
Remineralization Effects of Zinc-Containing Glass Ionomer Cement Restoratives on Demineralized Enamel Under pH Cycling Conditions




Abstract
1. Introduction
2. Materials and Methods
2.1. Specimen Preparation
2.2. WSL Formation
2.3. Reagent Application Protocols
- Group 1 (control): No treatment;
- Group 2 (cGIC): FujiIX treatment;
- Group 3 (zGIC): Caredyne Restore treatment.
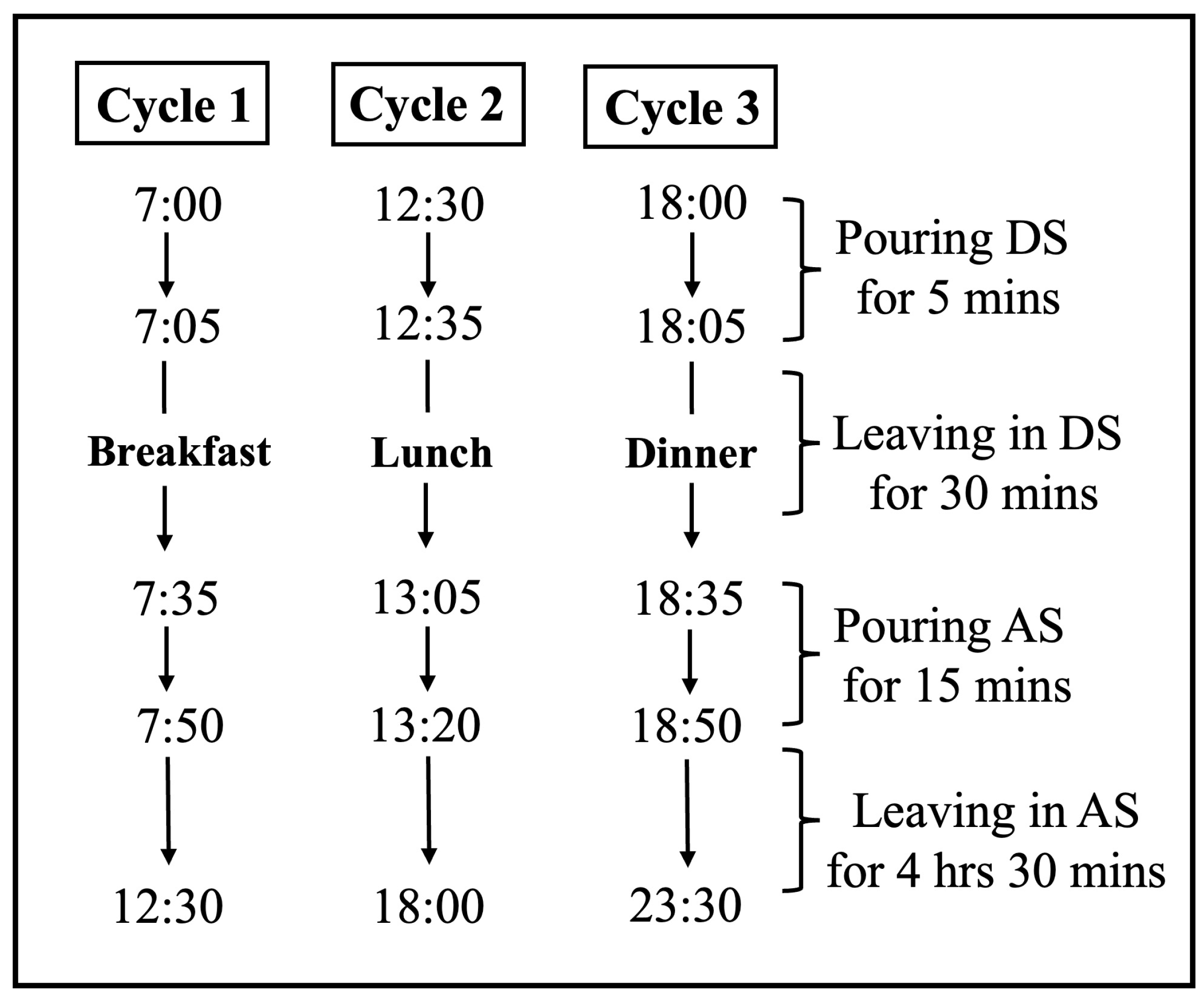
2.4. pH Cycling Condition
2.5. μCT Scanning
2.6. SEM
2.7. Statistical Analysis
3. Results
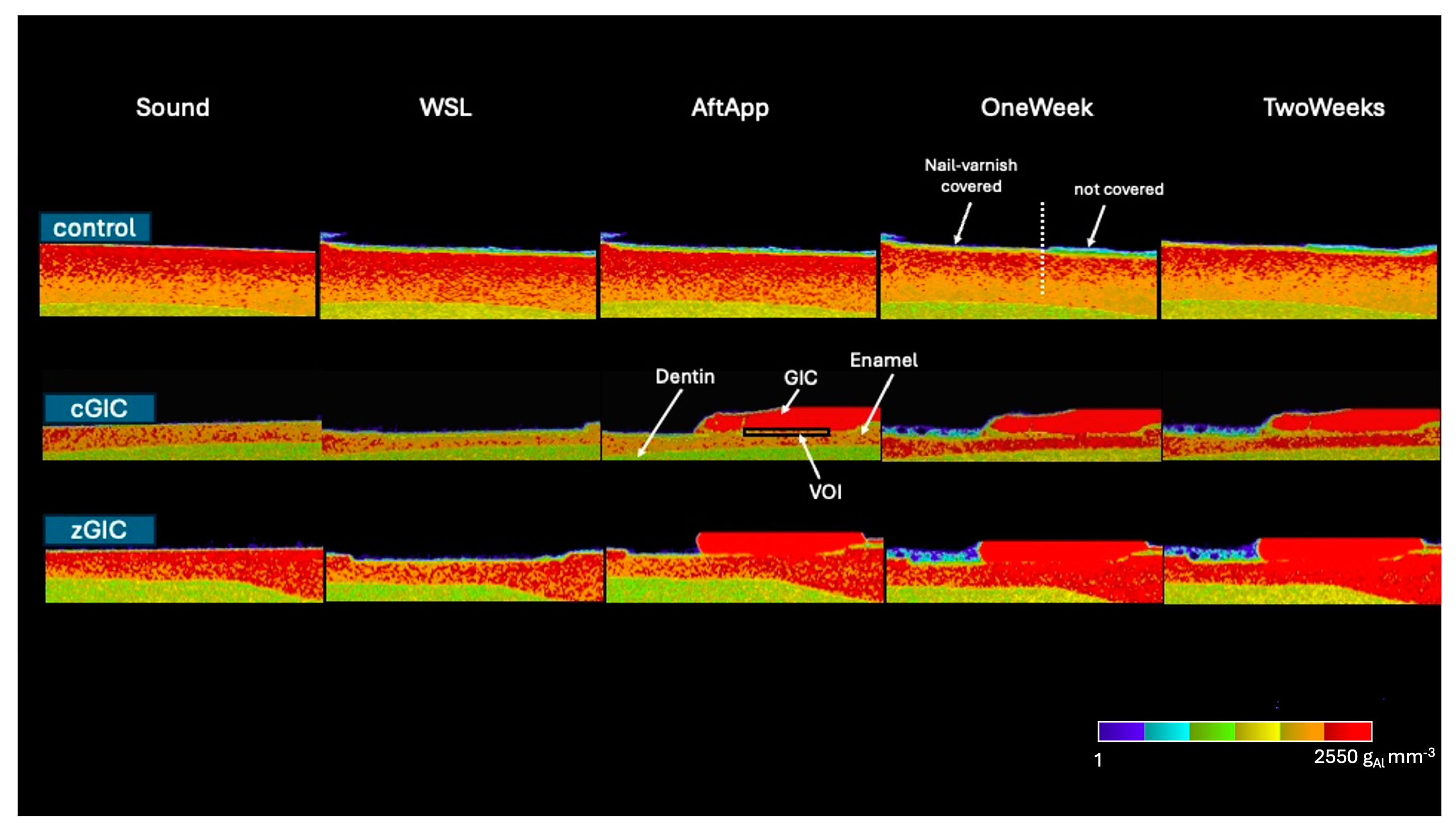
3.1. μCT Analysis
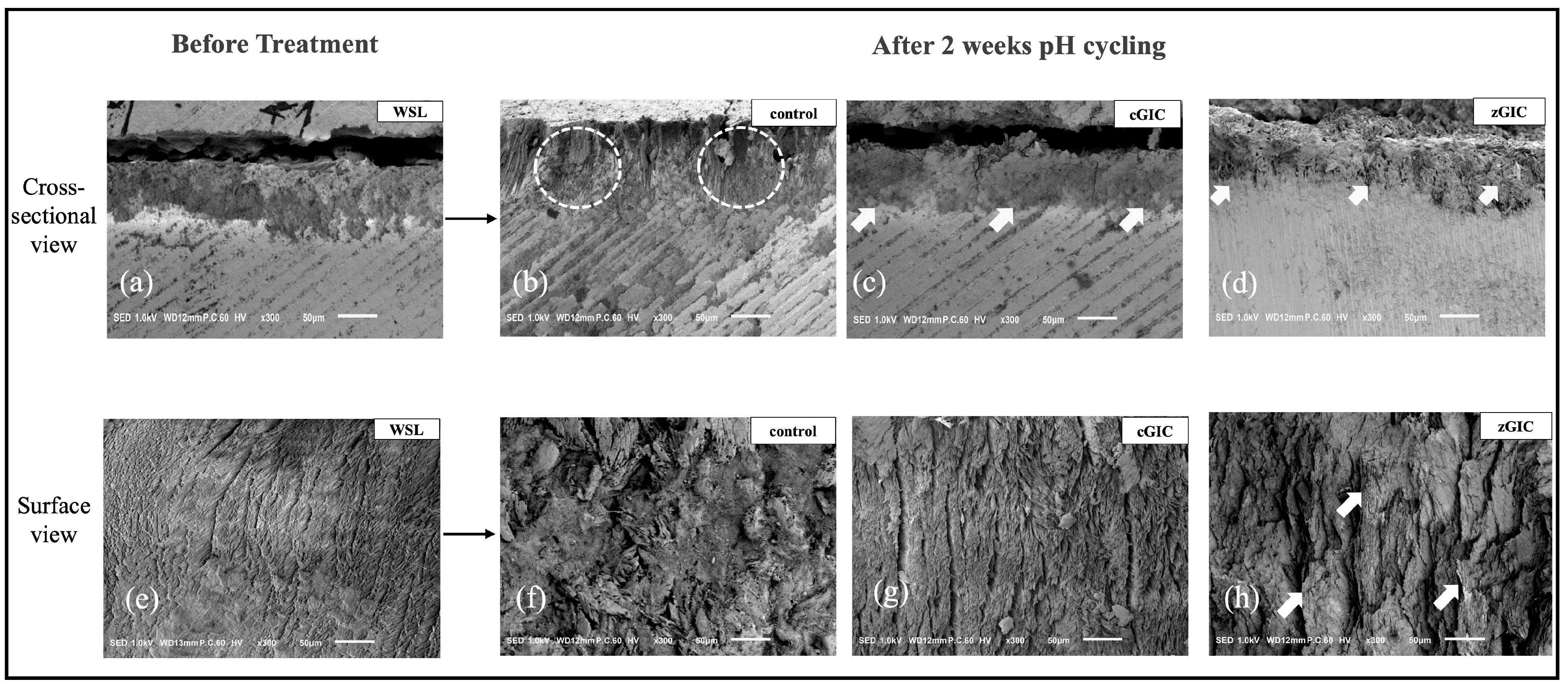
3.2. SEM Observations
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Huang, T.T.; Jones, A.S.; He, L.H.; Darendeliler, M.A.; Swain, M.V. Characterisation of enamel white spot lesions using X-ray micro-tomography. J. Dent. 2007, 35, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Aoba, T. Solubility properties of human tooth mineral and pathogenesis of dental caries. Oral Dis. 2004, 10, 249–257. [Google Scholar] [CrossRef]
- Ruan, Q.; Moradian-Oldak, J. Amelogenin and enamel biomimetics. J. Mater. Chem. B 2015, 3, 3112–3129. [Google Scholar] [CrossRef]
- Featherstone, J.D. The science and practice of caries prevention. J. Am. Dent. Assoc. 2000, 131, 887–899. [Google Scholar] [CrossRef] [PubMed]
- Kidd, E.A.M.; Fejerskov, O. What Consitututes Dental Caries? What Constitutes Dental Caries? Histopathology of Carious Enamel and Dentin Related to the Action of Cariogenic Biofilms. J. Dent. Res. 2004, 83, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Fan, Y.; Zhou, Z.; Tu, H.; Li, D.; Lv, X.; Ding, L.; Zhang, L. Promotion of enamel caries remineralization by an amelogenin-derived peptide in a rat model. Arch. Oral Biol. 2017, 73, 66–71. [Google Scholar] [CrossRef]
- Cassiano, L.; Pessan, J.; Comar, L.; Levy, F.; Cardoso, C.; Dionisio, A.; Manarelli, M.; Grizzo, L.; Magalhães, A.C.; Buzalaf, M. Frequency of intake and amount of fluoride in milk for remineralisation of artificial caries on enamel and dentine: Ex vivo/in situ study. Arch. Oral Biol. 2017, 73, 136–141. [Google Scholar] [CrossRef]
