CD271+ Human Mesenchymal Stem Cells Show Antiarrhythmic Effects in a Novel Murine Infarction Model

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Bone Marrow Aspiration
2.2. Cell Isolation
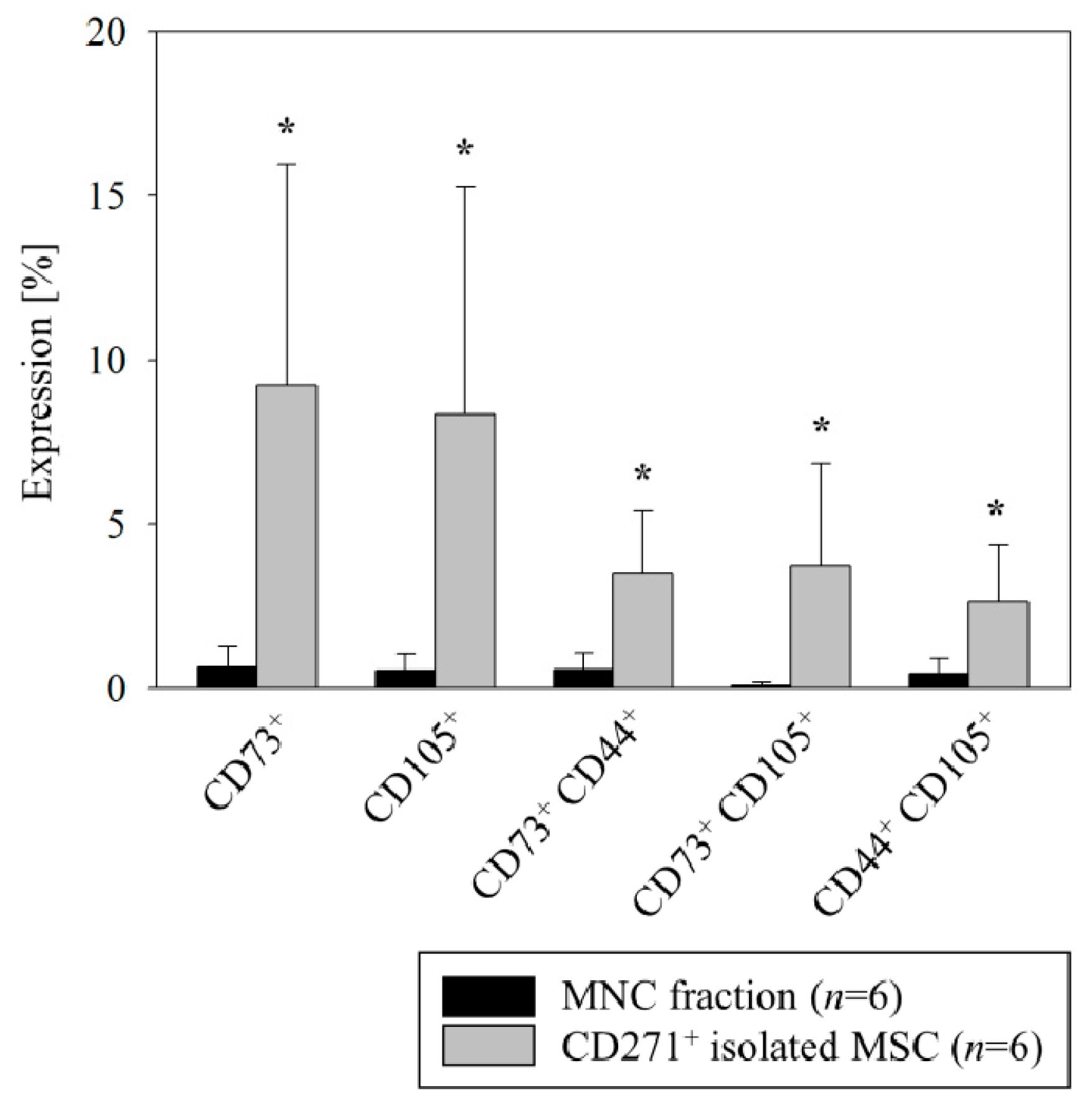
2.3. Flow Cytometric Analysis
2.4. Animals
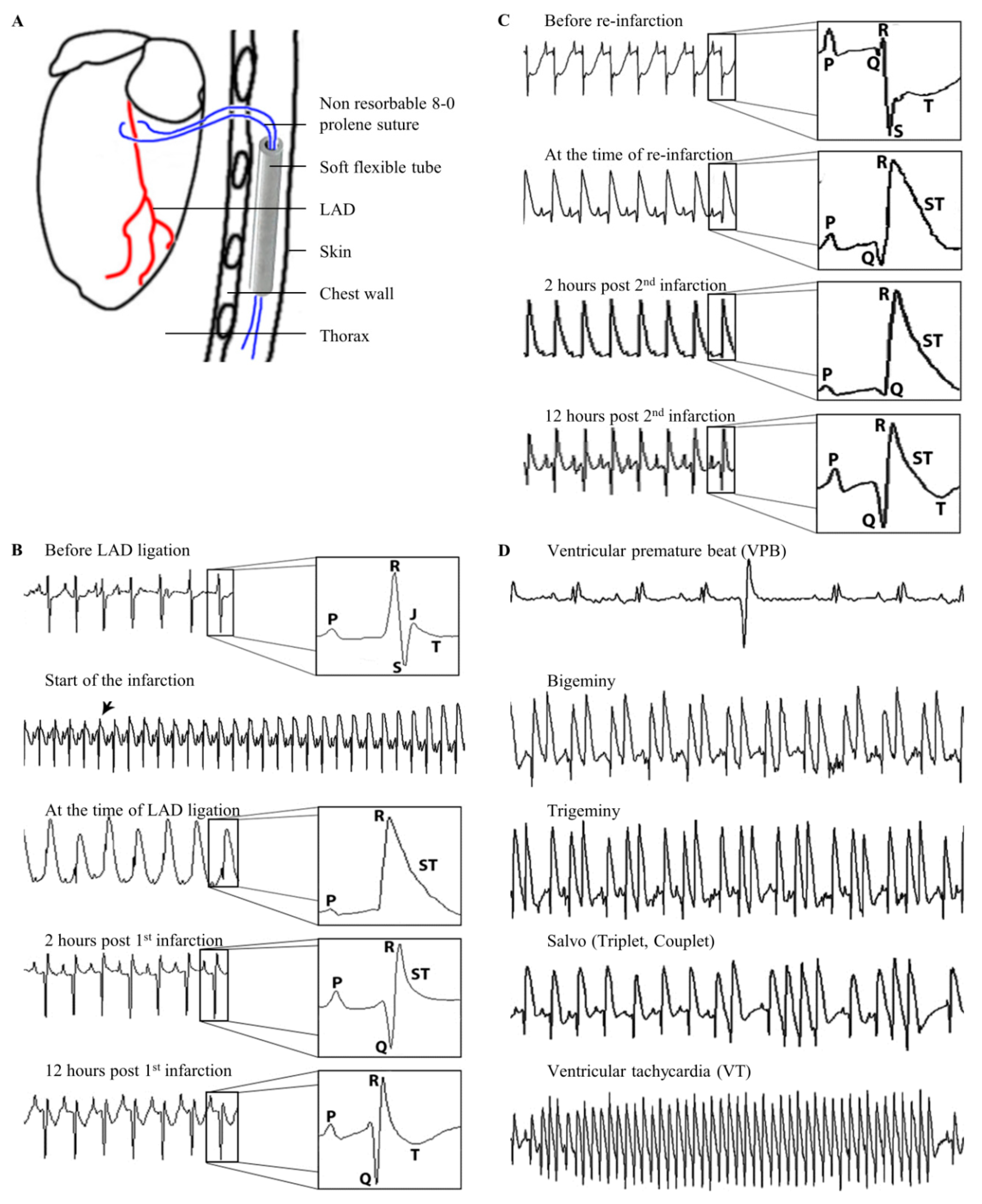
