
Circulating Tumor DNA Detects Minimal Residual Disease in Patients with Locally Advanced Rectal Cancer After Total Neoadjuvant Therapy

 , , ,
, , ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Response Assessments
2.3. Local Regrowth
2.4. ctDNA Testing
2.5. Statistical Analysis
3. Results
3.1. Patient Groups by ctDNA Positivity
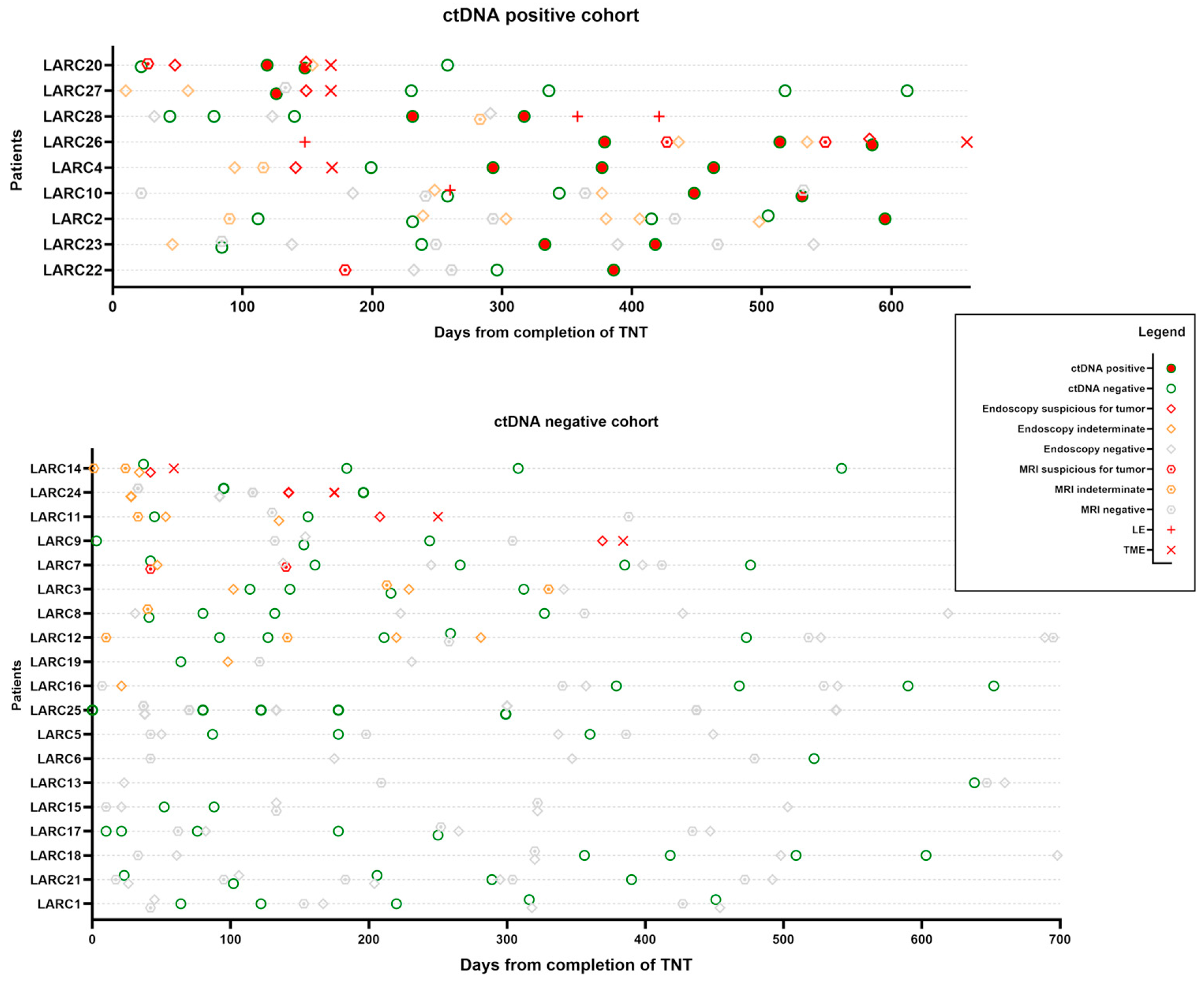
3.2. ctDNA Can Potentially Detect MRD in the Rectum in Patients Under Watch-and-Wait Protocol After TNT
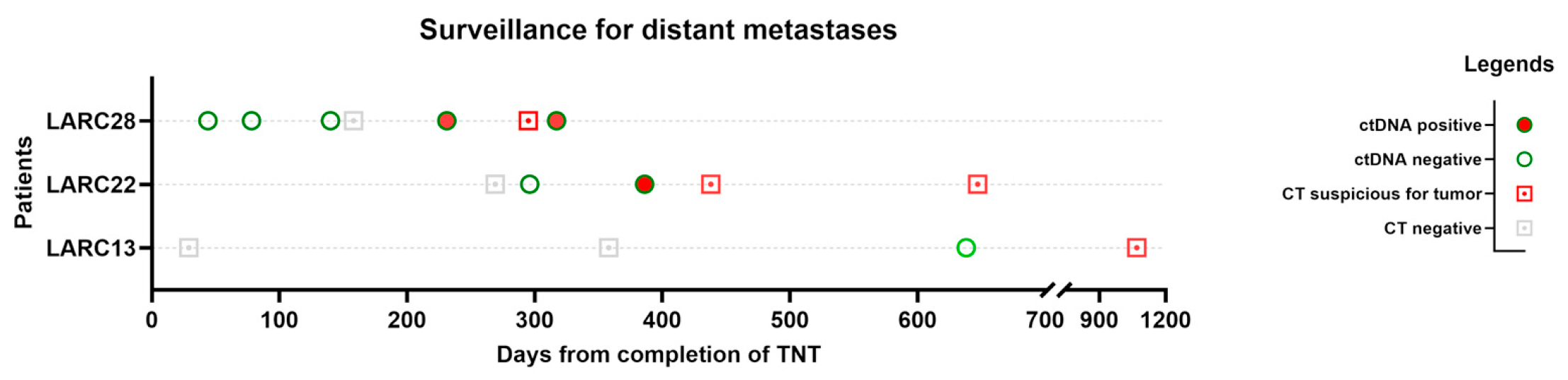
3.3. Potential Role of ctDNA in Detecting Distant Metastases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TNT | Total neoadjuvant therapy; |
| LARC | Locally advanced rectal cancer; |
| NOM | Non-operative management; |
| TME | Total mesorectal excision; |
| ctDNA | Circulating tumor DNA; |
| MRD | Minimally residual disease; |
| MMR | Mismatch repair; |
| LE | Local excision; |
| pCR | Pathologic complete response; |
| IRB | Institutional review board; |
| cCR | Complete clinical response; |
| nCR | Near complete response; |
| iCR | Incomplete response. |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J. Clin. 2025, 75, 10–45. [Google Scholar] [CrossRef]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109, djw322. [Google Scholar] [CrossRef]
- Liu, J.; Ladbury, C.; Glaser, S.; Fakih, M.; Kaiser, A.M.; Chen, Y.-J.; Williams, T.M.; Amini, A. Patterns of Care for Patients with Locally Advanced Rectal Cancer Treated with Total Neoadjuvant Therapy at Predominately Academic Centers between 2016–2020: An NCDB Analysis. Clin. Colorectal Cancer 2023, 22, 167–174. [Google Scholar] [CrossRef]
- Loria, A.; Tejani, M.A.; Temple, L.K.; Justiniano, C.F.; Melucci, A.D.; Becerra, A.Z.; Monson, J.R.T.; Aquina, C.T.; Fleming, F.J. Practice Patterns for Organ Preservation in US Patients with Rectal Cancer, 2006-2020. JAMA Oncol. 2024, 10, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Aguilar, J.; Patil, S.; Gollub, M.J.; Kim, J.K.; Yuval, J.B.; Thompson, H.M.; Verheij, F.S.; Omer, D.M.; Lee, M.; Dunne, R.F.; et al. Organ preservation in patients with rectal adenocarcinoma treated with total neoadjuvant therapy. J. Clin. Oncol. 2022, 40, 2546–2556. [Google Scholar] [CrossRef] [PubMed]
