
Strong Hsp90α/β Protein Expression in Advanced Primary CRC Indicates Short Survival and Predicts Response to the Hsp90α/β-Specific Inhibitor Pimitespib
Abstract

1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Tumor Sample Preparation
2.3. Immunohistochemistry and Evaluation of Biomarker Expression
2.4. Molecular Pathology
2.5. The Colorectal Patient-Derived Cancer Spheroid Model
2.6. Cell Line Culture
2.7. Cytospin Preparation
2.8. Treatment and Evaluation
2.9. Statistical Analysis
3. Results
3.1. Patient Characteristics and Survival
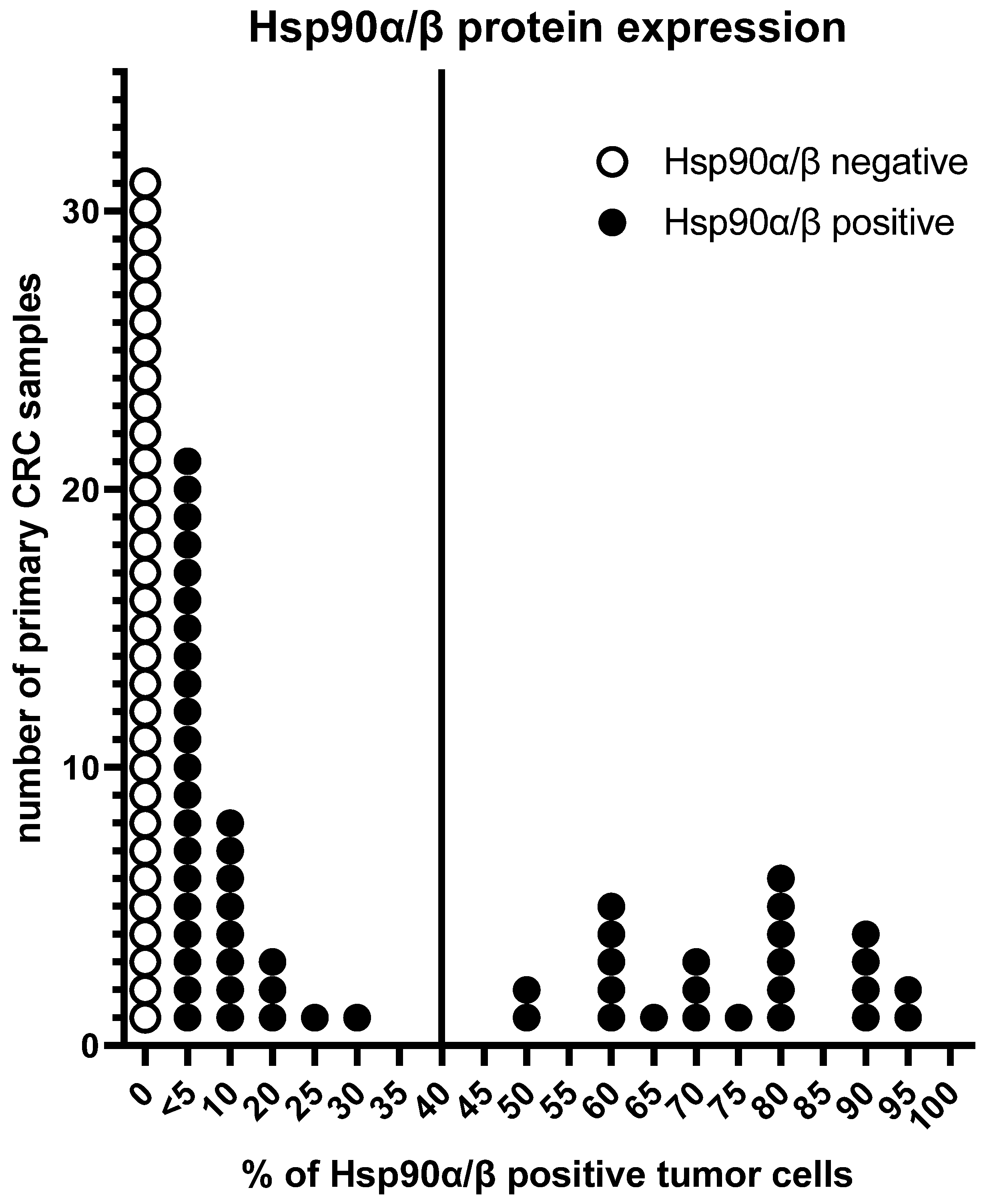
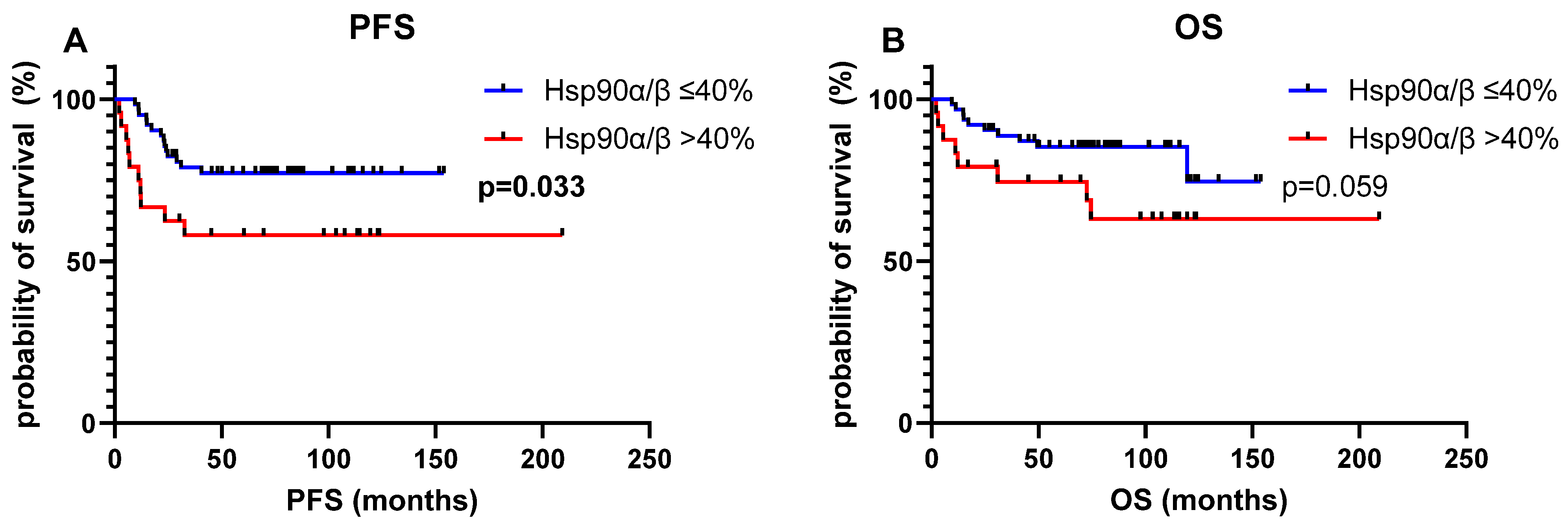
3.2. Hsp90α/β Protein Expression in Primary CRC and Survival
3.3. Colorectal Cancer Cell Line Characteristics
3.4. Hsp90 Inhibition in Primary Colorectal Cancer Cell Lines
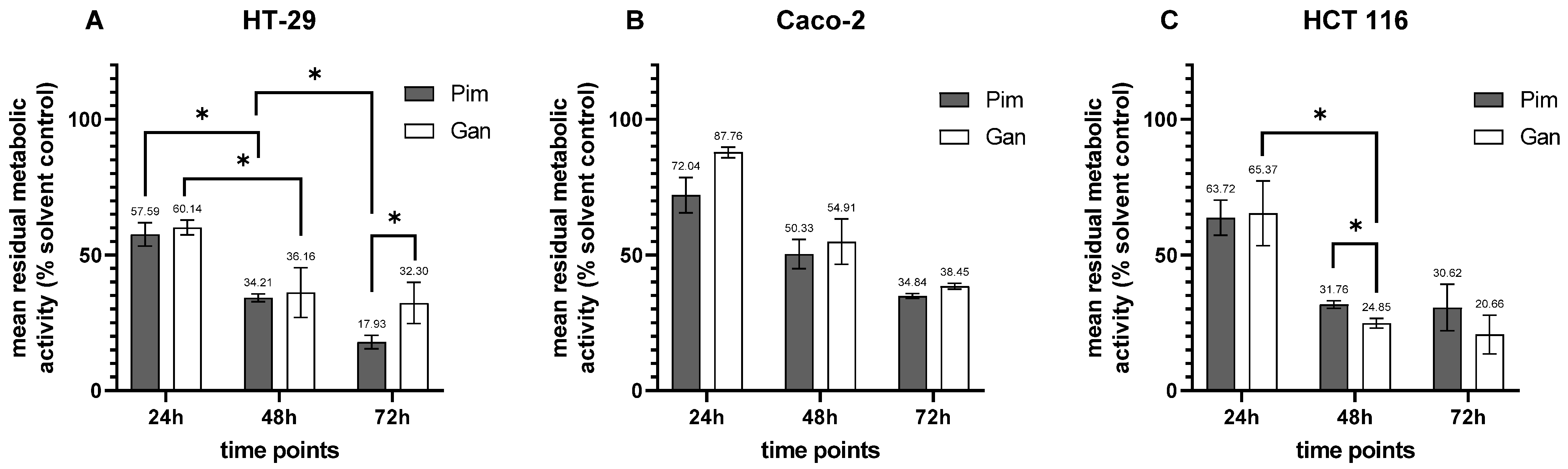
3.4.1. Hsp90 Inhibitors as Single Agents
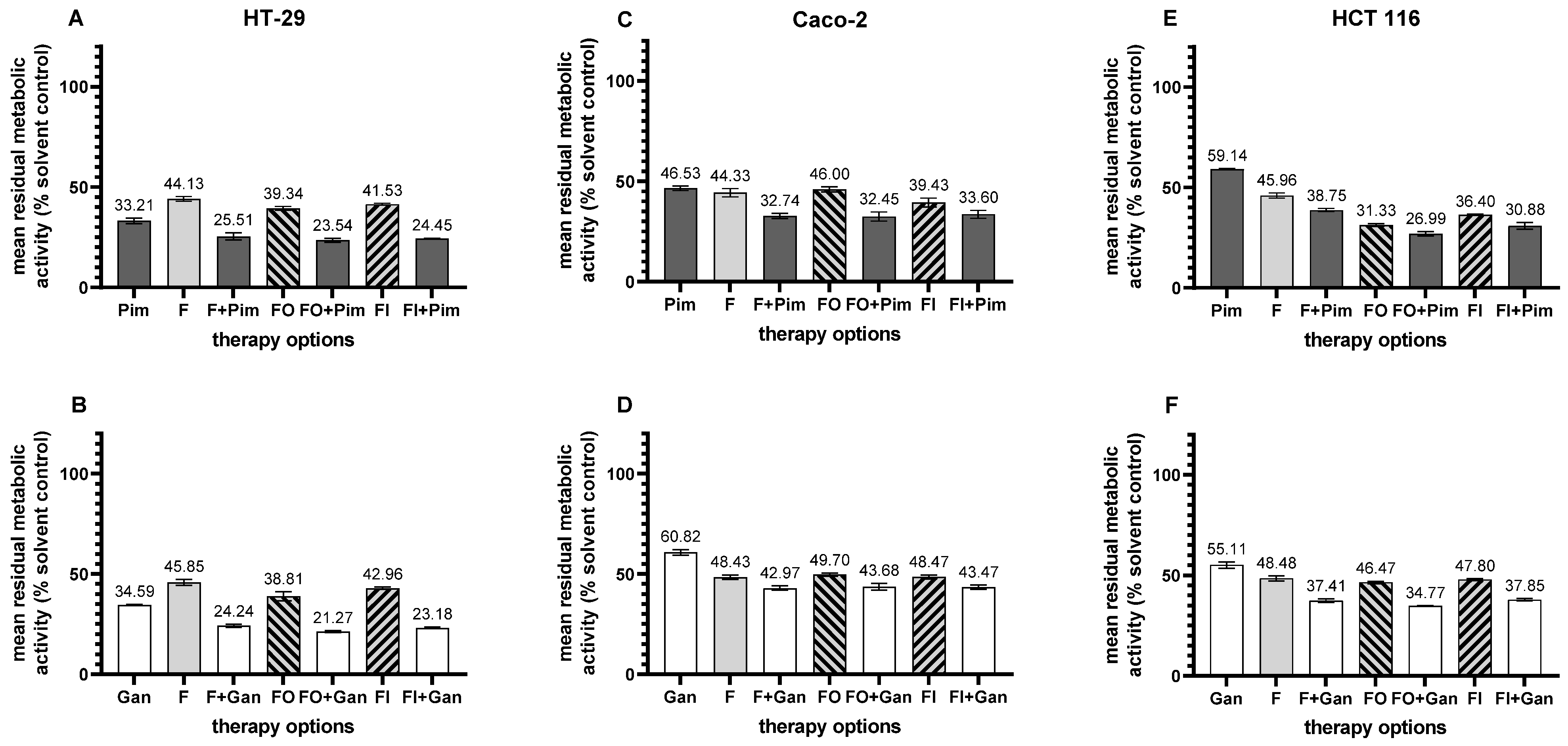
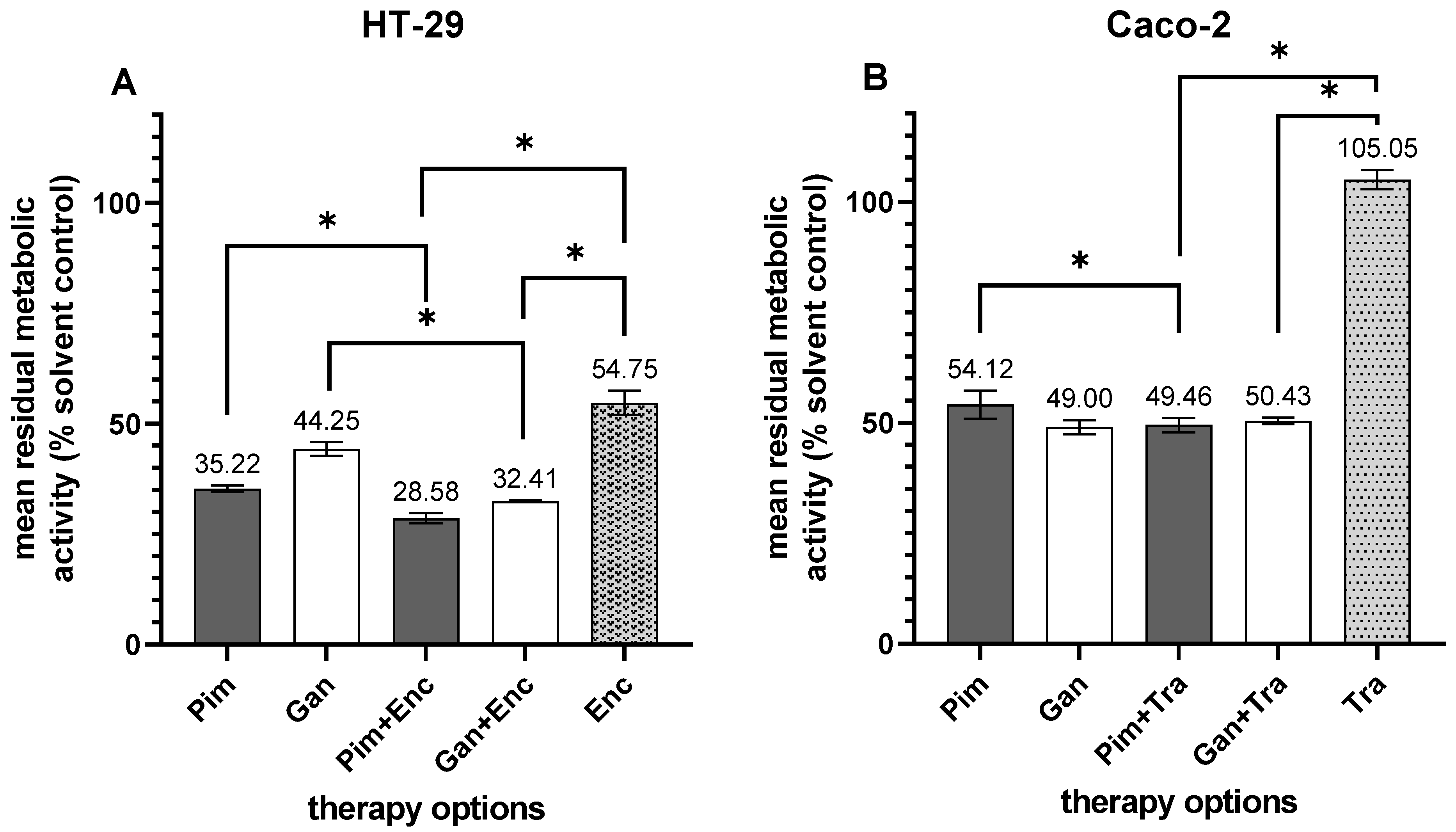
3.4.2. Hsp90 Inhibitors in Combination Therapy
3.5. Hsp90 Inhibition in the Colorectal Patient-Derived Cancer Spheroid Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Meaning |
| °C | degree Celsius |
| µm | micro-meters |
| 95% CI | 95% confidence interval |
| adeno-ca | adenocarcinoma |
| ADP | adenosine diphosphate |
| ATP | adenosine triphosphate |
| BRAF | B-Raf proto-oncogene |
| BRAF V600E | B-Raf proto-oncogene V600E mutation |
| Cat No | catalog number |
| cM | clinical metastasis stage |
| CRC | colorectal cancer |
| dMMR | deficient mismatch repair |
| DMSO | dimethyl sulfoxide |
| DNA | desoxyribonucleic acid |
| D-PBS | Dulbecco’s phosphate-buffered saline |
| EGF-R | epithelial growth factor receptor |
| Enc | encorafenib |
| EpCam | epithelial cell adhesion molecule |
| F; 5-FU | 5-fluorouracil |
| FCS | fetal cow serum |
| FDA | Food and Drug Administration |
| FI | 5-fluorouracil + Irinotecan |
| FO | 5-fluorouracil + oxaliplatin |
| Gan | ganetespib, STA-9090 |
| GIST | gastrointestinal stromal tumor |
| H&E | hematoxylin and eosin |
| HER2/neu | human epidermal growth factor receptor 2 |
| HR | hazard ratio |
| HRP | horseradish peroxidase |
| Hsp90 | heat shock protein 90 |
| Hsp90α/β | heat shock protein 90 alpha and beta isoform |
| HTCR | Human Tissue and Cell Research |
| ID | identification |
| KRAS | Kirsten rat sarcoma virus |
| L | lymphangiosis carcinomatosa |
| LMU | Ludwig Maximilians University |
| mab | monoclonal antibody |
