
Highly Correlated Recurrence Prognosis in Patients with Metastatic Colorectal Cancer by Synergistic Consideration of Circulating Tumor Cells/Microemboli and Tumor Markers CEA/CA19-9



Abstract
1. Introduction
2. Results
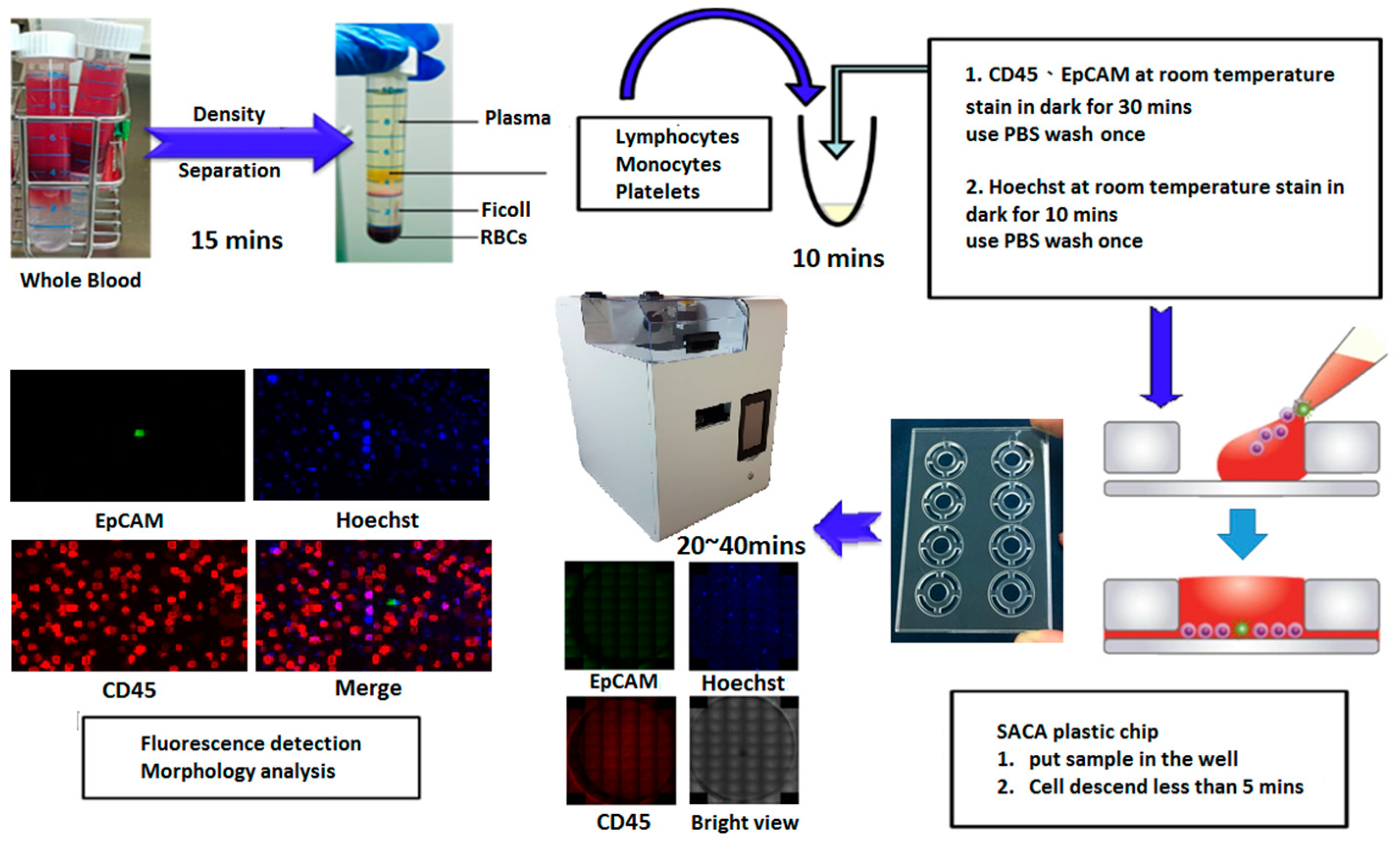
2.1. The Process for Preparing Clinical Samples
2.1.1. Identification and Detection of CTCs
2.1.2. Introduction of SACA Chip
2.1.3. Time Evaluation of Each Step for Colorectal Sample
2.1.4. Automatic Imaging Machine
2.2. CTC Phenotyping Analysis in Fluorescence Microscopy
2.2.1. Recovering Rate Analysis in SACA Chip by Spike-In Samples
2.2.2. Different Types of CTC Detected by the SACA Chip for CRC Patients
2.3. Affirmation in Clinical Samples
Patient Characteristics
2.4. Clinical Implications of CTCs, CTC Clusters, and CEA in Colorectal Cancer
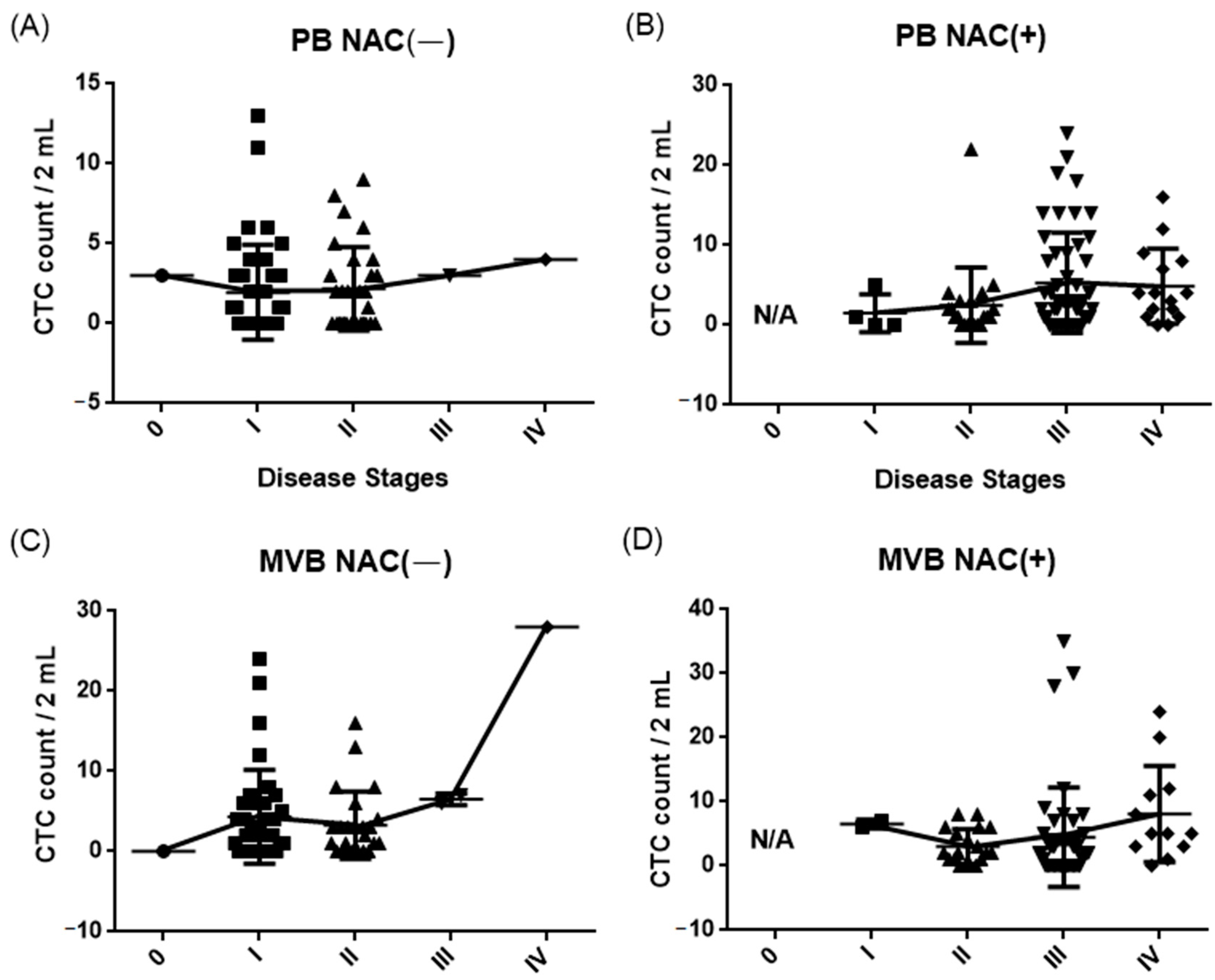
2.4.1. Results of CTC Detection by the SACA Chip
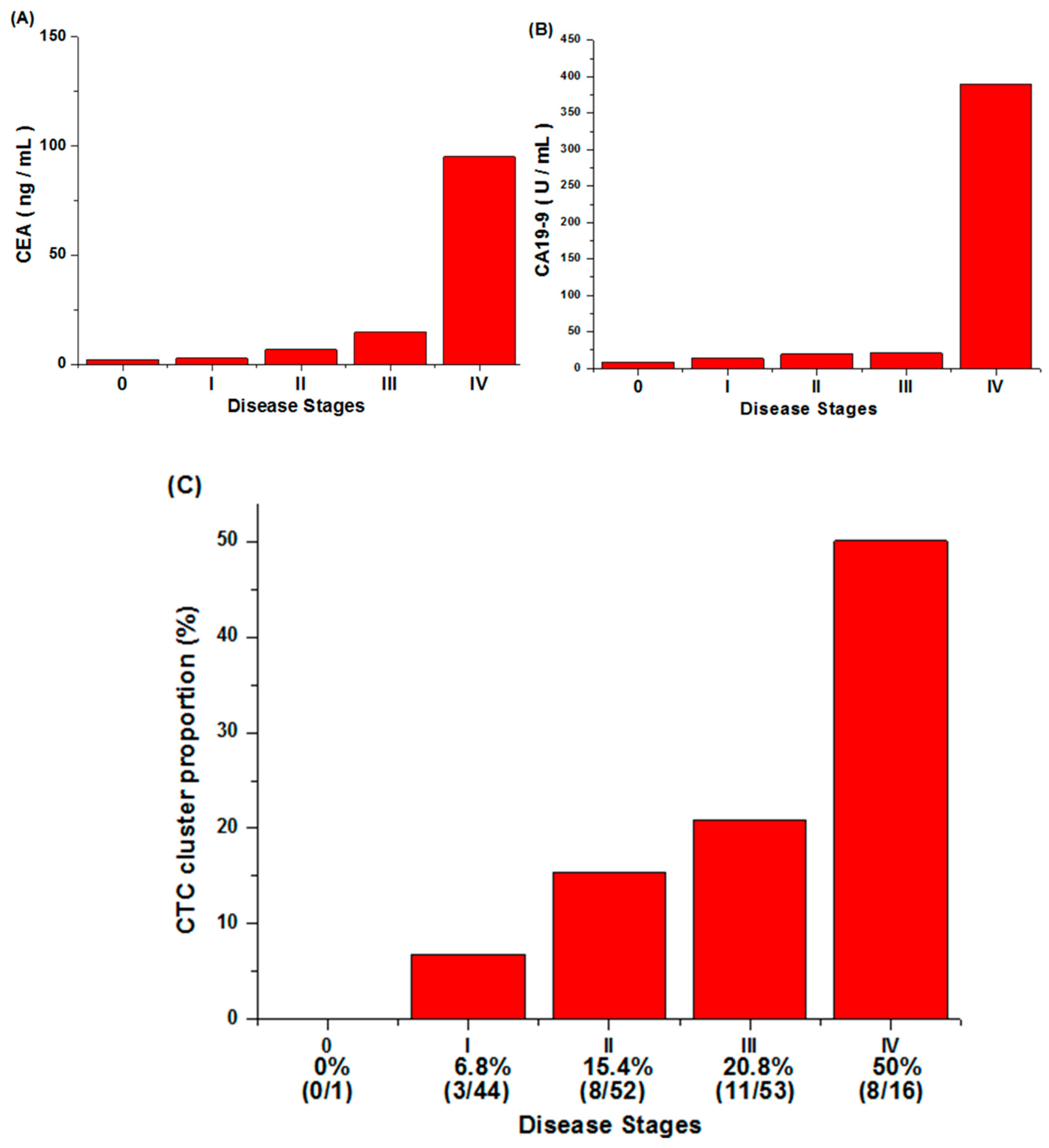
2.4.2. CEA, CA19-9 Value, and CTC Cluster Counts
2.5. Prediction of CRC Recurrence with CTCs, CTC Clusters, CEA, CA19-9, and Their Combination
2.5.1. Recurrence Rate and Odds Ratio Analysis
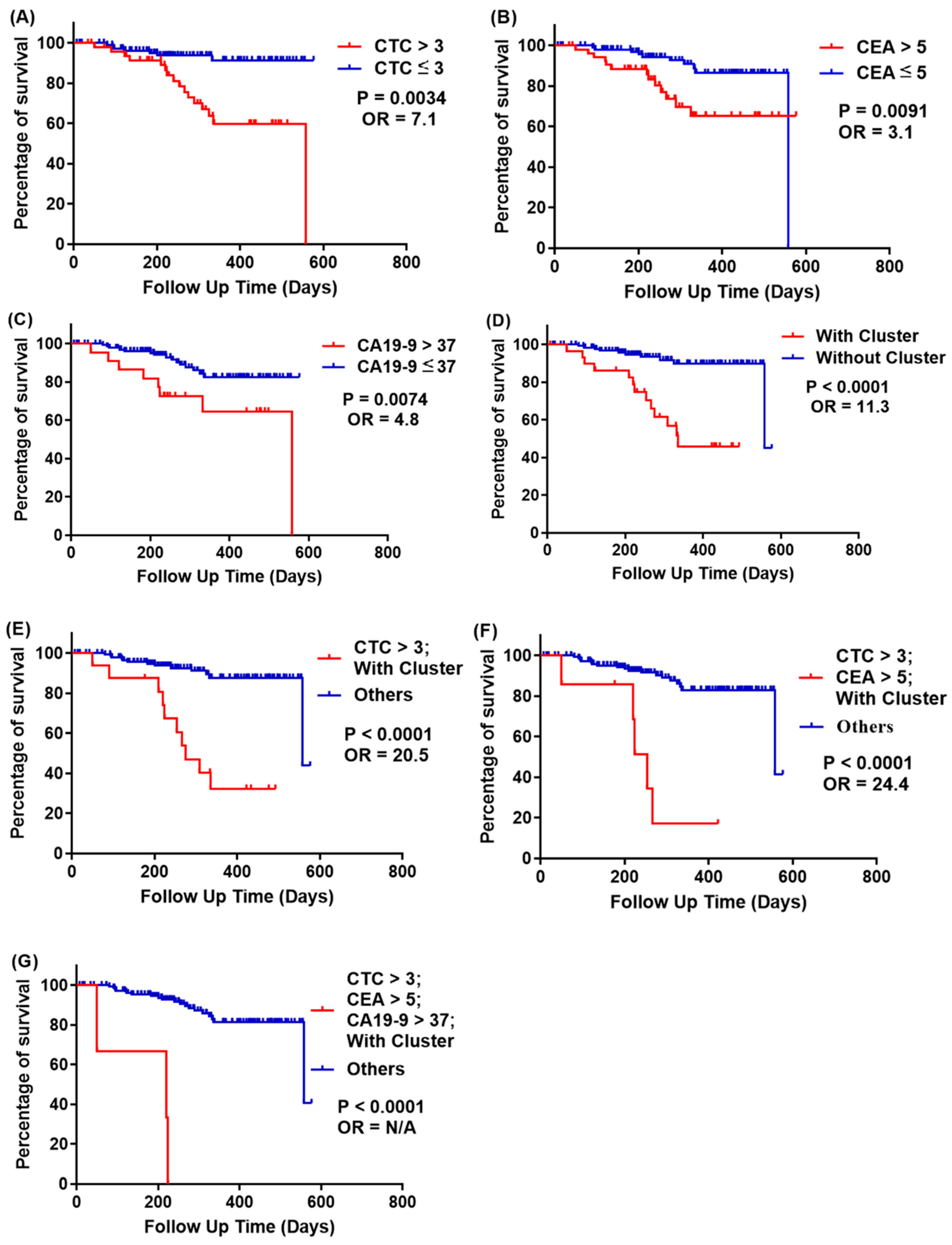
2.5.2. Survival Analysis
2.5.3. Prediction of CRC Recurrence at All Cancer Stages
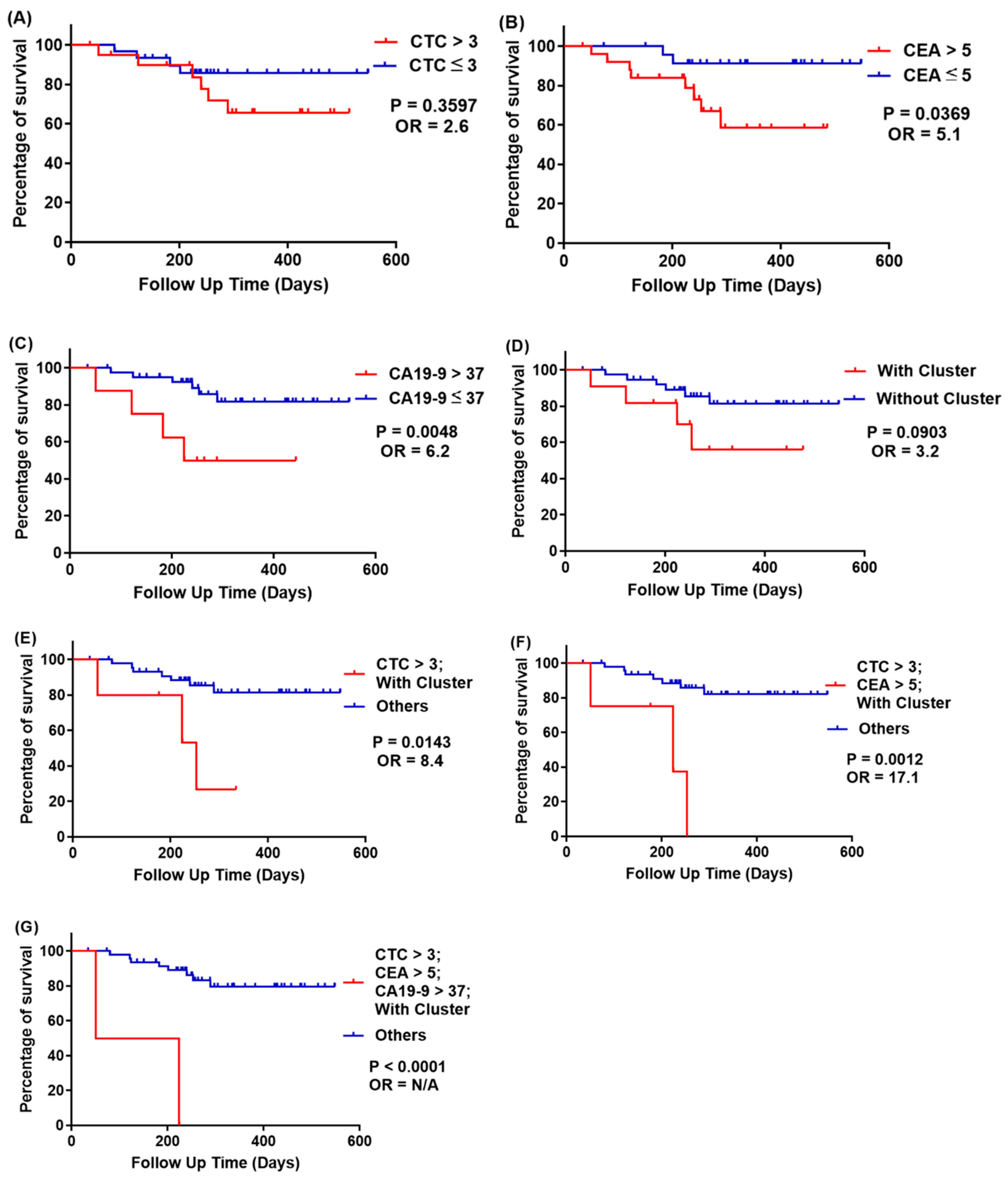
2.5.4. Prediction of Recurrence at Stage III CRC
3. Materials and Methods
3.1. Sample Resource
3.2. Cell Line Culture and Spike-In Testing
3.3. Statistical Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kochanek, K.D.; Murphy, S.L.; Xu, J.; Arias, E. Deaths: Final Data for 2017; DHHS Publication: Hyattsville, MD, USA, 2019. [Google Scholar]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Jemal, A.; Siegel, R.; Xu, J.; Ward, E. Cancer statistics, 2010. CA Cancer J. Clin. 2010, 60, 277–300. [Google Scholar] [CrossRef] [PubMed]