- van Kooten, R.T.; Elske van den Akker-Marle, M.; Putter, H.; Meershoek-Klein Kranenbarg, E.; van de Velde, C.J.H.; Wouters, M.W.J.M.; Tollenaar, R.A.E.M.; Peeters, K.C.M.J. The Impact of Postoperative Complications on Short- and Long-Term Health-Related Quality of Life After Total Mesorectal Excision for Rectal Cancer. Clin. Colorectal Cancer 2022, 21, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Yuval, J.B.; Patil, S.; Gangai, N.; Omer, D.M.; Akselrod, D.G.; Fung, A.; Harmath, C.B.; Kampalath, R.; Krehbiel, K.; Lee, S.; et al. MRI assessment of rectal cancer response to neoadjuvant therapy: A multireader study. Eur. Radiol. 2023, 33, 5761–5768. [Google Scholar] [CrossRef]
- Kawai, K.; Ishihara, S.; Nozawa, H.; Hata, K.; Kiyomatsu, T.; Morikawa, T.; Fukayama, M.; Watanabe, T. Prediction of pathological complete response using endoscopic findings and outcomes of patients who underwent watchful waiting after chemoradiotherapy for rectal cancer. Dis. Colon Rectum 2017, 60, 368–375. [Google Scholar] [CrossRef]
- Maas, M.; Lambregts, D.M.J.; Nelemans, P.J.; Heijnen, L.A.; Martens, M.H.; Leijtens, J.W.A.; Sosef, M.; Hulsewé, K.W.E.; Hoff, C.; Breukink, S.O.; et al. Assessment of Clinical Complete Response After Chemoradiation for Rectal Cancer with Digital Rectal Examination, Endoscopy, and MRI: Selection for Organ-Saving Treatment. Ann. Surg. Oncol. 2015, 22, 3873–3880. [Google Scholar] [CrossRef]
- Fernandez, L.M.; São Julião, G.P.; Renehan, A.G.; Beets, G.L.; Papoila, A.L.; Vailati, B.B.; Bahadoer, R.R.; Kranenbarg, E.M.-K.; Roodvoets, A.G.H.; Figueiredo, N.L.; et al. International Watch & Wait Database (IWWD) Consortium The risk of distant metastases in patients with clinical complete response managed by watch and wait after neoadjuvant therapy for rectal cancer: The influence of local regrowth in the international watch and wait database. Dis. Colon Rectum 2023, 66, 41–49. [Google Scholar] [CrossRef]
- Fernandez, L.M.; Figueiredo, N.L.; Habr-Gama, A.; São Julião, G.P.; Vieira, P.; Vailati, B.B.; Nasir, I.; Parés, O.; Santiago, I.; Castillo-Martin, M.; et al. Salvage surgery with organ preservation for patients with local regrowth after watch and wait: Is it still possible? Dis. Colon Rectum 2020, 63, 1053–1062. [Google Scholar] [CrossRef]
- Smith, J.J.; Strombom, P.; Chow, O.S.; Roxburgh, C.S.; Lynn, P.; Eaton, A.; Widmar, M.; Ganesh, K.; Yaeger, R.; Cercek, A.; et al. Assessment of a Watch-and-Wait Strategy for Rectal Cancer in Patients With a Complete Response After Neoadjuvant Therapy. JAMA Oncol. 2019, 5, e185896. [Google Scholar] [CrossRef]