| mRNA | messenger ribonucleic acid |
| MSI | microsatellite instability |
| mut | mutated |
| nc | non-computable |
| NSCLC | non-small-cell lung cancer |
| nt | non-treatable |
| NTRK | neurotropic tyrosinkinase |
| OS | overall survival |
| p | p-value |
| P | perineural invasion |
| PARP | poly-adenosine diphospate ribose polymerase |
| pCRC | primary colorectal cancer |
| PD-1 | programmed cell death protein 1 |
| PDAC | pancreatic ductal adenocarcinoma |
| PDCS | patient-derived cancer spheroid(s) |
| PD-L1 | programmed death-ligand 1 |
| PFS | progression-free survival |
| Pim | pimitespib; Tas-116 |
| pN | pathological lymph node stage |
| PPC | peak plasma concentration |
| pT | pathological tumor stage |
| R | resection status |
| SC | solvent control(s) |
| sCEA | soluble carcinoembryonic antigen |
| t | treatable |
| Tra | trastuzumab |
| UICC | Union Internationale Contre le Cancer |
| V | vessel invasion |
| wt | wild type |
| XRCC1 | X-ray repair cross complementing protein 1 |
Appendix A
Appendix A.1. Primary and Secondary Antibodies and the Detection Systems Used for Immunohistochemistry and Immunocytochemistry
| Antigen | Antibody Clone | Order Number | Host Species | Isotype | Working Concentration (µg/mL) | Kit | Supplier |
| primary antibodies | |||||||
| Hsp90α/β | AC88 | ab13492 | mouse | IgG1 | 10 | + | Abcam Cambridge, UK |
| Her2/neu | 4B5 | 05278368001 | rabbit | IgG | 1.5 | - | Roche basis supplier Basel, Switzerland |
| EpCam | BerEp4 | M080401-2 | mouse | IgG1 | 2.5 | - | Dako Jena, Germany |
| pan-cytokeratin | AE1/AE3 | NBP2-29429 | mouse | IgG1 | 0.5 | + | Novus Biological Centennial, CO, USA |
| MOPC-21 | MOPC-21 | MACF1081Z | mouse | IgG1 | 10 | + | Sigma-Aldrich, St. Louis, MO, USA |
| MOPC-21 | MOPC-21 | MACF1081Z | mouse | IgG1 | 2.5 | - | Sigma-Aldrich, St. Louis, MO, USA |
| DA1E | DA1E | 3900S | rabbit | IgG | 1.5 | - | CellSignaling, Danvers, MA, USA |
| secondary antibodies | |||||||
| rabbit anti-mouse | polyclonal | 315-065-045 | rabbit | IgG | 0.75 | Jackson ImmunoResearch, West Grove, PA, USA | |
| goat anti-rabbit | polyclonal | 111-065-144 | goat | IgG | 7 | Jackson ImmunoResearch | |
| detection systems | |||||||
| streptavidin–horseradish peroxidase | - | 016-030-084 | - | - | 1 | Jackson ImmunoResearch | |
| Zytochem Plus HRP Kit | polyclonal | HRP 060 | mouse, rabbit, rat | - | ready to use | Zytomed Systems GmbH, Berlin, Germany |
