
Primary or Interval Debulking Surgery for Advanced Endometrial Cancer with Carcinosis: A Systematic Review and Individual Patient Data Meta-Analysis of Survival Outcomes
 , , , ,
, , , ,  ,
, 

Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Database Queries and Study Selection
2.2. Data Extraction, Quality Assessment, and Statistical Analysis
3. Results
3.1. Article Screening Selection, Quality Assessment, and Description of Included Studies

{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Study Design, Enrollment Period | Age (Years) | Stages Included (Whole Cohort) | N. of Stage IVb pts with Peritoneal Dissemination | Extra-Abdominal Metastases | Abdominal Tumor Load | Histology |
|---|---|---|---|---|---|---|---|
| Bristow [22] 2000 USA | Retrospective Multicenter 1990–1998 | median 65 | IVb n = 65 | 65 | 9/65 Included in meta-analysis: 0/8 | pelvis 75.4% abdominal peritoneum 49.2% omentum 47.7% bowel serosa or mesentery 36.9% upper abdomen 24.6% (whole cohort) Included in meta-analysis: pelvis 7/8 abdominal peritoneum 5/8 omentum 3/8 bowel 2/8 | 21 serous 22 endometrioid 22 others (whole cohort) |
| Landrum [23] 2009 USA | Retrospective 1990–2006 | median 63 | IVb n = 55 | 55 | 0 | N.A. | 29 serous 24 endometrioid 2 clear cell (whole cohort) |
| Lee [24] 2014 USA | Retrospective Multicenter 1980–2011 | median 70 | IVb n = 48 | 48 | 0 | excluded unresectable disease 23 omentum only 25 extensive abdominal involvement | serous |
| Ueda [25] 2010 Japan | Retrospective 1991–2008 | median 63 | IVb n = 33 | 15 | 0 | abdominal peritoneum 42% omentum 39% retroperitoneal nodes 55% bowel/mesentery 21% (whole cohort) | 9 serous/clear cell 24 endometrioid (whole cohort) |
| Gehrig [26] 2004 USA | Retrospective 1990–2000 | median 68 | III–IV n = 24 | 11 | 0 | omental involvement | serous |
| Watari [27] 2005 Japan | Retrospective 1982–2002 | median 58 | IIIC–IV n = 55 | 11 | 0 | N.A. | 12 serous/clear cell 43 endometrioid (whole cohort) |
| Gitsch [28] 1994 Australia | Retrospective 1988–1993 | mean 73 | I–IV n = 18 | 4 | 0 | Included in meta-analysis: diaphragm 2/3 omentum 1/3 | serous |
| Nguyen [29] 2001 USA | Retrospective 1989–1998 | mean 65 | I–IV n = 22 | 1 | 0 | omental involvement | serous |
| Low [30] 2005 Singapore | Retrospective 1994–2003 | median 62 | I–IV n = 26 | 1 | 0 | N.A. | serous |
| Kelly [31] 2004 USA | Retrospective 1987–2002 | mean 68 | I–IV n = 51 | 9 | 0 | omental involvement | serous |
| Author, Year, Country | Abdominal RT After Surgery | Adjuvant Therapy | AC Regimens | Results | Included Patients For Meta-Analysis a | ||
