 2015, 6, 1418. [Google Scholar] [CrossRef]
- Anzalone, R.; Lo Iacono, M.; Loria, T.; Di Stefano, A.; Giannuzzi, P.; Farina, F.; La Rocca, G. Wharton’s jelly mesenchymal stem cells as candidates for beta cells regeneration: extending the differentiative and immunomodulatory benefits of adult mesenchymal stem cells for the treatment of type 1 diabetes. Stem Cell Rev. 2011, 7, 342–363. [Google Scholar] [CrossRef]
- Rilo, H.L.; Cagliani, J.; Grande, D.; Molmenti, E.P.; Miller, E.J. Immunomodulation by Mesenchymal Stromal Cells and Their Clinical Applications. J. Stem Cell Regen. Boil. 2017, 3, 1–14. [Google Scholar] [CrossRef]
- Grégoire, C.; Ritacco, C.; Hannon, M.; Seidel, L.; Delens, L.; Belle, L.; Dubois, S.; Vériter, S.; Lechanteur, C.; Briquet, A.; et al. Comparison of Mesenchymal Stromal Cells From Different Origins for the Treatment of Graft-vs.-Host-Disease in a Humanized Mouse Model. Front Immunol. 2019, 10, 619. [Google Scholar] [CrossRef]
- Sensebé, L.; Bourin, P.; Tarte, K. Good Manufacturing Practices Production of Mesenchymal Stem/Stromal Cells. Hum. Gene Ther. 2011, 22, 19–26. [Google Scholar] [CrossRef]
- Bieback, K.; Kuçi, S.; Schäfer, R. Production and quality testing of multipotent mesenchymal stromal cell therapeutics for clinical use. Transfusion 2019. [Google Scholar] [CrossRef]
- Bravery, C.A.; Carmen, J.; Fong, T.; Oprea, W.; Hoogendoorn, K.H.; Woda, J.; Burger, S.R.; Rowley, J.A.; Bonyhadi, M.L.; Hof, W.V. Potency assay development for cellular therapy products: an ISCT∗ review of the requirements and experiences in the industry. Cytotherapy 2013, 15, 9–19.e9. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Requirement | Informative |
|---|---|---|
| Maternal Blood | Negative for: HBsAb, HIV I/II, syphilis (TPPA), Chagas, HBcAb, HCV, anti-HTLV I/II, NAT (HCV-HIV, HBV), anti-Toxo IgM, anti-EBV VCA IgM, anti-CMV IgM | Anti-Toxo IgG, anti- EBV VCA IgG, anti-CMV IgG |
| Cord Blood | HBsAb, HIV I/II, syphilis (TPPA), Chagas, HBcAb, HCV, anti-HTLV I/II, NAT (HCV-HIV, HBV) | N/A |
| Umbilical Cord Fragment | ≥7 g, ≤ 80 h from birth | N/A |
| Critical Quality Attribute | Value |
|---|---|
| Dose | 1 × 107 ± 20% |
| Viability | ≥70% |
| Phenotype | CD45-/CD105+ ≥ 95% |
| CD31-/CD73+ ≥ 95% CD90+ ≥ 95% HLA-DR 1 | |
| Sterility | Sterile |
| Mycoplasma | Negative |
| Endotoxin | ≤1EU/mL |
| Adventitious Viruses | Negative |
| Immunomodulation | Positive |
| Critical Quality Attribute | Potential Failure Risk |
|---|---|
| Dose | Seeding density lower than the critical minimum |
| Cell viability lower than 70% | |
| Slow cell growth | |
| Cell loss along the manufacturing process (washing and concentration steps) | |
| Impurities | Contamination of the culture |
| Endotoxins out of range | |
| Positive result for virus adventitious | |
| Identity | Phenotype markers out of range |
| Karyotype alteration | |
| Potency | Failure in the immunomodulation test |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| Dose (×107) | 2.5 | 2.4 | 2.3 | 2.3 | 2.5 | 2.4 | 2.5 | 2.8 |
| Num. doses | 18 | 6 | 24 | 14 | 16 | 20 | 39 | 41 |
| Viability (%) | 97.3 | 94.4 | 95.9 | 98.2 | 97.1 | 97.1 | 97.1 | 97.6 |
| CD45−/CD105+ | 99.9 | 99.6 | 100 | 99.6 | 99.9 | 99.9 | 99.9 | 100 |
| CD31−/CD73+ | 99.9 | 99.5 | 99.8 | 99.6 | 99.8 | 99.9 | 99.9 | 99.9 |
| CD90+ | 99.8 | 99.1 | 99.9 | 99.7 | 99.9 | 99.7 | 99.8 | 99.7 |
| HLA-DR- | 99.4 | 98.3 | 99.2 | 97.9 | 99.4 | 99.3 | 99.6 | 99.5 |
| Karyotype | 46X, X | 46X, X | n.d. | 46X, Y | 46X, Y | 46X, Y | 46X, Y | 46X, Y |
| Sterility | - | - | - | - | - | - | - | - |
| Mycoplasma | - | - | - | - | - | - | - | - |
| Endotoxin | ≤1EU/mL | ≤1EU/mL | ≤1EU/mL | ≤1EU/mL | ≤1EU/mL | ≤1EU/mL | ≤1EU/mL | ≤1EU/mL |
| Adventitious viruses | - | - | - | - | - | - | - | - |
| Immunomodulation | 87.5 | 89.6 | 83.3 | 83.2 | 61.9 | 97.3 | 84.2 | 100 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grau-Vorster, M.; Rodríguez, L.; del Mazo-Barbara, A.; Mirabel, C.; Blanco, M.; Codinach, M.; Gómez, S.G.; Querol, S.; García-López, J.; Vives, J. Compliance with Good Manufacturing Practice in the Assessment of Immunomodulation Potential of Clinical Grade Multipotent Mesenchymal Stromal Cells Derived from Wharton’s Jelly. Cells 2019, 8, 484. https://doi.org/10.3390/cells8050484
Grau-Vorster M, Rodríguez L, del Mazo-Barbara A, Mirabel C, Blanco M, Codinach M, Gómez SG, Querol S, García-López J, Vives J. Compliance with Good Manufacturing Practice in the Assessment of Immunomodulation Potential of Clinical Grade Multipotent Mesenchymal Stromal Cells Derived from Wharton’s Jelly. Cells. 2019; 8(5):484. https://doi.org/10.3390/cells8050484
Chicago/Turabian StyleGrau-Vorster, Marta, Luciano Rodríguez, Anna del Mazo-Barbara, Clémentine Mirabel, Margarita Blanco, Margarita Codinach, Susana G. Gómez, Sergi Querol, Joan García-López, and Joaquim Vives. 2019. "Compliance with Good Manufacturing Practice in the Assessment of Immunomodulation Potential of Clinical Grade Multipotent Mesenchymal Stromal Cells Derived from Wharton’s Jelly" Cells 8, no. 5: 484. https://doi.org/10.3390/cells8050484
APA StyleGrau-Vorster, M., Rodríguez, L., del Mazo-Barbara, A., Mirabel, C., Blanco, M., Codinach, M., Gómez, S. G., Querol, S., García-López, J., & Vives, J. (2019). Compliance with Good Manufacturing Practice in the Assessment of Immunomodulation Potential of Clinical Grade Multipotent Mesenchymal Stromal Cells Derived from Wharton’s Jelly. Cells, 8(5), 484. https://doi.org/10.3390/cells8050484