
Analysis of Local Recurrence After Robotic-Assisted Total Mesorectal Excision (ALRITE): An International, Multicentre, Retrospective Cohort
 , , , , , , , ,
, , , , , , , ,
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Patients
2.3. Surgical Procedure
2.4. Outcomes and Definitions
2.5. Statistical Analysis
3. Results
3.1. Overall Results
3.2. Prediction Modelling Without over- and Undersampling
3.3. Prediction Modelling with Oversampling Only in Training-And-Testing
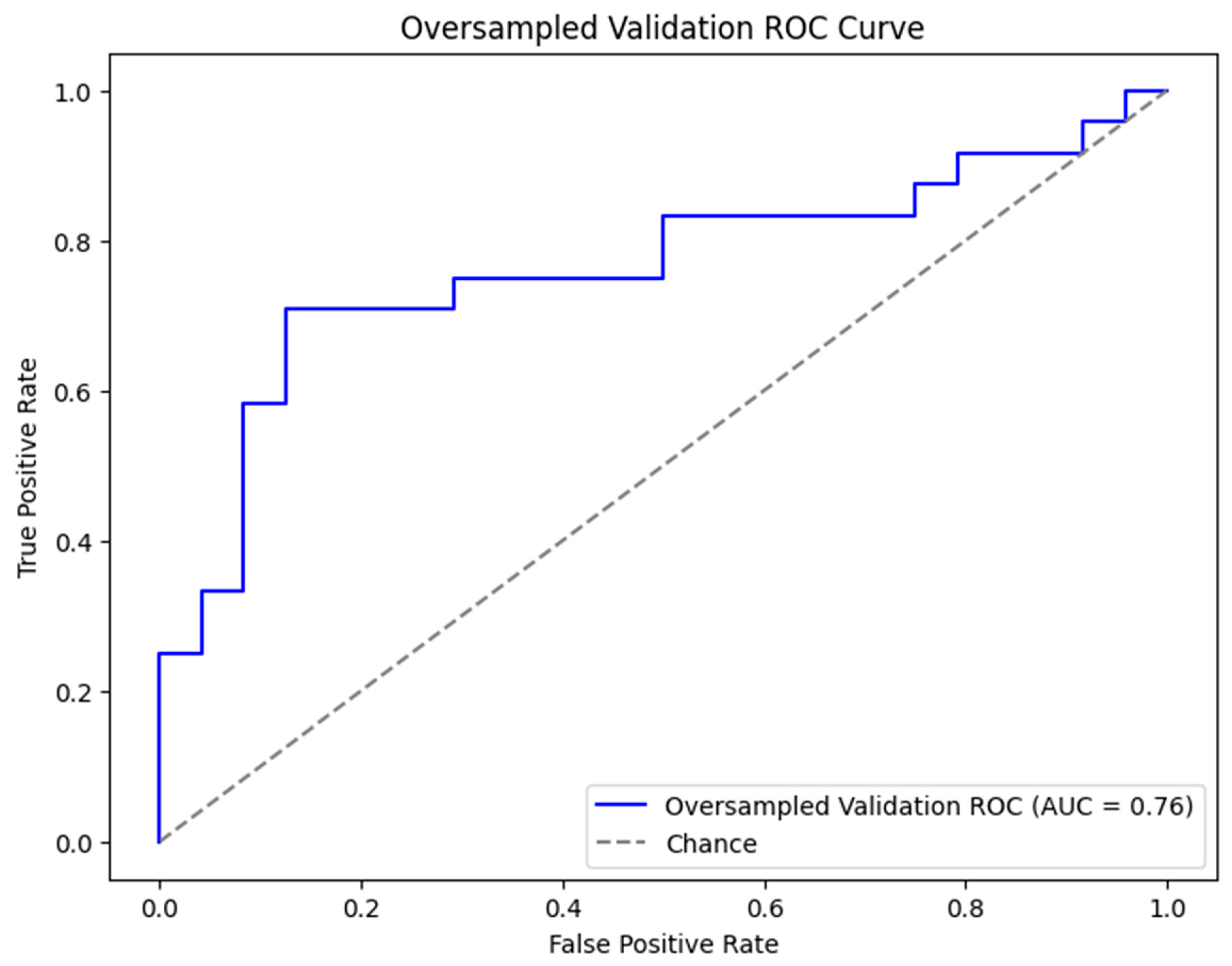
3.4. Prediction Modelling with Oversampling in Training-And-Testing and Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer Incidence and Mortality Patterns in Europe: Estimates for 40 Countries and 25 Major Cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Cancer Facts & Figures 2021|American Cancer Society. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2021.html (accessed on 10 October 2024).