- Boursi, B.; Arber, N. Current and future clinical strategies in colon cancer prevention and the emerging role of chemoprevention. Curr. Pharm. Des. 2007, 13, 2274–2282. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Chang–Claude, J.; Jansen, L.; Knebel, P.; Stock, C.; Hoffmeister, M. Reduced risk of colorectal cancer up to 10 years after screening, surveillance, or diagnostic colonoscopy. Gastroenterology 2014, 146, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, F.L.; Dehdashti, F.; Ogunbiyi, O.A.; Kodner, I.J.; Siegel, B.A. Utility of FDG-PET for investigating unexplained plasma CEA elevation in patients with colorectal cancer. Ann. Surg. 1998, 227, 319. [Google Scholar] [CrossRef]
- Cutait, R.; Alves, V.A.; Lopes, L.C.; Cutait, D.E.; Borges, J.L.A.; Singer, J.; da Silva, J.H.; Goffi, F.S. Restaging of colorectal cancer based on the identification of lymph node micrometastases through immunoperoxidase staining of CEA and cytokeratins. Dis. Colon Rectum 1991, 34, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-C.; Yang, S.-H.; Lin, J.-K.; Lin, T.-C.; Chen, W.-S.; Jiang, J.-K.; Wang, H.-S.; Chang, S.-C. Is it reasonable to add preoperative serum level of CEA and CA19-9 to staging for colorectal cancer? J. Surg. Res. 2005, 124, 169–174. [Google Scholar] [CrossRef]
- Duffy, M.J. Carcinoembryonic antigen as a marker for colorectal cancer: Is it clinically useful? Clin. Chem. 2001, 47, 624–630. [Google Scholar] [CrossRef]
- Fakih, M.G.; Padmanabhan, A. CEA monitoring in colorectal cancer. Oncology 2006, 20, 579–587. [Google Scholar]
- Plaks, V.; Koopman, C.D.; Werb, Z. Circulating tumor cells. Science 2013, 341, 1186–1188. [Google Scholar] [CrossRef]
- Giuliano, M.; Shaikh, A.; Lo, H.C.; Arpino, G.; De Placido, S.; Zhang, X.H.; Cristofanilli, M.; Schiff, R.; Trivedi, M.V. Perspective on circulating tumor cell clusters: Why it takes a village to metastasize. Cancer Res. 2018, 78, 845–852. [Google Scholar] [CrossRef]
- Danila, D.C.; Heller, G.; Gignac, G.A.; Gonzalez-Espinoza, R.; Anand, A.; Tanaka, E.; Lilja, H.; Schwartz, L.; Larson, S.; Fleisher, M. Circulating tumor cell number and prognosis in progressive castration-resistant prostate cancer. Clin. Cancer Res. 2007, 13, 7053–7058. [Google Scholar] [CrossRef]
