
Clinical Value and Molecular Function of Circulating MicroRNAs in Endometrial Cancer Regulation: A Systematic Review


 , , ,
, , ,
Abstract
:1. Introduction
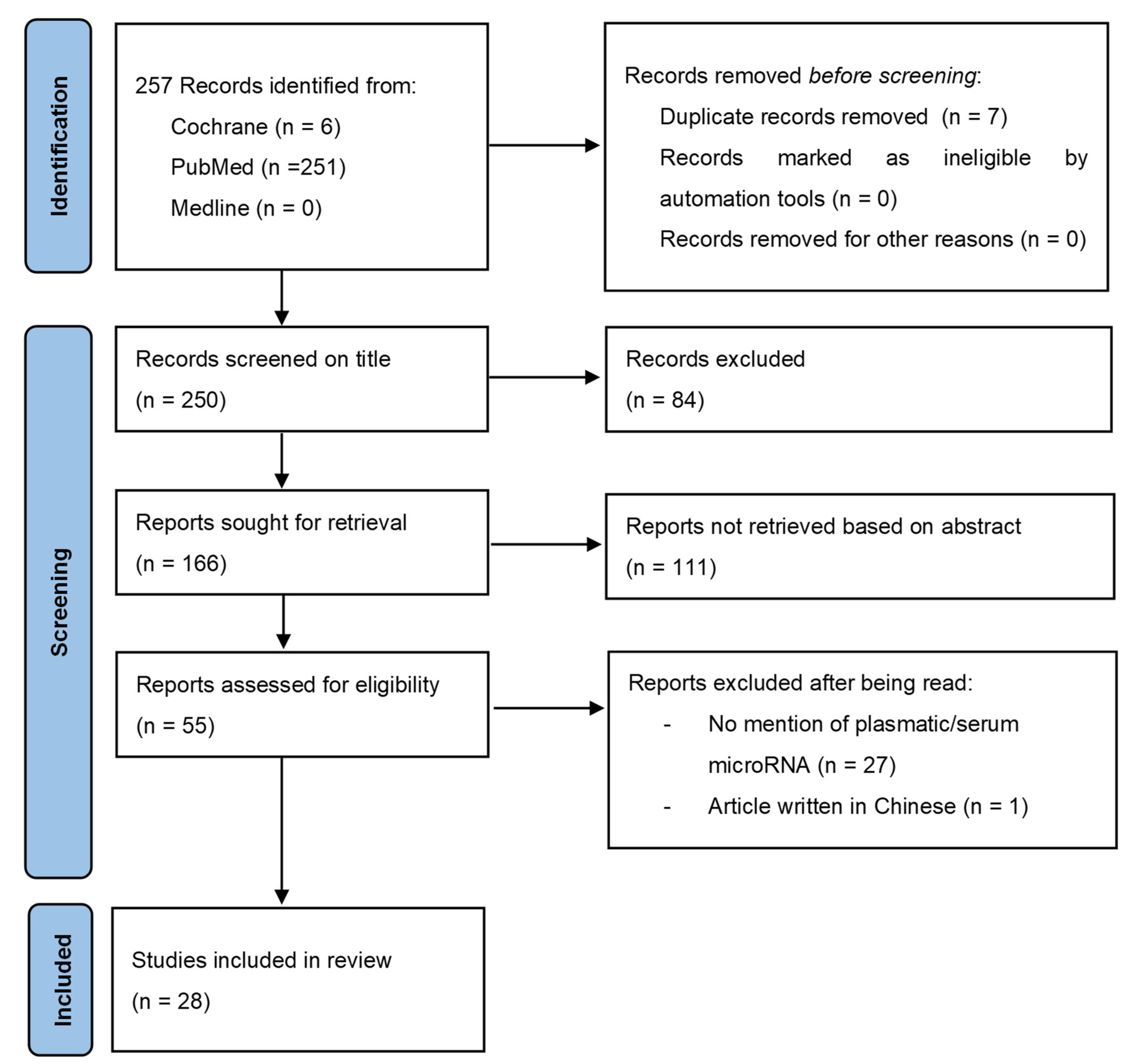
2. Materials and Methods
3. Results
3.1. Clinical Value
3.1.1. Circulating miRs in EC Patients Compared to Healthy Patients without EC
Diagnostic Performance
- Among these 33 miRs, 27 miRs were overexpressed in the plasma/serum of EC patients compared to healthy patients: miR-15b, miR-20b-5p, miR-27a, miR-92a, miR-99a, miR-100, miR-135b, miR-141, miR-142-3p, miR-143-3p, miR-146a-5p, miR-150-5p, miR-151a-5p, miR-186, miR-195-5p, miR-199b, miR-200a, miR-203, miR-205, miR-222, miR-223, miR-423-3p, miR-449a, miR-484, miR-887-5p, miR-1228, and miR-1290.
- Among these miRs, 3 miRs had the best diagnostic performance: miR-205 [11] had an AUC of 1.0 (95% IC: 1.000–1.000); miR-27a [20] was upregulated in the plasma of EC patients compared to patients without EC and had an AUC of 1.000 (p < 0.001) with a sensitivity and specificity of 100% and 100%, respectively, and a positive predictive value and a negative predictive value of 100% and 100%; and miR-150-5p [20] was upregulated in the plasma of EC patients compared to patients without EC and had an AUC of 0.982 (p < 0.001) with a sensitivity and specificity of 88.89% and 100%, respectively, and a positive predictive value and a negative predictive value of 100% and 78.9%. As noted in Table 2, these studies were based on a small number of patients (12 EC patients and 12 healthy patients for miR-205 and 36 EC patients and 36 healthy patients for miR-27a and miR-150-5p).
- Among these 33 miRs, 4 were under-expressed in the plasma/serum of patients with EC compared to healthy patients: miR-9, miR-29b, miR-30a-3p, and miR-301b. Among them, 1 miR had the best diagnostic performance: miR-29b [15] had an AUC of 0.976 (95% IC: 0.951–1.000) with a cutoff value of 0.940 and with a sensitivity of 96.1% and specificity of 97.9%. As noted in Table 2, this study was based on comparing 356 EC patients to 155 healthy patients. This miR was significantly lower in EC patients and had the same ability to discriminate EC patients from healthy patients whether the EC patients were metastatic or not [15]. MiR-29b also had the particularity to be able to discriminate EC patients from healthy patients and from patients with benign endometrial lesions (polyps, myomas): miR-29b expression remained significantly lower (p < 0.05) in patients with EC (0.893 ± 0.432) compared to healthy patients (1.070 ± 0.130) and patients with benign uterine lesions (1.036 ± 0.112) [15].
- Two miRs had various expression levels in the plasma/serum according to different studies (miR-21 and miR-204). Among them, 1 miR had the best diagnostic performance: miR-204 [13] had an AUC of 1.000 (95% IC: 1.000–1.000) with a sensitivity and specificity of 100% each. In this study, miR-204 was downregulated. As noted in Table 2, this study was based on a small number of patients (46 EC patients and 28 healthy patients). Two other studies [8,17] found that miR-204 was upregulated in the serum of patients with EC with a lower diagnostic value with an AUC of 0.740 (95% IC: 0.594–0.885) and 0.668 (95% IC: 0.592–0.743). In one study [21], miR-21 was able to discriminate EC patients from healthy patients and from patients with benign endometrial lesions (polyps, myomas) with a diagnostic performance for EC with an AUC of 0.831 (95% IC: 0.746–0.916) with a sensitivity and specificity of 70% and 92%, respectively, for a cutoff value of 2.937 compared to healthy patients. Healthy patients had an AUC of 0.710 (95% IC: 0.608–0.813) with a sensitivity and specificity of 64% and 76%, respectively, for a cutoff value of 3.457 compared to patients with benign uterine lesions.