- Eng, C.; Yoshino, T.; Ruíz-García, E.; Mostafa, N.; Cann, C.G.; O’Brian, B.; Benny, A.; Perez, R.O.; Cremolini, C. Colorectal Cancer. Lancet 2024, 404, 294–310. [Google Scholar] [CrossRef] [PubMed]
- Heald, R.J.; Husband, E.M.; Ryall, R.D.H. The Mesorectum in Rectal Cancer Surgery--the Clue to Pelvic Recurrence? Br. J. Surg. 1982, 69, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cao, G.; Mao, W.; Lao, W.; He, C. Robot-Assisted versus Laparoscopic Surgery for Rectal Cancer: A Systematic Review and Meta-Analysis. J. Cancer Res. Ther. 2020, 16, 979–989. [Google Scholar] [CrossRef]
- Sun, Y.; Xu, H.; Li, Z.; Han, J.; Song, W.; Wang, J.; Xu, Z. Robotic versus Laparoscopic Low Anterior Resection for Rectal Cancer: A Meta-Analysis. World J. Surg. Oncol. 2016, 14, 61. [Google Scholar] [CrossRef]
- Xiong, B.; Ma, L.; Huang, W.; Zhao, Q.; Cheng, Y.; Liu, J. Robotic versus Laparoscopic Total Mesorectal Excision for Rectal Cancer: A Meta-Analysis of Eight Studies. J. Gastrointest. Surg. 2015, 19, 516–526. [Google Scholar] [CrossRef]
- Feng, Q.; Yuan, W.; Li, T.; Tang, B.; Jia, B.; Zhou, Y.; Zhang, W.; Zhao, R.; Zhang, C.; Cheng, L.; et al. Robotic versus Laparoscopic Surgery for Middle and Low Rectal Cancer (REAL): Short-Term Outcomes of a Multicentre Randomised Controlled Trial. Lancet Gastroenterol. Hepatol. 2022, 7, 991–1004. [Google Scholar] [CrossRef]
- Kozu, T.; Akiyoshi, T.; Sakamoto, T.; Yamaguchi, T.; Yamamoto, S.; Okamura, R.; Konishi, T.; Umemoto, Y.; Hida, K.; Naitoh, T. Risk Factors for Local Recurrence in Patients with Clinical Stage II/III Low Rectal Cancer: A Multicenter Retrospective Cohort Study in Japan. Ann. Gastroenterol. Surg. 2024, 9, 128–136. [Google Scholar] [CrossRef]
- Jayne, D.; Pigazzi, A.; Marshall, H.; Croft, J.; Corrigan, N.; Copeland, J.; Quirke, P.; West, N.; Rautio, T.; Thomassen, N.; et al. Effect of Robotic-Assisted vs Conventional Laparoscopic Surgery on Risk of Conversion to Open Laparotomy Among Patients Undergoing Resection for Rectal Cancer: The ROLARR Randomized Clinical Trial. JAMA 2017, 318, 1569–1580. [Google Scholar] [CrossRef]
- Burghgraef, T.A.; Sikkenk, D.J.; Crolla, R.M.; Fahim, M.; Melenhorst, J.; Moumni, M.E.; Schelling, G.V.; Smits, A.B.; Stassen, L.P.; Verheijen, P.M.; et al. Assessing the Learning Curve of Robot-Assisted Total Mesorectal Excision: A Multicenter Study Considering Procedural Safety, Pathological Safety, and Efficiency. Int. J. Color. Dis. 2023, 38, 9. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. BMJ Br. Med. J. 2007, 335, 806. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, N.; de Neree tot Babberich, M.P.M.; d’Hoore, A.; Tiret, E.; Xynos, E.; Beets-Tan, R.G.H.; Nagtegaal, I.D.; Blomqvist, L.; Holm, T.; Glimelius, B.; et al. Definition of the Rectum: An International, Expert-Based Delphi Consensus. Ann. Surg. 2019, 270, 955–959. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, J.; Siddiqi, N.; Khan, L.; Kuzu, A.; Parvaiz, A. Standardized Technique for Single-Docking Robotic Rectal Surgery. Color. Dis. 2016, 18, O380–O384. [Google Scholar] [CrossRef] [PubMed]
