1. Introduction
The digital transformation in healthcare systems has been increasing its pace, hence enabling healthcare providers to digitally store and share medical information, helping to build a continuum of care for patients. The adoption of electronic health records (EHRs) has recently spread globally across many countries. EHRs are a digital collection of patients and population health information [
1] that can enhance healthcare services by making these data available to professionals and integrate the various stakeholders that patients meet along their continuum of care. Additionally, EHRs can also feed a broader database that can be useful for scientific research and epidemiological considerations.
EHR adoption is assisted by a multitude of technological frameworks employed for storing and accessing such records [
2]. The heterogeneity of EHR-based software systems, however, can be an obstacle to the seamless exchange of information among healthcare institutions, professionals, and patients. The effort to unify such different, and often siloed, systems can be complex and articulated. As a result, the majority of digital health systems are unable to interoperate, sometimes even within the same medical facility, and any shortcomings in information exchange can negatively impact the entire healthcare delivery process. Blockchain technology can offer opportunities for improvement, since its inherent characteristics make it suitable for storing and monitoring activities on medical data, and can tackle several existing challenges faced by current healthcare systems [
3,
4]. Unlike traditional systems, blockchain’s decentralized architecture ensures robustness against single points of failure and enhances security against attacks and data loss [
4,
5]. While blockchain cannot be used to store all data in EHR records, due to size constraints and storage cost, it can be employed to index them using hashing functions. This capability along with its inherent transparency, allows for the traceable and secure tamper-evident mapping of patient health data. The adoption of blockchain technology can establish a secure layer for certifying the interactions among various actors that perform activities on EHRs, thanks to its robust user authentication mechanisms. This level of security effectively addresses trust issues and can empower patients with full control over their health records; that is, blockchain can enable patients to manage and authorize access to their records, making it unnecessary to resort to a trusted authority. To employ the blockchain in this context, however, some limitations have to be addressed, such as the cost of on-chain storage or issues related to privacy preservation, as data saved in its blocks can be viewed by anyone who has access to the blockchain. According to privacy regulations such as the Health Insurance Portability and Accountability Act (HIPAA) [
6] in the United States or the General Data Protection Regulation (GDPR) [
7] in Europe, regardless of how they are stored, sensitive information, including health, demographic, and genetic data, is subject to stringent protection requirements.
Addressing these concerns requires innovative solutions that leverage the blockchain’s strengths such as decentralization (for security and resilience), interoperability across different systems, integrity of data, and a strong authorization system (to restrict the management of data). Other features need to be provided, such as ensuring adherence to privacy regulations, cost efficiency, ease of access for all relevant parties, scalable storage solutions for large data volumes, and the optimization of performance when using smart contracts. In this paper, we identify the key factors that are desirable for the development of a blockchain-based EHR and propose a novel model, called Edge-enhanced Decentralized Governance and EHRs (EdgeHR), as described in
Section 3,
Section 5 and
Section 6, which leverages the strengths of public blockchains, such as Ethereum [
3,
4], mitigating its inherent limitations, by integrating smart contract design patterns [
8,
9,
10,
11,
12] and the edge computing paradigm [
13,
14]. Detailed discussions on the specific design patterns utilized are provided in
Appendix A.
The remaining sections of the paper are as follows.
Section 2 gives a synoptic overview of some related works whose main contribution is the use of blockchains in EHR use cases.
Section 3 points out the unresolved issues of other blockchain-based EHRs and proposes a solution to address these issues.
Section 4 shows two use cases to further illustrate the proposed solution.
Section 5 provides a discussion of the main characteristics achieved by our proposed system.
Section 6 delves into the EdgeHR smart, also providing various code snippets that illustrate how the main functions operate.
Section 7 draws the conclusions.
Appendix A describes useful design patterns used in our solution.
3. Proposed Approach: EdgeHR
Our proposed approach for a blockchain-based EHR system leverages a public blockchain such as Ethereum. Our solution mitigates its inherent limitations by implementing the strategies described in this section and in
Section 5, while coping with the shortcomings of other approaches reported in
Section 2.
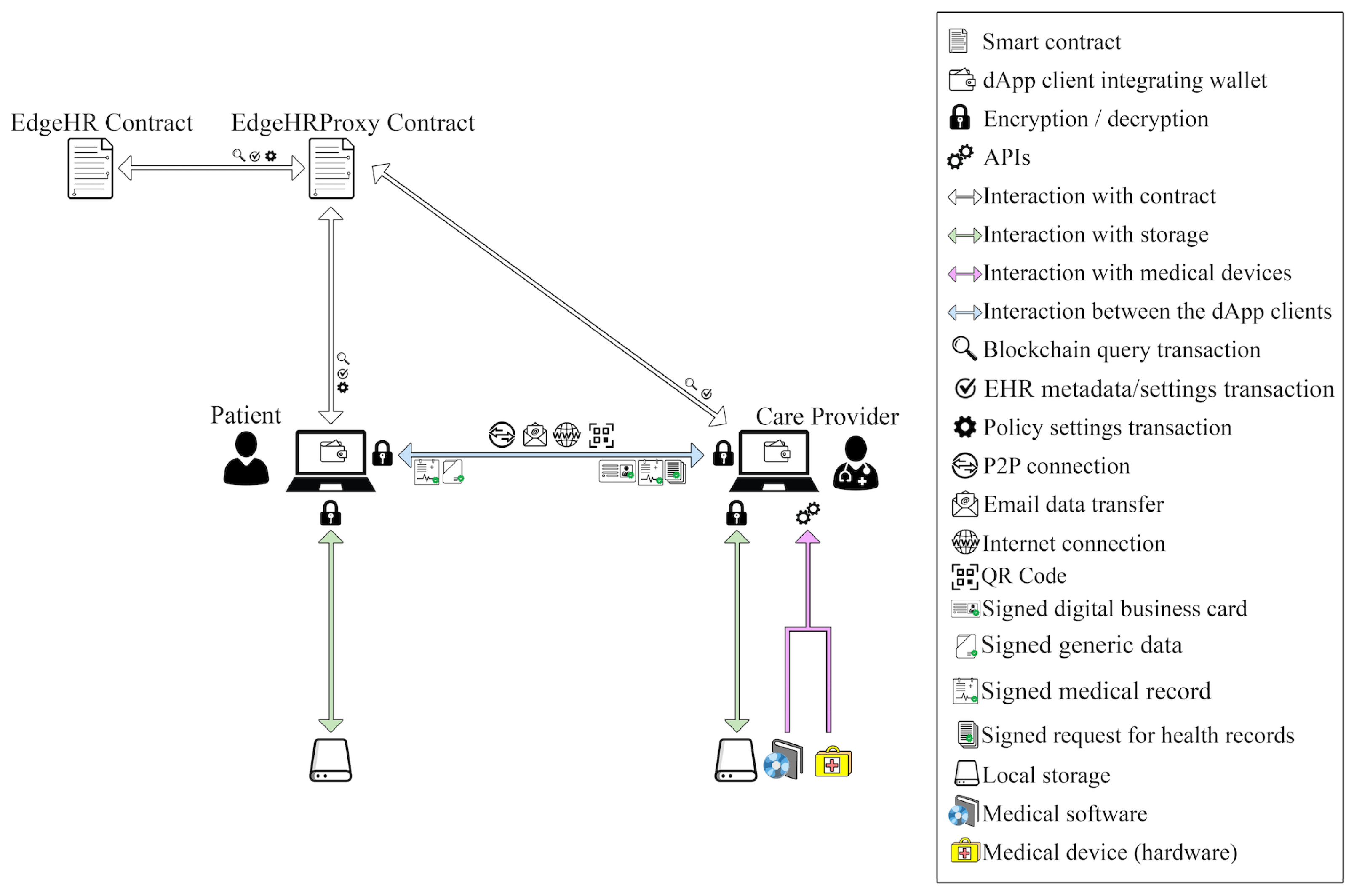
Figure 1 shows the key interactions among the proposed solution’s components. The client of the decentralized blockchain-based application (dApp) initiates interactions according to the user’s role and operates in conjunction with storage, some devices that are accessible locally, and the Edge smart contract that runs on the blockchain.