- Among them, the miR signature with the best diagnostic performance was “miR-222/miR-223/miR-186/miR-204” [8] with an AUC of 0.927 (95% IC: 0.845–1.000) and a sensitivity of 91.7% and a specificity of 87.5%. As noted in Table 2, this study was based on a small number of patients (26 EC patients and 22 healthy patients).
- The diagnostic performance of the 6-miR signature “miR-20b-5p/miR-143-3p/miR-195-5p/miR-204-5p/miR-423-3p/miR-484” [17] and the 3-miR signature “miR-142-3p/miR-146a-5p/miR-151a-5p” [19] remained significant in the diagnostic of EC compared to healthy patients when sub-categorizing the EC patients within their FIGO stage (I and II–IV) or within their histological grade (G1, G2, and G3).
Prognosis
Grade
- A total of 14 miRs had a significant variation of expression when comparing different histological grades in EC patients compared to healthy patients. When comparing EC with histological G1 to healthy patients, miR-9, miR-92a, miR-141, miR-200a, miR-203, miR-449, miR-1228, miR-1290, miR-143-3p, miR-195-5p, miR-20b-5p, miR-204-5p, miR-423-3p, and miR-484 expression were significantly different [9,17]. When comparing EC with histological G2 to healthy patients, miR-143-3p, miR-195-5p, miR-20b-5p, miR-204-5p, and miR-484 expression were significantly different [17]. When comparing EC with histological G3 to healthy patients, miR-20b-5p, miR-143-3p, miR-195-5p, miR-423-3p, and miR-484 expression were significantly different [17]. When comparing EC with histological G2–G3 to healthy patients, miR-9, miR-92a, miR-141, miR-200a, miR-449a, miR-1228, and miR-1290 expression were significantly different [9].
FIGO
- A total of 19 miRs had a significant variation of expression within different FIGO stages of EC patients compared to healthy patients. When comparing miR expression in patients with FIGO stage I EC to healthy patients, miR-186, miR-222, miR-223, miR 204, miR-143-3p, miR-195-5p, miR-20b-5p, miR-423-3p, and miR-484 expression levels were significant [13,17]. Furthermore, the expression levels and diagnostic performance of miR-186, miR-204, miR-222, and miR-223 remained significant with an AUC of 0.73 (p = 0.002), 1.00 (p < 0.0001), 0.71 (p = 0.006), and 0.85 (p < 0.0001), respectively [13]. When comparing miR expression in patients with FIGO stage II–IV EC to healthy patients, miR-143-3p, miR-195-5p, miR-20b-5p, miR-423-3p, and miR-484 expression levels were significant [17]. When comparing miR expression in patients with FIGO stage IA EC to healthy patients, miR-9, miR-92a, miR-99a, miR-141, miR-199b, miR-203, miR-449a, miR-1228, and miR-1290 expression levels were significant [7,9]. When comparing miR expression in patients with FIGO stages > IA EC to healthy patients, miR-9, miR-92a, miR-99a, miR-100, miR-141, miR-199b, miR-200a, miR-203, miR-449a, miR-1228, and miR-1290 expression levels were significant [7,9].
3.1.2. Prognosis in EC Patients
Histological Type
Histological Grade
Primitive Tumor Size
Myometrial Invasion
FIGO Stage
Lymph Node Metastasis
Lymphovascular Space Invasion
Distant Metastasis
Average Survival Rate
3.2. Molecular Function of Circulating miRs in EC
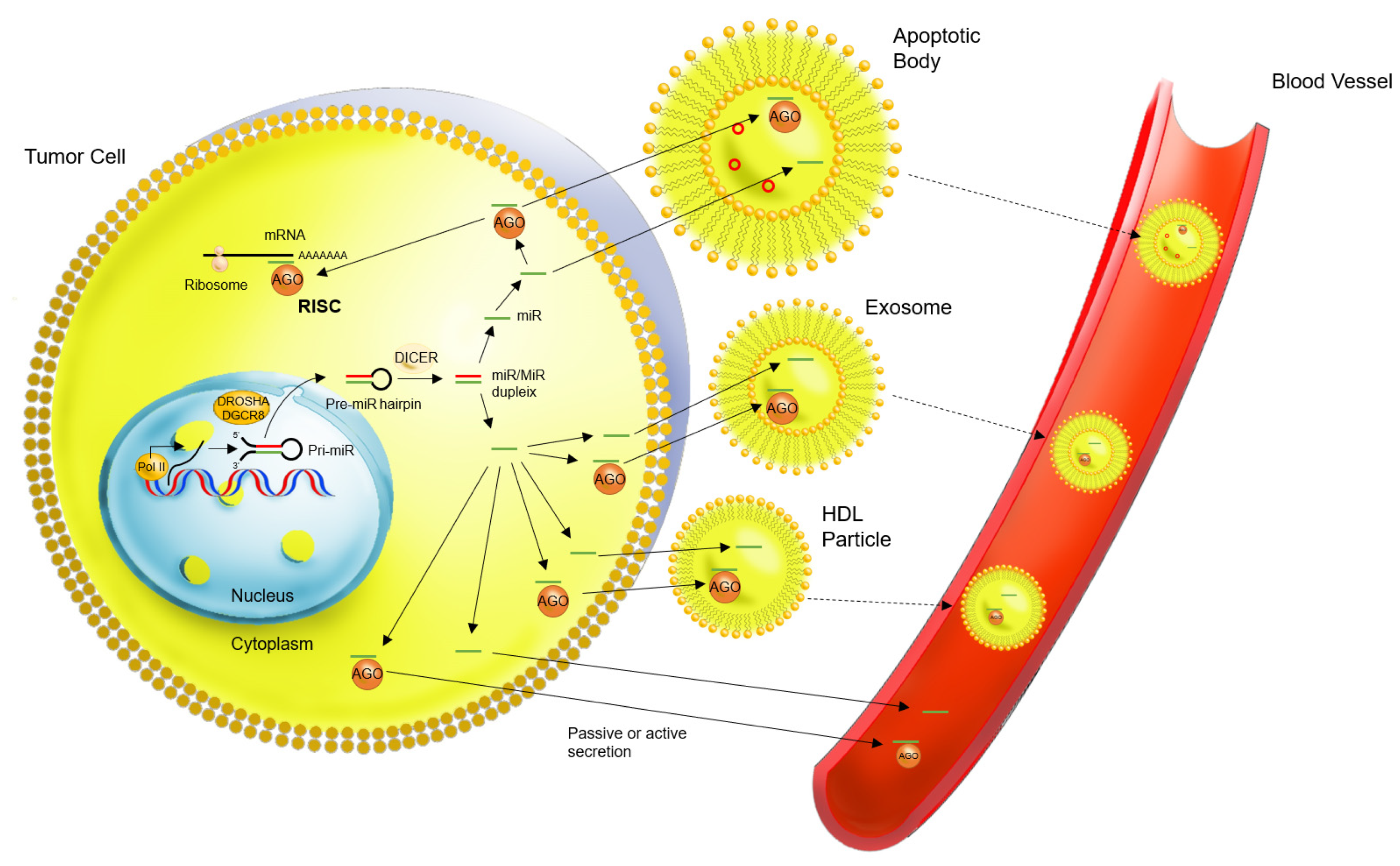
- Bound to Argonaute (AGO) proteins: AGO-protein-bounded miRs are the largest form of extracellular circulation and represent up to 90–95% of the circulating miRs that are found in plasma. The AGO protein binds with the miR in the intracellular compartment in order to create the RISC-complex, which regulates ARN messenger expression by cleavage or translational interference. It is this same AGO-protein–miR complex that is found in the extracellular compartment, either alone or within a micro-vesicle or an HDL-particle [22].