- Patriti, A.; Ceccarelli, G.; Bartoli, A.; Spaziani, A.; Biancafarina, A.; Casciola, L. Short- and Medium-Term Outcome of Robot-Assisted and Traditional Laparoscopic Rectal Resection. JSLS 2009, 13, 176. [Google Scholar]
- Kwak, J.M.; Kim, S.H.; Kim, J.; Son, D.N.; Baek, S.J.; Cho, J.S. Robotic vs Laparoscopic Resection of Rectal Cancer: Short-Term Outcomes of a Case-Control Study. Dis. Colon. Rectum 2011, 54, 151–156. [Google Scholar] [CrossRef]
- Popescu, I.; Vasilescu, C.; Tomulescu, V.; Vasile, S.; Sgarbura, O. The Minimally Invasive Approach, Laparoscopic and Robotic, in Rectal Resection for Cancer. A Single Center Experience. Acta Chir. Iugosl. 2010, 57, 29–35. [Google Scholar] [CrossRef]
- Hol, J.C.; Burghgraef, T.A.; Rutgers, M.L.W.; Crolla, R.M.P.H.; van Geloven, N.A.W.; Leijtens, J.W.A.; Polat, F.; Pronk, A.; Smits, A.B.; Tuynman, J.B.; et al. Comparison of Three-Year Oncological Results after Restorative Low Anterior Resection, Non-Restorative Low Anterior Resection and Abdominoperineal Resection for Rectal Cancer. Eur. J. Surg. Oncol. 2023, 49, 730–737. [Google Scholar] [CrossRef]
- Proliferative and Metastatic Potential of Exfoliated Colorectal Cancer Cells—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/3456069/ (accessed on 28 December 2024).
- Umpleby, H.C.; Fermor, B.; Symes, M.O.; Williamson, R.C.N. Viability of Exfoliated Colorectal Carcinoma Cells. Br. J. Surg. 1984, 71, 659–663. [Google Scholar] [CrossRef]
- Do Operations Facilitate Tumor Growth? An Experimental Model in Rats—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/3738755/ (accessed on 28 December 2024).
- The Influence of Surgical Trauma on Experimental Metastasis—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/2804892/ (accessed on 28 December 2024).
- Oosterling, S.J.; van der Bij, G.J.; van Egmond, M.; van der Sijp, J.R.M. Surgical Trauma and Peritoneal Recurrence of Colorectal Carcinoma. Eur. J. Surg. Oncol. 2005, 31, 29–37. [Google Scholar] [CrossRef]
- Denost, Q.; Quintane, L.; Buscail, E.; Martenot, M.; Laurent, C.; Rullier, E. Short- and Long-Term Impact of Body Mass Index on Laparoscopic Rectal Cancer Surgery. Color. Dis. 2013, 15, 463–469. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, X.; Zhuang, Z.; Wei, M.; Meng, W.; Deng, X.; Wang, Z. The Effect of BMI on Long-Term Outcome in Patients with Rectal Cancer and Establishment of a Nomogram Prediction Model. BMC Gastroenterol. 2023, 23, 5. [Google Scholar] [CrossRef] [PubMed]