- Reynolds, E.C.; Cai, F.; Cochrane, N.J.; Shen, P.; Walker, G.D.; Morgan, M.V.; Reynolds, C. Fluoride and Casein Phosphopeptide-Amorphous Calcium Phosphate. J. Dent. Res. 2008, 87, 344–348. [Google Scholar] [CrossRef]
- Bayne, S.C.; Ferracane, J.L.; Marshall, G.W.; Marshall, S.J.; van Noort, R. The Evolution of Dental Materials over the Past Century: Silver and Gold to Tooth Color and Beyond. J. Dent. Res. 2019, 98, 257–265. [Google Scholar] [CrossRef]
- Cramer, N.; Stansbury, J.; Bowman, C. Recent Advances and Developments in Composite Dental Restorative Materials. J. Dent. Res. 2011, 90, 402–416. [Google Scholar] [CrossRef]
- Chen, X.; Inoue, G.; Ikeda, M.; Sadr, A.; Shimada, Y. Time-dependent structural changes and hypermineralisation of artificially demineralised dentine following treatment with silver diammine fluoride and glass ionomer cement. J. Dent. 2023, 131, 104452. [Google Scholar] [CrossRef] [PubMed]
- Farooq, I.; Bugshan, A. The role of salivary contents and modern technologies in the remineralization of dental enamel: A review. F1000Res 2020, 9, 171. [Google Scholar] [CrossRef] [PubMed]
- Hafshejani, T.M.; Zamanian, A.; Venugopal, J.R.; Rezvani, Z.; Sefat, F.; Saeb, M.R.; Vahabi, H.; Zarrintaj, P.; Mozafari, M. Antibacterial glass-ionomer cement restorative materials: A critical review on the current status of extended release formulations. J. Control. Release 2017, 262, 317–328. [Google Scholar] [CrossRef]
- Imataki, R.; Shinonaga, Y.; Nishimura, T.; Abe, Y.; Arita, K. Mechanical and Functional Properties of a Novel Apatite-Ionomer Cement for Prevention and Remineralization of Dental Caries. Materials 2019, 12, 3998. [Google Scholar] [CrossRef]
- Diefenderfer, C.E.K. Caries remineralization therapy: Implication for dental readiness. Mil. Med. 2008, 173, 48–50. [Google Scholar] [PubMed]
- Abdulkareem, F.A.; Alwaheb, A. The effect of Zinc Oxide nanoparticles with sodium fluoride in remineralization of enamel caries. Bionatura 2023, 8, 1–11. [Google Scholar] [CrossRef]