- Encapsulated in micro-vesicles, such as exosomes. It remains uncertain whether miRs are always bound to an AGO protein inside these micro-vesicles or not. The circulation of miRs in exosomes can result from either a passive or an active secretion from the tumor cell. Micro-vesicular miRs may represent the smallest fraction of circulating miRs [22].
- Bound in High-density lipoproteins (HDL particles): miR stability could also be explained by the fact that they circulate in HDL-particles. It is also unknown if miRs circulate when bound to an AGO protein within the HDL-particles or not, and if its secretion in the extracellular compartment is active or passive [22].
- Apoptotic bodies: based on the theory that miR secretion could be a passive mechanism resulting in tumor cell waste, miRs could also circulate in apoptotic bodies [22].
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Morice, P.; Leary, A.; Creutzberg, C.; Abu-Rustum, N.; Darai, E. Endometrial cancer. The Lancet 2016, 387, 1094–1108. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boroń, D.; Zmarzły, N.; Wierzbik-Strońska, M.; Rosińczuk, J.; Mieszczański, P.; Grabarek, B.O. Recent Multiomics Approaches in Endometrial Cancer. Int. J. Mol. Sci. 2022, 23, 1237. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Ingolia, N.T.; Weissman, J.S.; Bartel, D.P. Mammalian microRNAs predominantly act to decrease target mRNA levels. Nature 2010, 466, 835–840. [Google Scholar] [CrossRef] [Green Version]
- Favier, A.; Rocher, G.; Larsen, A.K.; Delangle, R.; Uzan, C.; Sabbah, M.; Castela, M.; Duval, A.; Mehats, C.; Canlorbe, G. MicroRNA as Epigenetic Modifiers in Endometrial Cancer: A Systematic Review. Cancers 2021, 13, 1137. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Torres, A.; Torres, K.; Pesci, A.; Ceccaroni, M.; Paszkowski, T.; Cassandrini, P.; Zamboni, G.; Maciejewski, R. Deregulation of miR-100, miR-99a and miR-199b in tissues and plasma coexists with increased expression of mTOR kinase in endometrioid endometrial carcinoma. BMC Cancer 2012, 12, 369. [Google Scholar] [CrossRef] [Green Version]
- Jia, W.; Wu, Y.; Zhang, Q.; Gao, G.; Zhang, C.; Xiang, Y. Identification of four serum microRNAs from a genome-wide serum microRNA expression profile as potential non-invasive biomarkers for endometrioid endometrial cancer. Oncol. Lett. 2013, 6, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Torres, A.; Torres, K.; Pesci, A.; Ceccaroni, M.; Paszkowski, T.; Cassandrini, P.; Zamboni, G.; Maciejewski, R. Diagnostic and prognostic significance of miRNA signatures in tissues and plasma of endometrioid endometrial carcinoma patients. Int. J. Cancer 2013, 132, 1633–1645. [Google Scholar] [CrossRef]
- Wang, L.; Chen, Y.-J.; Xu, K.; Xu, H.; Shen, X.-Z.; Tu, R.-Q. Circulating microRNAs as a fingerprint for endometrial endometrioid adenocarcinoma. PLoS ONE 2014, 9, e110767. [Google Scholar] [CrossRef]
- Tsukamoto, O.; Miura, K.; Mishima, H.; Abe, S.; Kaneuchi, M.; Higashijima, A.; Miura, S.; Kinoshita, A.; Yoshiura, K.; Masuzaki, H. Identification of endometrioid endometrial carcinoma-associated microRNAs in tissue and plasma. Gynecol. Oncol. 2014, 132, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Wang, N.; Yin, D.; Li, Y.K.; Guo, L.; Shi, L.P.; Huang, X. Changes in the Expression of Serum MiR-887-5p in Patients With Endometrial Cancer. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2016, 26, 1143–1147. [Google Scholar] [CrossRef] [PubMed]
- Montagnana, M.; Benati, M.; Danese, E.; Giudici, S.; Perfranceschi, M.; Ruzzenenete, O.; Salvagno, G.L.; Bassi, A.; Gelati, M.; Paviati, E.; et al. Aberrant MicroRNA Expression in Patients With Endometrial Cancer. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2017, 27, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Benati, M.; Montagnana, M.; Danese, E.; Paviati, E.; Giudici, S.; Franchi, M.; Lippi, G. Evaluation of mir-203 Expression Levels and DNA Promoter Methylation Status in Serum of Patients with Endometrial Cancer. Clin. Lab. 2017, 63, 1675–1681. [Google Scholar] [CrossRef]
- Wang, H.; Wang, T.-T.; Lv, X.-P. Expression and prognostic value of miRNA-29b in peripheral blood for endometrial cancer. Future Oncol. Lond. Engl. 2018, 14, 1365–1376. [Google Scholar] [CrossRef]
- Ritter, A.; Hirschfeld, M.; Berner, K.; Jaeger, M.; Grundner-Culemann, F.; Schlosser, P.; Asberger, J.; Weiss, D.; Noethling, C.; Mayer, S.; et al. Discovery of potential serum and urine-based microRNA as minimally-invasive biomarkers for breast and gynecological cancer. Cancer Biomark. Sect. Dis. Markers 2020, 27, 225–242. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Zou, X.; Liu, C.; Cheng, W.; Zhang, S.; Geng, X.; Zhu, W. MicroRNA expression profile in serum reveals novel diagnostic biomarkers for endometrial cancer. Biosci. Rep. 2021, 41, BSR20210111. [Google Scholar] [CrossRef]
- Zhou, L.; Wang, W.; Wang, F.; Yang, S.; Hu, J.; Lu, B.; Pan, Z.; Ma, Y.; Zheng, M.; Zhou, L.; et al. Plasma-derived exosomal miR-15a-5p as a promising diagnostic biomarker for early detection of endometrial carcinoma. Mol. Cancer 2021, 20, 57. [Google Scholar] [CrossRef]
- Fan, X.; Cao, M.; Liu, C.; Zhang, C.; Li, C.; Cheng, W.; Zhang, S.; Zhang, H.; Zhu, W. Three plasma-based microRNAs as potent diagnostic biomarkers for endometrial cancer. Cancer Biomark. Sect. Dis. Markers 2021, 31, 127–138. [Google Scholar] [CrossRef]
- Ghazala, R.A.; El-Attar, E.A.; Abouzeid, Z.S. Circulating miRNA 27a and miRNA150-5p; A noninvasive approach to endometrial carcinoma. Mol. Biol. Rep. 2021, 48, 4351–4360. [Google Scholar] [CrossRef]