- Gebauer, B.; Meyer, F.; Ptok, H.; Steinert, R.; Otto, R.; Lippert, H.; Gastinger, I. Impact of Body Mass Index on Early Postoperative and Long-Term Outcome after Rectal Cancer Surgery. Visc. Med. 2017, 33, 373–382. [Google Scholar] [CrossRef]
- Seishima, R.; Okabayashi, K.; Hasegawa, H.; Sugiyama, D.; Ishii, Y.; Tsuruta, M.; Takebayashi, T.; Kitagawa, Y. Obesity Was Associated with a Decreased Postoperative Recurrence of Rectal Cancer in a Japanese Population. Surg. Today 2014, 44, 2324–2331. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Chi, P. Impact of Body Mass Index on Surgical and Oncological Outcomes in Laparoscopic Total Mesorectal Excision for Locally Advanced Rectal Cancer after Neoadjuvant 5-Fluorouracil-Based Chemoradiotherapy. Gastroenterol. Res. Pract. 2017, 2017, 1509140. [Google Scholar] [CrossRef]
- Meyerhardt, J.A.; Tepper, J.E.; Niedzwiecki, D.; Hollis, D.R.; McCollum, A.D.; Brady, D.; O’Connell, M.J.; Mayer, R.J.; Cummings, B.; Willett, C.; et al. Impact of Body Mass Index on Outcomes and Treatment-Related Toxicity in Patients with Stage II and III Rectal Cancer: Findings from Intergroup Trial 0114. J. Clin. Oncol. 2004, 22, 648–657. [Google Scholar] [CrossRef]
- You, J.F.; Tang, R.; Changchien, C.R.; Chen, J.S.; You, Y.T.; Chiang, J.M.; Yeh, C.Y.; Hsieh, P.S.; Tsai, W.S.; Fan, C.W.; et al. Effect of Body Mass Index on the Outcome of Patients with Rectal Cancer Receiving Curative Anterior Resection: Disparity between the Upper and Lower Rectum. Ann. Surg. 2009, 249, 783–787. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Wang, S.; Li, X.T.; Wang, Y.P.; Shi, Y.J.; Wang, L.; Wu, A.W.; Sun, Y.S. MRI of Extramural Venous Invasion in Locally Advanced Rectal Cancer: Relationship to Tumor Recurrence and Overall Survival. Radiology 2018, 289, 677–685. [Google Scholar] [CrossRef]
- Taylor, F.G.M.; Quirke, P.; Heald, R.J.; Moran, B.J.; Blomqvist, L.; Swift, I.R.; Sebag-Montefiore, D.; Tekkis, P.; Brown, G. Preoperative Magnetic Resonance Imaging Assessment of Circumferential Resection Margin Predicts Disease-Free Survival and Local Recurrence: 5-Year Follow-up Results of the MERCURY Study. J. Clin. Oncol. 2014, 32, 34–43. [Google Scholar] [CrossRef]
- Battersby, N.J.; How, P.; Moran, B.; Stelzner, S.; West, N.P.; Branagan, G.; Strassburg, J.; Quirke, P.; Tekkis, P.; Pedersen, B.G.; et al. Prospective Validation of a Low Rectal Cancer Magnetic Resonance Imaging Staging System and Development of a Local Recurrence Risk Stratification Model: The MERCURY II Study. Ann. Surg. 2016, 263, 751–760. [Google Scholar] [CrossRef]
- Taylor, F.G.M.; Quirke, P.; Heald, R.J.; Moran, B.; Blomqvist, L.; Swift, I.; Sebag-Montefiore, D.J.; Tekkis, P.; Brown, G. Preoperative High-Resolution Magnetic Resonance Imaging Can Identify Good Prognosis Stage I, II, and III Rectal Cancer Best Managed by Surgery Alone: A Prospective, Multicenter, European Study. Ann. Surg. 2011, 253, 711–719. [Google Scholar] [CrossRef]