| Bristow [22] 2000 USA | 26 RT = 0 cm 10 RT ≤ 1 cm 29 RT > 1 cm (4 no hysterectomy) Included in meta-analysis: 6 RT = 0 cm 1 RT ≤ 1 cm 1 RT > 1 cm | 27 CT 14 CT + RTx 11 RTx 3 HT 3 no therapy 7 unknown Included in meta-analysis: 3 CT 5 CT + RTx | platinum-based | Pts who received a treatment sequence of CT followed by RTx had a median survival rate of 40.0 months, compared to only 14.0 months for pts not receiving this combination (p = 0.004) The median survival of all pts undergoing optimal cytoreduction (≤1 cm RT) was 34.3 months, compared to 11.0 months for patients left with suboptimal RT (p = 0.0001) On MVA, only age and RT ≤ 1 cm retained significance as predictors of survival | 8 OS | ||
| Landrum [23] 2009 USA | 48 RT ≤ 1 cm (whole cohort) | 33 CT 14 CT + RTx 8 RTx | platinum-based | Median PFS for all patients (optimal and suboptimal cytoreduction) was 13 months Optimal cytoreduction was associated with a survival advantage with an HR of 2.4 At 2 years, OS for all patients treated with PDS and adjuvant CT was 53% | 47 OS | ||
| Lee [24] 2014 USA | 22 RT = 0 cm 14 RT < 1 cm 4 RT = 2–5 cm 5 RT > 5 cm 3 RT unknown (whole cohort) | 19 CT 16 CT + RTx 5 RTx 8 no therapy | platinum-based | At 5 years, DFS and OS rates were 12% and 19% On MVA, among pts treated with CT, optimal surgical cytoreduction (HR 0.09, 95% CI 0.02–0.35) and RTx (HR 0.36, 95% CI 0.15–0.80) were associated with a decreased rate of recurrence or progression Optimal cytoreductive surgery (HR 0.09, 95% CI 0.02–0.38) was the only significant prognostic factor for OS when the model was adjusted for age | 35 PFS | ||
| Ueda [25] 2010 Japan | 10 RT ≤ 2 cm 5 RT > 2 cm | 15 CT | platinum-based at least 90% c | Median OS RT ≤ 2 cm was 19 months vs. 6 months if RT > 2 cm (p = 0.0007) Median PFS RT ≤ 2 cm was 10 months vs. 1 months if RT > 2 cm (p = 0.0003) | 15 OS & PFS | ||
| Gehrig [26] 2004 USA | 7 RT = 0 cm 4 RT > 0 cm Included in meta-analysis: 6 RT = 0 cm, 4 RT > 0 cm | 10 CT 1 RTx | platinum-based | In the whole cohort (stages III and IV) time to progression for pts receiving RTx was 5.3 months as compared with 12.4 months for pts receiving CT (p = 0.01) Mean time to death for the RTx group was 8 months compared to 18 months in the CT group (p = 0.04) | 10 OS | ||
| Watari [27] 2005 Japan | N.A. | 11 CT | platinum-based | 5-year survival rate of stage IV pts was 20% | 11 OS | ||
| Gitsch [28] 1994 Australia | 2 RT < 2 cm 2 RT > 2 cm Included in meta-analysis: 2 RT < 2 cm, 1 RT > 2 cm | 1 CT 2 CT + RTx 1 no therapy | platinum-based | Of the pts with stages III and IV disease, 4 of 12 are alive with no evidence of disease after a mean follow-up of 22.5 months (range, 8–45 months) Eight of 12 women who received CT are alive with no evidence of disease, 4 of whom had stage III or IV disease | 3 OS | ||
| Nguyen [29] 2001 USA | RT = 0 | 1 CT | platinum-based | The projected 2-year survival was 40% for pts with stages III and IV as compared with 60% for pts with stages I and II | 1 OS | ||
| Low [30] 2005 Singapore | minimal RT | 1 CT + RTx | platinum-based | The OS at 5 years was 72.9% for stage I, 100% for stage II, 58.9% for stage III, and 0% for stage IV | 1 OS | ||