Appendix A.2. PCR and Sequencing Primers
| KRAS codon 12 + 13 a | forward | 5′-NNNGGCCTGCTGAAAATGACTGAA-3′ |
| reverse | 5′-Bio-TTAGCTGTATCGTCAAGGCACTCT-3′ | |
| sequencing | 5′-TGTGGTAGTTGGAGCT-3′ | |
| KRAS codon 12 + 13 b | forward | 5′-Bio-TGACTGAATATAAACTTGTGGTAGTTG-3′ |
| reverse | 5′-TCGTCCACAAAATGATTCTGA-3′ | |
| sequencing | 5′-GCACTCTTGCCTACG-3′ | |
| BRAF V600E | forward | 5′-TGAAGACCTCACAGTAAAAATAGG-3′ |
| reverse | 5′-Bio-TCCAGACAACTGTTCAAACTGAT-3′ | |
| sequencing | 5′-GTAAAAATAGGTGATTTTGG-3′ | |
| a sequencing according to Ogino [41]; b sequencing according to Poehlmann [42]. | ||
Appendix A.3. Drugs Used for Treatment
| Name of the Drug | Target | Peak Plasma Concentration (µg/mL) | Solvent Control | Supplier | Order Number | Ref. |
| pimitespib (Pim) | Hsp90α/β | 1.625 | DMSO | Selleckchem Cologne, Germany | S7716 | [34] |
| ganetespib (Gan) | pan-Hsp90 | 4.41 | DMSO | MedChem Express Monmouth Junction, NJ, USA | HY-15205 | [64,82] |
| encorafenib (Enc) | BRAF V600 mutation | 1.556 | DMSO | Selleckchem | S7108 | [83] |
| trastuzumab (Tra) | Her2/neu protein | 132.00 | water | Pharmacy, LMU Munich, Germany | not available | [84] |
| 5-fluorouracil (F) | 100.00 | water | Pharmacy, LMU | not available | [85] | |
| oxaliplatin (O) | 1.89 | water | Pharmacy, LMU | not available | [86] | |
| irinotecan (I) | 2.10 | water | Pharmacy, LMU | not available | [87] |
References
- Wiesmueller, F.; Schuetz, R.; Langheinrich, M.; Brunner, M.; Weber, G.F.; Grützmann, R.; Merkel, S.; Krautz, C. Defining early recurrence in patients with resected primary colorectal carcinoma and its respective risk factors. Int. J. Colorectal Dis. 2021, 36, 1181–1191. [Google Scholar] [CrossRef] [PubMed]
- Chuang, J.P.; Tsai, H.L.; Chen, P.J.; Chang, T.K.; Su, W.C.; Yeh, Y.S.; Huang, C.W.; Wang, J.Y. Comprehensive Review of Biomarkers for the Treatment of Locally Advanced Colon Cancer. Cells 2022, 11, 3744. [Google Scholar] [CrossRef]
- Leitlinienprogramm Onkologie (Deutsche Krbsgesellschaft, D.K., AWMF). S3-Leitlinie Kolorektales Krzinom, Langversion 2.1, AWMF. 2019. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/kolorektales-karzinom/ (accessed on 10 February 2025).
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- Cervantes, A.; Adam, R.; Roselló, S.; Arnold, D.; Normanno, N.; Taïeb, J.; Seligmann, J.; De Baere, T.; Osterlund, P.; Yoshino, T.; et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 10–32. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Guidelines. Colon Cancer Version 1.2025. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 10 February 2025).