- Gao, Y.; Dai, M.; Liu, H.; He, W.; Lin, S.; Yuan, T.; Chen, H.; Dai, S. Diagnostic value of circulating miR-21: An update meta-analysis in various cancers and validation in endometrial cancer. Oncotarget 2016, 7, 68894–68908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Zhang, J.; Xie, B.; Li, H.; Shen, J.; Chen, J. MicroRNA-200 Family Profile: A Promising Ancillary Tool for Accurate Cancer Diagnosis. Am. J. Ther. 2016, 23, e388–e397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, F.; Zhang, L.; Xu, H.; Li, R.; Xu, L.; Qin, Z.; Zhong, B. The Significance Role of microRNA-200c as a Prognostic Factor in Various Human Solid Malignant Neoplasms: A Meta-Analysis. J. Cancer 2019, 10, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Rižner, T.L. Discovery of biomarkers for endometrial cancer: Current status and prospects. Expert Rev. Mol. Diagn. 2016, 16, 1315–1336. [Google Scholar] [CrossRef]
- Donkers, H.; Bekkers, R.; Galaal, K. Diagnostic value of microRNA panel in endometrial cancer: A systematic review. Oncotarget 2020, 11, 2010–2023. [Google Scholar] [CrossRef]
- Klicka, K.; Grzywa, T.M.; Klinke, A.; Mielniczuk, A.; Włodarski, P.K. The Role of miRNAs in the Regulation of Endometrial Cancer Invasiveness and Metastasis—A Systematic Review. Cancers 2021, 13, 3393. [Google Scholar] [CrossRef]
- Zhao, Y.-N.; Chen, G.-S.; Hong, S.-J. Circulating MicroRNAs in gynecological malignancies: From detection to prediction. Exp. Hematol. Oncol. 2014, 3, 14. [Google Scholar] [CrossRef] [Green Version]
- Yanokura, M.; Banno, K.; Adachi, M.; Aoki, D.; Abe, K. Genome-wide DNA methylation sequencing reveals miR-663a is a novel epimutation candidate in CIMP-high endometrial cancer. Int. J. Oncol. 2017, 50, 1934–1946. [Google Scholar] [CrossRef] [Green Version]
- Zavesky, L.; Jandakova, E.; Turyna, R.; Langmeierova, L.; Weinberger, V.; Minar, L.; Kohoutova, M. New perspectives in diagnosis of gynaecological cancers: Emerging role of circulating microRNAs as novel biomarkers. Neoplasma 2015, 62, 509–520. [Google Scholar] [CrossRef] [Green Version]
- Kanekura, K.; Nishi, H.; Isaka, K.; Kuroda, M. MicroRNA and gynecologic cancers. J. Obstet. Gynaecol. Res. 2016, 42, 612–617. [Google Scholar] [CrossRef]
- Muinelo-Romay, L.; Casas-Arozamena, C.; Abal, M. Liquid Biopsy in Endometrial Cancer: New Opportunities for Personalized Oncology. Int. J. Mol. Sci. 2018, 19, 2311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Q.; An, Q.; Niu, B.; Lu, X.; Zhang, N.; Cao, X. Role of miR-221/222 in Tumor Development and the Underlying Mechanism. J. Oncol. 2019, 2019, 7252013. [Google Scholar] [CrossRef] [PubMed]
- De Bruyn, C.; Baert, T.; Van den Bosch, T.; Coosemans, A. Circulating Transcripts and Biomarkers in Uterine Tumors: Is There a Predictive Role? Curr. Oncol. Rep. 2020, 22, 12. [Google Scholar] [CrossRef]
- Openshaw, M.R.; McVeigh, T.P. Non-invasive Technology Advances in Cancer-A Review of the Advances in the Liquid Biopsy for Endometrial and Ovarian Cancers. Front. Digit. Health 2020, 2, 573010. [Google Scholar] [CrossRef] [PubMed]
- Peng, Q.; Feng, Z.; Shen, Y.; Zhu, J.; Zou, L.; Shen, Y.; Zhu, Y. Integrated analyses of microRNA-29 family and the related combination biomarkers demonstrate their widespread influence on risk, recurrence, metastasis and survival outcome in colorectal cancer. Cancer Cell Int. 2019, 19, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Pan, B.; Sun, L.; Chen, X.; Zeng, K.; Hu, X.; Xu, T.; Xu, M.; Wang, S. Circulating Exosomal miR-27a and miR-130a Act as Novel Diagnostic and Prognostic Biomarkers of Colorectal Cancer. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2018, 27, 746–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Li, B.; Zhao, H.; Chang, J. The expression and clinical significance of serum miR-205 for breast cancer and its role in detection of human cancers. Int. J. Clin. Exp. Med. 2015, 8, 3034–3043. [Google Scholar]
- Gregory, P.A.; Bert, A.G.; Paterson, E.L.; Barry, S.C.; Tsykin, A.; Farshid, G.; Vadas, M.A.; Khew-Goodall, Y.; Goodall, G.J. The miR-200 family and miR-205 regulate epithelial to mesenchymal transition by targeting ZEB1 and SIP1. Nat. Cell Biol. 2008, 10, 593–601. [Google Scholar] [CrossRef]
- Imboden, S.; Nastic, D.; Ghaderi, M.; Rydberg, F.; Siegenthaler, F.; Mueller, M.D.; Rau, T.T.; Epstein, E.; Carlson, J.W. Implementation of the 2021 molecular ESGO/ESTRO/ESP risk groups in endometrial cancer. Gynecol. Oncol. 2021, 162, 394–400. [Google Scholar] [CrossRef]
- Daix, M.; Angeles, M.A.; Migliorelli, F.; Kakkos, A.; Martinez Gomez, C.; Delbecque, K.; Mery, E.; Tock, S.; Gabiache, E.; Decuypere, M.; et al. Concordance between preoperative ESMO-ESGO-ESTRO risk classification and final histology in early-stage endometrial cancer. J. Gynecol. Oncol. 2021, 32, e48. [Google Scholar] [CrossRef]
- Delangle, R.; De Foucher, T.; Larsen, A.K.; Sabbah, M.; Azaïs, H.; Bendifallah, S.; Daraï, E.; Ballester, M.; Mehats, C.; Uzan, C.; et al. The Use of microRNAs in the Management of Endometrial Cancer: A Meta-Analysis. Cancers 2019, 11, 832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, W.-C.; Han, N.; Ping, G.-F.; Zheng, P.-F.; Feng, H.-L.; Qin, L.; He, P. microRNA-9 functions as a tumor suppressor in colorectal cancer by targeting CXCR4. Int. J. Clin. Exp. Pathol. 2018, 11, 526–536. [Google Scholar] [PubMed]
- Zhu, B.; Xi, X.; Liu, Q.; Cheng, Y.; Yang, H. MiR-9 functions as a tumor suppressor in acute myeloid leukemia by targeting CX chemokine receptor 4. Am. J. Transl. Res. 2019, 11, 3384–3397. [Google Scholar] [PubMed]
- Lu, J.; Liu, Q.-H.; Wang, F.; Tan, J.-J.; Deng, Y.-Q.; Peng, X.-H.; Liu, X.; Zhang, B.; Xu, X.; Li, X.-P. Exosomal miR-9 inhibits angiogenesis by targeting MDK and regulating PDK/AKT pathway in nasopharyngeal carcinoma. J. Exp. Clin. Cancer Res. CR 2018, 37, 147. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Wu, N.; Liu, X.; Xia, Y.; Chen, Y.; Li, S.; Deng, Z. MicroRNA-142-3p inhibits cell proliferation and chemoresistance in ovarian cancer via targeting sirtuin 1. Exp. Ther. Med. 2018, 15, 5205–5214. [Google Scholar] [CrossRef]