- Gazzaniga, P.; Gradilone, A.; De Berardinis, E.; Busetto, G.; Raimondi, C.; Gandini, O.; Nicolazzo, C.; Petracca, A.; Vincenzi, B.; Farcomeni, A. Prognostic value of circulating tumor cells in nonmuscle invasive bladder cancer: A CellSearch analysis. Ann. Oncol. 2012, 23, 2352–2356. [Google Scholar] [CrossRef]
- Rack, B.; Schindlbeck, C.; Andergassen, U.; Schneeweiss, A.; Zwingers, T.; Lichtenegger, W.; Beckmann, M.; Sommer, H.; Pantel, K.; Janni, W. Use of circulating tumor cells (CTC) in peripheral blood of breast cancer patients before and after adjuvant chemotherapy to predict risk for relapse: The SUCCESS trial. J. Clin. Oncol. 2010, 28, 1003. [Google Scholar] [CrossRef]
- Wang, F.-B.; Yang, X.-Q.; Yang, S.; Wang, B.-C.; Feng, M.-H.; Tu, J.-C. A higher number of circulating tumor cells (CTC) in peripheral blood indicates poor prognosis in prostate cancer patients--a meta-analysis. Asian Pac. J. Cancer. Prev. 2011, 12, 2629–2635. [Google Scholar] [PubMed]
- Chu, H.-Y.; Lu, L.-S.; Cho, W.; Wu, S.-Y.; Chang, Y.-C.; Lin, C.-P.; Yang, C.-Y.; Lin, C.-H.; Jiang, J.-K.; Tseng, F.-G. Enumerating circulating tumor cells with a Self-Assembled Cell Array (SACA) Chip: A feasibility study in patients with colorectal cancer. Cancers 2019, 11, 56. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.J.; Ewald, A.J. A collective route to metastasis: Seeding by tumor cell clusters. Science 2016, 352, 167–169. [Google Scholar] [CrossRef]
- Fabisiewicz, A.; Grzybowska, E. CTC clusters in cancer progression and metastasis. Med. Oncol. 2017, 34, 12. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Mu, Z.; Chervoneva, I.; Austin, L.; Ye, Z.; Rossi, G.; Palazzo, J.P.; Sun, C.; Abu-Khalaf, M.; Myers, R.E. Longitudinally collected CTCs and CTC-clusters and clinical outcomes of metastatic breast cancer. Breast Cancer Res. Treat. 2017, 161, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Aceto, N.; Bardia, A.; Miyamoto, D.T.; Donaldson, M.C.; Wittner, B.S.; Spencer, J.A.; Yu, M.; Pely, A.; Engstrom, A.; Zhu, H. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell 2014, 158, 1110–1122. [Google Scholar] [CrossRef] [PubMed]