- Underwood, P.W.; Pawlik, T.M. Precision Medicine for Metastatic Colorectal Cancer: Where Do We Stand? Cancers 2024, 16, 3870. [Google Scholar] [CrossRef]
- Diener, M.K.; Fichtner-Feigl, S. Biomarkers in colorectal liver metastases: Rising complexity and unknown clinical significance? Ann. Gastroenterol. Surg. 2021, 5, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.; Baumgart, J.; Roth, W.; Moehler, M.; Kloth, M. Cancer gene related characterization of patterns and point of recurrence after resection of colorectal liver metastases. Ann. Transl. Med. 2021, 9, 1372. [Google Scholar] [CrossRef]
- Richter, M.; Sonnow, L.; Mehdizadeh-Shrifi, A.; Richter, A.; Koch, R.; Zipprich, A. German oncology certification system for colorectal cancer—Relative survival rates of a single certified centre vs. national and international registry data. Innov. Surg. Sci. 2021, 6, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, Y.; Honma, Y.; Sawaki, A.; Naito, Y.; Iwagami, S.; Komatsu, Y.; Takahashi, T.; Nishida, T.; Doi, T. Pimitespib in patients with advanced gastrointestinal stromal tumor (CHAPTER-GIST-301): A randomized, double-blind, placebo-controlled phase III trial. Ann. Oncol. 2022, 33, 959–967. [Google Scholar] [CrossRef]
- Naoki, K.; Igawa, S.; Uojima, H.; Tsumura, H.; Sengoku, N.; Karayama, M.; Shimomura, A.; Ohtake, T.; Shio, Y.; Hosokawa, A.; et al. Cardiovascular safety of pimitespib in patients with advanced solid tumors: An open-label, nonrandomized, phase 1 study. Cancer 2024, 130, 3745–3756. [Google Scholar] [CrossRef]
- Rastogi, S.; Joshi, A.; Sato, N.; Lee, S.; Lee, M.J.; Trepel, J.B.; Neckers, L. An update on the status of HSP90 inhibitors in cancer clinical trials. Cell Stress Chaperones 2024, 29, 519–539. [Google Scholar] [CrossRef] [PubMed]
- Hoter, A.; El-Sabban, M.E.; Naim, H.Y. The HSP90 Family: Structure, Regulation, Function, and Implications in Health and Disease. Int. J. Mol. Sci. 2018, 19, 2560. [Google Scholar] [CrossRef] [PubMed]
- Maiti, S.; Picard, D. Cytosolic Hsp90 Isoform-Specific Functions and Clinical Significance. Biomolecules 2022, 12, 1166. [Google Scholar] [CrossRef] [PubMed]
- Picard, D. Hsp90 Interactors. Available online: https://www.picard.ch/downloads/Hsp90interactors.pdf (accessed on 12 February 2025).