- Schwickert, A.; Weghake, E.; Brüggemann, K.; Engbers, A.; Brinkmann, B.F.; Kemper, B.; Seggewiß, J.; Stock, C.; Ebnet, K.; Kiesel, L.; et al. microRNA miR-142-3p Inhibits Breast Cancer Cell Invasiveness by Synchronous Targeting of WASL, Integrin Alpha V, and Additional Cytoskeletal Elements. PLoS ONE 2015, 10, e0143993. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.; Li, Z.; Li, W.; Ai, J.; Chen, X. MicroRNA-142-3p suppresses endometriosis by regulating KLF9-mediated autophagy in vitro and in vivo. RNA Biol. 2019, 16, 1733–1748. [Google Scholar] [CrossRef]
- Wang, C.; Li, Q.; He, Y. MicroRNA-21-5p promotes epithelial to mesenchymal transition by targeting SRY-box 17 in endometrial cancer. Oncol. Rep. 2020, 43, 1897–1905. [Google Scholar] [CrossRef] [Green Version]
- Jing, L.; Hua, X.; Yuanna, D.; Rukun, Z.; Junjun, M. Exosomal miR-499a-5p Inhibits Endometrial Cancer Growth and Metastasis via Targeting VAV3. Cancer Manag. Res. 2020, 12, 13541–13552. [Google Scholar] [CrossRef]
- Mueller, A.C.; Sun, D.; Dutta, A. The miR-99 family regulates the DNA damage response through its target SNF2H. Oncogene 2013, 32, 1164–1172. [Google Scholar] [CrossRef] [Green Version]
- Kong, J.; He, X.; Wang, Y.; Li, J. Effect of microRNA-29b on proliferation, migration, and invasion of endometrial cancer cells. J. Int. Med. Res. 2019, 47, 3803–3817. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, R.; Tripathi, R.; Sridhar, T.S.; Korlimarla, A.; Choudhury, K.D.; Suryavanshi, M.; Mehta, A.; Doval, D.C. Prognostic role of microRNA 182 and microRNA 18a in locally advanced triple negative breast cancer. PLoS ONE 2020, 15, e0242190. [Google Scholar] [CrossRef] [PubMed]
- Huan, T.; Chen, G.; Liu, C.; Bhattacharya, A.; Rong, J.; Chen, B.H.; Seshadri, S.; Tanriverdi, K.; Freedman, J.E.; Larson, M.G.; et al. Age-associated microRNA expression in human peripheral blood is associated with all-cause mortality and age-related traits. Aging Cell 2018, 17, e12687. [Google Scholar] [CrossRef] [PubMed]
- Hijmans, J.G.; Diehl, K.J.; Bammert, T.D.; Kavlich, P.J.; Lincenberg, G.M.; Greiner, J.J.; Stauffer, B.L.; DeSouza, C.A. Influence of Overweight and Obesity on Circulating Inflammation-Related microRNA. MicroRNA Shariqah United Arab Emir. 2018, 7, 148–154. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Yuan, Y.; Cho, J.-H.; McClarty, S.; Baxter, D.; Galas, D.J. Comparing the MicroRNA spectrum between serum and plasma. PLoS ONE 2012, 7, e41561. [Google Scholar] [CrossRef] [PubMed]
- Chiam, K.; Mayne, G.C.; Wang, T.; Watson, D.I.; Irvine, T.S.; Bright, T.; Smith, L.T.; Ball, I.A.; Bowen, J.M.; Keefe, D.M.; et al. Serum outperforms plasma in small extracellular vesicle microRNA biomarker studies of adenocarcinoma of the esophagus. World J. Gastroenterol. 2020, 26, 2570–2583. [Google Scholar] [CrossRef]
- Xu, W.; Zhou, Y.; Xu, G.; Geng, B.; Cui, Q. Transcriptome analysis reveals non-identical microRNA profiles between arterial and venous plasma. Oncotarget 2017, 8, 28471–28480. [Google Scholar] [CrossRef]
- Sriram, H.; Khanka, T.; Kedia, S.; Tyagi, P.; Ghogale, S.; Deshpande, N.; Chatterjee, G.; Rajpal, S.; Patkar, N.V.; Subramanian, P.G.; et al. Improved protocol for plasma microRNA extraction and comparison of commercial kits. Biochem. Medica 2021, 31, 030705. [Google Scholar] [CrossRef]
- Hoshino, I. The usefulness of microRNA in urine and saliva as a biomarker of gastroenterological cancer. Int. J. Clin. Oncol. 2021, 26, 1431–1440. [Google Scholar] [CrossRef]
- Donkers, H.; Hirschfeld, M.; Weiß, D.; Erbes, T.; Jäger, M.; Pijnenborg, J.; Bekkers, R.; Galaal, K. Detection of microRNA in urine to identify patients with endometrial cancer: A feasibility study. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2021, 31, 868–874. [Google Scholar] [CrossRef] [PubMed]
- O’Flynn, H.; Ryan, N.A.J.; Narine, N.; Shelton, D.; Rana, D.; Crosbie, E.J. Diagnostic accuracy of cytology for the detection of endometrial cancer in urine and vaginal samples. Nat. Commun. 2021, 12, 952. [Google Scholar] [CrossRef] [PubMed]
- Pegtel, D.M.; Gould, S.J. Exosomes. Annu. Rev. Biochem. 2019, 88, 487–514. [Google Scholar] [CrossRef] [PubMed]
- Elewaily, M.I.; Elsergany, A.R. Emerging role of exosomes and exosomal microRNA in cancer: Pathophysiology and clinical potential. J. Cancer Res. Clin. Oncol. 2021, 147, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Shi, K.; Yang, S.; Liu, J.; Zhou, Q.; Wang, G.; Song, J.; Li, Z.; Zhang, Z.; Yuan, W. Effect of exosomal miRNA on cancer biology and clinical applications. Mol. Cancer 2018, 17, 147. [Google Scholar] [CrossRef] [PubMed]
- Turchinovich, A.; Weiz, L.; Langheinz, A.; Burwinkel, B. Characterization of extracellular circulating microRNA. Nucleic Acids Res. 2011, 39, 7223–7233. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors | Date | Publication | Name of article |
|---|---|---|---|
| Original Article | |||
| Torres, A. et al. [7] | 2012 | BMC Cancer | Deregulation of miR-100, miR-99a and miR-199b in tissues and plasma coexists with increased expression of mTOR kinase in endometrioid endometrial carcinoma |
| Jia, W. et al. [8] | 2013 | Oncol. Lett. | Identification of four serum microRNAs from a genome-wide serum microRNA expression profile as potential non- invasive biomarkers for endometrioid endometrial cancer |
| Torres, A. et al. [9] | 2013 | Int. J. Cancer. | Diagnostic and prognostic significance of miRNA signatures in tissues and plasma of endometrioid endometrial carcinoma patients |
| Wang, L. et al. [10] | 2014 | PLoS ONE | Circulating microRNAs as a fingerprint for endometrial endometrioid adenocarcinoma |
| Tsukamoto, O. et al. [11] | 2014 | Gynecol. Oncol. | Identification of endometrioid endometrial carcinoma-associated microRNAs in tissue and plasma |
| Jiang, Y. et al. [12] | 2016 | Int. J. Gynecol. Cancer | Changes in the Expression of Serum MiR-887-5p in Patients With Endometrial Cancer |
| Montagnana, M. et al. [13] | 2017 | Int. J. Gynecol. Cancer | Aberrant MicroRNA Expression in Patients With Endometrial Cancer |