The clients are executed on devices, such as personal computers, laptops, smartphones, or tablets with storage capabilities, that can connect to a LAN network and have access to the Internet. Clients incorporate cryptographic libraries, notably secp256k1 [
38], to implement functionalities like the Elliptic Curve Digital Signature Algorithm (ECDSA) used by Ethereum. Clients can also access the blockchain and execute the wallet functionalities through the use of web3.js, a JavaScript library that provides a set of APIs for interacting with a local or remote Ethereum node. This enables seamless integration of blockchain functionalities into the user interface, such as sending transactions, interacting with smart contracts, and managing accounts. As shown in
Figure 1, the exchange of information between the patient and care providers, both acting as dApp clients, occurs through various communication methods such as a P2P connection on the same LAN, email, or other online channels, depending on the situation, as detailed below.
The type of interaction between these actors can be described by means of three phases: (i) first contact of patient and care provider; (ii) exchange of medical data and updating of metadata records; (iii) medical data consultation. Such phases are detailed in the following subsections.
3.1. Phase 1: Patient and Care Provider First Contact
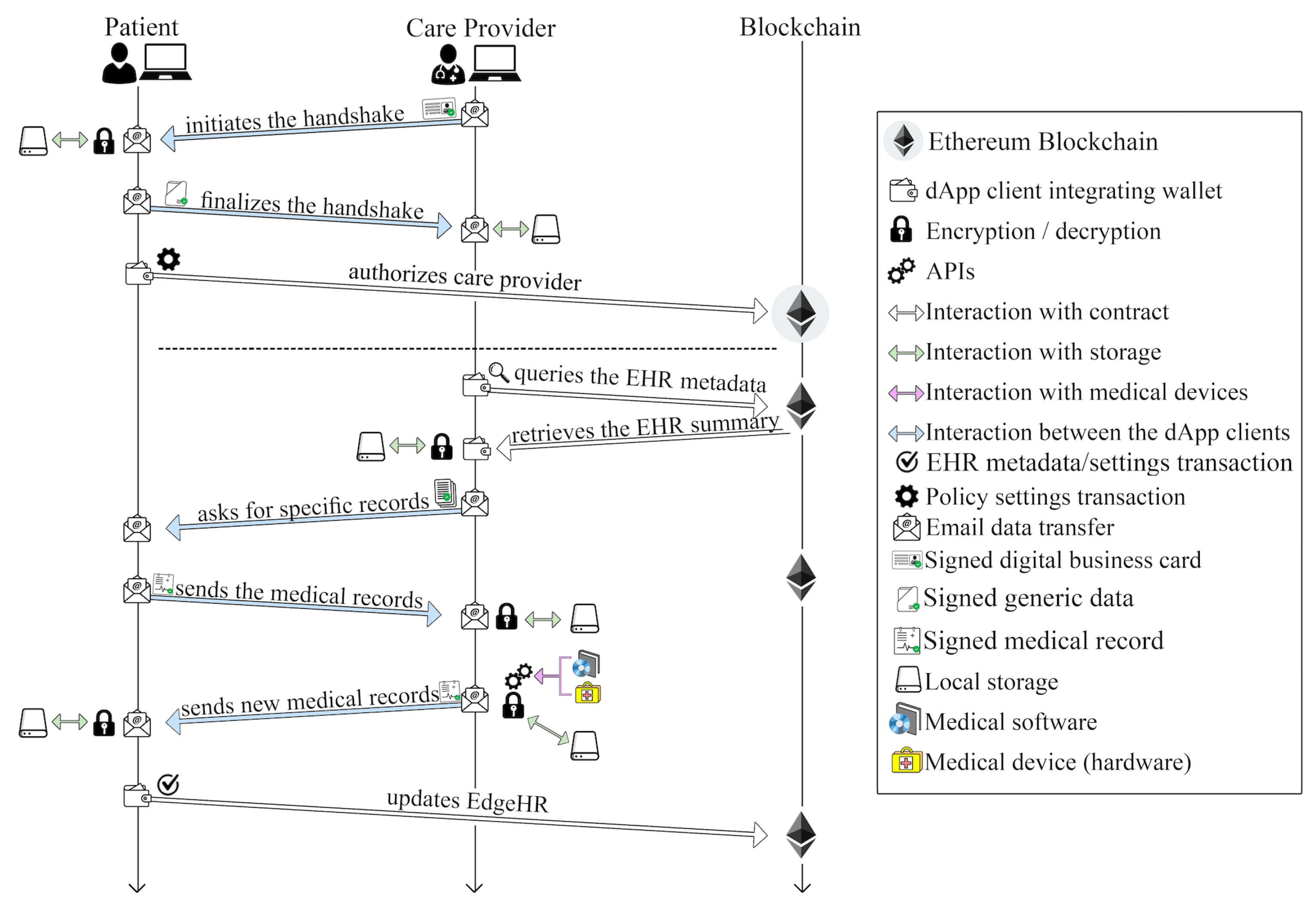
Typically, a patient may request multiple care providers to issue a specialist report on the state of their health. Therefore, the patient’s EHR has to be accessed by several care providers at different times. To safeguard this process, access to the EHR has to be properly authorized by the patient. To ensure this, proper mechanisms are put into place in our solution. When a user (patient or care provider) joins the system, they log into the dApp client, which allows them to either create a new wallet address or import an existing one. The client’s response varies depending on the user type. Specifically, for patients accessing the service for the first time, the client triggers the deployment of two distinct smart contracts, the EdgeHR and the EdgeHRProxy smart contracts, ensuring that every patient has their unique personal instances.