- Birbo, B.; Madu, E.E.; Madu, C.O.; Jain, A.; Lu, Y. Role of HSP90 in Cancer. Int. J. Mol. Sci. 2021, 22, 10317. [Google Scholar] [CrossRef]
- Miyata, Y.; Nakamoto, H.; Neckers, L. The therapeutic target Hsp90 and cancer hallmarks. Curr. Pharm. Des. 2013, 19, 347–365. [Google Scholar] [CrossRef]
- Rappa, F.; Sciume, C.; Lo Bello, M.; Bavisotto, C.C.; Marino Gammazza, A.; Barone, R.; Campanella, C.; David, S.; Carini, F.; Zarcone, F.; et al. Comparative analysis of Hsp10 and Hsp90 expression in healthy mucosa and adenocarcinoma of the large bowel. Anticancer Res. 2014, 34, 4153–4159. [Google Scholar]
- Zhang, S.; Guo, S.; Li, Z.; Li, D.; Zhan, Q. High expression of HSP90 is associated with poor prognosis in patients with colorectal cancer. PeerJ 2019, 7, e7946. [Google Scholar] [CrossRef]
- Milicevic, Z.; Bogojevic, D.; Mihailovic, M.; Petrovic, M.; Krivokapic, Z. Molecular characterization of hsp90 isoforms in colorectal cancer cells and its association with tumour progression. Int. J. Oncol. 2008, 32, 1169–1178. [Google Scholar]
- Javid, H.; Hashemian, P.; Yazdani, S.; Sharbaf Mashhad, A.; Karimi-Shahri, M. The role of heat shock proteins in metastatic colorectal cancer: A review. J. Cell. Biochem. 2022, 123, 1704–1735. [Google Scholar] [CrossRef]
- Kim, K.; Lee, H.W.; Lee, E.H.; Park, M.I.; Lee, J.S.; Kim, M.S.; Kim, K.; Roh, M.S.; Pak, M.G.; Oh, J.E.; et al. Differential expression of HSP90 isoforms and their correlations with clinicopathologic factors in patients with colorectal cancer. Int. J. Clin. Exp. Pathol. 2019, 12, 978–986. [Google Scholar]
- Doi, T.; Yamamoto, N.; Ohkubo, S. Pimitespib for the treatment of advanced gastrointestinal stromal tumors and other tumors. Future Oncol. 2024, 20, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Kryeziu, K.; Bruun, J.; Guren, T.K.; Sveen, A.; Lothe, R.A. Combination therapies with HSP90 inhibitors against colorectal cancer. Biochim. Biophys. Acta Rev. Cancer 2019, 1871, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Balibrea, E.; Martínez-Cardús, A.; Ginés, A.; Ruiz de Porras, V.; Moutinho, C.; Layos, L.; Manzano, J.L.; Bugés, C.; Bystrup, S.; Esteller, M.; et al. Tumor-Related Molecular Mechanisms of Oxaliplatin Resistance. Mol. Cancer Ther. 2015, 14, 1767–1776. [Google Scholar] [CrossRef]
- Trials.gov. A Study of Pimitespib in Combination with Imatinib in Patients with GIST (CHAPTER-GIST-101). Available online: https://clinicaltrials.gov/study/NCT05245968?intr=TAS-116&rank=4 (accessed on 12 February 2025).
- Clinicaltrials.gov. AB122 Platform Study. Available online: https://clinicaltrials.gov/study/NCT04999761 (accessed on 12 February 2025).
- jRCT. Phase 2 platform Study Evaluating Combination Therapy with TAS-116 (Pimitespib) in Patients with Malignant Tumors (CHAPTER-Platform-201). Available online: https://jrct.mhlw.go.jp/en-latest-detail/jRCT2031230263 (accessed on 12 February 2025).
- jRCT. A Phase I Study of Niraparib and Pimitespib in Patients with Solid Tumor. Available online: https://jrct.mhlw.go.jp/en-latest-detail/jRCT2031220179 (accessed on 12 February 2025).
- Ohkubo, S.; Kodama, Y.; Muraoka, H.; Hitotsumachi, H.; Yoshimura, C.; Kitade, M.; Hashimoto, A.; Ito, K.; Gomori, A.; Takahashi, K.; et al. TAS-116, a highly selective inhibitor of heat shock protein 90α and β, demonstrates potent antitumor activity and minimal ocular toxicity in preclinical models. Mol. Cancer Ther. 2015, 14, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Zhou, L.; Dicker, D.T.; Lev, A.; Zhang, S.; Ross, E.; El-Deiry, W.S. Anti-cancer efficacy including Rb-deficient tumors and VHL-independent HIF1α proteasomal destabilization by dual targeting of CDK1 or CDK4/6 and HSP90. Sci. Rep. 2021, 11, 20871. [Google Scholar] [CrossRef]
- Kawazoe, A.; Itahashi, K.; Yamamoto, N.; Kotani, D.; Kuboki, Y.; Taniguchi, H.; Harano, K.; Naito, Y.; Suzuki, M.; Fukutani, M.; et al. TAS-116 (Pimitespib), an Oral HSP90 Inhibitor, in Combination with Nivolumab in Patients with Colorectal Cancer and Other Solid Tumors: An Open-Label, Dose-Finding, and Expansion Phase Ib Trial (EPOC1704). Clin. Cancer Res. 2021, 27, 6709–6715. [Google Scholar] [CrossRef]
- Komatsu, Y.; Shimokawa, T.; Akiyoshi, K.; Karayama, M.; Shimomura, A.; Kawamoto, Y.; Yuki, S.; Tambo, Y.; Kasahara, K. An open-label, crossover study to compare different formulations and evaluate effect of food on pharmacokinetics of pimitespib in patients with advanced solid tumors. Investig. New Drugs 2022, 40, 1011–1020. [Google Scholar] [CrossRef]
- Engstrom, P.F.; Benson, A.B., 3rd; Saltz, L. Colon cancer. Clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2003, 1, 40–53. [Google Scholar] [CrossRef]
- Benson, A.B.; Arnoletti, J.P.; Bekaii-Saab, T.; Chan, E.; Chen, Y.-J.; Choti, M.A.; Cooper, H.S.; Dilawari, R.A.; Engstrom, P.F.; Enzinger, P.C.; et al. Colon Cancer. J. Natl. Compr. Cancer Netw. 2011, 9, 1238–1290. [Google Scholar] [CrossRef]
- Wrana, F.; Dötzer, K.; Prüfer, M.; Werner, J.; Mayer, B. High Dual Expression of the Biomarkers CD44v6/α2β1 and CD44v6/PD-L1 Indicate Early Recurrence after Colorectal Hepatic Metastasectomy. Cancers 2022, 14, 1939. [Google Scholar] [CrossRef]
- Mendel, D.B.; Ortí, E. Isoform composition and stoichiometry of the approximately 90-kDa heat shock protein associated with glucocorticoid receptors. J. Biol. Chem. 1988, 263, 6695–6702. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. PATHWAY anti-HER-2/neu (4B5) Rabbit Monoclonal Primary Antibody. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf/P990081S047A.pdf (accessed on 12 February 2025).