2.5. Ambulatory ECG Monitoring and Ligation of the Left Anterior Descending Artery
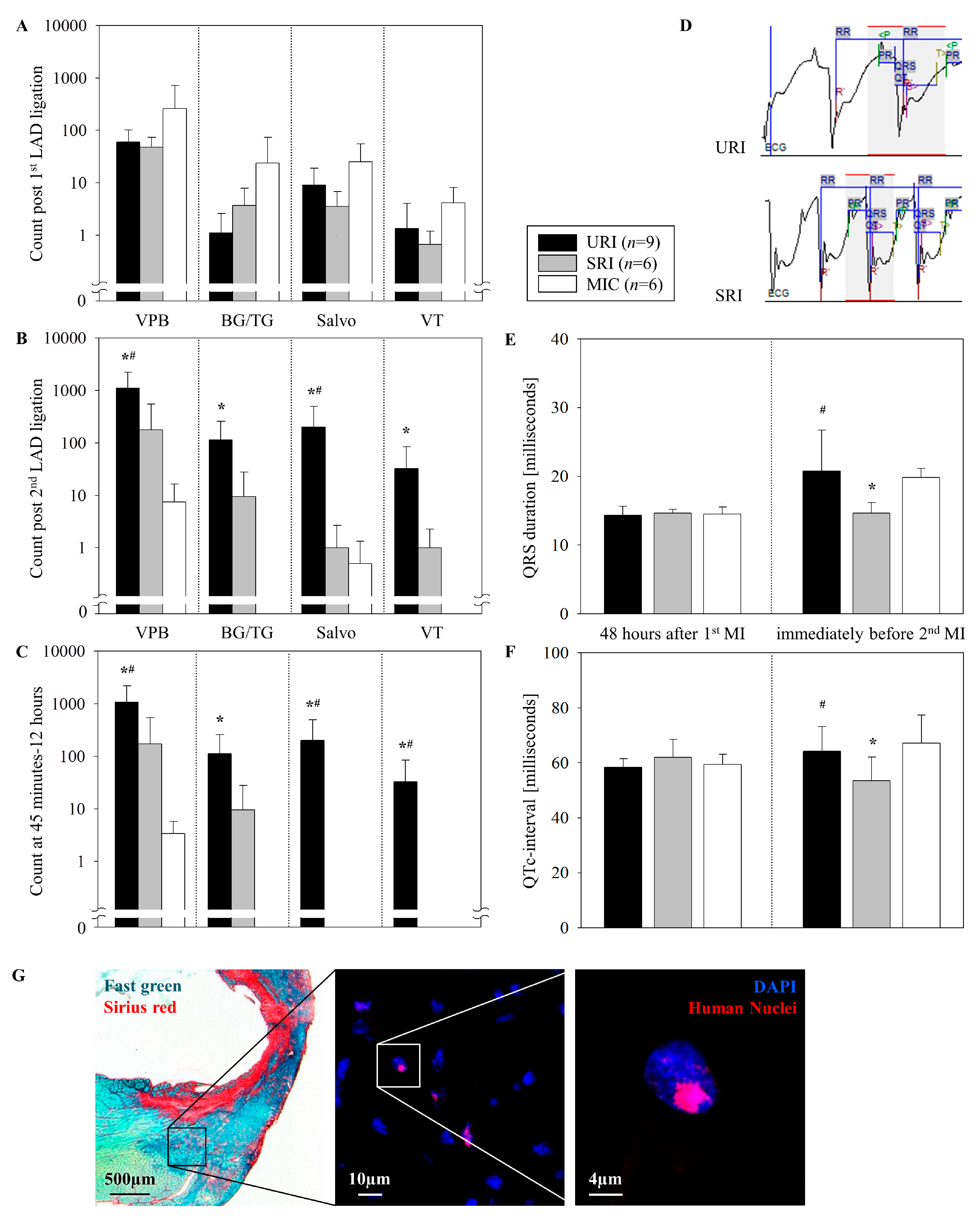
2.6. Basic ECG Parameters
2.7. Definitions of Various Ventricular Arrhythmias
2.7.1. Ventricular premature beats
2.7.2. Bigeminies and trigeminies
2.7.3. Salvos
2.7.4. Ventricular tachycardia
2.8. Organ Harvesting