| Kelly [31] 2004 USA | 8 RT < 2 cm 1 RT > 2 cm | at least 8 CT b | platinum-based | Eight of the 10 stage IIIC/IV pts either progressed or recurred, and their median DFS was 6 months (range, 0–24 months) | 9 OS | ||
| Author, Year, Country | Study Design, Enrollment Period | Age (Years) | Stages Included (Whole Cohort) | N. of pts Stage IVb with Peritoneal Dissemination | Extra-Abdominal Metastases | Abdominal Tumor Load | Histology | N. of NACT Cycles | Response to NACT |
|---|---|---|---|---|---|---|---|---|---|
| Vandenput [21] 2009 Belgium | Prospective 1999–2007 | median 65 | IVb n = 30 | 30 | some may have had pleural effusion | N.A. | 27 serous 2 endometrioid 1 clear cell (whole cohort) | 3–4 | 2 CR 20 PR 6 SD 2 PD (no IDS) |
| Lim [32] 2022 Korea | Retrospective Multicenter 2008–2020 | median 56 | IIIC–IVb n = 32 | 10 | 8/10 | “unresectable” | 2 serous 5 endometrioid 3 carcinosarcoma | median 6 | 10 PR |
| Jani [33] 2021 USA | Retrospective 2003–2019 | median 63 | III–IV n = 40 | 22 b | pleural effusion 9/40 lung metastasis 3/40 liver 4/40 | carcinomatosis 32.5% omental caking 32.5% ascites 55% extensive nodal involvement 55% bowel/mesentery 7.5% (whole cohort) Included in meta-analysis: at least omentum 22/22 | 18 serous 2 endometrioid 6 clear cell 9 carcinosarcoma 2 mixed 3 undifferentiated (whole cohort) | 25 pts 3–4 15 pts ≥ 5 (whole cohort) | 3 CR 29 PR 6 SD 2 PD (whole cohort) |
| Author, Year, Country | NACT Regimens | Abdominal RT After Surgery | Adjuvant Therapy | AC Regimens | Results | Included Patients for Meta-Analysis a | |||
| Vandenput [21] 2009 Belgium | platinum-based | 22 RT = 0 cm 2 RT < 1 cm | 24 CT | 22 platinum-based 2 “switch” to other type | Histopathological features of chemoresponse in both uterus and omentum were related to a better PFS (p = 0.017, HR = 0.785) and OS (p = 0.014, HR = 0.707) The use of NACT resulted in a high rate (80%) of optimal IDS | 24 OS & PFS c | |||
| Lim [32] 2022 Korea | platinum-based | 9 RT = 0 cm 1 RT ≤ 1 cm | 10 CT | 9 platinum-based 1 ifosfamide–paclitaxel | On MVA, non-endometrioid histology and RT after IDS were independent poor prognostic factors for PFS (adjusted HR 7.322, p < 0.001; and 5.934, p = 0.001, respectively) On UVA non-endometrioid histology was the only factor associated with worse OS (adjusted HR 4.523, p = 0.0032) | 10 OS & PFS | |||
| Jani [33] 2021 USA | platinum-based | 23 RT = 0 6 RT < 1 cm 11 RT ≥ 1 cm (whole cohort) | N.A. | N.A. | Pts with higher chemotherapy response scores had longer PFS and OS and a higher rate of complete cytoreduction | 22 OS & PFS | |||
| Author, Year, Country | Study Design, Enrollment Period | Age (Years) | Stages Included (Whole Cohort) | N. of pts Stage IVb with Peritoneal Dissemination | N. of pts PDS/IDS | Extra-Abdominal Metastases | Abdominal Tumor Load | Histology | N. of NACT Cycles | Response to NACT |