- Yahya, J.; Baber, M.; Nabavizadeh, N.; Goodyear, S.M.; Kardosh, A. A Review of Circulating Tumor DNA as a Biomarker Guide for Total Neoadjuvant Therapy in Patients with Locally Advanced Rectal Cancer. J. Gastrointest. Cancer 2023, 54, 1140–1150. [Google Scholar] [CrossRef]
- Faulkner, L.G.; Howells, L.M.; Pepper, C.; Shaw, J.A.; Thomas, A.L. The utility of ctDNA in detecting minimal residual disease following curative surgery in colorectal cancer: A systematic review and meta-analysis. Br. J. Cancer 2023, 128, 297–309. [Google Scholar] [CrossRef]
- Dasari, A.; Morris, V.K.; Allegra, C.J.; Atreya, C.; Benson, A.B.; Boland, P.; Chung, K.; Copur, M.S.; Corcoran, R.B.; Deming, D.A.; et al. ctDNA applications and integration in colorectal cancer: An NCI Colon and Rectal-Anal Task Forces whitepaper. Nat. Rev. Clin. Oncol. 2020, 17, 757–770. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, N.J.; Temperley, H.C.; Kyle, E.T.; Sweeney, K.J.; O’Neill, M.; Gilham, C.; O’Sullivan, J.; O’Kane, G.; Mehigan, B.; O’Toole, S.; et al. Assessing circulating tumour DNA (ctDNA) as a prognostic biomarker in locally advanced rectal cancer: A systematic review and meta-analysis. Int. J. Colorectal Dis. 2024, 39, 82. [Google Scholar] [CrossRef] [PubMed]
- Parikh, A.R.; Van Seventer, E.E.; Siravegna, G.; Hartwig, A.V.; Jaimovich, A.; He, Y.; Kanter, K.; Fish, M.G.; Fosbenner, K.D.; Miao, B.; et al. Minimal Residual Disease Detection using a Plasma-only Circulating Tumor DNA Assay in Patients with Colorectal Cancer. Clin. Cancer Res. 2021, 27, 5586–5594. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Watanabe, J.; Akazawa, N.; Hirata, K.; Kataoka, K.; Yokota, M.; Kato, K.; Kotaka, M.; Kagawa, Y.; Yeh, K.-H.; et al. ctDNA-based molecular residual disease and survival in resectable colorectal cancer. Nat. Med. 2024, 30, 3272–3283. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Adam, M.; Chang, G.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.A.; Cooper, H.S.; Deming, D.; Garrido-Laguna, I.; et al. NCCN guidelines® insights: Rectal cancer, version 3.2024. J. Natl. Compr. Canc. Netw. 2024, 22, 366–375. [Google Scholar] [CrossRef]
- Lord, A.C.; Corr, A.; Chandramohan, A.; Hodges, N.; Pring, E.; Airo-Farulla, C.; Moran, B.; Jenkins, J.T.; Di Fabio, F.; Brown, G. Assessment of the 2020 NICE criteria for preoperative radiotherapy in patients with rectal cancer treated by surgery alone in comparison with proven MRI prognostic factors: A retrospective cohort study. Lancet Oncol. 2022, 23, 793–801. [Google Scholar] [CrossRef]