2.9. Human Cells Detection
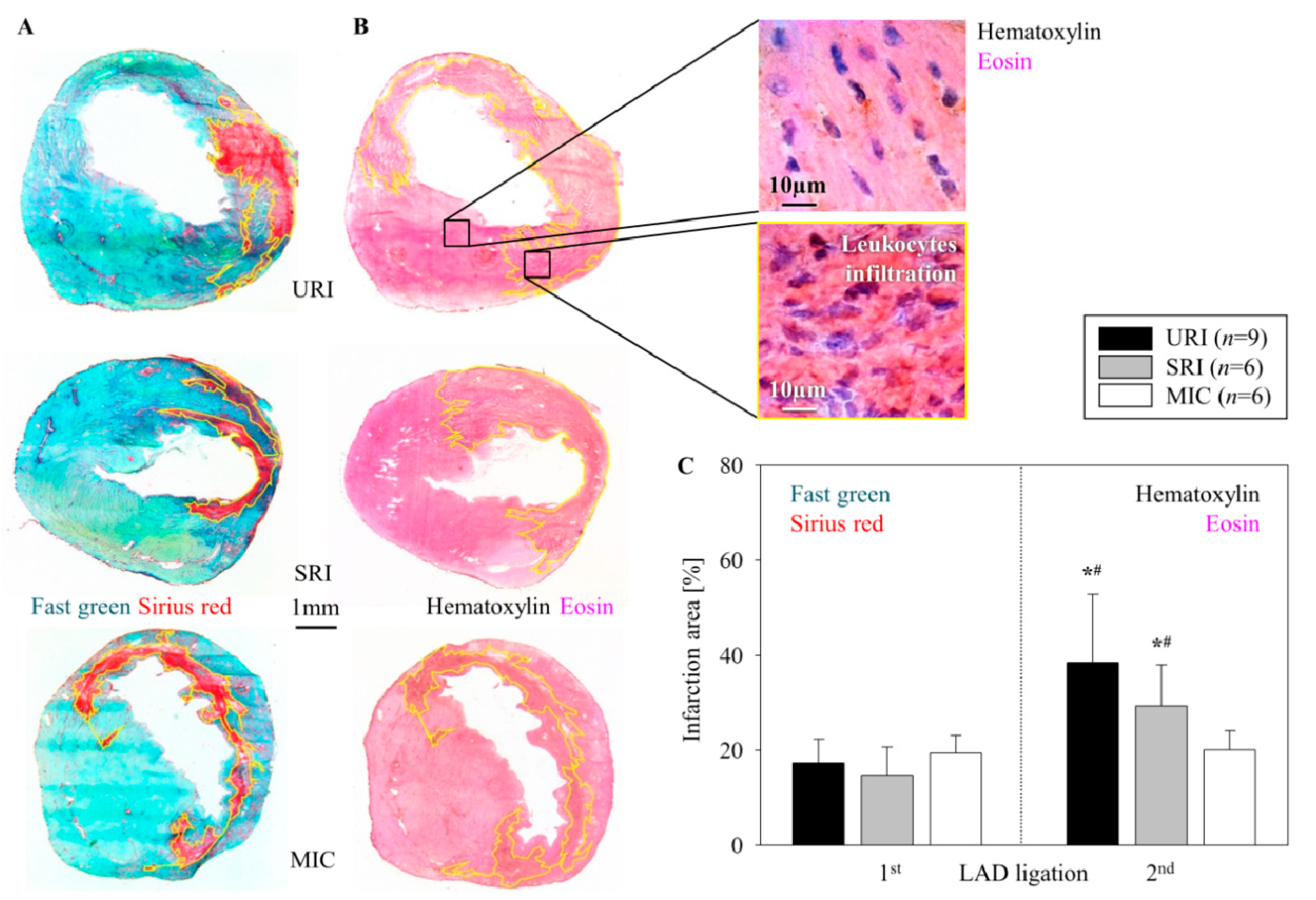
2.10. Infarction Size and Leukocytes Infiltration Area Analysis
2.11. Statistical Analysis
3. Results
3.1. Immunophenotypic Analysis of CD271+ Mesenchymal Stem Cells
3.2. Induced Ventricular Arrhythmias
3.3. Induction of Ventricular Arrhythmias after the Reinfarction
3.4. Antiarrhythmic Effects of CD271+ MSC Engraftment
3.5. Alterations of the Infarct Scar
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Herzstiftung eV D. 28. Deutscher Herzbericht. Deutsche Herzstiftung eV. 2016. Available online: www.herzstiftung.de/herzbericht (accessed on 18 August 2019).