- Rüschoff, J.; Dietel, M.; Baretton, G.; Arbogast, S.; Walch, A.; Monges, G.; Chenard, M.P.; Penault-Llorca, F.; Nagelmeier, I.; Schlake, W.; et al. HER2 diagnostics in gastric cancer-guideline validation and development of standardized immunohistochemical testing. Virchows Arch. 2010, 457, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Ogino, S.; Kawasaki, T.; Brahmandam, M.; Yan, L.; Cantor, M.; Namgyal, C.; Mino-Kenudson, M.; Lauwers, G.Y.; Loda, M.; Fuchs, C.S. Sensitive sequencing method for KRAS mutation detection by Pyrosequencing. J. Mol. Diagn. 2005, 7, 413–421. [Google Scholar] [CrossRef]
- Poehlmann, A.; Kuester, D.; Meyer, F.; Lippert, H.; Roessner, A.; Schneider-Stock, R. K-ras mutation detection in colorectal cancer using the Pyrosequencing technique. Pathol. Res. Pract. 2007, 203, 489–497. [Google Scholar] [CrossRef]
- Hoffmann, O.I.; Ilmberger, C.; Magosch, S.; Joka, M.; Jauch, K.W.; Mayer, B. Impact of the spheroid model complexity on drug response. J. Biotechnol. 2015, 205, 14–23. [Google Scholar] [CrossRef]
- Duarte, D.; Vale, N. Evaluation of synergism in drug combinations and reference models for future orientations in oncology. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100110. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, D.; Eide, P.W.; Eilertsen, I.A.; Danielsen, S.A.; Eknæs, M.; Hektoen, M.; Lind, G.E.; Lothe, R.A. Epigenetic and genetic features of 24 colon cancer cell lines. Oncogenesis 2013, 2, e71. [Google Scholar] [CrossRef]
- Berg, K.C.G.; Eide, P.W.; Eilertsen, I.A.; Johannessen, B.; Bruun, J.; Danielsen, S.A.; Bjørnslett, M.; Meza-Zepeda, L.A.; Eknæs, M.; Lind, G.E.; et al. Multi-omics of 34 colorectal cancer cell lines—A resource for biomedical studies. Mol. Cancer 2017, 16, 116. [Google Scholar] [CrossRef]
- van Erk, M.J.; Krul, C.A.; Caldenhoven, E.; Stierum, R.H.; Peters, W.H.; Woutersen, R.A.; van Ommen, B. Expression profiling of colon cancer cell lines and colon biopsies: Towards a screening system for potential cancer-preventive compounds. Eur. J. Cancer Prev. 2005, 14, 439–457. [Google Scholar] [CrossRef]
- Pinto, M.; Robine-Leon, S.; Appay, M.D.; Kedinger, M.; Triadou, N.; Dussaulx, E.; Lacroix, B.; Simon-Assmann, P.; Haffen, K.; Fogh, J.; et al. Enterocyte-like Differentiation and Polarization of the Human Colon Carcinoma Cell Line Caco-2 in Culture. Biol. Cell 1983, 47, 323–330. [Google Scholar]
- Calabresi, P.; Dexter, D.L.; Heppner, G.H. Clinical and pharmacological implications of cancer cell differentiation and heterogeneity. Biochem. Pharmacol. 1979, 28, 1933–1941. [Google Scholar] [CrossRef] [PubMed]
- Trainer, D.L.; Kline, T.; McCabe, F.L.; Faucette, L.F.; Feild, J.; Chaikin, M.; Anzano, M.; Rieman, D.; Hoffstein, S.; Li, D.J.; et al. Biological characterization and oncogene expression in human colorectal carcinoma cell lines. Int. J. Cancer 1988, 41, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.; Chee, C.E.; Wong, W.; Lam, R.C.T.; Tan, I.B.H.; Ma, B.B.Y. Current advances in targeted therapy for metastatic colorectal cancer—Clinical translation and future directions. Cancer Treat. Rev. 2024, 125, 102700. [Google Scholar] [CrossRef]
- Chen, W.S.; Lee, C.C.; Hsu, Y.M.; Chen, C.C.; Huang, T.S. Identification of heat shock protein 90α as an IMH-2 epitope-associated protein and correlation of its mRNA overexpression with colorectal cancer metastasis and poor prognosis. Int. J. Colorectal Dis. 2011, 26, 1009–1017. [Google Scholar] [CrossRef]
- Nagaraju, G.P.; Long, T.E.; Park, W.; Landry, J.C.; Taliaferro-Smith, L.; Farris, A.B.; Diaz, R.; El-Rayes, B.F. Heat shock protein 90 promotes epithelial to mesenchymal transition, invasion, and migration in colorectal cancer. Mol. Carcinog. 2015, 54, 1147–1158. [Google Scholar] [CrossRef]
- Albakova, Z. HSP90 multi-functionality in cancer. Front. Immunol. 2024, 15, 1436973. [Google Scholar] [CrossRef]
- Dernovšek, J.; Tomašič, T. Following the design path of isoform-selective Hsp90 inhibitors: Small differences, great opportunities. Pharmacol. Ther. 2023, 245, 108396. [Google Scholar] [CrossRef] [PubMed]
- Amatya, E.; Blagg, B.S.J. Recent advances toward the development of Hsp90 C-terminal inhibitors. Bioorg. Med. Chem. Lett. 2023, 80, 129111. [Google Scholar] [CrossRef]
- Reynolds, T.S.; Blagg, B.S.J. Extracellular heat shock protein 90 alpha (eHsp90α)’s role in cancer progression and the development of therapeutic strategies. Eur. J. Med. Chem. 2024, 277, 116736. [Google Scholar] [CrossRef]
- Tang, D.W.; Chen, I.C.; Chou, P.Y.; Lai, M.J.; Liu, Z.Y.; Tsai, K.K.; Cheng, L.H.; Zhao, J.X.; Cho, E.C.; Chang, H.H.; et al. HSP90/LSD1 dual inhibitors against prostate cancer as well as patient-derived colorectal organoids. Eur. J. Med. Chem. 2024, 278, 116801. [Google Scholar] [CrossRef]
- Chiosis, G.; Digwal, C.S.; Trepel, J.B.; Neckers, L. Structural and functional complexity of HSP90 in cellular homeostasis and disease. Nat. Rev. Mol. Cell Biol. 2023, 24, 797–815. [Google Scholar] [CrossRef] [PubMed]
- Youssef, M.E.; Cavalu, S.; Hasan, A.M.; Yahya, G.; Abd-Eldayem, M.A.; Saber, S. Role of Ganetespib, an HSP90 Inhibitor, in Cancer Therapy: From Molecular Mechanisms to Clinical Practice. Int. J. Mol. Sci. 2023, 24, 5014. [Google Scholar] [CrossRef] [PubMed]
- Landmann, H.; Proia, D.A.; He, S.; Ogawa, L.S.; Kramer, F.; Beißbarth, T.; Grade, M.; Gaedcke, J.; Ghadimi, M.; Moll, U.; et al. UDP glucuronosyltransferase 1A expression levels determine the response of colorectal cancer cells to the heat shock protein 90 inhibitor ganetespib. Cell Death Dis. 2014, 5, e1411. [Google Scholar] [CrossRef]
- He, S.; Smith, D.L.; Sequeira, M.; Sang, J.; Bates, R.C.; Proia, D.A. The HSP90 inhibitor ganetespib has chemosensitizer and radiosensitizer activity in colorectal cancer. Investig. New Drugs 2014, 32, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Nagaraju, G.P.; Alese, O.B.; Landry, J.; Diaz, R.; El-Rayes, B.F. HSP90 inhibition downregulates thymidylate synthase and sensitizes colorectal cancer cell lines to the effect of 5FU-based chemotherapy. Oncotarget 2014, 5, 9980–9991. [Google Scholar] [CrossRef]