- Patel, U.B.; Blomqvist, L.K.; Taylor, F.; George, C.; Guthrie, A.; Bees, N.; Brown, G. MRI after treatment of locally advanced rectal cancer: How to report tumor response--the MERCURY experience. AJR Am. J. Roentgenol. 2012, 199, W486–W495. [Google Scholar] [CrossRef]
- Thompson, H.M.; Omer, D.M.; Lin, S.; Kim, J.K.; Yuval, J.B.; Verheij, F.S.; Qin, L.-X.; Gollub, M.J.; Wu, A.J.-C.; Lee, M.; et al. OPRA Consortium Organ preservation and survival by clinical response grade in patients with rectal cancer treated with total neoadjuvant therapy: A secondary analysis of the OPRA randomized clinical trial. JAMA Netw. Open 2024, 7, e2350903. [Google Scholar] [CrossRef]
- Smith, J.J.; Chow, O.S.; Gollub, M.J.; Nash, G.M.; Temple, L.K.; Weiser, M.R.; Guillem, J.G.; Paty, P.B.; Avila, K.; Garcia-Aguilar, J. Rectal Cancer Consortium Organ Preservation in Rectal Adenocarcinoma: A phase II randomized controlled trial evaluating 3-year disease-free survival in patients with locally advanced rectal cancer treated with chemoradiation plus induction or consolidation chemotherapy, and total mesorectal excision or nonoperative management. BMC Cancer 2015, 15, 767. [Google Scholar] [CrossRef]
- Andersen, L.; Kisistók, J.; Henriksen, T.V.; Bramsen, J.B.; Reinert, T.; Øgaard, N.; Mattesen, T.B.; Birkbak, N.J.; Andersen, C.L. Exploring the biology of ctDNA release in colorectal cancer. Eur. J. Cancer 2024, 207, 114186. [Google Scholar] [CrossRef]
- Cercek, A.; Lumish, M.; Sinopoli, J.; Weiss, J.; Shia, J.; Lamendola-Essel, M.; El Dika, I.H.; Segal, N.; Shcherba, M.; Sugarman, R.; et al. PD-1 Blockade in Mismatch Repair-Deficient, Locally Advanced Rectal Cancer. N. Engl. J. Med. 2022, 386, 2363–2376. [Google Scholar] [CrossRef] [PubMed]
- Reinert, T.; Henriksen, T.V.; Christensen, E.; Sharma, S.; Salari, R.; Sethi, H.; Knudsen, M.; Nordentoft, I.; Wu, H.-T.; Tin, A.S.; et al. Analysis of Plasma Cell-Free DNA by Ultradeep Sequencing in Patients with Stages I to III Colorectal Cancer. JAMA Oncol. 2019, 5, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Clasen, K.; Gani, C.; Schuetz, L.; Clasen, S.; Ballin, N.; Bonzheim, I.; Orth, M.; Ossowski, S.; Riess, O.; Niyazi, M.; et al. Dynamics of cell-free tumor DNA correlate with early MRI response during chemoradiotherapy in rectal cancer. Radiat. Oncol. 2024, 19, 153. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yang, L.; Bao, H.; Fan, X.; Xia, F.; Wan, J.; Shen, L.; Guan, Y.; Bao, H.; Wu, X.; et al. Utility of ctDNA in predicting response to neoadjuvant chemoradiotherapy and prognosis assessment in locally advanced rectal cancer: A prospective cohort study. PLoS Med. 2021, 18, e1003741. [Google Scholar] [CrossRef]