Figure 2 shows this process as it occurs over time. EdgeHR serves as a patient-dedicated repository for the EHR index and metadata, while EdgeHRProxy is an intermediary smart contract that stores the address of the EdgeHR instance, as detailed in in
Section 6. This mechanism implements the Proxy design pattern (see
Appendix A), a solution for making the logic of smart contracts “upgradable” (i.e., masking the challenges associated with the immutability of smart contracts.
By using the Owner design pattern (see
Appendix A), the patient becomes the owner of both the smart contracts, meaning that only the patient’s wallet address can trigger specific functions. For subsequent logins, the deployed smart contracts will already be available.
When care providers interact with a patient for the first time, the dApp client generates a message M, which acts as a digital “business card” that is used to initiate secure communication with the patient’s client and to facilitate authorization policies management. This message includes the care provider’s wallet address and the related public key P, in addition to other pertinent information such as the professional’s name, and contacts or clinic address. The authenticity of this message is ensured by its digital signature. The initial interaction between medical professionals and patients involves performing a “handshake”, which can be executed via a direct P2P connection within the same LAN, using a QR code, or remotely via email. The care provider’s dApp client sends the message M to the patient’s dApp client. Upon verifying the message’s authenticity and ensuring that it originates from the intended care provider, the patient’s dApp client authorizes the healthcare provider’s address. This authorization is carried out through the EdgeHR smart contract’s authorizeCareProvider function, which grants access to the patient EHR, setting permissions and their duration. In response to concluding the handshake, the patient’s dApp client sends back specific data, including the patient’s wallet address, the address of the EdgeHRProxy smart contract instance owned by the patient, and the existing textual descriptions of the types of records, already mapped in the dApp client, such as visits, exams, analyses, treatments, and medical histories.
3.2. Phase 2: Exchange of Medical Data and EHRs Update
As a result of a medical visit or examination, the care provider generates data meant to update the patient’s EHR record. These data can be any type of media (text files, formatted documents, images, videos, 3D models, etc.). At this point, several possible scenarios arise.
Digital data only: the provider only generates digital records.
Physical media or hard copy documents: the provider produces data in some physical formats.
Hybrid documentation: the provider creates a combination of both digital records and physical media or hard copy documents.
In the first case, which represents the best-case scenario, the provider supplies such data to their dApp client, which, in turn, formats them into a file f and signs them. Subsequently, the care provider’s client computes the hash of f, encrypts f using the private key of the care provider, and stores the encrypted file (denoted as) f’ locally. If its size is smaller than a threshold t (determined by the patient’s dApp client, based on the device type), the provider transfers f’ to the patient’s client, via a P2P connection. If the file size exceeds the threshold t, or if the care provider and the patient are not on the same LAN, and thus cannot connect their devices running the dApp clients, the care provider will resort to alternative methods such as digital media, email, online services, or the transfer capabilities of the software they use for patient services, to deliver f’ to the patient. Independently of how it is received, the patient’s client decrypts the file with the care provider’s public key and saves it locally by encrypting it with their own private key.
Figure 1 shows the interaction between the care provider and the patient’s smart contract, which is performed by means of the patient’s proxy smart contract. The care provider can update the indexing of the patient’s EHR or, alternatively, could opt to transfer to the patient a signed gasless transaction (following the EIP-2771 protocol
https://eips.ethereum.org/EIPS/eip-2771, accessed on 17 April 2024), which invokes the functions that update the smart contract’s EHR indexing. The EIP-2771 standard allows a third party (or relayer), in this case the patient, to submit the transaction to the blockchain on behalf of the original sender, in this case the care provider. This process retains the transaction’s integrity, as the original signature from the provider is preserved, while the gas fee is handled separately, ensuring that the original sender does not incur gas costs since they are covered by the relayer. This approach can be particularly useful during network congestion, when gas fees might be excessively high. Considering the successful secure storage of data within both dApp clients, it is strategically viable to defer updating the EHR indexing within the smart contract.
An additional alternative involves allowing the patient to directly update the EHR indexing in the smart contract. Using functions exclusively accessible to the owner, the patient can update the smart contract’s state with the records produced by the care provider, including the provider’s wallet address. In case the provider produces physical media or hard copy documents, namely the worst-case scenario, it will be the user’s responsibility to digitize and store them through the dApp client, which, subsequently, can create and send a transaction carrying the file’s hash along with other required information to update the EHR. In cases where the provider produces hybrid documentation, the same principles from the previously mentioned points can be applied.
The dApp clients offer the option to transfer or copy the medical records to additional local storage solutions, such as external hard drives used for backup purposes, to enhance data security. While the care provider might delete these data on their end, each patient is responsible for maintaining their EHRs. From the patients’ perspective, maintaining EHRs is no more complex than managing traditional paper-based data, which are, however, prone to physical deterioration or loss. This approach empowers patients with control over their own personal health data, but it places the responsibility for their maintenance on them.
3.3. Phase 3: Medical Data Consultation
To consult a patient’s medical records, a care provider, who has previously engaged with the patient, can utilize their dApp client to retrieve them (when already present in their local storage) with no need to interact with the smart contract. However, in situations where the medical records are inaccessible, such as when data are not present in the local storage of the care provider’s dApp, or particularly when the patient engages with a new medical facility, with which they have had no prior interaction that requires the examination of their records, (new) care providers can conduct a preliminary search. The smart contract’s function getSummary (see
Section 6) enables authorized entities to download the record summaries from the EHR’s on-chain data. This process assumes that the patient has previously granted the necessary access permissions to the (new) care provider in the smart contract, after having completed the “handshake” (see
Section 3.1), exchanging their initial digital “business card” message and the Proxy smart contract address along with the kind descriptions. Subsequently, (new) care providers can identify and select relevant data types based on their search criteria. Upon reviewing this summary, whether planning to meet the patient in person or to provide remote consultations, they can generate and sign a specific request, RecordAccessRequest, for detailed records through their dApp client. This request, including the progressive numbers of the required records and the corresponding data hashes, is sent to the patient via email or instant messaging services.
Upon receiving and opening this message, the patient’s dApp client first verifies its authenticity. Following successful verification, the application decrypts the requested records and re-encrypts them using the care provider’s public key. Finally, these re-encrypted records are sent back to the requester, as an email attachment, through a P2P connection if the patient and the care provider are on the same LAN, or via alternative communication channels.
5. Discussion
The proposed system aims to achieve several essential key features, for an effective EHR system, including decentralization, accessibility, enhanced security, patient control, enhanced privacy, interoperability, storage and cost efficiency, and optimized performance, which will be discussed in the following paragraphs.