| Benati, M. et al. [14] | 2017 | Clin. Lab. | Evaluation of mir-203 Expression Levels and DNA Promoter Methylation Status in Serum of Patients with Endometrial Cancer |
| Wang, H. et al. [15] | 2018 | Future Oncol. | Expression and prognostic value of miRNA-29b in peripheral blood for endometrial cancer |
| Ritter, A. et al. [16] | 2020 | Cancer Biomark. | Discovery of potential serum and urine-based microRNA as minimally-invasive biomarkers for breast and gynecological cancer |
| Fan, X. et al. [17] | 2021 | Biosci. Rep. | MicroRNA expression profile in serum reveals novel diagnostic biomarkers for endometrial cancer |
| Zhou, L. et al. [18] | 2021 | Mol. Cancer | Plasma-derived exosomal miR-15a-5p as a promising diagnostic biomarker for early detection of endometrial carcinoma |
| Fan, X. et al. [19] | 2021 | Cancer Biomark. | Three plasma-based microRNAs as potent diagnostic biomarkers for endometrial cancer |
| Ghazala, R.A. et al. [20] | 2021 | Mol. Biol. Rep. | Circulating miRNA 27a and miRNA150-5p; a noninvasive approach to endometrial carcinoma |
| Original Article with Meta-Analysis | |||
| Gao, Y. et al. [21] | 2016 | Oncotarget | Diagnostic value of circulating miR-21: An update meta-analysis in various cancers and validation in endometrial cancer |
| Meta-Analysis | |||
| Liu, X. et al. [22] | 2016 | Am. J. Ther. | MicroRNA-200 Family Profile: A Promising Ancillary Tool for Accurate Cancer Diagnosis |
| Wang, F. et al. [23] | 2019 | Clin. Lab. | The Significance Role of microRNA-200c as a Prognostic Factor in Various Human Solid Malignant Neoplasms: A Meta-Analysis |
| Systematic Review | |||
| Rižner, T.L. [24] | 2016 | Expert Rev. Mol. Diagn. | Discovery of biomarkers for endometrial cancer: current status and prospects |
| Donkers, H. et al. [25] | 2020 | Oncotarget | Diagnostic value of microRNA panel in endometrial cancer: A systematic review |
| Klicka, K. et al. [26] | 2021 | Cancers | The Role of miRNAs in the Regulation of Endometrial Cancer Invasiveness and Metastasis—A Systematic Review |
| Review | |||
| Zhao, Y.N. et al. [27] | 2014 | Exp. Hematol. Oncol. | Circulating MicroRNAs in gynecological malignancies: from detection to prediction |
| Yanokura, M. et al. [28] | 2015 | EXCLI J. | MicroRNAS in endometrial cancer: recent advances and potential clinical applications |
| Zavesky, L. et al. [29] | 2015 | Neoplasma | New perspectives in diagnosis of gynecological cancers: Emerging role of circulating microRNAs as novel biomarkers |
| Kanekura, K. et al. [30] | 2016 | J. Obstet. Gynaecol. Res. | MicroRNA and gynecologic cancers |
| Muinelo-Romay, L. et al. [31] | 2018 | Int. J. Mol. Sci. | Liquid Biopsy in Endometrial Cancer: New Opportunities for Personalized Oncology |
| Song, Q. et al. [32] | 2019 | J. Oncol. | Role of miR-221/222 in Tumor Development and the Underlying Mechanism |
| De Bruyn, C. et al. [33] | 2020 | Curr. Oncol. Rep. | Circulating Transcripts and Biomarkers in Uterine Tumors: Is There a Predictive Role? |
| Openshaw, M.R. et al. [34] | 2020 | Front. Digit Health | Non-invasive Technology Advances in Cancer-A Review of the Advances in the Liquid Biopsy for Endometrial and Ovarian Cancer |
| Name of miR | Sample | EC Patients n | Healthy Patients (Without EC) n | Circulating miR Variation in EC Vs. Healthy Patients | AUC (95% CI/p) | Cut-Off Value | Se | Spe | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Training Phase (TP) | Validation Phase (VP) | |||||||||
| Individual miR | ||||||||||
| miR-9 [9] | plasma | 34 | 14 | Down | - | 0.768 (0.622–0.879) | 2.6 | 88 | 71 | |
| miR-15b [10] | plasma | Screening phase: 9 Validation phase: 31 | Screening phase: 20 Validation phase: 33 | Up | - | 0.768 (0.653–0.882) | - | 74.2 | 69.7 | |
| miR-20b-5p [17] | serum | Screening phase: 2 Testing phase: 21 Validation phase: 41 External validation: 30 | Screening phase: 1 Testing phase: 24 Validation phase: 48 External validation: 30 | Up | 0.756 (0.689-0.823) † | - | - | - | ||
| miR-21 | [21] | serum | 50 | 50 (50 *) | Up (Up *) | - | 0.831 (0.746–0.916) 0.710 * (0.608–0.813) * | 2.937 (3.457 *) | 70 (64 *) | 92 (76 *) |
| [11] | serum | 12 | 12 | Down | - | 0.757 (0.561–0.953) | - | - | - | |
| miR-27a | [10] | plasma | Screening phase: 9 Validation phase: 31 | Screening phase: 20 Validation phase: 33 | Up | - | 0.813 (0.699–0.927) | - | 77.4 | 81.8 |
| [20] | serum | 36 | 36 | Up | - | 1.000 (<0.001) | 0.2872 | 100 | 100 | |
| miR-29b | Located EC [15] | Venous blood ** | 356 | 155 (149 *) | Down | - | 0.976 (0.951–1.000) | 0.940 | 96.1 | 97.9 |
| Metastatic EC [15] | Venous blood ** | 356 | 155 (149 *) | Down | - | 0.974 (0.949–0.999) | 0.917 | 96.7 | 95 | |
| miR-30a-5p [11] | Plasma | 12 | 12 | Down | - | 0.813 (0.638–0.987) | - | - | - | |
| miR-92a [9] | Plasma | 34 | 14 | Up | - | 0.794 (0.651–0.898) | 1.6 | 61 | 93 | |
| miR-99a [7] | Plasma | 34 | 14 | Up | - | 0.810 (0.669–0.909) | 1.23 | 76 | 79 | |
| miR-100 [7] | Plasma | 34 | 14 | Up | - | 0.740 (0.592–0.857) | 1.5 | 64 | 79 | |
| miR-135b [11] | Plasma | 12 | 12 | Up | - | 0.972 (0.913–1.000) | - | - | - | |
| miR-141 [9] | plasma | 34 | 14 | Up | - | 0.766 (0.620–0.877) | 2.5 | 58 | 93 | |
| miR-142-3p [19] | Plasma | Screening phase: 2 Testing phase: 22 Validation phase: 44 External validation: 27 | Screening phase: 1 Testing phase: 22 Validation phase: 34 External validation: 23 | Up | 0.689 (0.611–0.767) † | - | - | - | ||
| miR-143-3p [17] | serum | Screening phase: 2 Testing phase: 21 Validation phase: 41 External validation: 30 | Screening phase: 1 Testing phase: 24 Validation phase: 48 External validation: 30 | Up | 0.677 (0.602–0.751) † | - | - | - | ||
| miR-146a-5p [19] | Plasma | Screening phase: 2 Testing phase: 22 Validation phase: 44 External validation: 27 | Screening phase: 1 Testing phase: 22 Validation phase: 34 External validation: 23 | Up | 0.694 (0.616-0.772) † | - | - | - | ||
| miR-150-5p [20] | Serum | 36 | 36 | Up | - | 0.982 (<0.001) | 1.02 | 88.89 | 100 | |