|---|---|---|---|---|---|---|---|---|---|---|
| Bogani [9] 2019 Italy | Retrospective propensity-matched 2005–2016 | PDS mean 65, IDS mean 63 | IVb n = 30 | 30 | 15/15 | 0 | unresectable disease in patients undergoing NACT | all serous | 3–6 | N.A. |
| Unsal [34] 2022 Turkey | Retrospective multicenter N.A. | median 64 | IVb n = 42 | 42 | 32/10 | 0 | omental involvement 88.1% no other information | all serous | 3–8 | N.A. |
| Rajkumar [35] 2019 UK | Retrospective multicenter 2010–2016 | 22 pts < 65, 23 pts ≥ 65 | IIIC–IVb n = 45 | 13 | 6/7 | 1/7 IDS | PDS: omentum 2/6, pelvis 5/6, bowel 1/6, retroperitoneal nodes 4/6 IDS: omentum 5/7, pelvis 5/7, bowel 1/7, retroperitoneal nodes 1/7, upper abdomen 1/7 | PDS: 3 serous, 3 endometrioid IDS: 2 serous, 3 endometrioid, 1 clear cell, 1 mixed | 3–6 | N.A. |
| Author, Year, Country | NACT regimens | Abdominal RT after Surgery | Adjuvant therapy | AC regimens | Results | Included Patients for Meta-Analysis a | ||||
| PDS | IDS | |||||||||
| Bogani [9] 2019 Italy | All platinum-based | PDS: 13 RT = 0 cm, 2 RT < 1 cm IDS: 14 RT = 0 cm, 1 RT < 1 cm | PDS: 15 CT IDS: 14 CT, 1 CT + RTx | All platinum-based except 1 treated with gemcitabine in the IDS group | Similar cytoreduction rate Median DFS was 12.0 vs. 15.3 months in the IDS vs. PDS group (p = 0.663) Median OS was 16.7 vs. 18.0 months in the IDS vs. PDS group (p = 0.349) | 15 OS & PFS b | 15 OS & PFS | |||
| Unsal [34] 2022 Turkey | All platinum-based | PDS: 26 RT = 0, 6 RT > 0 IDS: 8 RT = 0, 2 RT > 0 | PDS: 32 CT IDS: not clear | all platinum-based | Receiving NACT did not affect DFS and DSS in UVA | 32 OS & PFS | 10 OS & PFS | |||
| Rajkumar [35] 2019 UK | >90% Platinum-based 1 capecitabine in the whole NACT cohort | PDS: 5 RT ≤ 1 cm, 1 RT > 1 cm IDS: 6 RT ≤ 1 cm, 1 RT > 1 cm | PDS: 6 CT ± RTx c,d IDS: 7 CT ± RTx d | all platinum-based | Only poor performance status (p = 0.035), presence of bowel disease (p = 0.05) and suboptimal cytoreduction (p = 0.006) retained significance as predictors of poor survival on MVA Suboptimal cytoreduction surgery, compared to optimal cytoreduction, showed a 3.55-fold increased risk of death independent of performance status and anatomic region with disease (HR 3.55 (95% CI 1.44–8.73), p = 0.006) | 6 OS | 7 OS | |||
3.2. Clinical and Pathological Features
3.3. Neoadjuvant/Adjuvant Treatment and Residual Tumor
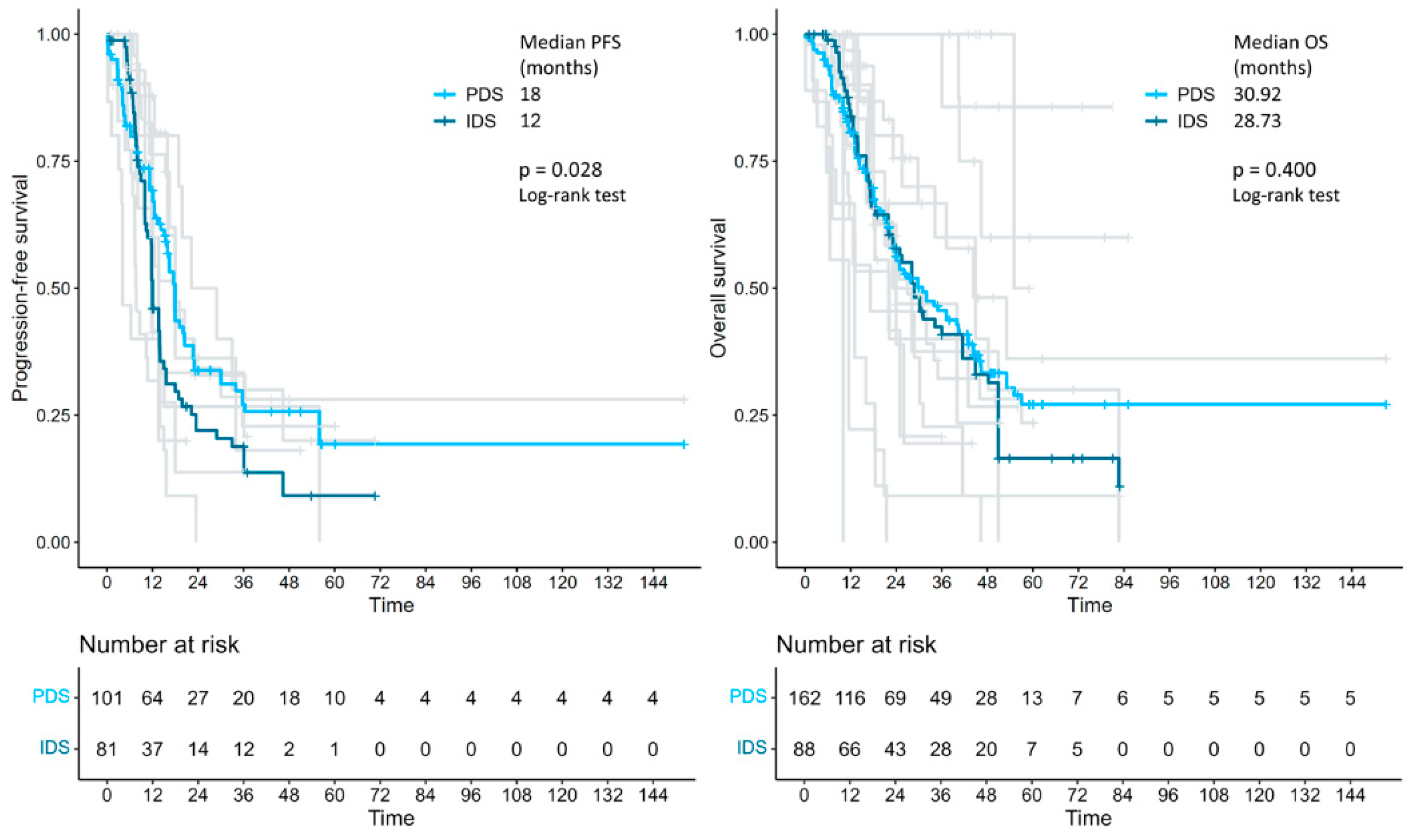
3.4. Individual Patient Data Meta-Analysis of Survival Outcomes
4. Discussion
4.1. Summary of Main Results
4.2. Results in the Context of Published Literature
4.3. Strengths and Weaknesses
4.4. Implications for Practice and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Today. Available online: https://gco.iarc.who.int/today/ (accessed on 16 May 2024).