- Sastre, J.; Maestro, M.; Puente, J.; Veganzones, S.; Alfonso, R.; Rafael, S.; Garcia-Saenz, J.; Vidaurreta, M.; Martin, M.; Arroyo, M. Circulating tumor cells in colorectal cancer: Correlation with clinical and pathological variables. Ann. Oncol. 2008, 19, 935–938. [Google Scholar] [CrossRef]
- Stott, S.L.; Hsu, C.-H.; Tsukrov, D.I.; Yu, M.; Miyamoto, D.T.; Waltman, B.A.; Rothenberg, S.M.; Shah, A.M.; Smas, M.E.; Korir, G.K. Isolation of circulating tumor cells using a microvortex-generating herringbone-chip. Proc. Natl. Acad. Sci. USA 2010, 107, 18392–18397. [Google Scholar] [CrossRef]
- Martin, V.; Siewert, C.; Scharl, A.; Harms, T.; Heinze, R.; Ohl, S.; Radbruch, A.; Miltenyi, S.; Schmitz, J. Immunomagnetic enrichment of disseminated epithelial tumor cells from peripheral blood by MACS. Exp. Hematol. 1998, 26, 252–264. [Google Scholar]
- Shi, G.; Cui, W.; Benchimol, M.; Liu, Y.-T.; Mattrey, R.F.; Mukthavaram, R.; Kesari, S.; Esener, S.C.; Simberg, D. Isolation of rare tumor cells from blood cells with buoyant immuno-microbubbles. PLoS ONE 2013, 8, e58017. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.J.; Kim, T.H.; Zhang, Z.; Azizi, E.; Pham, T.M.; Paoletti, C.; Lin, J.; Ramnath, N.; Wicha, M.S.; Hayes, D.F. Sensitive capture of circulating tumour cells by functionalized graphene oxide nanosheets. Nat. Nanotechnol. 2013, 8, 735. [Google Scholar] [CrossRef] [PubMed]
- Andree, K.C.; van Dalum, G.; Terstappen, L.W. Challenges in circulating tumor cell detection by the CellSearch system. Mol. Oncol. 2016, 10, 395–407. [Google Scholar] [CrossRef] [PubMed]
- Müller, V.; Riethdorf, S.; Rack, B.; Janni, W.; Fasching, P.A.; Solomayer, E.; Aktas, B.; Kasimir-Bauer, S.; Pantel, K.; Fehm, T. Prognostic impact of circulating tumor cells assessed with the CellSearch System™ and AdnaTest Breast™ in metastatic breast cancer patients: The DETECT study. Breast Cancer Res. 2012, 14, R118. [Google Scholar] [CrossRef]