| miR-151a-5p [19] | Plasma | Screening phase: 2 Testing phase: 22 Validation phase: 44 External validation: 27 | Screening phase: 1 Testing phase: 22 Validation phase: 34 External validation: 23 | Up | 0.680 (0.601–0.759) † | - | - | - | ||
| miR-186 | [13] *** | Serum | 46 | 28 | Up | - | 0.7000 (=0.004) | - | - | - |
| [8] | Serum | Screening phase: 7 Validation phase: 26 | Screening phase: 20 Validation phase: 22 | Up | - | 0.865 (0.755–0.974) | - | - | - | |
| miR-195-5p [17] | serum | Screening phase: 2 Testing phase: 21 Validation phase: 41 External validation: 30 | Screening phase: 1 Testing phase: 24 Validation phase: 48 External validation: 30 | Up | 0.669 (0.593–0.745) † | - | - | - | ||
| miR-199b [7] | Plasma | 34 | 14 | Up | - | 0.786 (0.642–0.892) | 2.48 | 79 | 71 | |
| miR-200a [9] | Plasma | 34 | 14 | Up | - | 0.792 (0.649–0.897) | 2.2 | 67 | 93 | |
| miR-203 | [14] | Serum | 45 | 30 | Up | - | 0.710 (0.590–0.830) | - | - | - |
| [9] | Plasma | 34 | 14 | Up | - | 0.766 (0.620–0.877) | 3.3 | 64 | 93 | |
| miR-204 | [13] *** | Serum | 46 | 28 | Down | - | 1.000 (<0.0001) | - | 100 | 100 |
| [8] | Serum | Screening phase: 7 Validation phase: 26 | Screening phase: 20 Validation phase: 22 | Up | - | 0.740 (0.594–0.885) | - | - | - | |
| [17] | serum | Screening phase: 2 Testing phase: 21 Validation phase: 41 External validation: 30 | Screening phase: 1 Testing phase: 24 Validation phase: 48 External validation: 30 | Up | 0.668 (0.592–0.743) † | - | - | - | ||
| miR-205 [11] | Plasma | 12 | 12 | Up | - | 1.000 (1.000–1.000) | - | - | - | |
| miR-222 | [13] *** | Serum | 46 | 28 | Up | - | 0.720 (=0.002) | - | - | - |
| [8] | Serum | Screening phase: 7 Validation phase: 26 | Screening phase: 20 Validation phase: 22 | Up | - | 0.837 (0.726–0.948) | - | - | - | |
| miR-223 | [13] *** | Serum | 46 | 28 | Up | - | 0.880 (<0.0001) | - | - | - |
| [8] | Serum | Screening phase: 7 Validation phase: 26 | Screening phase: 20 Validation phase: 22 | Up | - | 0.727 (0.577–0.877) | - | - | - | |
| [10] | Plasma | Screening phase: 9 Validation phase: 31 | Screening phase: 20 Validation phase: 33 | Up | - | 0.768 (0.651–0.885) | - | 64.5 | 81.8 | |
| miR-301b [9] | Plasma | 34 | 14 | Down | - | 0.660 (0.507–0.792) | 2.3 | 55 | 86 | |
| miR-423-3p [17] | serum | Screening phase: 2 Testing phase: 21 Validation phase: 41 External validation: 30 | Screening phase: 1 Testing phase: 24 Validation phase: 48 External validation: 30 | Up | 0.689 (0.611–0.767) † | - | - | - | ||
| miR-449 [9] | Plasma | 34 | 14 | Up | - | 0.879 (0.750–0.956) | 5.5 | 91 | 86 | |
| miR-484 [17] | serum | Screening phase: 2 Testing phase: 21 Validation phase: 41 External validation: 30 | Screening phase: 1 Testing phase: 24 Validation phase: 48 External validation: 30 | Up | 0.644 (0.566–0.722) † | - | - | - | ||
| miR-887-5p [12] | Serum | Screening phase: 50 Validation phase: 20 | Screening phase: 50 Validation phase: 20 | Up | - | 0.729 (0.563–0.892) | - | 60 | 95 | |
| miR-1228 [9] | Plasma | 34 | 14 | Up | - | 0.890 (0.764–0.962) | 4 | 73 | 100 | |
| miR-1290 [9] | Plasma | 34 | 14 | Up | - | 0.773 (0.627–0.882) | 1.9 | 76 | 86 | |
| Association of miR | ||||||||||
| miR-222, miR-223, miR-186, miR-204 [8] | Serum | Screening phase: 7 Validation phase: 26 | Screening phase: 20 Validation phase: 22 | - | 0.927 (0.845–1.000) | - | 91.7 | 87.5 | ||
| miR-142-3p, miR-146a-5p, miR-151a-5p [19] **** | Plasma | Screening phase: 2 Testing phase: 22 Validation phase: 44 External validation: 27 | Screening phase: 1 Testing phase: 22 Validation phase: 34 External validation: 23 | 0.729 (0.580–0.879) | 0.751 (0.645–0.858) ± | 0.528 † | 62 † | 64.5† | ||
| miR-143-3p, miR-195-5p, miR-20b-5p, miR-204-5p, miR-423-3p, miR-484 [17] **** | serum | Screening phase: 2 Testing phase: 21 Validation phase: 41 External validation: 30 | Screening phase: 1 Testing phase: 24 Validation phase: 48 External validation: 30 | 0.748 (0.599–0.897) | 0.833 (0.745–0.921) ‡ | - | TP: 83.3 VP: 77.1 | TP: 66.7 VP: 82.9 | ||
| miR-9/miR-92a [9] | Plasma | 34 | 14 | - | 0.909 (0.789–0.973) | 0.89 | 73 | 100 | ||
| miR-9/miR-1229 [9] | Plasma | 34 | 14 | - | 0.913 (0.794–0.976) | 0.83 | 79 | 100 | ||
| miR-99a/miR-199b [7] | Plasma | 34 | 14 | - | 0.903 (0.780–0.970) | 0.73 | 88 | 93 | ||
| Association miR and Other Markers | ||||||||||
| miR-27a and CA 125 [10] | plasma | Screening phase: 9 Validation phase: 31 | Screening phase: 20 Validation phase: 33 | - | 0.894 (0.807–0.980) | - | 77.4 | 97 | ||
| Clinical and Prognostic Characteristic | Upregulated | Downregulated | NS |
|---|---|---|---|
| Histological Grade | |||
| G1 | [9]: miR-92a, miR-141, miR-200a, miR-203, miR-449a, miR-1228, miR-1290 [17]: miR-20b-5p, miR-143-3p, miR-195-5p, miR-204-5p, miR-423-3p, miR-484 | [9]: miR-9 | [9]: miR-301b |
| G2 | [17]: miR-20b-5p, miR-143-3p, miR-195-5p, miR-204-5p, miR-484 | [17]: miR-423-3p | |
| G3 | [17]: miR-20b-5p, miR-143-3p, miR-195-5p, miR-423-3p, miR-484 | [17]: miR-204-5p | |
| G2–G3 | [9]: miR-92a, miR-141, miR-200a, miR-449a, miR-1228, miR-1290 | [9]: miR-9 | [9]: miR-203, miR-301b |
| FIGO Stages | |||
| I | [17]: miR-20b-5p, miR-143-3p, miR-195-5p, miR-204-5p, miR-423-3p, miR-484 [13]: miR-186 *, miR-222 *, miR-223 * | [13]: miR-204 * | |
| II–IV | [17]: miR-20b-5p, miR-143-3p, miR-195-5p, miR-423-3p, miR-484 | [17]: miR-204-5p | |
| IA | [9]: miR-92a, miR-141, miR-203, miR-449a, miR-1228, miR-1290 [7]: miR-99a, miR-199b | [9]: miR-9 | [9]: miR-200a, miR-301b [7]: miR-100 |
| >IA | [9]: miR-92a, miR-141, miR-200a, miR-203, miR-449a, miR-1228, miR-1290 [7]: miR-99a, miR-100, miR-199b | [9]: miR-9 | [9]: miR-301b |
| miR | Histological Type | Histological Grade | Primitive Tumor Size | Myometrial Invasion | FIGO Stage | LNM | LVSI | Distant Metastasis | Average Survival Rate | |
|---|---|---|---|---|---|---|---|---|---|---|
| miR-9 [9] | - | X | - | NS | NS | - | - | - | - | |