- Smits, P.C.; van Geuns, R.J.M.; Poldermans, D.; Bountioukos, M.; Onderwater, E.E.M.; Lee, C.H.; Maat, A.P.W.M.; Serruys, P.W. Catheter-based intramyocardial injection of autologous skeletal myoblasts as a primary treatment of ischemic heart failure: Clinical experiencewith six-month follow-up. J. Am. Coll. Cardiol. 2003, 42, 2063–2069. [Google Scholar] [CrossRef] [PubMed]
- Hagège, A.A.; Marolleau, J.P.; Vilquin, J.T.; Alhéritière, A.; Peyrard, S.; Duboc, D.; Abergel, E.; Messas, E.; Mousseaux, E.; Schwartz, K.; et al. Skeletal myoblast transplantation in ischemic heart failure: Long-term follow-up of the first phase I cohort of patients. Circulation 2006, 114, 108–113. [Google Scholar] [CrossRef]
- Roell, W.; Lewalter, T.; Sasse, P.; Tallini, Y.N.; Choi, B.R.; Breitbach, M.; Doran, R.; Becher, U.M.; Hwang, S.-M.; Bostani, T.; et al. Engraftment of connexin 43-expressing cells prevents post-infarct arrhythmia. Nature 2007, 450, 819. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.J.; Chang, W.; Song, B.-W.; Song, H.; Cha, M.J.; Kim, I.K.; Lim, S.; Choi, E.J.; Ham, O.; Lee, S.Y.; et al. Antiarrhythmic potential of mesenchymal stem cell is modulated by hypoxic environment. J. Am. Coll. Cardiol. 2012, 60, 1698–1706. [Google Scholar] [CrossRef] [PubMed]
- Steinhoff, G.; Nesteruk, J.; Wolfien, M.; Kundt, G.; Börgermann, J.; David, R.; Garbade, J.; Große, J.; Haverich, A.; Hennig, H.; et al. Cardiac function improvement and bone marrow response outcome analysis of the randomized perfect phase III clinical trial of intramyocardial CD133+ application after myocardial infarction. EBioMedicine 2017, 22, 208–224. [Google Scholar] [CrossRef] [PubMed]
- Mueller, P.; Gaebel, R.; Lemcke, H.; Wiekhorst, F.; Hausburg, F.; Lang, C.; Zarniko, N.; Westphal, B.; Steinhoff, G.; David, R. Intramyocardial fate and effect of iron nanoparticles co-injected with MACS® purified stem cell products. Biomaterials 2017, 135, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Skorska, A.; Müller, P.; Gaebel, R.; Große, J.; Lemcke, H.; Lux, C.A.; Bastian, M.; Hausburg, F.; Zarniko, N.; Bubritzki, S.; et al. GMP-conform on-site manufacturing of a CD133+ stem cell product for cardiovascular regeneration. Stem Cell Res. Ther. 2017, 8, 33. [Google Scholar] [CrossRef]
- Gaebel, R.; Furlani, D.; Sorg, H.; Polchow, B.; Frank, J.; Bieback, K.; Wang, W.; Klopsch, C.; Ong, L.-L.; Li, W.; et al. Cell origin of human mesenchymal stem cells determines a different healing performance in cardiac regeneration. PLoS ONE 2011, 6, e15652. [Google Scholar] [CrossRef]
- Ludwig, M.; Skorska, A.; Tölk, A.; Hopp, H.-H.; Patejdl, R.; Li, J.; Steinhoff, G.; Noack, T. Characterization of ion currents of murine CD117+ stem cells in vitro and their modulation under AT2R stimulation. Acta Physiol. 2013, 208, 274–287. [Google Scholar] [CrossRef]