- Mögele, T.; Höck, M.; Sommer, F.; Friedrich, L.; Sommer, S.; Schmutz, M.; Altenburger, A.; Messmann, H.; Anthuber, M.; Kröncke, T.; et al. Circulating tumor DNA for prediction of complete pathological response to neoadjuvant radiochemotherapy in locally advanced rectal cancer (NEORECT trial). Cancers 2024, 16, 4173. [Google Scholar] [CrossRef]
- Alden, S.L.; Lee, V.; Narang, A.K.; Meyer, J.; Gearhart, S.L.; Christenson, E.S. Circulating tumor DNA to predict radiographic and pathologic response to total neoadjuvant therapy in locally advanced rectal cancer. Oncologist 2024, 29, e414–e418. [Google Scholar] [CrossRef] [PubMed]
- Murahashi, S.; Akiyoshi, T.; Sano, T.; Fukunaga, Y.; Noda, T.; Ueno, M.; Zembutsu, H. Serial circulating tumour DNA analysis for locally advanced rectal cancer treated with preoperative therapy: Prediction of pathological response and postoperative recurrence. Br. J. Cancer 2020, 123, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Kalashnikova, E.; Aushev, V.N.; Malashevich, A.K.; Tin, A.; Krinshpun, S.; Salari, R.; Scalise, C.B.; Ram, R.; Malhotra, M.; Ravi, H.; et al. Correlation between variant allele frequency and mean tumor molecules with tumor burden in patients with solid tumors. Mol. Oncol. 2024, 18, 2649–2657. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Wang, Y.; Loree, J.M.; Cohen, J.D.; Espinosa, D.; Wong, R.; Price, T.J.; Tebbutt, N.C.; Lee, M.; Burge, M.E.; et al. ctDNA-guided adjuvant chemotherapy escalation in stage III colon cancer: Primary analysis of the ctDNA-positive cohort from the randomized AGITG dynamic-III trial (intergroup study of AGITG and CCTG). J. Clin. Oncol. 2025, 43, 3503. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Shi, Q.; Dasari, A.; Garcia-Aguilar, J.; Sanoff, H.; George, T.J.; Hong, T.; Yothers, G.; Philip, P.; Nelson, G.; et al. Alliance A022104/NRG-GI010: The Janus Rectal Cancer Trial: A randomized phase II/III trial testing the efficacy of triplet versus doublet chemotherapy regarding clinical complete response and disease-free survival in patients with locally advanced rectal cancer. BMC Cancer 2024, 24, 901. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| ctDNA-Positive | ctDNA-Negative | p-Value | |
|---|---|---|---|
| Number of patients | 9 | 19 | |
| Age (years) (mean, std dev) | 60 (11) | 66 (12) | 0.25 |