- Riethdorf, S.; Fritsche, H.; Müller, V.; Rau, T.; Schindlbeck, C.; Rack, B.; Janni, W.; Coith, C.; Beck, K.; Jänicke, F. Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: A validation study of the CellSearch system. Clin. Cancer Res. 2007, 13, 920–928. [Google Scholar] [CrossRef]
- Van der Auwera, I.; Peeters, D.; Benoy, I.; Elst, H.; Van Laere, S.; Prove, A.; Maes, H.; Huget, P.; Van Dam, P.; Vermeulen, P. Circulating tumour cell detection: A direct comparison between the CellSearch System, the AdnaTest and CK-19/mammaglobin RT–PCR in patients with metastatic breast cancer. Br. J. Cancer 2010, 102, 276–284. [Google Scholar] [CrossRef]
- Chen, T.-J.; Wu, J.-K.; Chang, Y.-C.; Fu, C.-Y.; Wang, T.-P.; Lin, C.-Y.; Chang, H.-Y.; Chieng, C.-C.; Tzeng, C.-Y.; Tseng, F.-G. High-efficiency rare cell identification on a high-density self-assembled cell arrangement chip. Biomicrofluidics 2014, 8, 036501. [Google Scholar] [CrossRef]
- Cho, W.; Weng, Y.H.; Chen, H.Y.; Chu, H.Y.; Chiou, T.-J.; Lin, C.P.; Jiang, J.-K.; Yang, C.-Y.; Tseng, F.G. CTCs detection by SACA chip and image analysis. In Proceedings of the 2017 IEEE 12th International Conference on Nano/Micro Engineered and Molecular Systems (NEMS), Los Angeles, CA, USA, 9–12 April 2017; pp. 360–363. [Google Scholar]
- Hoo, Z.H.; Candlish, J.; Teare, D. What is an ROC curve? Emerg. Med. J. 2016, 34, 349–356. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (A) Peripheral Vein Blood (PB) | ||
| Characteristics | Patients (n) | Percentage (%) |
| Age (years) | ||
| <60 | 58 | 35.60% |
| ≥60 | 105 | 64.40% |
| Sex | ||
| Male | 105 | 64.40% |
| Female | 58 | 35.60% |
| T status | ||
| T0-T2 | 57 | 35% |
| T3-T4 | 106 | 65% |
| (B) Mesenteric Vein Blood (MVB) | ||
| Characteristics | Patients (n) | Percentage (%) |
| Age (years) | ||
| <60 | 52 | 36.90% |
| ≥60 | 89 | 63.10% |
| Sex | Sex | |
| Male | 92 | 65.20% |
| Female | 49 | 34.80% |