- Ludwig, M.; Tölk, A.; Skorska, A.; Maschmeier, C.; Gaebel, R.; Lux, C.A.; Steinhoff, G.; David, R. Exploiting AT2R to improve CD117 stem cell function in vitro and in vivo-perspectives for cardiac stem cell therapy. Cell Physiol. Biochem. 2015, 37, 77–93. [Google Scholar] [CrossRef]
- Song, J.; Willinger, T.; Rongvaux, A.; Eynon, E.E.; Stevens, S.; Manz, M.G.; Flavell, R.A.; Galán, J.E. A mouse model for the human pathogen Salmonella typhi. Cell Host Microbe 2010, 8, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.P.; Blundell, M.P.; Lopes, L.; Kinnon, C.; Di Santo, J.P.; Thrasher, A.J. Enhanced human cell engraftment in mice deficient in RAG2 and the common cytokine receptor gamma chain. Br. J. Haematol. 1998, 103, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Mazurier, F.; Fontanellas, A.; Salesse, S.; Taine, L.; Landriau, S.; Moreau-Gaudry, F.; Reiffers, J.; Peault, B.; Di Santo, J.P.; De Verneuil, H. A novel immunodeficient mouse model--RAG2 x common cytokine receptor gamma chain double mutants-requiring exogenous cytokine administration for human hematopoietic stem cell engraftment. J. Interf. Cytokine Res. 1999, 19, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Berul, C.I.; Aronovitz, M.J.; Wang, P.J.; Mendelsohn, M.E. In vivo cardiacelectrophysiology studies in the mouse. Circulation 1996, 94, 2641–2648. [Google Scholar] [CrossRef] [PubMed]
- Hagendorff, A.; Schumacher, B.; Kirchhoff, S.; Lüderitz, B.; Willecke, K. Conductiondisturbances and increased atrialvulnerability in connexin40-deficientmice analysed by transoesophageal stimulation. Circulation 1999, 99, 1508–1515. [Google Scholar] [CrossRef]
- Lemcke, H.; Gaebel, R.; Skorska, A.; Voronina, N.; Lux, C.A.; Petters, J.; Sasse, S.; Zarniko, N.; Steinhoff, G.; David, R. Mechanisms of stem cell based cardiac repair-gap junctional signaling promotes the cardiac lineage specifcation of mesenchymal stem cells. Sci. Rep. 2017, 7, 9755. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Jeron, A.; Koren, G. Measurement of heart rate and Q-T interval in the con-scious mouse. Am. J. Physiol. 1998, 274, 747–751. [Google Scholar] [CrossRef]
- Curtis, M.J.; Hancox, J.C.; Farkas, A.; Wainwright, C.L.; Stables, C.L.; Saint, D.A.; Clements-Jeweryg, H.; Lambiaseh, P.D.; Billmani, G.E.; Janse, M.J.; et al. The Lambeth Conventions (II): Guidelines for the study of animal and human ventricular and supraVA. Pharmacol. Ther. 2013, 139, 213–248. [Google Scholar] [CrossRef]
- Walker, M.J.A.; Curtis, M.J.; Hearse, D.J.; Campbell, R.W.F.; Janse, M.J.; Yellon, D.M.; Cobbe, S.M.; Coker, S.J.; Harness, J.B.; Harron, D.W.G.; et al. The Lambeth Conventions: Guidelines for the study of arrhythmias in ischaemia, infarction, and reperfusion. Cardiovasc. Res. 1988, 22, 447–455. [Google Scholar] [CrossRef]
- Zipes, D.P.; Camm, A.J.; Borggrefe, M.; Buxton, A.E.; Chaitman, B.; Fromer, M. ACC/AHA/ESC 2006 guidelines for management of patients with VA and the prevention of sudden cardiac death–executive summary. Eur. Heart J. 2006, 27, 2099–2140. [Google Scholar] [CrossRef]