- Cancer of the Endometrium—Cancer Stat Facts. SEER. Available online: https://seer.cancer.gov/statfacts/html/corp.html (accessed on 16 May 2024).
- Berek, J.S.; Matias-Guiu, X.; Creutzberg, C.; Fotopoulou, C.; Gaffney, D.; Kehoe, S.; Lindemann, K.; Mutch, D.; Concin, N.; Endometrial Cancer Staging Subcommittee; et al. FIGO staging of endometrial cancer: 2023. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2023, 162, 383–394. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Petrillo, M.; Vizzielli, G.; Fanfani, F.; Gallotta, V.; Cosentino, F.; Chiantera, V.; Legge, F.; Carbone, V.; Scambia, G.; Fagotti, A. Definition of a dynamic laparoscopic model for the prediction of incomplete cytoreduction in advanced epithelial ovarian cancer: Proof of a concept. Gynecol. Oncol. 2015, 139, 5–9. [Google Scholar] [CrossRef]
- Perrone, A.M.; Coada, C.A.; Ravegnini, G.; De Leo, A.; Damiano, G.; De Crescenzo, E.; Tesei, M.; Di Costanzo, S.; Genovesi, L.; Rubino, D.; et al. Post-operative residual disease and number of cycles of neoadjuvant chemotherapy in advanced epithelial ovarian carcinoma. Int. J. Gynecol. Cancer 2023, 33, 1270–1278. [Google Scholar] [CrossRef]
- Coada, C.A.; Dondi, G.; Ravegnini, G.; Di Costanzo, S.; Tesei, M.; Fiuzzi, E.; Di Stanislao, M.; Giunchi, S.; Zamagni, C.; Bovicelli, A.; et al. Optimal number of neoadjuvant chemotherapy cycles prior to interval debulking surgery in advanced epithelial ovarian cancer: A systematic review and meta-analysis of progression-free survival and overall survival. J. Gynecol. Oncol. 2023, 34, e82. [Google Scholar] [CrossRef]
- de Lange, N.M.; Ezendam, N.P.M.; Kwon, J.S.; Vandenput, I.; Mirchandani, D.; Amant, F.; van der Putten, L.J.M.; Pijnenborg, J.M.A. Neoadjuvant chemotherapy followed by surgery for advanced-stage endometrial cancer. Curr. Oncol. Tor. Ont. 2019, 26, e226–e232. [Google Scholar] [CrossRef]
- Bogani, G.; Ditto, A.; Leone Roberti Maggiore, U.; Scaffa, C.; Mosca, L.; Chiappa, V.; Martinelli, F.; Lorusso, D.; Raspagliesi, F. Neoadjuvant chemotherapy followed by interval debulking surgery for unresectable stage IVB Serous endometrial cancer. Tumori J. 2019, 105, 92–97. [Google Scholar] [CrossRef]
- Huang, A.B.; Wu, J.; Chen, L.; Albright, B.B.; Previs, R.A.; Moss, H.A.; Davidson, B.A.; Havrilesky, L.J.; Melamed, A.; Wright, J.D. Neoadjuvant chemotherapy for advanced stage endometrial cancer: A systematic review. Gynecol. Oncol. Rep. 2021, 38, 100887. [Google Scholar] [CrossRef]
- Capozzi, V.A.; Scarpelli, E.; De Finis, A.; Rotondella, I.; Scebba, D.; Gallinelli, A.; Montrucchio, C.; Martignon, G.; Leotta, M.; Ghi, T.; et al. Optimal Management for Stage IVB Endometrial Cancer: A Systematic Review. Cancers 2023, 15, 5123. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic Version 1.2025—September 11, 2024 NCCN.org. NCCN. Available online: https://www.nccn.org/guidelines/guidelines-detail (accessed on 3 March 2024).