| T status | ||
| T0–T2 | 50 | 35.50% |
| T3–T4 | 91 | 64.50% |
| (C) All patients | ||
| Characteristics | Patients (n) | Percentage (%) |
| Lymph Node Metastasis | ||
| Negative | 101 | 60.80% |
| Positive | 65 | 39.10% |
| Preoperative Serum CEA | ||
| ≤5 ng/mL | 55 | 33.10% |
| >5 ng/mL | 111 | 66.90% |
| Preoperative Serum CA19-9 | ||
| <37 U/mL | 143 | 86.10% |
| ≥37 U/mL | 23 | 13.90% |
| (A) CTC Count in 2 mL PB Blood | |||||||||||||
| NAC (−) | NAC (+) | ||||||||||||
| Disease Stages | No. of Cases | Range | Mean | Median | SD | Mode | Disease Stages | No. of Cases | Range | Mean | Median | SD | Mode |
| 0 | 1 | N/A | 3 | N/A | N/A | N/A | 0 | 0 | N/A | N/A | N/A | N/A | N/A |
| I | 40 | 0–13 | 1.95 | 1 | 2.94 | 0 | I | 4 | 0–5 | 1.5 | 0.5 | 2.06 | 0 |
| II | 30 | 0–9 | 2.17 | 2 | 2.27 | 0 | II | 21 | 0–22 | 2.48 | 1 | 4.61 | 0 |
| III | 1 | N/A | 3 | N/A | N/A | N/A | III | 50 | 0–24 | 5.28 | 3 | 6.22 | 0 |
| IV | 1 | N/A | 4 | N/A | N/A | N/A | IV | 15 | 0–16 | 4.87 | 4 | 4.51 | 4 |
| (B) CTC Count in 2 mL MVB Blood | |||||||||||||
| NAC (−) | NAC (+) | ||||||||||||
| Disease Stages | No. of Cases | Range | Mean | Median | SD | Mode | Disease Stages | No. of Cases | Range | Mean | Median | SD | Mode |
| 0 | 1 | N/A | 0 | N/A | N/A | N/A | 0 | 0 | N/A | N/A | N/A | N/A | N/A |
| I | 35 | 0–24 | 4.31 | 2 | 5.76 | 0 | I | 2 | 6–7 | 6.5 | 6.5 | 0.5 | N/A |
| II | 25 | 6–7 | 3.16 | 2 | 4.09 | 0 | II | 18 | 0–8 | 2.72 | 2 | 2.45 | 2 |
| III | 2 | 0–17 | 6.5 | 6.5 | 0.5 | N/A | III | 45 | 0–35 | 4.44 | 2 | 7.69 | 0 |
| IV | 1 | N/A | 28 | N/A | N/A | N/A | IV | 12 | 0–24 | 8.08 | 5 | 7.16 | 5 |
| All Cancer Stages (163 Cases) | No. of Cases | |||
|---|---|---|---|---|
| CTCs per 2 mL Blood | Recurrence | No Recurrence | Recurrence Rate | (Odds Ratio, OR) |
| CTCs > 3 | 16 | 34 | 32% | 7.1 |
| CTCs ≤ 3 | 7 | 106 | 6.2% | |
| CEA > 5 | 13 | 41 | 24% | 3.1 |
| CEA ≤ 5 | 10 | 99 | 9.2% | |
| CA19-9 > 37 | 8 | 14 | 36.4% | 4.8 |
| CA19-9 ≤ 37 | 15 | 126 | 10.6% | |