- Fiedler, V.B. Reduction of myocardial infarction and dysrhythmic activity by nafazatrom in the conscious rat. Eur. J. Pharmacol. 1983, 88, 263–267. [Google Scholar] [CrossRef]
- Quirici, N.; Soligo, D.; Bossolasco, P.; Servida, F.; Lumini, C.; Deliliers, G.L. Isolation of bone marrow mesenchymal stem cells by anti-nerve growth factor receptor antibodies. Exp. Hematol. 2002, 30, 783–791. [Google Scholar] [CrossRef]
- Wit, A.L.; Peters, N.S. The role of gap junctions in the arrhythmias of ischemia and infarction. Heart Rhythm 2012, 9, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Lujan, H.L.; DiCarlo, S.E. Reperfusion-induced sustained ventricular tachycardia, leading to ventricular fibrillation, in chronically instrumented, intact, conscious mice. Physiol. Rep. 2014, 2, e12057. [Google Scholar] [CrossRef][Green Version]
- Leprán, I.; Koltai, M.; Siegmund, W.; Szekeres, L. Coronary artery ligation, early arrhythmias, and determination of the ischemic area in conscious rats. J. Pharmacol. Methods 1983, 9, 219–230. [Google Scholar] [CrossRef]
- Betsuyaku, T.; Kanno, S.; Lerner, D.L.; Schuessler, R.B.; Saffitz, J.E.; Yamada, K.A. Spontaneous and inducible ventricular arrhythmias after myocardial infarction in mice. Cardiovasc. Pathol. 2004, 13, 156–164. [Google Scholar] [CrossRef]
- Boink, G.J.J.; Lu, J.; Driessen, H.E.; Duan, L.; Sosunov, E.A.; Anyukhovsky, E.P.; Shlapakova, I.N.; Lau, D.H.; Rosen, T.S.; Danilo, P.; et al. Effect of skeletal muscle Na+ channel delivered via a cell platform on cardiac conduction and arrhythmia induction. Circ. Arrhyth. Electrophysiol. 2012, 5, 831–840. [Google Scholar] [CrossRef]
- Hare, J.M.; Traverse, J.H.; Henry, T.D.; Dib, N.; Strumpf, R.K.; Schulman, S.P.; Gerstenblith, G.; De Maria, A.N.; Denktas, A.E.; Gammon, R.S.; et al. A Randomized, Double-Blind, Placebo-Controlled, Dose-Escalation Study of Intravenous Adult Human Mesenchymal Stem Cells (Prochymal) After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2009, 54, 2277–2286. [Google Scholar] [CrossRef]
- Bhar-Amato, J.; Davies, W.; Agarwal, S. Ventricular Arrhythmia after Acute Myocardial Infarc-tion: ‘The Perfect Storm’. Arrhyth. Electrophysiol. Rev. 2017, 6, 134–139. [Google Scholar] [CrossRef]
- Yang, F.; Liu, Y.H.; Yang, X.P.; Xu, J.; Kapke, A.; Carretero, O.A. Myocardial Infarction and Cardiac Remodelling in Mice. Exp. Physiol. 2002, 87, 547–555. [Google Scholar] [CrossRef]
- Beeres, S.L.; Zeppenfeld, K.; Bax, J.J.; Dibbets-Schneider, P.; Stokkel, M.P.; Fibbe, W.E.; van der Wall, E.E.; Atsma, D.E.; Schalij, M.J. Electrophysiological and arrhythmogenic effects of intramyocardial bone marrow cell injection in patients with chronic ischemic heart disease. Heart Rhythm 2007, 4, 257–265. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First LAD Ligation (Mean ± SD) | Second LAD Ligation (Mean ± SD) | |||||