- Takatsuka, T.; Tanaka, K.; Iijima, Y. Inhibition of dentine demineralization by zinc oxide: In vitro and in situ studies. Dent. Mater. 2005, 21, 1170–1177. [Google Scholar] [CrossRef]
- Oh, S.; Jung, H.-S.; Kim, H.-J.; Jang, J.-H.; Kim, D.-S.; Choi, K.-K.; Kim, S.-Y. Effect of zinc on the collagen degradation in acid-etched dentin. J. Dent. Sci. 2018, 13, 97–102. [Google Scholar] [CrossRef]
- Toledano, M.; Yamauti, M.; Osorio, E.; Osorio, R. Zinc-Inhibited MMP-Mediated Collagen Degradation after Different Dentine Demineralization Procedures. Caries Res. 2012, 46, 201–207. [Google Scholar] [CrossRef]
- Hasegawa, T.; Takenaka, S.; Ohsumi, T.; Ida, T.; Ohshima, H.; Terao, Y.; Naksagoon, T.; Maeda, T.; Noiri, Y. Effect of a novel glass ionomer cement containing fluoro-zinc-silicate fillers on biofilm formation and dentin ion incorporation. Clin. Oral Investig. 2020, 24, 963–970. [Google Scholar] [CrossRef]
- Liu, Y.; Kohno, T.; Tsuboi, R.; Kitagawa, H.; Imazato, S. Acidity-induced release of zinc ion from BioUnionTM filler and its inhibitory effects against Streptococcus mutans. Dent. Mater. J. 2020, 39, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Noach, N.; Lavy, E.; Reifen, R.; Friedman, M.; Kirmayer, D.; Zelinger, E.; Ritter, A.; Yaniv, D.; Reifen, E. Zinc chloride is effective as an antibiotic in biofilm prevention following septoplasty. Sci. Rep. 2023, 13, 1–12. [Google Scholar] [CrossRef]
- Chen, X.; Inoue, G.; Fan, L.; Sekizawa, O.; Nitta, K.; Ikeda, M.; Shimada, Y. Enhancement of mineral density and mechanical properties in root caries treated with silver diammine fluoride and glass ionomer cement, with emphasis on silver ion distribution. J. Dent. 2024, 146, 105041. [Google Scholar] [CrossRef]
- Cate, J.M.T. pH-cycling of enamel and dentin lesions in the presence of low concentrations of fluoride. Eur. J. Oral. Sci. 1995, 103, 362–367. [Google Scholar] [PubMed]
- Matsuda, Y.; Komatsu, H.; Murata, Y.; Tanaka, T.; Sano, H. A Newly Designed Automatic pH-cycling System to Simulate Daily pH Fluctuations. Dent. Mater. J. 2006, 25, 280–285. [Google Scholar]