| With CTC clusters | 14 | 17 | 45.2% | 11.3 |
| Without CTC clusters | 9 | 123 | 6.8% | |
| CTCs > 3; CEA > 5 | 10 | 12 | 45.5% | 8.2 |
| Others | 13 | 128 | 9.2% | |
| CTCs > 3; CA19-9 > 37 | 4 | 3 | 57.1% | 9.6 |
| Others | 19 | 137 | 12.8% | |
| CTCs > 3; With CTC clusters | 11 | 6 | 64.7% | 20.5 |
| Others | 12 | 134 | 8.2% | |
| CEA > 5; CA19-9 > 37 | 5 | 7 | 41.7% | 5.3 |
| Others | 18 | 133 | 11.9% | |
| CEA > 5; With CTC clusters | 7 | 8 | 46.7% | 7.2 |
| Others | 16 | 132 | 10.8% | |
| CA19-9 > 37; With CTC clusters | 5 | 4 | 55.6% | 9.4 |
| Others | 18 | 136 | 11.7% | |
| CTCs > 3; CEA > 5; CA19-9 > 37 | 3 | 1 | 75% | 20.9 |
| Others | 20 | 139 | 12.8% | |
| CTCs > 3; CEA > 5; With CTC clusters | 6 | 2 | 75% | 24.4 |
| Others | 17 | 138 | 11% | |
| CTCs > 3; CA19-9 > 37; With CTC clusters | 1 | 1 | 50% | 6.3 |
| Others | 22 | 139 | 13.7% | |
| CEA > 5; CA19-9 > 37; With CTC clusters | 3 | 3 | 50% | 6.9 |
| Others | 20 | 137 | 12.7% | |
| CTCs > 3; CEA > 5; CA19-9 > 37; With CTC clusters | 3 | 0 | 100% | N/A |
| Others | 20 | 140 | 12.5% | |
| Stage III CRC (51 Cases) | No. of Cases | |||
|---|---|---|---|---|
| Recurrence | No Recurrence | Recurrence Rate | (Odds Ratio, OR) | |
| CTCs > 3 | 6 | 4 | 28.6% | 2.6 |
| CTCs ≤ 3 | 15 | 26 | 13.3% | |
| CEA > 5 | 8 | 18 | 30.8% | 5.1 |
| CEA ≤ 5 | 2 | 23 | 8% | |
| CA19-9 > 37 | 4 | 4 | 50% | 6.2 |
| CA19-9 ≤ 37 | 6 | 37 | 14% | |
| With CTC clusters | 4 | 7 | 36.4% | 3.2 |
| Without CTC clusters | 6 | 34 | 15% | |
| CTCs > 3; CEA > 5 | 6 | 7 | 46.2% | 7.3 |
| Others | 4 | 34 | 10.5% | |
| CTCs > 3; CA19-9 > 37 | 2 | 0 | 100% | N/A |
| Others | 8 | 41 | 16.3% | |
| CTCs > 3; With CTC clusters | 3 | 2 | 60% | 8.4 |
| Others | 7 | 39 | 15.2% | |
| CEA > 5; CA19-9 > 37 | 3 | 3 | 50% | 5.4 |
| Others | 7 | 38 | 15.6% | |
| CEA > 5; With CTC clusters | 4 | 5 | 44.4% | 4.8 |
| Others | 6 | 36 | 14.3% | |
| CA19-9 > 37; With CTC clusters | 3 | 3 | 50% | 5.4 |
| Others | 7 | 38 | 15.6% | |
| CTCs > 3; CEA > 5; CA19-9 > 37 | 2 | 0 | 100% | N/A |