| miR-21 [11] | - | X | - | - | X | - | - | - | - | |
| miR-27a [20] | X | NS | - | NS | NS | NS | NS | - | - | |
| miR-29b [15] | NS | NS | X | NS | X | X | - | - | X | |
| miR-30a-3[11] | - | NS | - | - | NS | - | - | - | - | |
| miR-92a [9] | - | NS | - | NS | NS | - | - | - | - | |
| miR-99a [7] | - | NS | - | NS | X | - | - | - | - | |
| miR-100 [7] | - | NS | - | NS | NS | - | - | - | - | |
| miR-135b [11] | - | NS | - | - | NS | - | - | - | - | |
| miR-141 [9] | - | NS | - | NS | NS | - | - | - | - | |
| miR-142-3p [19] | - | X | - | - | NS | - | - | - | - | |
| miR-146a-5p [19] | - | - | - | - | NS | - | - | - | - | |
| miR-150-5p [20] | NS | NS | - | NS | NS | NS | NS | - | - | |
| miR-151-5p [19] | - | - | - | - | NS | - | - | - | - | |
| miR-186 [13] | - | NS | - | - | - | - | - | - | - | |
| miR-199b [7] | - | NS | - | NS | NS | - | - | - | - | |
| miR-200a [9] | - | NS | - | NS | NS | - | - | - | - | |
| miR-203 | [14] | - | NS | - | - | NS | - | - | - | - |
| [9] | - | NS | - | NS | NS | - | - | - | - | |
| miR-205 [11] | - | NS | - | - | NS | - | - | - | - | |
| miR-222 [13] | - | NS | - | - | - | - | - | - | - | |
| miR-223 [13] | - | NS | - | - | - | - | - | - | - | |
| miR-301b [9] | - | NS | - | NS | NS | - | - | - | - | |
| miR-449a [9] | - | NS | - | NS | X | - | - | - | - | |
| miR-1228 [9] | - | NS | - | NS | NS | - | - | - | - | |
| miR-1290 [9] | - | NS | - | NS | NS | - | - | - | - | |
| Panel miR-200b/miR-200c/miR-203/miR-449a [9] | - | - | - | X | - | - | - | - | - | |
| Ref | Type of Sample | Conservation | Extraction | Micro-Array | qT-PCR |
|---|---|---|---|---|---|
| +6969.68/7 [7] | Plasma | −80 °C | mirVana Paris Kit (Ambion) | Precision nanoScript Reverse Transcription kit (Primer Design) | |
| [8] | Serum | −70 °C | TRIzol reagent (Invitrogen) | TaqMan microRNA RT kit and Megaplex RT primers (Invitrogen) | AMV reverse transcriptase (Takara Dalian, Liaoning, China) and the stem-loop RT primer (Applied Biosystems) |
| [9] | Plasma | −80 °C | mirVana Paris Kit (Ambion) | TaqMan MicroRNA Reverse Transcription Kit and specific primers (Applied Biosystems) | |
| [10] | Plasma | −80 °C | miRcute miRNA Isolation Kit | Sharpvue 26 Universal qPCR Master Mix High Rox kit (Biovue, Shanghai, China) and Sharpvue Human miRNA Primer Array kit (Biovue, Shanghai, China) | Sharpvue miRNA First Strand Kit (Biovue, Shanghai, China) |
| [11] | Plasma | −80 °C | mirVana Paris Kit (Ambion) | TaqMan MicroRNA Assays (Applied Biosystems) | |
| [12] | Serum | −80 °C | mirVana Paris Kit (Ambion) | Solexa sequencing | PrimeScript RT Reagent Kit et SYBR Premix Ex Taq Kit |
| [21] | Serum | - | miRNeasy Serum/Plasma Kit (Qiagen) | miScript II RT Kit and miScript SYBR Green PCR Kit (Qiagen) | |
| [13] | Serum | −80 °C | mirVana Paris Kit (Ambion) | TaqMan MicroRNA Assay | |
| [14] | Serum | −80 °C | mirVana PARIS Kit (Ambion) | TaqMan Advanced miRNA cDNA synthesis Kit | |
| [15] | Venous blood | - | RNA extraction kit (Shanghai LifeFeng Biotech Co.) | RNA reverse transcription kit (ThermoFisher Scientific) | |
| [16] | Serum | −20 °C | Norgen Total RNA Purification Kit | Human miRNA microarray chip analysis (Agilent-070156 Human) | Reaction mix |
| [17] | Serum | −80 °C | mirVana Paris Kit (Ambion) | Exiqon miRCURY-Ready-to-Use PCR-Human-panel- I+II-V1.M | Bulge-Loop™ miRNA qRT-PCR primer set |
| [18] | Plasma | −80 °C | miRNeasy Micro Kit (QIAgen) | QIAquick PCR Purification Kit (QIAgen) | KAPA Library Quantification Kit (KAPA Biosystems) |
| [19] | Plasma | −80 °C | mirVana Paris Kit (Ambion) | Exiqon miRCURY Ready-to-Use PCR-Human-panel- I+II-V1.M | Bulge-LoopTM miRNA qRT-PCR Primer Set |
| [20] | Serum | - | miRNeasy Micro Kit (QIAgen) | TaqMan MicroRNA Reverse Transcription Kit |
| Name of miR | Circulating miR Variation in EC Vs. Healthy Patients | miRNA-Cancer Data Base (dbDEMC) | |
|---|---|---|---|
| miR-9 [9] | Down | Up | |
| miR-15b [10] | Up | Up | |
| miR-20b-5p [17] | Up | Up | |
| miR-21 | [21] | Up (Up *) | Up |
| [11] | Down | ||
| miR-27a | [10] | Up | Up |
| [20] | Up | ||
| miR-29b | Located EC [15] | Down | Down |
| Metastatic EC [15] | Down | ||
| miR-30a-5p [11] | Down | Up | |
| miR-92a [9] | Up | Up | |
| miR-99a [7] | Up | Up | |
| miR-100 [7] | Up | Up | |
| miR-135b [11] | Up | Up | |
| miR-141 [9] | Up | Down | |
| miR-142-3p [19] | Up | Down | |
| miR-143-3p [17] | Up | Down | |
| miR-146a-5p [19] | Up | Up | |
| miR-150-5p [20] | Up | Down | |
| miR-151a-5p [19] | Up | Up | |
| miR-186 | [13] | Up | Down |
| [8] | Up | ||
| miR-195-5p [17] | Up | Down | |
| miR-199b [7] | Up | Down | |
| miR-200a [9] | Up | Down | |
| miR-203 | [14] | Up | Down |
| [9] | Up | ||
| miR-204 | [13] | Down | Down |
| [8] | Up | ||
| [17] | Up | ||
| miR-205 [11] | Up | Down | |
| miR-222 | [13] | Up | Up |
| [8] | Up | ||
| miR-223 | [13] | Up | Down |
| [8] | Up | ||
| [10] | Up | ||
| miR-301b [9] | Down | Up | |
| miR-423-3p [17] | Up | Up | |
| miR-449 [9] | Up | - | |
| miR-484 [17] | Up | Up | |
| miR-887-5p [12] | Up | - | |
| miR-1228 [9] | Up | - | |
| miR-1290 [9] | Up | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bloomfield, J.; Sabbah, M.; Castela, M.; Mehats, C.; Uzan, C.; Canlorbe, G. Clinical Value and Molecular Function of Circulating MicroRNAs in Endometrial Cancer Regulation: A Systematic Review. Cells 2022, 11, 1836. https://doi.org/10.3390/cells11111836
Bloomfield J, Sabbah M, Castela M, Mehats C, Uzan C, Canlorbe G. Clinical Value and Molecular Function of Circulating MicroRNAs in Endometrial Cancer Regulation: A Systematic Review. Cells. 2022; 11(11):1836. https://doi.org/10.3390/cells11111836
Chicago/Turabian StyleBloomfield, Joy, Michèle Sabbah, Mathieu Castela, Céline Mehats, Catherine Uzan, and Geoffroy Canlorbe. 2022. "Clinical Value and Molecular Function of Circulating MicroRNAs in Endometrial Cancer Regulation: A Systematic Review" Cells 11, no. 11: 1836. https://doi.org/10.3390/cells11111836