5.1. Decentralization
True decentralization, not only from an architectural standpoint but also in terms of independence from one or more trusted entities, is fully realized only through a public blockchain. To meet the requirement for decentralization, we have concluded that Ethereum is the optimal solution, as it operates independently of any specific entity and allows any user to operate a node. Although becoming a validator in Ethereum requires staking 32 ETH [
39], users have the option to delegate their stake and participate in a staking pool [
40]. Despite this limitation, the number of nodes in a public blockchain like Ethereum is significantly higher compared to a consortium blockchain. According to Etherscan (
https://beaconscan.com/validators#active accessed on 17 April 2024), there were a total of 977,948 active validators at the time of writing. This extensive network of nodes contributes to greater decentralization, enhancing security and reducing dependency on trusted entities. This aspect is particularly important in the context of healthcare data, where security and reliability are paramount. Adopting a public blockchain for EHRs offers real patient sovereignty, reduces risks associated with centralized control, and improves network integrity and auditability. However, the transition to a public blockchain, such as Ethereum, is not straightforward, as it necessitates addressing its inherent limitations, especially (i) the difficulty in ensuring all three aspects of scalability, security, and decentralization [
41,
42,
43,
44], (ii) the costs associated with transactions, and (iii) the potential bugs in the code. In the following subsections, we detail our solution and how it addresses these issues.
5.2. Accessibility and Enhanced Security
Accessibility and authentication security are crucial to ensuring that all stakeholders can interact with the system both easily and securely. Blockchain technology inherently provides robust authentication solutions that do not require any additional trusted authorities. This technology employs native account management, which is implemented using strong cryptographic mechanisms and relies on the consensus algorithms utilized by the validator nodes. Furthermore, the economic cost associated with transactions’ execution acts as a deterrent against potential attacks, thereby adding an additional layer of security and preserving the integrity of the system. Regarding the implementation of wallet software, we believe that different versions are functionally equivalent. Wallet applications authenticate users and authorize transactions using private keys, from which the wallet addresses are derived. Typically, for any given blockchain, there are multiple wallet implementations available, including hardware wallet versions that enhance security since they are less susceptible to online attacks and malware. Hardware wallets store private keys within a physical device, making them more resilient to unauthorized access. They are capable of signing transactions without the need for a direct connection to a PC or other devices. Once signed, the transactions can then be transferred to the computer or device via USB or Bluetooth to be sent to the blockchain network.
In conclusion, the fundamental pillar of user access security in blockchain-based applications lies in the robust cryptography employed by the blockchain technology itself. The client of our dApp leverages this cryptography and utilizes the Web3 library through APIs that harness the native wallet functionalities of Ethereum. This ensures that the previously described security features are fully integrated into the dApp client.
5.3. Patient Control
The employment of smart contracts enables a dynamic and secure mechanism where users can directly control who has access to their health records and under what conditions, ensuring that each patient is placed at the center of their healthcare data management. Even in cases where data are directly acquired by users, specifically from hard copies provided by care providers, EdgeHR still offers a solution allowing for the self-entry of data by patients, enhancing its adaptability to a wider range of data entry scenarios, giving patients unprecedented control over their personal medical information. This approach is unlike other previous proposals, which limit updates to care providers only, and their solutions are then possible when care providers are fully equipped to use the proposed blockchain-based EHR systems. Furthermore, interactions between patients and doctors are initiated directly by the stakeholders themselves without the need for prior authorization or management by a third party, reinforcing the autonomy and immediacy of patient care. Lastly, by storing health data directly on users’ own devices, data remain genuinely in the hands of the stakeholders, avoiding reliance on centralized storage solutions and reducing vulnerability to external access or control
5.4. Enhanced Privacy
One of the primary challenges when adopting the blockchain in an EHR system is related to privacy. Due to the transparent nature of public blockchains, all transactions are visible to anyone. This degree of openness, while beneficial for transparency, raises significant concerns when dealing with sensitive data, where confidentiality is paramount. This issue extends to compliance with regulatory standards, since the immutable nature of the blockchain may conflict with the requirements for data to be alterable or deletable. In our EHR model, to ensure that data are not constantly exposed to online vulnerabilities, we have implemented the paradigm of edge computing: data are stored off-chain, locally on the users’s own devices, while only their hashes are saved on the blockchain.
Although these data could potentially be subject to modification, their integrity is ensured by the use of cryptographic hash functions, which generate the unique digital fingerprints stored on-chain and are reinforced by the care provider’s digital signature. This approach also guarantees non-repudiation, ensuring that the originator cannot deny their authorship. Additionally, stored data are encrypted, ensuring that, in the event of unauthorized access, they remain indecipherable. This method adds an essential layer of accountability and trust to the system by ensuring that every transaction and data exchange is verifiable. It enables secure storage outside the blockchain and maintains a highly available indexing system on the blockchain for easy retrieval and verification, thereby effectively safeguarding health information and adhering to privacy standards.
5.5. Interoperability
Interoperability is crucial for EHR systems. Although it depends on the data format rather than the infrastructure used to save these data, the edge computing paradigm allows for greater interoperability as the locally stored data can be re-written and modified according to various standards, ontologies, and methodologies that define clinical data models in a standardized and reusable way. This approach not only enhances EHR flexibility and system compatibility but also promotes the seamless exchange and utilization of health information across various environments, as patients and care providers can utilize format translators to revise the format of previously saved records to comply with different and new standards.
5.6. Storage and Cost Efficiency
The necessity to integrate off-chain storage solutions introduces additional complexity and potential points of failure, as data must be securely and reliably synchronized with the blockchain. Through the strategies and mechanisms adopted in our methodology, the blockchain extends its inherent robustness and strengths across all components of the system, including external storage. By using the edge computing paradigm and storing data on user devices, as described in our approach, integrity, ownership, and non-repudiation of data are preserved without incurring the economic costs associated with blockchain storage or external cloud services. This approach is similar to the one described in [
12], where we previously provided a blockchain-based solution for the green energy market, described in the form of a design pattern, which also leverages edge computing to optimize data management. The cost for transaction processing and the overall throughput of public blockchains are also significant constraints, potentially becoming a critical bottleneck for blockchain-based distributed applications.
The dApp client’s capability to postpone blockchain transactions to times beyond the conclusion of a medical visit or examination offers a significant benefit in terms of reducing transaction costs. This delay may also allow for the aggregation of multiple data entries into a single transaction, reducing the frequency and, consequently, the total cost of transactions, while also addressing the issue of limited throughput. The dApp client also features a real-time gas cost monitoring tool that tracks gas prices to detect periods of lower average costs, offering an opportunity to execute transactions more cheaply. This feature enhances the efficiency of blockchain interactions and is beneficial during fluctuating network conditions.