- Hamba, H.; Nikaido, T.; Sadr, A.; Nakashima, S.; Tagami, J. Enamel Lesion Parameter Correlations between Polychromatic Micro-CT and TMR. J. Dent. Res. 2012, 91, 586–591. [Google Scholar] [CrossRef]
- Hamba, H.; Nikaido, T.; Inoue, G.; Sadr, A.; Tagami, J. Effects of CPP-ACP with sodium fluoride on inhibition of bovine enamel demineralization: A quantitative assessment using micro-computed tomography. J. Dent. 2011, 39, 405–413. [Google Scholar] [CrossRef] [PubMed]
- De Rooij, J.; Nancollas, G. The Formation and Remineralization of Artificial White Spot Lesions: A Constant Composition Approach. J. Dent. Res. 1984, 63, 864–867. [Google Scholar]
- Amaral, M.T.; Guedes-Pinto, A.C.; Chevitarese, O. Effects of a glass-ionomer cement on the remineralization of occlusal caries-an in situ study Efeito de um cimento de ionômero de vidro sobre a remineralização de cárie na superfície oclusal-estudo in situ. Braz. Oral Res. 2006, 20, 91–96. [Google Scholar]
- Simeonov, M.; Gussiyska, A.; Mironova, J.; Nikolova, D.; Apostolov, A.; Sezanova, K.; Dyulgerova, E.; Vassileva, E. Novel hybrid chitosan/calcium phosphates microgels for remineralization of demineralized enamel—A model study. Eur. Polym. J. 2019, 119, 14–21. [Google Scholar] [CrossRef]
- Hamba, H.; Nakamura, K.; Nikaido, T.; Tagami, J.; Muramatsu, T. Remineralization of enamel subsurface lesions using toothpaste containing tricalcium phosphate and fluoride: An In Vitro µCT analysis. BMC Oral. Health 2020, 20, 292. [Google Scholar] [CrossRef]
- Naksagoon, T.; Ohsumi, T.; Takenaka, S.; Nagata, R.; Hasegawa, T.; Maeda, T.; Noiri, Y. Effect of water aging on the anti-biofilm properties of glass ionomer cement containing fluoro-zinc-silicate fillers. Biofouling 2020, 36, 1090–1099. [Google Scholar] [CrossRef] [PubMed]
- Cate, J.T.; Duijsters, P. Alternating Demineralization and Remineralization of Artificial Enamel Lesions. Caries Res. 1982, 16, 201–210. [Google Scholar] [CrossRef]