- Cercek, A.; Shia, J.; Gollub, M.; Chou, J.F.; Capanu, M.; Raasch, P.; Reidy-Lagunes, D.; Proia, D.A.; Vakiani, E.; Solit, D.B.; et al. Ganetespib, a novel Hsp90 inhibitor in patients with KRAS mutated and wild type, refractory metastatic colorectal cancer. Clin. Colorectal Cancer 2014, 13, 207–212. [Google Scholar] [CrossRef]
- Meehan, R.; Kummar, S.; Do, K.; O’Sullivan Coyne, G.; Juwara, L.; Zlott, J.; Rubinstein, L.; Doroshow, J.H.; Chen, A.P. A Phase I Study of Ganetespib and Ziv-Aflibercept in Patients with Advanced Carcinomas and Sarcomas. Oncologist 2018, 23, 1269-e1125. [Google Scholar] [CrossRef]
- Goldman, J.W.; Raju, R.N.; Gordon, G.A.; El-Hariry, I.; Teofilivici, F.; Vukovic, V.M.; Bradley, R.; Karol, M.D.; Chen, Y.; Guo, W.; et al. A first in human, safety, pharmacokinetics, and clinical activity phase I study of once weekly administration of the Hsp90 inhibitor ganetespib (STA-9090) in patients with solid malignancies. BMC Cancer 2013, 13, 152. [Google Scholar] [CrossRef]
- Eroglu, Z.; Chen, Y.A.; Gibney, G.T.; Weber, J.S.; Kudchadkar, R.R.; Khushalani, N.I.; Markowitz, J.; Brohl, A.S.; Tetteh, L.F.; Ramadan, H.; et al. Combined BRAF and HSP90 Inhibition in Patients with Unresectable BRAF (V600E)-Mutant Melanoma. Clin. Cancer Res. 2018, 24, 5516–5524. [Google Scholar] [CrossRef]
- Modi, S.; Stopeck, A.; Linden, H.; Solit, D.; Chandarlapaty, S.; Rosen, N.; D’Andrea, G.; Dickler, M.; Moynahan, M.E.; Sugarman, S.; et al. HSP90 inhibition is effective in breast cancer: A phase II trial of tanespimycin (17-AAG) plus trastuzumab in patients with HER2-positive metastatic breast cancer progressing on trastuzumab. Clin. Cancer Res. 2011, 17, 5132–5139. [Google Scholar] [CrossRef]
- Tse, A.N.; Klimstra, D.S.; Gonen, M.; Shah, M.; Sheikh, T.; Sikorski, R.; Carvajal, R.; Mui, J.; Tipian, C.; O’Reilly, E.; et al. A phase 1 dose-escalation study of irinotecan in combination with 17-allylamino-17-demethoxygeldanamycin in patients with solid tumors. Clin. Cancer Res. 2008, 14, 6704–6711. [Google Scholar] [CrossRef] [PubMed]
- Vaishampayan, U.N.; Burger, A.M.; Sausville, E.A.; Heilbrun, L.K.; Li, J.; Horiba, M.N.; Egorin, M.J.; Ivy, P.; Pacey, S.; Lorusso, P.M. Safety, efficacy, pharmacokinetics, and pharmacodynamics of the combination of sorafenib and tanespimycin. Clin. Cancer Res. 2010, 16, 3795–3804. [Google Scholar] [CrossRef]
- Subramaniam, S.; Goodman, G.E.; Boatman, B.; Smith, A.W.; Iriarte, D.; Gold, P.J. A phase Ib study of AUY922 and cetuximab in patients with KRAS wild-type (WT) metastatic colorectal cancer (mCRC). J. Clin. Oncol. 2015, 33, 3540. [Google Scholar] [CrossRef]
- Bendell, J.C.; Jones, S.F.; Hart, L.; Pant, S.; Moyhuddin, A.; Lane, C.M.; Earwood, C.; Murphy, P.; Patton, J.; Penley, W.C.; et al. A Phase I Study of the Hsp90 Inhibitor AUY922 plus Capecitabine for the Treatment of Patients with Advanced Solid Tumors. Cancer Investig. 2015, 33, 477–482. [Google Scholar] [CrossRef]
- Do, K.T.; O’Sullivan Coyne, G.; Hays, J.L.; Supko, J.G.; Liu, S.V.; Beebe, K.; Neckers, L.; Trepel, J.B.; Lee, M.-J.; Smyth, T.; et al. Phase 1 study of the HSP90 inhibitor onalespib in combination with AT7519, a pan-CDK inhibitor, in patients with advanced solid tumors. Cancer Chemother. Pharmacol. 2020, 86, 815–827. [Google Scholar] [CrossRef] [PubMed]
- Mooradian, M.J.; Cleary, J.M.; Giobbie-Hurder, A.; Darville, L.N.F.; Parikh, A.; Buchbinder, E.I.; Cohen, J.V.; Lawrence, D.P.; Shapiro, G.I.; Keer, H.; et al. Dose-escalation trial of combination dabrafenib, trametinib, and AT13387 in patients with BRAF-mutant solid tumors. Cancer 2023, 129, 1904–1918. [Google Scholar] [CrossRef]
- Zhang, J.; Li, H.; Liu, Y.; Zhao, K.; Wei, S.; Sugarman, E.T.; Liu, L.; Zhang, G. Targeting HSP90 as a Novel Therapy for Cancer: Mechanistic Insights and Translational Relevance. Cells 2022, 11, 2778. [Google Scholar] [CrossRef]
- Chang, C.; Tang, X.; Woodley, D.T.; Chen, M.; Li, W. The Distinct Assignments for Hsp90α and Hsp90β: More Than Skin Deep. Cells 2023, 12, 277. [Google Scholar] [CrossRef]
- Shimomura, A.; Yamamoto, N.; Kondo, S.; Fujiwara, Y.; Suzuki, S.; Yanagitani, N.; Horiike, A.; Kitazono, S.; Ohyanagi, F.; Doi, T.; et al. First-in-Human Phase I Study of an Oral HSP90 Inhibitor, TAS-116, in Patients with Advanced Solid Tumors. Mol. Cancer Ther. 2019, 18, 531–540. [Google Scholar] [CrossRef]
- Mosele, M.F.; Westphalen, C.B.; Stenzinger, A.; Barlesi, F.; Bayle, A.; Bièche, I.; Bonastre, J.; Castro, E.; Dienstmann, R.; Krämer, A.; et al. Recommendations for the use of next-generation sequencing (NGS) for patients with advanced cancer in 2024: A report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2024, 35, 588–606. [Google Scholar] [CrossRef]
- Halfter, K.; Ditsch, N.; Kolberg, H.C.; Fischer, H.; Hauzenberger, T.; von Koch, F.E.; Bauerfeind, I.; von Minckwitz, G.; Funke, I.; Crispin, A.; et al. Prospective cohort study using the breast cancer spheroid model as a predictor for response to neoadjuvant therapy--the SpheroNEO study. BMC Cancer 2015, 15, 519. [Google Scholar] [CrossRef] [PubMed]
- Halfter, K.; Hoffmann, O.; Ditsch, N.; Ahne, M.; Arnold, F.; Paepke, S.; Grab, D.; Bauerfeind, I.; Mayer, B. Testing chemotherapy efficacy in HER2 negative breast cancer using patient-derived spheroids. J. Transl. Med. 2016, 14, 112. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, O.I.; Regenauer, M.; Czogalla, B.; Brambs, C.; Burges, A.; Mayer, B. Interpatient Heterogeneity in Drug Response and Protein Biomarker Expression of Recurrent Ovarian Cancer. Cancers 2022, 14, 2279. [Google Scholar] [CrossRef] [PubMed]
- Goyal, L.; Wadlow, R.C.; Blaszkowsky, L.S.; Wolpin, B.M.; Abrams, T.A.; McCleary, N.J.; Sheehan, S.; Sundaram, E.; Karol, M.D.; Chen, J.; et al. A phase I and pharmacokinetic study of ganetespib (STA-9090) in advanced hepatocellular carcinoma. Investig. New Drugs 2015, 33, 128–137. [Google Scholar] [CrossRef]
- European Medicines Agency; Assessment Report Encorafenib. Available online: https://www.ema.europa.eu/en/documents/variation-report/braftovi-h-c-4280-ws-1695-epar-assessment-report-variation_en.pdf (accessed on 12 February 2025).
- U.S. Food & Drug Administration. Herceptin (Trastuzumab) for Injection, for Intravenous Use. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/103792s5354lbl.pdf (accessed on 12 February 2025).