|---|---|---|---|---|---|---|
| URI (n = 9) | SRI (n = 6) | MIC (n = 6) | URI (n = 9) | SRI (n = 6) | MIC (n = 6) | |
| VPB | ||||||
| 0–12 h | 60.1 ± 42.19 | 47.5 ± 25.8 | 259.0 ± 457.69 | 1105.0 ± 1146.72 | 178.16 ± 370.12 | 7.5 ± 8.98 |
| 0–15 min | 1.8 ± 4.25 | 2.0 ± 3.63 | 7.5 ± 14.08 | 7.1 ± 7.97 | 4.0 ± 4.04 | 0.3 ± 0.81 |
| 15–45 min | 3.6 ± 4.30 | 3.0 ± 4.69 | 4.6 ± 5.57 | 15.6 ± 22.75 | 0.33 ± 0.51 | 3.8 ± 7.22 |
| 45 min–12 h | 54.5 ± 39.85 | 42.5 ± 27.38 | 246.8 ± 440.84 | 1082.2 ± 1127.77 | 173.8 ± 371.56 | 3.3 ± 2.42 |
| BG/TG | ||||||
| 0–12 h | 1.1 ± 1.45 | 3.66 ± 4.17 | 23.6 ± 49.35 | 113.8 ± 146.02 | 9.5 ± 18.41 | 0 ± 0 |
| 0–15 min | 0 ± 0 | 0.16 ± 0.40 | 1.3 ± 3.26 | 0.5 ± 0.72 | 0 ± 0 | 0 ± 0 |
| 15–45 min | 0.1 ± 0.33 | 0.16 ± 0.40 | 0.6 ± 1.21 | 0.6 ± 1.65 | 0 ± 0 | 0 ± 0 |
| 45 min–12 h | 1.0 ± 1.50 | 3.33 ± 4.32 | 21.6 ± 45.89 | 112.6 ± 144.78 | 9.5 ± 18.41 | 0 ± 0 |
| Salvos | ||||||
| 0–12 h | 9.0 ± 9.89 | 3.5 ± 3.27 | 25.3 ± 29.96 | 201.7 ± 296.77 | 1.0 ± 1.67 | 0.5 ± 0.83 |
| 0–15 min | 0 ± 0 | 1.16 ± 1.83 | 1.0 ± 1.54 | 0.3 ± 0.50 | 1.0 ± 1.67 | 0 ± 0 |
| 15–45 min | 0.5 ± 0.88 | 0.5 ± 0.54 | 12.1 ± 0.64 | 0 ± 0 | 0 ± 0 | 0.5 ± 0.83 |
| 45 min–12 h | 8.4 ± 10.17 | 1.83 ± 2.56 | 12.1 ± 18.17 | 201.4 ± 296.89 | 0 ± 0 | 0 ± 0 |
| VT | ||||||
| 0–12 h | 1.3 ± 2.69 | 0.66 ± 0.51 | 4.1 ±3.97 | 32.6 ± 52.51 | 1.0 ± 1.26 | 0 ± 0 |
| 0–15 min | 0.5 ± 0.83 | 0.16 ± 0.40 | 0 ± 0 | 0 ± 0 | 0.83 ± 1.16 | 0 ± 0 |
| 15–45 min | 0.3 ± 1.00 | 0.16 ± 0.40 | 2.0 ± 4.42 | 0 ± 0 | 0.16 ± 0.40 | 0 ± 0 |
| 45 min–12 h | 1.0 ± 2.64 | 0.33 ± 0.51 | 1.6 ±1.86 | 32.6 ± 52.51 | 0 ± 0 | 0 ± 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sadraddin, H.; Gaebel, R.; Skorska, A.; Lux, C.A.; Sasse, S.; Ahmad, B.; Vasudevan, P.; Steinhoff, G.; David, R. CD271+ Human Mesenchymal Stem Cells Show Antiarrhythmic Effects in a Novel Murine Infarction Model. Cells 2019, 8, 1474. https://doi.org/10.3390/cells8121474
Sadraddin H, Gaebel R, Skorska A, Lux CA, Sasse S, Ahmad B, Vasudevan P, Steinhoff G, David R. CD271+ Human Mesenchymal Stem Cells Show Antiarrhythmic Effects in a Novel Murine Infarction Model. Cells. 2019; 8(12):1474. https://doi.org/10.3390/cells8121474
Chicago/Turabian StyleSadraddin, Haval, Ralf Gaebel, Anna Skorska, Cornelia Aquilina Lux, Sarah Sasse, Beschan Ahmad, Praveen Vasudevan, Gustav Steinhoff, and Robert David. 2019. "CD271+ Human Mesenchymal Stem Cells Show Antiarrhythmic Effects in a Novel Murine Infarction Model" Cells 8, no. 12: 1474. https://doi.org/10.3390/cells8121474
APA StyleSadraddin, H., Gaebel, R., Skorska, A., Lux, C. A., Sasse, S., Ahmad, B., Vasudevan, P., Steinhoff, G., & David, R. (2019). CD271+ Human Mesenchymal Stem Cells Show Antiarrhythmic Effects in a Novel Murine Infarction Model. Cells, 8(12), 1474. https://doi.org/10.3390/cells8121474