- Miller, D.S.; Filiaci, V.L.; Mannel, R.S.; Cohn, D.E.; Matsumoto, T.; Tewari, K.S.; DiSilvestro, P.; Pearl, M.L.; Argenta, P.A.; Powell, M.A.; et al. Carboplatin and Paclitaxel for Advanced Endometrial Cancer: Final Overall Survival and Adverse Event Analysis of a Phase III Trial (NRG Oncology/GOG0209). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 3841–3850. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Shepherd, J.H. Revised FIGO staging for gynaecological cancer. Br. J. Obstet. Gynaecol. 1989, 96, 889–892. [Google Scholar] [CrossRef]
- Pecorelli, S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int. J. Gynaecol. Obstet. 2009, 105, 103–104. [Google Scholar] [CrossRef]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef]
- R Core Team. European Environment Agency, 2020. Available online: https://www.eea.europa.eu/data-and-maps/indicators/oxygen-consuming-substances-in-rivers/r-development-core-team-2006 (accessed on 1 May 2024).
- Rogula, B.; Lozano-Ortega, G.; Johnston, K.M. A Method for Reconstructing Individual Patient Data From Kaplan-Meier Survival Curves That Incorporate Marked Censoring Times. MDM Policy Pract. 2022, 7, 23814683221077643. [Google Scholar] [CrossRef]
- Kassambara, A.; Kosinski, M.; Biecek, P.; Fabian, S. Survminer: Drawing Survival Curves using “ggplot2”. 9 March 2021. Available online: https://cran.r-project.org/web/packages/survminer/index.html (accessed on 7 July 2024).
- Vandenput, I.; Van Calster, B.; Capoen, A.; Leunen, K.; Berteloot, P.; Neven, P.; Moerman, P.; Vergote, I.; Amant, F. Neoadjuvant chemotherapy followed by interval debulking surgery in patients with serous endometrial cancer with transperitoneal spread (stage IV): A new preferred treatment? Br. J. Cancer 2009, 101, 244–249. [Google Scholar] [CrossRef]
- Bristow, R.E.; Zerbe, M.J.; Rosenshein, N.B.; Grumbine, F.C.; Montz, F.J. Stage IVB endometrial carcinoma: The role of cytoreductive surgery and determinants of survival. Gynecol. Oncol. 2000, 78, 85–91. [Google Scholar] [CrossRef]
- Landrum, L.M.; Moore, K.N.; Myers, T.K.; Lanneau, G.S., Jr.; McMeekin, D.S.; Walker, J.L.; Gold, M.A. Stage IVB endometrial cancer: Does applying an ovarian cancer treatment paradigm result in similar outcomes? A case-control analysis. Gynecol. Oncol. 2009, 112, 337–341. [Google Scholar] [CrossRef]
- Lee, L.J.; Demaria, R.; Berkowitz, R.; Matulonis, U.; Viswanathan, A.N. Clinical predictors of long-term survival for stage IVB uterine papillary serous carcinoma confined to the abdomen. Gynecol. Oncol. 2014, 132, 65–69. [Google Scholar] [CrossRef]
- Ueda, Y.; Enomoto, T.; Miyatake, T.; Egawa-Takata, T.; Ugaki, H.; Yoshino, K.; Fujita, M.; Kimura, T. Endometrial carcinoma with extra-abdominal metastasis: Improved prognosis following cytoreductive surgery. Ann. Surg. Oncol. 2010, 17, 1111–1117. [Google Scholar] [CrossRef]
- Gehrig, P.A.; Morris, D.E.; Van Le, L. Uterine serous carcinoma: A comparison of therapy for advanced-stage disease. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2004, 14, 515–520. [Google Scholar] [CrossRef]
- Watari, H.; Todo, Y.; Takeda, M.; Ebina, Y.; Yamamoto, R.; Sakuragi, N. Lymph-vascular space invasion and number of positive para-aortic node groups predict survival in node-positive patients with endometrial cancer. Gynecol. Oncol. 2005, 96, 651–657. [Google Scholar] [CrossRef]
- Gitsch, G.; Friedlander, M.L.; Wain, G.V.; Hacker, N.F. Uterine papillary serous carcinoma. A clinical study. Cancer 1995, 75, 2239–2243. [Google Scholar] [CrossRef]