It is important to note that the initial expense of deploying smart contracts is incurred only once, and the total cost varies depending on network traffic at the time of deployment. Additionally, patients have the option, within the dApp client, to set a maximum fee limit, lower than the expected costs when an average gas price is utilized. The dApp then strategically delays the deployment until the transaction demand and the average gas prices decrease. This approach does lead to a delay in the deployment transaction processing, as validator nodes prioritize transactions with higher fees. However, choosing to monitor conditions and wait rather than initiating a transaction with a potentially lower fee in the hopes that it will eventually be processed provides greater control and predictability. This strategy helps avoid potential queue backlogs where transactions might not get processed for an extended period. Specifically, a transaction with a very low gas price might never be processed if it consistently falls below the minimum gas price accepted by validators. Such transactions can remain stuck in the mempool until they are either dropped due to node policies (which vary) or replaced by the sender with another transaction with a higher gas price—a method known as “fee bumping”.
5.7. Smart Contracts and Optimized Performance
The security and efficiency of smart contracts on a decentralized blockchain pose unique challenges. The immutable nature of blockchain technology ensures the permanence and reliability of the stored information, whether it involves transactions or user data. Once data are stored in the blockchain, altering or deleting them becomes virtually impossible. This characteristic extends to smart contracts as well and makes post-deployment modifications or bug fixes challenging. To overcome this limitation, our model leverages the Proxy design pattern, which is designed to enhance performance and address the inherent constraints of blockchain and smart contract development. These design patterns are described in
Appendix A.
In addition, the creation of individual smart contract instances for each patient avoids accumulating excessive data in a single smart contract responsible for managing different patients, a scenario that would become unfeasible with a large number of users. Conversely, by providing each user with their own smart contract instance, it becomes possible to streamline the management of each patient’s data, ensuring that the system remains scalable and efficient even as the user base grows. In this way, costs become proportional to the individual user’s data volume, and each patient’s information is isolated and protected within their individual contract. Furthermore, this separation of instances reinforces the system’s patient-centric focus since the patient becomes the only owner (see
Appendix A) of the smart contract, who can define access policies for their own data.
6. Smart Contract Details
This section outlines the structure and functionalities of the EdgeHR and EdgeHRProxy smart contracts implemented in Solidity [
45], and includes snippets of the code of key functions. When the patient’s client deploys its own EdgeHR and EdgeHRProxy instances, the constructors (see Listing 1) of the smart contracts are activated. They both employ the Owner design pattern (see
Appendix A) and are designed to store the wallet address of the transaction’s sender (the patient), as the owner of the contract.
| Listing 1. Setting the state variable for the owner. |
| constructor() { owner = payable(msg.sender); } |
msg.sender is the sender of the transaction and is stored in the owner variable, which is of the type
address. This setup enables the smart contract to restrict specific operations to the authorized user by comparing the sender’s address in transaction requests with the stored owner’s address, utilizing the
onlyOwner modifier (see Listing 2). A modifier in Solidity is a reusable portion of code that can be attached to functions to alter their behavior and is used to simplify and centralize validation or precondition checks. Such a mechanism ensures that the patient is the exclusive authority with the capability to set access policies for their EHR. Following the successful on-chain deployment of the EdgeHR smart contract, the EdgeHRProxy smart contract is then provided with the EdgeHR instance’s address, implementing the Proxy design pattern (see
Appendix A). The address of the EdgeHRProxy instance becomes the gateway for accessing the service, as it forwards all requests to the EdgeHR smart contract. This approach maintains a fixed access point for users, facilitating the flexible evolution of the contract’s functionality; that is, the underlying logic of the service can be updated by deploying a new version of the smart contract and obtaining a new address, which is then stored in the proxy smart contract.
| Listing 2. Some contract management functions. |
modifier onlyOwner() { require(msg.sender==owner, ‘must be owner’); _; }
function getOwner() public view returns(address) { return owner; }
function lock() public onlyOwner { _locked = 1; }
function unlock() public onlyOwner { _locked = 0; } |
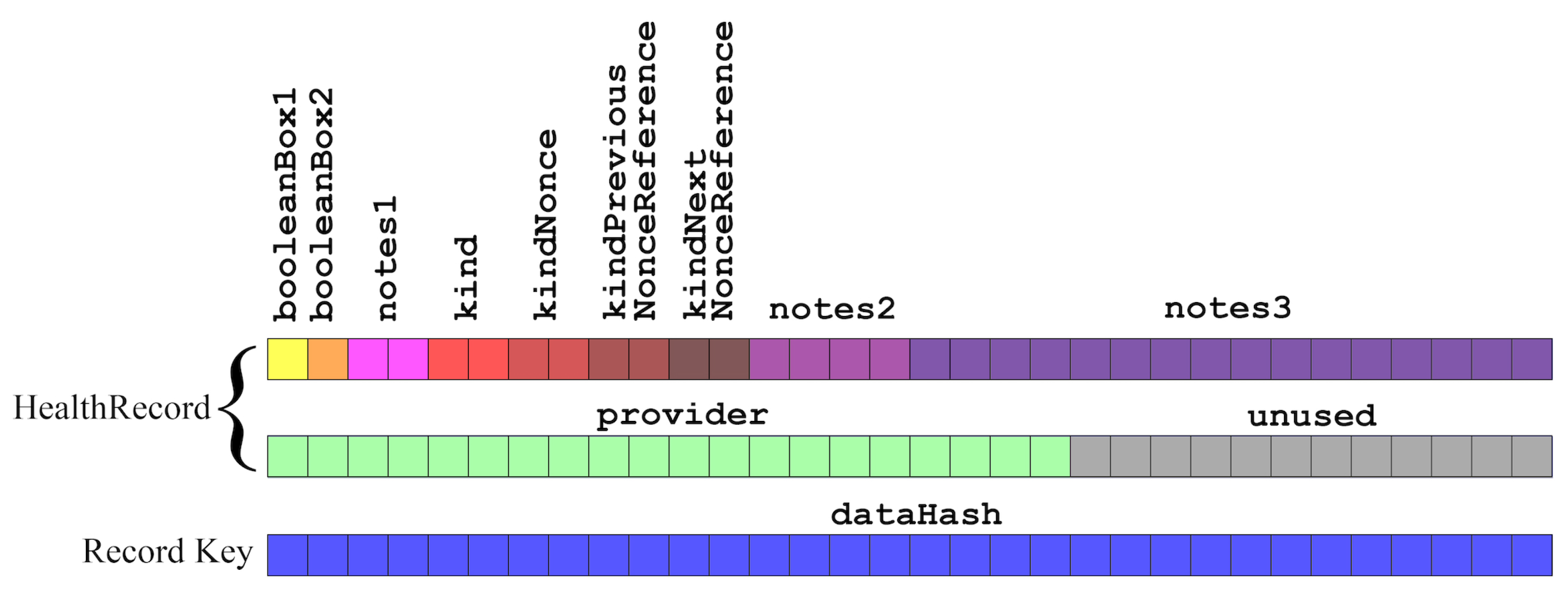
EdgeHR smart contract stores the references to EHRs in a hash table that maps the hash of each EHR to an instance of the HealthRecord structure shown in
Figure 5, facilitating the indexing and retrieval of the records, which are stored locally by the dApp clients.