- Hida, K.; Okamura, R.; Park, S.Y.; Nishigori, T.; Takahashi, R.; Kawada, K.; Choi, G.S.; Sakai, Y. A New Prediction Model for Local Recurrence After Curative Rectal Cancer Surgery: Development and Validation as an Asian Collaborative Study. Dis. Colon. Rectum 2017, 60, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Bach, S.P.; Hill, J.; Monson, J.R.T.; Simson, J.N.L.; Lane, L.; Merrie, A.; Warren, B.; Mortensen, N.J.M.C. A Predictive Model for Local Recurrence after Transanal Endoscopic Microsurgery for Rectal Cancer. Br. J. Surg. 2009, 96, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Valentini, V.; Van Stiphout, R.G.P.M.; Lammering, G.; Gambacorta, M.A.; Barba, M.C.; Bebenek, M.; Bonnetain, F.; Bosset, J.F.; Bujko, K.; Cionini, L.; et al. Nomograms for Predicting Local Recurrence, Distant Metastases, and Overall Survival for Patients with Locally Advanced Rectal Cancer on the Basis of European Randomized Clinical Trials. J. Clin. Oncol. 2011, 29, 3163–3172. [Google Scholar] [CrossRef] [PubMed]
- Weiser, M.R. AJCC 8th Edition: Colorectal Cancer. Ann. Surg. Oncol. 2018, 25, 1454–1455. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of Surgical Complications: A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Descriptive Variables Used for LR Prediction Model | ||||
|---|---|---|---|---|
| Level | Full Dataset | No LR | LR | |
| n | 1039 | 984 | 41 | |
| Site (%) | The Netherlands | 363 (34.9) | 346 (35.2) | 16 (39.0) |
| France | 190 (18.3) | 179 (18.2) | 9 (22.0) | |
| UK | 148 (14.2) | 143 (14.5) | 3 (7.3) | |
| Spain | 233 (22.4) | 221 (22.5) | 11 (26.8) | |
| Italy | 74 (7.1) | 66 (6.7) | 1 (2.4) | |
| Belgium | 31 (3.0) | 29 (2.9) | 1 (2.4) | |
| Sex (%) | Male | 669 (64.4) | 633 (64.3) | 27 (65.9) |
| Female | 370 (35.6) | 351 (35.7) | 14 (34.1) | |
| Age at time of surgery in years (median [IQR]) | 68.00 [61.00, 75.00] | 67.00 [60.00, 74.00] | 67.00 [61.00, 75.00] | |
| ASA score (%) | I | 173 (16.7) | 166 (16.9) | 7 (17.1) |
| II | 675 (65.1) | 638 (64.8) | 27 (65.9) | |
| III | 184 (17.7) | 175 (17.8) | 7 (17.1) | |
| IV | 5 (0.5) | 5 (0.5) | 0 (0.0) | |
| BMI (median [IQR]) | 25.92 [23.49, 29.06] | 26.00 [23.50, 28.93] | 25.41 [23.71, 27.93] | |
| Diabetic comorbidity (%) | No | 648 (89.3) | 620 (89.6) | 23 (79.3) |
| Yes | 78 (10.7) | 72 (10.4) | 6 (20.7) | |
| Cardiovascular comorbidity (%) | No | 461 (68.4) | 440 (68.3) | 18 (69.2) |
| Yes | 213 (31.6) | 204 (31.7) | 8 (30.8) | |
| History of abdominal surgery (%) | No | 519 (74.5) | 493 (74.1) | 23 (82.1) |
| Yes | 178 (25.5) | 172 (25.9) | 5 (17.9) | |
| cT (%) | cT1 | 27 (3.6) | 27 (3.8) | 0 (0.0) |