- Nguyen, N.P.; Sallah, S.; Karlsson, U.; Vos, P.; Ludin, A.; Semer, D.; Tait, D.; Salehpour, M.; Jendrasiak, G.; Robiou, C. Prognosis for papillary serous carcinoma of the endometrium after surgical staging. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2001, 11, 305–311. [Google Scholar] [CrossRef]
- Low, J.S.; Wong, E.H.; Tan, H.S.; Yap, S.P.; Chua, E.J.; Sethi, V.K.; Soh, L.T.; Low, J.; Tay, E.H.; Chew, S.H. Adjuvant sequential chemotherapy and radiotherapy in uterine papillary serous carcinoma. Gynecol. Oncol. 2005, 97, 171–177. [Google Scholar] [CrossRef]
- Kelly, M.G.; O’Malley, D.; Hui, P.; McAlpine, J.; Dziura, J.; Rutherford, T.J.; Azodi, M.; Chambers, S.K.; Schwartz, P.E. Patients with uterine papillary serous cancers may benefit from adjuvant platinum-based chemoradiation. Gynecol. Oncol. 2004, 95, 469–473. [Google Scholar] [CrossRef]
- Lim, H.; Bang, S.H.; Kim, Y.; Cho, S.H.; Shin, W.; Kim, S.I.; Kim, T.H.; Suh, D.H.; Lim, M.C.; Kim, J.W.; et al. Clinical implications of neoadjuvant chemotherapy in advanced endometrial cancer: A multi-center retrospective cohort study. BMC Cancer 2022, 22, 703. [Google Scholar] [CrossRef]
- Jani, I.; Lastra, R.R.; Brito, K.S.; Liao, C.; Lazo, I.; Lee, N.K.; Yamada, S.D.; Kurnit, K.C. Chemotherapy response score as a prognostic tool in patients with advanced stage endometrial carcinoma treated with neoadjuvant chemotherapy. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2021, 31, 852–858. [Google Scholar] [CrossRef]
- Unsal, M.; Kilic, C.; Cakir, C.; Kilic, F.; Ersak, B.; Karakas, S.; Tokgozoglu, N.; Varli, B.; Oktar, O.; Kimyon Comert, G.; et al. Neoadjuvant chemotherapy in patients with stage IVB uterine serous carcinoma: A Turkish multicentric study. J. Obstet. Gynaecol. 2023, 43, 2151355. [Google Scholar] [CrossRef]
- Rajkumar, S.; Nath, R.; Lane, G.; Mehra, G.; Begum, S.; Sayasneh, A. Advanced stage (IIIC/IV) endometrial cancer: Role of cytoreduction and determinants of survival. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 234, 26–31. [Google Scholar] [CrossRef]
- Tobias, C.J.; Chen, L.; Melamed, A.; St Clair, C.; Khoury-Collado, F.; Tergas, A.I.; Hou, J.Y.; Hur, C.; Ananth, C.V.; Neugut, A.I.; et al. Association of Neoadjuvant Chemotherapy With Overall Survival in Women With Metastatic Endometrial Cancer. JAMA Netw. Open 2020, 3, e2028612. [Google Scholar] [CrossRef] [PubMed]
- Eto, T.; Saito, T.; Shimokawa, M.; Hatae, M.; Takeshima, N.; Kobayashi, H.; Kasamatsu, T.; Yoshikawa, H.; Kamura, T.; Konishi, I.; et al. Status of treatment for the overall population of patients with stage IVb endometrial cancer, and evaluation of the role of preoperative chemotherapy: A retrospective multi-institutional study of 426 patients in Japan. Gynecol. Oncol. 2013, 131, 574–580. [Google Scholar] [CrossRef]
- Wilkinson-Ryan, I.; Frolova, A.I.; Liu, J.; Stewart Massad, L.; Thaker, P.H.; Powell, M.A.; Mutch, D.G.; Hagemann, A.R. Neoadjuvant chemotherapy versus primary cytoreductive surgery for stage IV uterine serous carcinoma. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2015, 25, 63–68. [Google Scholar] [CrossRef]
- Thomas, M.B.; Mariani, A.; Cliby, W.A.; Keeney, G.L.; Podratz, K.C.; Dowdy, S.C. Role of cytoreduction in stage III and IV uterine papillary serous carcinoma. Gynecol. Oncol. 2007, 107, 190–193. [Google Scholar] [CrossRef]
- Chi, D.S.; Welshinger, M.; Venkatraman, E.S.; Barakat, R.R. The role of surgical cytoreduction in Stage IV endometrial carcinoma. Gynecol. Oncol. 1997, 67, 56–60. [Google Scholar] [CrossRef]
- Goff, B.A.; Goodman, A.; Muntz, H.G.; Fuller, A.F., Jr.; Nikrui, N.; Rice, L.W. Surgical stage IV endometrial carcinoma: A study of 47 cases. Gynecol. Oncol. 1994, 52, 237–240. [Google Scholar] [CrossRef]