| Sex (N, %) | >0.9 | ||
| Male | 5 (56%) | 12 (63%) | |
| Female | 4 (44%) | 7 (37%) | |
| cT (N, %) | 0.21 | ||
| 2 | 1 (11%) | 1 (5%) | |
| 3 | 6 (67%) | 17 (90%) | |
| 4 | 2 (22%) | 1 (5%) | |
| cN (N, %) | 0.65 | ||
| 0 | 2 (22%) | 6 (32%) | |
| 1 | 6 (67%) | 9 (47%) | |
| 2 | 1 (11%) | 4 (21%) | |
| MMR status (N, %) | >0.9 | ||
| MMR-proficient | 8 (89%) | 16 (84%) | |
| MMR-deficient | 0 (0%) | 1 (5%) | |
| Unknown | 1 (11%) | 2 (11%) | |
| Tumor distance (cm) (mean, std) | 5.7 (3.8) | 5.9 (4.2) | 0.84 |
| Total neoadjuvant therapy (N, %) | 9 (100%) | 19 (100%) | >0.9 |
| Local Regrowth (N, %) | 6 (66%) | 4 (21%) | 0.035 |
| Definitive treatment of primary tumor (N, %) | 0.041 | ||
| LE | 2 (22%) | 0 (0%) | |
| TME | 4 (44%) | 4 (21%) | |
| NOM | 3 (33%) | 14 (74%) | |
| Median follow-up (years) | 1.81 | 1.47 | 0.72 |
| Distant recurrence (N, %) | 2 (22%) | 1 (5%) | 0.23 |
| Local recurrence (N, %) | 0 (0%) | 0 (0%) | |
| Resection Pathology (N) | 6 | 4 | |
| pCR | 0 (0%) | 1 (25%) | |
| Residual tumor | 6 (100%) | 3 (75%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.K.; Alden, A.J.; Knaus, S.; Thakkar, R.; Moudgill, L.; Chudzinski, A.; Cavallaro, P.; Martinez, C.; Bennett, R.D.; Marcet, J. Circulating Tumor DNA Detects Minimal Residual Disease in Patients with Locally Advanced Rectal Cancer After Total Neoadjuvant Therapy. Cancers 2025, 17, 2560. https://doi.org/10.3390/cancers17152560
Kim JK, Alden AJ, Knaus S, Thakkar R, Moudgill L, Chudzinski A, Cavallaro P, Martinez C, Bennett RD, Marcet J. Circulating Tumor DNA Detects Minimal Residual Disease in Patients with Locally Advanced Rectal Cancer After Total Neoadjuvant Therapy. Cancers. 2025; 17(15):2560. https://doi.org/10.3390/cancers17152560
Chicago/Turabian StyleKim, Jin K., Ashley J. Alden, Sarah Knaus, Rishabh Thakkar, Lisa Moudgill, Allen Chudzinski, Paul Cavallaro, Carolina Martinez, Robert D. Bennett, and Jorge Marcet. 2025. "Circulating Tumor DNA Detects Minimal Residual Disease in Patients with Locally Advanced Rectal Cancer After Total Neoadjuvant Therapy" Cancers 17, no. 15: 2560. https://doi.org/10.3390/cancers17152560
APA StyleKim, J. K., Alden, A. J., Knaus, S., Thakkar, R., Moudgill, L., Chudzinski, A., Cavallaro, P., Martinez, C., Bennett, R. D., & Marcet, J. (2025). Circulating Tumor DNA Detects Minimal Residual Disease in Patients with Locally Advanced Rectal Cancer After Total Neoadjuvant Therapy. Cancers, 17(15), 2560. https://doi.org/10.3390/cancers17152560