- Fujimoto, S. Promising antitumor activity of a novel quinoline derivative, TAS-103, against fresh clinical specimens of eight types of tumors measured by flow cytometric DNA analysis. Biol. Pharm. Bull. 2007, 30, 1923–1929. [Google Scholar] [CrossRef]
- Burz, C.; Berindan-Neagoe, I.B.; Balacescu, O.; Tanaselia, C.; Ursu, M.; Gog, A.; Vlase, L.; Chintoanu, M.; Balacescu, L.; Leucuta, S.E.; et al. Clinical and pharmacokinetics study of oxaliplatin in colon cancer patients. J. Gastrointest. Liver Dis. 2009, 18, 39–43. [Google Scholar]
- Ducreux, M.; Ychou, M.; Seitz, J.F.; Bonnay, M.; Bexon, A.; Armand, J.P.; Mahjoubi, M.; Méry-Mignard, D.; Rougier, P. Irinotecan combined with bolus fluorouracil, continuous infusion fluorouracil, and high-dose leucovorin every two weeks (LV5FU2 regimen): A clinical dose-finding and pharmacokinetic study in patients with pretreated metastatic colorectal cancer. J. Clin. Oncol. 1999, 17, 2901–2908. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Groups | Frequency | PFS | OS | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | Distribution | Percent | n | Log-Rank, p-Value | Risk Ratio | Log-Rank, p-Value | Risk Ratio | ||
| sex | 89 | 87 | |||||||
| male | 50 | 56.18 | 0.195 | 1.72 | 0.200 | 1.93 | |||
| female | 39 | 43.82 | |||||||
| age (years) | 89 | 87 | |||||||
| median (range) | 69 (43–90) | ||||||||
| ≤median | 47 | 52.81 | 0.146 | 0.59 | 0.101 | 0.45 | |||
| >median | 42 | 47.19 | |||||||
| tumor location | 89 | 87 | |||||||
| right-sided ∞ | 42 | 47.19 | 0.922 | 1.01 | 0.305 | 0.68 | |||
| left-sided # | 47 | 52.81 | |||||||
| tumor diameter (cm) | 89 | 87 | |||||||
| mean (range) | 4.72 (1.20–11.50) | ||||||||
| ≤mean | 48 | 53.93 | 0.549 | 1.23 | 0.960 | 0.98 | |||
| >mean | 41 | 46.07 | |||||||
| histological type | 89 | 87 | |||||||
| adenocarcinoma | 76 | 85.39 | 0.135 | 1.82 | 0.232 | 1.97 | |||
| mucinous adenocarcinoma | 13 | 14.61 | |||||||
| histologic grade (G) | 89 | 87 | |||||||
| G1/2 | 57 | 64.00 | 2.53 | 0.057 | 2.26 | ||||
| G3/4 | 32 | 36.00 | 0.005 | ||||||
| pT stage | 89 | 87 | |||||||
| pT1/2 | 16 | 18.00 | nc | nc | |||||
| pT3/4 | 73 | 82.00 | 0.012 | 0.023 | |||||
| pN stage | 89 | 87 | |||||||
| pN0 | 57 | 64.00 | 3.80 | 3.80 | |||||
| pN1/2 | 32 | 36.00 | <0.001 | <0.001 | |||||
| cM stage | 89 | 87 | |||||||
| cM0 | 75 | 84.27 | 6.16 | 10.43 | |||||
| cM1 | 14 | 15.73 | <0.001 | <0.001 | |||||
| UICC | 89 | 87 | |||||||
| I-IIA | 47 | 52.81 | 12.93 | 19.98 | |||||
| IIB-IV | 42 | 47.19 | <0.001 | <0.001 | |||||
| lymphangiosis carcinomatosa (L) x | 75 | 73 | |||||||
| L0 | 57 | 76.00 | 4.80 | 6.11 | |||||
| L1 | 18 | 24.00 | <0.001 | <0.001 | |||||
| vessel invasion (V) x | 76 | 74 | |||||||
| V0 | 70 | 92.11 | 3.02 | 5.04 | |||||
| V1 | 6 | 7.89 | 0.001 | <0.001 | |||||
| perineural invasion (P) x | 57 | 56 | |||||||
| P0 | 52 | 91.23 | 4.08 | 5.10 | |||||
| P1 | 5 | 8.77 | <0.001 | <0.001 | |||||
| resection status (R) | 89 | 87 | |||||||
| R0 | 85 | 95.51 | 4.15 | 5.93 | |||||
| R1/2 | 4 | 4.49 | <0.001 | <0.001 | |||||
| sCEA x | 86 | 85 | |||||||
| physiological | 43 | 50.00 | 3.71 | 7.81 | |||||
| pathological | 43 | 50.00 | <0.001 | <0.001 | |||||
| Factor | Groups | PFS | OS | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| sex * | male vs. female | 0.791 | 0.323–1.937 | 0.608 | 1.031 | 0.369–2.879 | 0.954 |
| histological grade | G3/4 vs. G1/2 | 1.928 | 0.834–4.456 | 0.125 | 1.446 | 0.544–3.845 | 0.459 |
| UICC stage | IIB/IV vs. I/IIA | 19.667 | 4.194–92.235 | <0.001 | 21.732 | 2.692–175.434 | 0.004 |
| resection status | R1/2 vs. R0 | 6.886 | 1.957–24.223 | 0.003 | 12.953 | 3.281–51.148 | <0.001 |
| Hsp90α/β positive tumor cells | >40% vs. ≤40% | 3.785 | 1.578–9.078 | 0.003 | 3.502 | 1.292–9.494 | 0.014 |
| HT-29 | Caco-2 | HCT 116 | DLD-1 | LS 174T | SW1116 | Source | |
|---|---|---|---|---|---|---|---|
| Biological Characteristics | |||||||
| Hsp90α/β % positive cells | 90 | 70 | 95 | 50 | 95 | 95 | Results of the present study |
| Her2/neu % positive cells | <10 | 70 | <10 | <10 | 0 | 0 | |
| EpCAM % positive cells | 95 | 95 | 95 | 95 | 90 | 95 | |
| BRAF V600E | mut | wt $ | wt | wt | wt $ | wt $ | $ [45,46] |
| Clinical–Pathological Characteristics | |||||||
| sex | female | female | male | male | female | male | [45,46,47] |
| age (years) | 44 | 72 | 48 | 45 | 58 | 73 | [45,46,47,48,49] |
| primary tumor location | colon | colon | colon ascendens | sigmoid colon | colon | colon | [45,46,47,49,50] |
| histological type | adeno-ca | adeno-ca | adeno-ca | adeno-ca | adeno-ca | adeno-ca | [45,47,48,49] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmitz, S.B.M.; Gülden, J.; Niederreiter, M.; Eichner, C.; Werner, J.; Mayer, B. Strong Hsp90α/β Protein Expression in Advanced Primary CRC Indicates Short Survival and Predicts Response to the Hsp90α/β-Specific Inhibitor Pimitespib. Cells 2025, 14, 836. https://doi.org/10.3390/cells14110836
Schmitz SBM, Gülden J, Niederreiter M, Eichner C, Werner J, Mayer B. Strong Hsp90α/β Protein Expression in Advanced Primary CRC Indicates Short Survival and Predicts Response to the Hsp90α/β-Specific Inhibitor Pimitespib. Cells. 2025; 14(11):836. https://doi.org/10.3390/cells14110836
Chicago/Turabian StyleSchmitz, Sebastian B. M., Jakob Gülden, Marlene Niederreiter, Cassandra Eichner, Jens Werner, and Barbara Mayer. 2025. "Strong Hsp90α/β Protein Expression in Advanced Primary CRC Indicates Short Survival and Predicts Response to the Hsp90α/β-Specific Inhibitor Pimitespib" Cells 14, no. 11: 836. https://doi.org/10.3390/cells14110836
APA StyleSchmitz, S. B. M., Gülden, J., Niederreiter, M., Eichner, C., Werner, J., & Mayer, B. (2025). Strong Hsp90α/β Protein Expression in Advanced Primary CRC Indicates Short Survival and Predicts Response to the Hsp90α/β-Specific Inhibitor Pimitespib. Cells, 14(11), 836. https://doi.org/10.3390/cells14110836