- Albright, B.B.; Monuszko, K.A.; Kaplan, S.J.; Davidson, B.A.; Moss, H.A.; Huang, A.B.; Melamed, A.; Wright, J.D.; Havrilesky, L.J.; Previs, R.A. Primary cytoreductive surgery for advanced stage endometrial cancer: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 225, e1–e237. [Google Scholar] [CrossRef]
- Kanno, M.; Yunokawa, M.; Kurihara, N.; Aoki, Y.; Omi, M.; Tanigawa, T.; Kanao, H. Efficacy of intra-abdominal cytoreductive surgery in advanced endometrial cancer with distant metastasis. J. Gynecol. Oncol. 2023, 34, e77. [Google Scholar] [CrossRef]
- Lyman, G.H.; Kuderer, N.M. The strengths and limitations of meta-analyses based on aggregate data. BMC Med. Res. Methodol. 2005, 5, 14. [Google Scholar] [CrossRef]
- de Biase, D.; Maloberti, T.; Corradini, A.G.; Rosini, F.; Grillini, M.; Ruscelli, M.; Coluccelli, S.; Altimari, A.; Gruppioni, E.; Sanza, V.; et al. Integrated clinicopathologic and molecular analysis of endometrial carcinoma: Prognostic impact of the new ESGO-ESTRO-ESP endometrial cancer risk classification and proposal of histopathologic algorithm for its implementation in clinical practice. Front. Med. 2023, 10, 1146499. [Google Scholar] [CrossRef]
- Chacon, E.; Boria, F.; Lyer, R.R.; Fanfani, F.; Malzoni, M.; Bretová, P.; Luzarraga Aznar, A.; Fruscio, R.; Jedryka, M.A.; Tóth, R.; et al. SENECA study: Staging endometrial cancer based on molecular classification. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2024, 34, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]


| PDS N = 197 | IDS N = 88 | p-Value | |
|---|---|---|---|
| Histology—n (%): | <0.001 | ||
| Serous | 113 (57.4) | 29 (33.0) | |
| Other histotypes | 3 (1.5) | 13 (14.8) | |
| N.A. | 81 (41.1) | 46 (52.2) | |
| Residual tumor—n (%): | 0.009 | ||
| RT = 0 | 55 (27.9) | 55 (62.5) | |
| RT > 0 | 19 (9.7) | 5 (5.7) | |
| N.A. | 123 (62.4) | 28 (31.8) | |
| Adjuvant treatment—n (%): | 0.002 | ||
| CT | 148 (75.1) | 48 (54.5) | |
| CT + RTx | 38 (19.3) | 1 (1.2) | |
| N.A. | 11 (5.6) a | 39 (44.3) b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantovani, G.; Coada, C.A.; Di Costanzo, S.; Mezzapesa, F.; Genovesi, L.; Bogani, G.; Raspagliesi, F.; Morganti, A.G.; De Iaco, P.; Perrone, A.M. Primary or Interval Debulking Surgery for Advanced Endometrial Cancer with Carcinosis: A Systematic Review and Individual Patient Data Meta-Analysis of Survival Outcomes. Cancers 2025, 17, 1026. https://doi.org/10.3390/cancers17061026
Mantovani G, Coada CA, Di Costanzo S, Mezzapesa F, Genovesi L, Bogani G, Raspagliesi F, Morganti AG, De Iaco P, Perrone AM. Primary or Interval Debulking Surgery for Advanced Endometrial Cancer with Carcinosis: A Systematic Review and Individual Patient Data Meta-Analysis of Survival Outcomes. Cancers. 2025; 17(6):1026. https://doi.org/10.3390/cancers17061026
Chicago/Turabian StyleMantovani, Giulia, Camelia Alexandra Coada, Stella Di Costanzo, Francesco Mezzapesa, Lucia Genovesi, Giorgio Bogani, Francesco Raspagliesi, Alessio Giuseppe Morganti, Pierandrea De Iaco, and Anna Myriam Perrone. 2025. "Primary or Interval Debulking Surgery for Advanced Endometrial Cancer with Carcinosis: A Systematic Review and Individual Patient Data Meta-Analysis of Survival Outcomes" Cancers 17, no. 6: 1026. https://doi.org/10.3390/cancers17061026
APA StyleMantovani, G., Coada, C. A., Di Costanzo, S., Mezzapesa, F., Genovesi, L., Bogani, G., Raspagliesi, F., Morganti, A. G., De Iaco, P., & Perrone, A. M. (2025). Primary or Interval Debulking Surgery for Advanced Endometrial Cancer with Carcinosis: A Systematic Review and Individual Patient Data Meta-Analysis of Survival Outcomes. Cancers, 17(6), 1026. https://doi.org/10.3390/cancers17061026