Figure 5 shows several boxes, where each box represents one byte of storage. The fields booleanBox1 and booleanBox2 are one byte, utilizing the
uint8 type. Fields note1, kind, kindNonce, kindPreviousNonceReference, kindNextNonceReference are two bytes each and are represented by the
uint16 type. The notes2 field occupies four bytes and is defined as
uint32, while notes3 is considerably larger, spanning 16 bytes and defined as
uint128. The provider field, an
address, uses 20 bytes. Lastly, the dataHash key, defined as
bytes32, occupies 32 bytes.
In the HealthRecord struct, the variables have been designed, grouped together, and ordered by size (starting with the smallest and ending with the largest), to enable Solidity’s compiler to perform variable packing within single 256-bit words (see
Appendix A), maximizing space efficiency. This feature significantly reduces the storage allocation on the Ethereum blockchain, thereby lowering associated gas costs.
Each field serves a specific purpose, contributing to the management of health data: the booleanBox1 and booleanBox2 are two bytes allocated for storing Boolean variables, utilizing them as binary flags related to the EHR. This approach implements the BooleanBox design pattern [
11] (see
Appendix A), leveraging a compact and efficient method for Boolean data management in Solidity (the code for this library can be found in
https://github.com/Crypto-Patterns/Solidity-Patterns, accessed on 9 May 2024). These two fields implement 16 Boolean variables, designed for internal use, that can provide additional context about the status of the recorded data. Medical professionals can customize them according to their preferences, with the exception of the first bit in booleanBox1, which is reserved for denoting whether the record had been deleted, as detailed in the explanation of the replaceMetaData functions. Examples of potential uses include flags for “Urgency of follow-up”, to indicate if the data point to a condition that requires follow-up examinations; “Verified”, denoting whether the data have been verified for accuracy; “Data completeness”, showing whether the record is complete or if additional information is required; “Text notes by patient”, distinguishing if the text in the notes fields, stored as binary numbers, was written by the care provider or the patient; “Emit events”, to control event emission by record-updating functions; “Patient consent forms”, indicating whether patient consent has been obtained for the particular medical procedure or data usage.
The three note fields, totaling 176 bits (22 bytes), are designed to store short text strings that serve multiple purposes. The text must be converted into binary, utilizing ASCII encoding, and segmented into 16, 32, and 128 bits by the client. Such notes can be used to represent short personalized remarks from the doctor or the patient, or to specify whether a specific data format, such as HL7, FHIR, or openHR, is used.
The kind is an identifier that classifies the type or category of the record, while kindNonce ensures uniqueness within each category. The unique identification of each record is achieved through the combination of both. Additionally, kindPreviousNonceReference serves as a reference to a previous record within the same kind, establishing a backward link. Conversely, kindNextNonceReference points to a subsequent record, forming a forward connection. This field can only be updated when a following record is added, and its nonce is known. These references facilitate the creation of a bidirectional linked list of records, enhancing the organization and contextual understanding of related health events or statuses within a particular category. The provider field represents the wallet address of the care provider responsible for generating the medical record. Finally, the dataHash represents the hash of the actual data.
Utilizing uint16 for kind and kindNonce, rather than a whole 256-bit word, does not compromise the system’s longevity. Although the maximum values for these uint16 fields could theoretically be reached, considering the current growth rate of Ethereum (approximately 2,628,000 blocks per year) and a usage pattern of one new record per block, it would take several centuries for the combination of kind and nonce to reach their maximum values. This approach, therefore, ensures the longevity and practical utility of the system for the foreseeable future, striking a balance between storage efficiency and future scalability.
In the client application, the data are replicated using the same structure with the addition of an extra string field called blockStamp. The blockstamp denotes a reference to the block where the transaction, which updated the metadata, has been stored. This reference is represented by the unique hash of said block, providing a precise and verifiable pointer to the block’s location within the blockchain, which contains the transaction. This field also establishes a temporal marker based on the blockchain’s timeline, synchronized with the blockchain’s pace. It allows us to overcome issues associated with timestamps, which can be inaccurate due to potential clock tampering or malfunctions. This mechanism ensures traceability and integrity of the transaction history related to metadata updates.
The smart contract is equipped with functions that we distinguish into two groups: the first one allows the patient, as the contract’s owner, to manage and customize the smart contract, while the second group is designed for interacting with the medical metadata.
6.1. Management and Customization Functions
The proposed EdgeHR smart contract implements several management functions. The following shows the main ones, which are also reported in Listing 2. The getOwner function identifies the owner’s address, representing the patient. The lock and unlock functions, restricted to the owner, serve as a security mechanism to halt the smart contract in the case of anomalies or when vulnerabilities are discovered, to mitigate potential (or further) risk. These two functions toggle the smart contract’s active state, performing an emergency stop. In the halted state, the smart contract blocks the transactions, giving developers time to address the issue or fix any bugs. Listing 2 also provides the onlyOnwer modifier.
The authorizeCareProvider function (see Listing 3) allows the owner to manage access controls, specifying for different addresses an authorization level, mapped into a dictionary, or Solidity’s mapping. The framework establishes four tiers of permissions: level 1 for data reading, level 2 for data writing, level 3 for adding data to records created by a different care provider, and level 4 for data modification by the original creator. The expiration of the authorization is defined by a specific number of blocks, set in the authorizationDurationInBlocks parameter, after which the authorization becomes invalid. Given tat Ethereum’s block time is 12 s (i.e., a new block is minted every 12 s, except in unexpected conditions), 24 h corresponds to 7200 blocks, 10 days to 72,000 blocks, and 1 month (31 days) to 223,200 blocks.
| Listing 3. Controlling access according to addresses’ authorization level. |
function authorizeCareProvider(address _address, uint128 _level,
uint128 _blockDuration) external onlyIfUnlocked onlyOwner {
require(_address != address(0), "address cannot be null");
require(_level >=0 && _level <=4, "level must be from 0 to 4");
PermissonRecord memory permission;
permission.level = _level;
permission.expirationBlock = _blockDuration + uint128(block.number);
permissions[_address] = permission;
} |
Consistency between metadata record types and the actual data stored locally is ensured by the “kind” variable. In the client, these values are paired with descriptive strings and are specific to each patient’s EHR. Existing descriptions, which originated from earlier interactions with other care providers, are downloaded by the client’s dApp when a new medical professional completes the handshake process. When new types and descriptions were not previously defined, they are added and then shared with any subsequent care providers that the patient interacts with. Before adding a new description that might duplicate an existing one, the dApp client assesses the similarity between the newly entered data and the descriptions already in the system by employing a string distance function. It then asks the medical professional for confirmation if whether it is truly necessary to add this new type/description pair. This indexing mechanism allows the system to manage a common consistent subset of record types and descriptions for each patient, shared with their care providers, accommodating personalized medical histories that reflect the unique and specific medical interactions a patient may experience.