| cT2 | 223 (29.4) | 213 (29.7) | 8 (27.6) | |
| cT3 | 469 (62.0) | 440 (61.3) | 19 (65.5) | |
| cT4 | 38 (5.0) | 36 (5.0) | 2 (6.9) | |
| cN (%) | cN0 | 300 (46.6) | 291 (47.8) | 7 (30.4) |
| cN1 | 245 (38.0) | 226 (37.1) | 9 (39.1) | |
| cN2 | 99 (15.4) | 92 (15.1) | 7 (30.4) | |
| cM (%) | cM0 | 704 (92.1) | 671 (92.9) | 22 (75.9) |
| cM1 | 60 (7.9) | 51 (7.1) | 7 (24.1) | |
| Distance from the ARJ on MRI in cm (median [IQR]) | 7.00 [5.00, 9.00] | 7.00 [4.30, 9.00] | 5.00 [2.88, 9.00] | |
| Tumour location on MRI (%) | Anterior | 107 (16.1) | 106 (16.7) | 1 (3.7) |
| Circumferential | 270 (40.5) | 255 (40.2) | 14 (51.9) | |
| Lateral | 59 (8.9) | 57 (9.0) | 2 (7.4) | |
| Posterior | 95 (14.3) | 88 (13.9) | 3 (11.1) | |
| Semi-circumferential | 15 (2.3) | 15 (2.4) | 0 (0.0) | |
| Other | 120 (18.0) | 113 (17.8) | 7 (25.9) | |
| MRF on MRI (%) | MRF− | 386 (58.2) | 370 (58.7) | 15 (53.6) |
| MRF+ | 277 (41.8) | 260 (41.3) | 13 (46.4) | |
| EMVI on MRI (%) | EMVI− | 252 (50.8) | 244 (51.2) | 8 (44.4) |
| EMVI+ | 244 (49.2) | 234 (48.8) | 10 (55.6) | |
| Neoadjuvant therapy (%) | No | 425 (40.9) | 410 (41.7) | 12 (29.3) |
| Yes | 614 (59.1) | 574 (58.3) | 29 (70.7) | |
| Type of neoadjuvant therapy (%) | None | 425 (41.0) | 410 (41.8) | 12 (29.3) |
| Only chemo | 10 (1.0) | 9 (0.9) | 1 (2.4) | |
| Short-course radiotherapy | 90 (8.7) | 86 (8.8) | 3 (7.3) | |
| Long-course radiotherapy | 2 (0.2) | 2 (0.2) | 0 (0.0) | |
| Chemoradiation | 358 (34.6) | 338 (34.4) | 14 (34.1) | |
| Chemoradiation + chemo (TNT) | 109 (10.5) | 99 (10.1) | 9 (22.0) | |
| Other | 42 (4.1) | 37 (3.8) | 2 (4.8) | |
| Conversion (%) | No | 1002 (96.4) | 950 (96.5) | 38 (92.7) |
| Yes | 37 (3.6) | 34 (3.5) | 3 (7.3) | |
| Anastomosis performed (%) | No | 128 (12.4) | 123 (12.5) | 3 (7.3) |
| Yes | 908 (87.6) | 858 (87.5) | 38 (92.7) | |
| Stoma placed (%) | No | 310 (29.8) | 301 (30.6) | 8 (19.5) |
| Yes | 729 (70.2) | 683 (69.4) | 33 (80.5) | |
| Drain placed (%) | No | 197 (32.7) | 190 (32.9) | 7 (28.0) |
| Yes | 406 (67.3) | 388 (67.1) | 18 (72.0) | |
| Intraoperative complication (%) | No | 633 (96.3) | 596 (96.3) | 26 (96.3) |
| Yes | 24 (3.7) | 23 (3.7) | 1 (3.7) | |
| Intraoperative perforation (%) | No | 615 (98.7) | 581 (98.6) | 25 (100.0) |
| Yes | 8 (1.3) | 8 (1.4) | 0 (0.0) | |
| Other intraoperative complication (%) | No | 612 (99.2) | 577 (99.1) | 25 (100.0) |
| Pancreas, liver, choledo, gallbladder | 2 (0.3) | 1 (0.2) | 0 (0.0) | |
| Bladder requiring sutures | 2 (0.3) | 2 (0.3) | 0 (0.0) | |
| Other | 1 (0.2) | 2 (0.3) | 0 (0.0) | |
| Operative time (median [IQR]) | 245.00 [195.00, 300.00] | 243.00 [195.00, 300.00] | 260.00 [182.00, 338.00] | |
| pT (%) | pT0 | 79 (7.8) | 78 (8.0) | 0 (0.0) |
| pT1 | 102 (10.0) | 101 (10.3) | 1 (2.4) | |
| pT2 | 312 (30.7) | 301 (30.7) | 8 (19.5) | |