- Lippert, F. Dose-Response Effects of Zinc and Fluoride on Caries Lesion Remineralization. Caries Res. 2012, 46, 62–68. [Google Scholar] [CrossRef]
- Cate, J.M.T.; Cummins, D. Fluoride toothpaste containing 1.5% arginine and insoluble calcium as a new standard of care in caries prevention. J. Clin. Dent. 2013, 24, 79–87. [Google Scholar] [PubMed]
- Imazato, S.; Kohno, T.; Tsuboi, R.; Thongthai, P.; Xu, H.H.; Kitagawa, H. Cutting-edge filler technologies to release bio-active components for restorative and preventive dentistry. Dent. Mater. J. 2020, 39, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Lynch, R.; Churchley, D.; Butler, A.; Kearns, S.; Thomas, G.; Badrock, T.; Cooper, L.; Higham, S. Effects of Zinc and Fluoride on the Remineralisation of Artificial Carious Lesions under Simulated Plaque Fluid Conditions. Caries Res. 2011, 45, 313–322. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Quintini, M.; Lelli, M.; Tarterini, F.; Foltran, I.; Scribante, A. Biomimetic Action of Zinc Hydroxyapatite on Remineralization of Enamel and Dentin: A Review. Biomimetics 2023, 8, 71. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mayer, I.; Featherstone, J. Dissolution studies of Zn-containing carbonated hydroxyapatites. J. Cryst. Growth 2000, 219, 98–101. [Google Scholar] [CrossRef]
- Li, M.; Xiao, X.; Liu, R.; Chen, C.; Huang, L. Structural characterization of zinc-substituted hydroxyapatite prepared by hydrothermal method. J. Mater. Sci. Mater. Med. 2008, 19, 797–803. [Google Scholar] [CrossRef]
- Dornelas, J.; Dornelas, G.; Rossi, A.; Piattelli, A.; Di Pietro, N.; Romasco, T.; Mourão, C.F.; Alves, G.G. The Incorporation of Zinc into Hydroxyapatite and Its Influence on the Cellular Response to Biomaterials: A Systematic Review. J. Funct. Biomater. 2024, 15, 178. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, K.; Shimada, Y.; Shinno, Y.; Ono, S.; Yamaji, K.; Ohara, N.; Sadr, A.; Sumi, Y.; Tagami, J.; Yoshiyama, M. Assessment of Demineralization Inhibition Effects of Dentin Desensitizers Using Swept-Source Optical Coherence Tomography. Materials 2021, 14, 1876. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Composition | Company | Lot No. |