Maintaining verbose descriptions of the metadata types in the smart contract is not operationally necessary, but it can be beneficial if the patient wishes to authorize third parties, such as researchers or medical professionals, to access these descriptions, enabling them to conduct statistical analysis or scientific research using the descriptions of the metadata records (see
Section 6.2).
The manageKindDescription function mirrors this mapping in the smart contract. Once set, a description becomes permanently mapped to the kind’s index. If the user opts to store these details on the blockchain, the smart contract will use the data structure in Listing 4, a hash table, to map the record type indexes to their corresponding ASCII-encoded textual descriptions, allowing for 32 bytes of text. In this structure, the uint16 serves as the index for the record type, while the uint256 encodes the textual description in ASCII.
| Listing 4. Hash table for mapping record type indexes to descriptions. |
| mapping (uint16 => uint256) private kindDescriptions; |
Before a new health record is created on-chain, the function manageKindDescription (see Listing 5) verifies whether the type’s description already exists in the mapping and determines the necessary actions based on its presence or absence. If a description is already linked to that type, the process continues without making any changes. If there is no description associated with that type, the function creates a new entry for that kind with the provided description. Finally, if a description for that type already exists but is different from the one currently provided, an event can be emitted to alert that the care provider has entered a description that is different from the expected one for that type.
| Listing 5. Update EHR descriptions of types. |
function manageKindDescription (uint16 _kind, uint256 _description,
uint8 _emitEvents) private view {
require(_kind>0 && _kind<=kindDescriptionsProgressiveIndex+1, "wrong kind");
if(_kind > kindDescriptionsProgressiveIndex) {
//add the description
kindDescriptions[_kind] = _description;
kindDescriptionsProgressiveIndex++;
if(_emitEvents == 1)
emit KindDescriptionAdded(msg.sender, _kind, _description);
}
else {
if(kindDescriptions[_kind] != _description) {
//description mismatch
if(_emitEvents == 1)
emit KindDescriptionMismatch(msg.sender, kindDescriptions[_kind],
_description);
}
}
} |
When care providers need to define the meaning of specific Boolean values set in the booleanBox field, they can utilize the setBooleansDescriptions function to specify what each flag represents. The function maps integers to ASCII-encoded strings inside a dictionary, describing the binary flags, and this dictionary is nested within another one, which employs address types as its keys, as shown in Listing 6, linking each entry to the function’s caller. The function does not allow for overwriting existing entries.
| Listing 6. Nested mapping for Boolean flag descriptions. |
| mapping(address => mapping(uint8 => uint256)) private booleansDescriptions; |
The getBooleanDescription function allows for the retrieval of the descriptions associated with the booleanBoxes’ flags. It can be executed by the owner or entities with reading permissions and requires the provider address and the index of the booleanBox flag as input (see
Appendix A), returning descriptions individually. This approach is also adopted to accommodate Solidity’s limitations in handling dynamic arrays of strings.
6.2. Functions for Interactions with Metadata
The functions addMetaData, appendMetaData, appendMetaDataToSameProviderRecords, appendMetaDataToDifferentProviderRecords, and replaceMetaData are available in multiple variants, utilizing polymorphism to cater to different users. Specifically, certain versions are exclusive to the owner, while others are accessible to care providers. The key differences among these variants stem from the level of authorization needed and the requirement to assign a value to the booleanBox and notes variables. When these parameters are unnecessary, invoking the more streamlined versions of the functions reduces data transmission, thereby enhancing performance and lowering gas costs.
The addMetaData function is accessible to the owner or entities authorized at level 2 and requires the hash of the actual data, their type (kind), and various parameters as inputs depending on the variant of the function. To prevent duplicate entries, the function first verifies that the record, uniquely identified by the provided dataHash, does not already exist. This verification is carried out using a required statement that ensures both the provider field and the kind field of the mapping entry default to uninitialized values, specifically address(0), for provider and 0 for kind, as indicated in Listing 7.
| Listing 7. Verification of entry initialization conditions. |
require(healthRecords[_dataHash].provider == address(0) &&
healthRecords[_dataHash].kind == 0, "the hash is already in the EHR"); |
If the record does exist, the function reverts the transaction; otherwise, if the supplied hash does not exist, the function initializes a new HealthRecord structure instance by setting up its fields. The kindNonce value for the new record is determined by incrementing the last known nonce value for the given kind, which is stored in the latestNonces mapping. The new record is added to the healthRecords mapping using the dataHash variable as the key, ensuring each record can be uniquely identified and accessed directly via the hash of its related medical data. Additionally, to enable a sequential access similar to an array, but without the considerable computational costs of utilizing dynamic arrays, a second mapping, called healthRecordsIndexes, is employed. This mapping links each record’s index to its corresponding medical data hash, implementing the ’Mapping vs. Array’ design pattern which optimizes storage space on the blockchain (see
Appendix A). The ehrProgressiveIndex variable, incremented for each new record, serves as the key in this secondary mapping (starting from one since zero is reserved in place of null). Finally, if the emitEvents flag is set, the function emits a MetaDataAdded event (see
Section 6.3), signaling the successful addition of a new record including details such as the care provider address (
msg.sender) and the ehrProgressiveIndex. This event can be used by external observers to track updates to the EHR system in real time.
Upon successful addition, the function addMetaData returns the unique index and the kindNonce for the new record. The owner-specific versions of the function enable the patient to update records autonomously. By specifying the address that uniquely identifies the healthcare provider, the patient can ensure that EHRs are accurately attributed to the appropriate medical professional. This functionality is crucial in scenarios where the healthcare provider may not have the capability to execute or create the transaction themselves and empowers the patient to take a more active role in record management while preserving the traceability and accountability of each provider’s contributions to EHRs. Listing 8 presents the most generic version of the addMetaData function, intended for care providers, which also accommodates the booleanBoxes and the notes.