| pT3 | 499 (49.1) | 463 (47.2) | 27 (65.9) | |
| pT4 | 25 (2.5) | 21 (2.1) | 4 (9.8) | |
| pN (%) | pN0 | 667 (64.8) | 645 (66.1) | 14 (35.0) |
| pN1 | 285 (27.7) | 265 (27.2) | 15 (37.5) | |
| pN2 | 78 (7.6) | 66 (6.8) | 11 (27.5) | |
| pM (%) | pM0 | 732 (92.7) | 695 (93.0) | 28 (84.8) |
| pM1 | 58 (7.3) | 52 (7.0) | 5 (15.2) | |
| Lymph nodes harvested (median [IQR]) | 15.00 [11.00, 21.00] | 15.00 [11.00, 21.00] | 15.00 [9.00, 22.00] | |
| Number of positive lymph nodes harvested (median [IQR]) | 0.00 [0.00, 1.00] | 0.00 [0.00, 1.00] | 1.00 [0.00, 3.75] | |
| CRM (%) | CRM− | 935 (96.0) | 891 (96.5) | 32 (84.2) |
| CRM+ | 39 (4.0) | 32 (3.5) | 6 (15.8) | |
| DRM (median [IQR]) | 10.00 [10.00, 30.00] | 10.00 [10.00, 30.00] | 10.00 [5.00, 20.00] | |
| Completeness of resection (%) | Incomplete | 24 (3.2) | 23 (3.3) | 0 (0.0) |
| Nearly complete | 67 (9.1) | 61 (8.7) | 6 (21.4) | |
| Complete | 649 (87.7) | 617 (88.0) | 22 (78.6) | |
| Pathological resection radicality (%) | R0 | 946 (95.6) | 904 (96.3) | 31 (79.5) |
| R1 | 37 (3.7) | 30 (3.2) | 6 (15.4) | |
| R2 | 7 (0.7) | 5 (0.5) | 2 (5.1) | |
| Pathological histology (%) | Adenocarcinoma | 789 (92.3) | 749 (92.8) | 32 (86.5) |
| Mucinous | 54 (6.3) | 48 (5.9) | 4 (10.8) | |
| Signet cell | 1 (0.1) | 1 (0.1) | 0 (0.0) | |
| Other | 11 (1.3) | 9 (1.1) | 1 (2.7) | |
| Pathological perforation (%) | No | 489 (98.0) | 466 (97.9) | 22 (100.0) |
| Yes | 10 (2.0) | 10 (2.1) | 0 (0.0) | |
| Postoperative complications (%) | No | 544 (53.2) | 514 (53.1) | 21 (51.2) |
| Yes | 478 (46.8) | 454 (46.9) | 20 (48.8) | |
| Postoperative complications within 30 days (%) | No | 366 (58.5) | 341 (57.8) | 17 (65.4) |
| Yes | 260 (41.5) | 249 (42.2) | 9 (34.6) | |
| Ileus (%) | No | 525 (86.5) | 498 (86.8) | 19 (76.0) |
| Yes | 82 (13.5) | 76 (13.2) | 6 (24.0) | |
| Wound infection (%) | No | 566 (93.1) | 534 (93.2) | 23 (92.0) |
| Yes | 42 (6.9) | 39 (6.8) | 2 (8.0) | |
| Bleeding (%) | No | 804 (95.3) | 757 (95.1) | 36 (97.3) |
| Yes | 40 (4.7) | 39 (4.9) | 1 (2.7) | |
| Other postoperative complications (%) | No | 414 (68.7) | 386 (68.2) | 19 (73.1) |
| Yes | 54 (9.0) | 50 (8.8) | 3 (11.5) | |
| Infectious | 8 (1.3) | 7 (1.2) | 1 (3.8) | |
| Neurologic | 4 (0.7) | 4 (0.7) | 0 (0.0) | |
| Urological | 21 (3.5) | 21 (3.7) | 0 (0.0) | |
| Other non-surgical | 18 (3.0) | 18 (3.2) | 0 (0.0) | |
| Abscess | 7 (1.2) | 7 (1.2) | 0 (0.0) | |
| Fascia dehiscence | 1 (0.2) | 1 (0.2) | 0 (0.0) | |
| Bowel perforation | 5 (0.8) | 4 (0.7) | 0 (0.0) | |
| Leakage of bladder/ureter | 1 (0.2) | 1 (0.2) | 0 (0.0) | |
| Other surgical complication | 45 (7.5) | 45 (8.0) | 0 (0.0) | |
| Pulmonary | 13 (2.2) | 11 (1.9) | 2 (7.7) | |
| Cardiac | 11 (1.8) | 11 (1.9) | 0 (0.0) | |
| Thromboembolic | 1 (0.2) | 0 (0.0) | 1 (3.8) | |