|---|---|---|---|
| Caredyne Restore (zGIC) | Powder: fluoroaluminosilicate glass, fluorozincsilicate glass (BioUnionTM filler), polyacrylic acid powder Liquid: polyacrylic acid, polybasic carboxylic acid, phosphoric acid, distilled water | GC Dental Industrial Corporation | P: 2102161 L: 2102181 |
| Fuji IX (cGIC) | Powder: fluoroaluminosilicate glass, polyacrylic acid powder Liquid: polyacrylic acid, polybasic carboxylic acid, distilled water | GC Dental Industrial Corporation | P: 2206061 L: 2205301 |
| Control | cGIC | zGIC | |
|---|---|---|---|
| Before | 2213.83 ± 66.52 aA | 2223.47 ± 68.27 aA | 2223.10 ± 72.12 aA |
| White Spot | 1954.58 ± 59.82 bA | 1958.15 ± 99.62 bA | 1916.40 ±78.36 bA |
| Aft App | 1965.42 ± 54.26 bA | 2108.21 ± 71.77 bB | 2309.95 ± 62.41 acC |
| 1 week | 2088.50 ± 59.04 cA | 2215.51 ± 44.92 aB | 2389.50 ± 67.41 cdC |
| 2 weeks | 2127.35 ± 45.99 acA | 2259.80 ± 50.52 aB | 2450.70 ± 77.94 dC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myanmar, K.; Inoue, G.; Chen, X.; Shimada, Y. Remineralization Effects of Zinc-Containing Glass Ionomer Cement Restoratives on Demineralized Enamel Under pH Cycling Conditions. Crystals 2025, 15, 329. https://doi.org/10.3390/cryst15040329
Myanmar K, Inoue G, Chen X, Shimada Y. Remineralization Effects of Zinc-Containing Glass Ionomer Cement Restoratives on Demineralized Enamel Under pH Cycling Conditions. Crystals. 2025; 15(4):329. https://doi.org/10.3390/cryst15040329
Chicago/Turabian StyleMyanmar, Khin, Go Inoue, Xuefei Chen, and Yasushi Shimada. 2025. "Remineralization Effects of Zinc-Containing Glass Ionomer Cement Restoratives on Demineralized Enamel Under pH Cycling Conditions" Crystals 15, no. 4: 329. https://doi.org/10.3390/cryst15040329
APA StyleMyanmar, K., Inoue, G., Chen, X., & Shimada, Y. (2025). Remineralization Effects of Zinc-Containing Glass Ionomer Cement Restoratives on Demineralized Enamel Under pH Cycling Conditions. Crystals, 15(4), 329. https://doi.org/10.3390/cryst15040329