| Others | 8 | 41 | 16.3% | |
| CTCs > 3; CEA > 5; With CTC clusters | 3 | 1 | 75% | 17.1 |
| Others | 7 | 40 | 14.9% | |
| CTCs > 3; CA19-9 > 37; With CTC clusters | 2 | 0 | 100% | N/A |
| Others | 8 | 41 | 16.3% | |
| CEA > 5; CA19-9 > 37; With CTC clusters | 3 | 3 | 50% | 5.4 |
| Others | 7 | 38 | 15.6% | |
| CTCs > 3; CEA > 5; CA19-9 > 37; With CTC clusters | 2 | 0 | 100% | N/A |
| Others | 8 | 41 | 16.3% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, H.-Y.; Yang, C.-Y.; Yeh, P.-H.; Hsu, C.-J.; Chang, L.-W.; Chan, W.-J.; Lin, C.-P.; Lyu, Y.-Y.; Wu, W.-C.; Lee, C.-W.; et al. Highly Correlated Recurrence Prognosis in Patients with Metastatic Colorectal Cancer by Synergistic Consideration of Circulating Tumor Cells/Microemboli and Tumor Markers CEA/CA19-9. Cells 2021, 10, 1149. https://doi.org/10.3390/cells10051149
Chu H-Y, Yang C-Y, Yeh P-H, Hsu C-J, Chang L-W, Chan W-J, Lin C-P, Lyu Y-Y, Wu W-C, Lee C-W, et al. Highly Correlated Recurrence Prognosis in Patients with Metastatic Colorectal Cancer by Synergistic Consideration of Circulating Tumor Cells/Microemboli and Tumor Markers CEA/CA19-9. Cells. 2021; 10(5):1149. https://doi.org/10.3390/cells10051149
Chicago/Turabian StyleChu, Hsueh-Yao, Chih-Yung Yang, Ping-Hao Yeh, Chun-Jieh Hsu, Lu-Wei Chang, Wei-Jen Chan, Chien-Ping Lin, You-You Lyu, Wei-Cheng Wu, Chun-Wei Lee, and et al. 2021. "Highly Correlated Recurrence Prognosis in Patients with Metastatic Colorectal Cancer by Synergistic Consideration of Circulating Tumor Cells/Microemboli and Tumor Markers CEA/CA19-9" Cells 10, no. 5: 1149. https://doi.org/10.3390/cells10051149
APA StyleChu, H.-Y., Yang, C.-Y., Yeh, P.-H., Hsu, C.-J., Chang, L.-W., Chan, W.-J., Lin, C.-P., Lyu, Y.-Y., Wu, W.-C., Lee, C.-W., Wu, J.-K., Jiang, J.-K., & Tseng, F.-G. (2021). Highly Correlated Recurrence Prognosis in Patients with Metastatic Colorectal Cancer by Synergistic Consideration of Circulating Tumor Cells/Microemboli and Tumor Markers CEA/CA19-9. Cells, 10(5), 1149. https://doi.org/10.3390/cells10051149