| Clavien–Dindo (%) | None | 544 (53.2) | 514 (53.1) | 21 (51.2) |
| I | 117 (11.4) | 111 (11.5) | 6 (14.6) | |
| II | 190 (18.6) | 184 (19.0) | 5 (12.2) | |
| IIIa | 37 (3.6) | 32 (3.3) | 5 (12.2) | |
| IIIb | 103 (10.1) | 96 (9.9) | 4 (9.8) | |
| IV | 21 (2.1) | 21 (2.1) | 0 (0) | |
| V | 10 (1.0) | 10 (1.0) | 0 (0) | |
| Anastomotic leakage (%) | No | 731 (85.0) | 695 (85.0) | 27 (87.1) |
| Yes | 129 (15.0) | 123 (15.0) | 4 (12.9) | |
| Reintervention within 31 days (%) | No | 919 (88.6) | 870 (88.5) | 38 (92.7) |
| Yes | 118 (11.4) | 113 (11.5) | 3 (7.3) | |
| Readmission within 31 days (%) | No | 924 (89.1) | 876 (89.1) | 36 (87.8) |
| Yes | 113 (10.9) | 107 (10.9) | 5 (12.2) | |
| Length of stay (postoperative) (median (IQR)) | 7.00 [5.00, 11.00] | 7.00 [5.00, 11.00] | 11.00 [6.00, 17.00] | |
| Adjuvant chemotherapy (%) | No | 694 (70.5) | 664 (70.8) | 24 (61.5) |
| Yes | 291 (29.5) | 274 (29.2) | 15 (38.5) | |
| Systemic recurrence (%) | No | 852 (83.0) | 825 (83.8) | 26 (63.4) |
| Yes | 175 (17.0) | 159 (16.2) | 15 (36.6) | |
| Local recurrence (%) | No | 984 (96.0) | 984 (100) | 0 (0) |
| Yes | 41 (4.0) | 0 (0) | 41 (100) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geitenbeek, R.T.J.; Duhoky, R.; Burghgraef, T.A.; Piozzi, G.N.; Masum, S.; Hopgood, A.A.; Denost, Q.; van Eetvelde, E.; Bianchi, P.; Rouanet, P.; et al. Analysis of Local Recurrence After Robotic-Assisted Total Mesorectal Excision (ALRITE): An International, Multicentre, Retrospective Cohort. Cancers 2025, 17, 992. https://doi.org/10.3390/cancers17060992
Geitenbeek RTJ, Duhoky R, Burghgraef TA, Piozzi GN, Masum S, Hopgood AA, Denost Q, van Eetvelde E, Bianchi P, Rouanet P, et al. Analysis of Local Recurrence After Robotic-Assisted Total Mesorectal Excision (ALRITE): An International, Multicentre, Retrospective Cohort. Cancers. 2025; 17(6):992. https://doi.org/10.3390/cancers17060992
Chicago/Turabian StyleGeitenbeek, Ritch T. J., Rauand Duhoky, Thijs A. Burghgraef, Guglielmo Niccolò Piozzi, Shamsul Masum, Adrian A. Hopgood, Quentin Denost, Ellen van Eetvelde, Paolo Bianchi, Philippe Rouanet, and et al. 2025. "Analysis of Local Recurrence After Robotic-Assisted Total Mesorectal Excision (ALRITE): An International, Multicentre, Retrospective Cohort" Cancers 17, no. 6: 992. https://doi.org/10.3390/cancers17060992
APA StyleGeitenbeek, R. T. J., Duhoky, R., Burghgraef, T. A., Piozzi, G. N., Masum, S., Hopgood, A. A., Denost, Q., van Eetvelde, E., Bianchi, P., Rouanet, P., Hompes, R., Gómez Ruiz, M., Briggs, J., Khan, J. S., Consten, E. C. J., & on behalf of the ALRITE Study Group. (2025). Analysis of Local Recurrence After Robotic-Assisted Total Mesorectal Excision (ALRITE): An International, Multicentre, Retrospective Cohort. Cancers, 17(6), 992. https://doi.org/10.3390/cancers17060992