| Listing 8. Function recording useful metadata of EHRs. |
function addMetaData(
uint8 _booleanBox1, uint8 _booleanBox2, uint8 _emitEvents, uint16 _notes1,
uint16 _kind, uint16 _kindPreviousNonceReference, uint32 _notes2,
uint128 _notes3, bytes32 _dataHash, uint256 _description)
external onlyIfUnlocked hasPermission(2) returns (uint16, uint16) {
require(_kind > 0, "the kind must be specified");
require(healthRecords[_dataHash].provider == address(0) &&
healthRecords[_dataHash].kind == 0, "the hash is already in the EHR");
if (booleanBoxGlobal.getFlag(1) && _description > 0)
manageKindDescription(_kind, _description, _emitEvents);
HealthRecord memory newRecord = HealthRecord({
booleanBox1: _booleanBox1, booleanBox2: _booleanBox2, notes1: _notes1,
kind: _kind, kindNonce: latestNonces[_kind] + 1,
kindPreviousNonceReference: _kindPreviousNonceReference,
kindNextNonceReference: 0, notes2: _notes2, notes3: _notes3,
provider: msg.sender});
latestNonces[_kind] = newRecord.kindNonce;
healthRecords[_dataHash] = newRecord;
ehrProgressiveIndex++;
healthRecordsIndexes[ehrProgressiveIndex] = _dataHash;
if(_emitEvents == 1)
emit MetaDataAdded(msg.sender, ehrProgressiveIndex, _kind,
newRecord.kindNonce);
return (ehrProgressiveIndex, newRecord.kindNonce);
} |
The appendMetaData, appendMetaDataToSameProviderRecords, appendMetaDataToDifferentProviderRecords, and replaceMetaData functions operate similarly and can also be executed by the owner. Besides the basic inputs, they require a reference to a nonce of an existing record, enabling the creation of a continuity link between records. The appendMetaDataToSameProviderRecords functions operate in the same way and can be executed by an entity with level 2 permission. However, they can append metadata only to records that were originally created by the same entity that is invoking the function. The appendMetaDataToDifferentProviderRecords functions, accessible to the owner or entities with level 3 permission, operate with a broader scope. These functions enable one to append metadata to records that were not necessarily created by the same entity invoking the function.
The replaceMetaData functions, requiring the highest authorization level and, in the case of the owner, the care provider address, are designed to correct data errors. This includes modifications to booleanBoxes, notes, and the data hash, while the kind, kindNonce, kindPreviousNonceReference, and kindNextNonceReference fields cannot be altered. Additionally, care providers who have the necessary authorization can still only modify their own records and not any others. The functions can also be used to partially delete a record by setting some fields to zero. However, a duplicate of the old records persists within the dApp clients and must be manually deleted by the users. These functions should be used cautiously, but despite their sensitive nature, they are essential to enable care providers to rectify potential errors. Moreover, although the hashed data do not reveal the original information, the patient’s right to delete them from the blockchain remains paramount.
The polymorphic getSummary function (see Listing 9) extracts notes and record type descriptions from the mappings, temporarily stores them in an array in memory, and returns them as output. This allows authorized care providers to retrieve a condensed high-level view of the medical records, thus offering an overview of the patient’s medical history. The function allows to specify limits and offsets to support data pagination.
| Listing 9. Function providing notes and descriptions. |
function getSummary(uint16 _limit, uint16 _offset) external view onlyIfUnlocked
returns(PreliminarySearchStruct[] memory) {
uint256 effectiveLimit = uint16(min(_limit + _offset, ehrProgressiveIndex));
require(effectiveLimit > _offset, "invalid limit or offset");
uint256 extractedRecords = effectiveLimit - _offset;
PreliminarySearchStruct[] memory PreliminarySearch =
new PreliminarySearchStruct[](extractedRecords);
uint16 index;//defaults to 0
_offset++;
while(_offset <= effectiveLimit) {
bytes32 tempHash = healthRecordsIndexes[_offset];
HealthRecordStruct memory tempRecord = healthRecords[tempHash];
PreliminarySearchStruct memory newRecord = PreliminarySearchStruct({
notes1: tempRecord.notes1, notes2: tempRecord.notes2,
notes3: tempRecord.notes3,
description: kindDescriptions[tempRecord.kind]
});
PreliminarySearch[index] = newRecord;
index++;
_offset++;
}
return PreliminarySearch;
} |
The getSummaryByKind function scans the records stored within the smart contract to extract and set a summary of records for a certain category. Like the previous one, this function is accessible to the contract owner, authorized entities, or when the patient has explicitly opted to share their data. The getRecordByIndex function can be utilized by either the owner or an authorized entity to retrieve a record, enabling the reconstruction of a patient’s medical history. This function facilitates the validation of stored information’s integrity by enabling a comparison between the stored data hash and the hash of the actual data. The getRecordByHash function, accessible by the owner or authorized entities, retrieves specific record details, including the index based on the data hash provided to the function.
Patients can explicitly choose (by setting a Boolean flag in a global BooleanBox variable) to mirror the textual descriptions of their EHRs on-chain and publicly share them with non-authorized third parties such as medical professionals or researchers. Third parties can download data by invoking the getDescription function for evaluative or research purposes. If they identify relevant record descriptions and wish to request detailed EHRs, they can contact the patient using the contactPatient function, WHICH triggers an event that records their address and their email contact. Once notified, the patient can review the credentials of the institution or research center and opt to reply with an email message to facilitate further communication.
6.3. Events
Events facilitate communication with observers outside the blockchain by triggering actions in the front-end interface (see
Appendix A.4). Within the EdgeHR smart contract, all functions can optionally emit events. For those interacting with the EHR, this option is explicitly specified at the time of invocation through a parameter. For contract management functions, this feature is controlled by a global BooleanBox flag, which only the owner can set. These events document the actions taken on the records and identify the address responsible for the action, assisting in the reconstruction of the EHR history by providing a transparent and traceable footprint of changes. They also serve to facilitate communication with observers outside the blockchain by triggering actions in the front-end interface (see
Appendix A.4) and notifying the owner about key activities or errors. Listing 10 shows a list of the events, along with a brief description of their purposes.
| Listing 10. Events of the EdgeHR smart contract. |
event KindDescriptionAdded(address _address, uint16 _kind, uint256 _descripion);
event KindDescriptionMismatch(address _address, uint256 _storedDescripion,
uint256 _providedDescription);
event MetaDataAdded(address _address, uint16 _index, uint16 _kind,
uint16 _kindNonce);
event MetaDataAppended(address _address, uint16 _index, uint16 _kind,
uint16 _kindNonce, uint16 kindPreviousNonceReference);
event MetaDataReplaced(address _address, uint16 _index, uint16 _kind,
uint16 _kindNonce);
event RequestContact(address _address, string _email);
event SummaryDownloaded(address _address, uint16 _first, uint16 _last);
event RecordRetrievedByIndex(address _address, uint16 _index);
event RecordRetrievedByHash(address _address, uint16 _index); |
KindDescriptionAdded is emitted when a new description for a kind is added to the system, logging the address, kind identifier, and description details. KindDescriptionMismatch is emitted when there is a discrepancy between stored and provided descriptions for a kind; MetaDataAdded logs the addition of new metadata; MetaDataAppended is emitted when data are appended to an existing record; MetaDataReplaced is emitted when a record is replaced; RequestContact is triggered to send contact information to facilitate future interaction; SummaryDownloaded is emitted when a summary of records is downloaded; RecordRetrievedByIndex is emitted when a record is retrieved by its index; and RecordRetrievedByHash logs when a record is retrieved by hash.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}