
Immune Modulation During Treatment with Enzalutamide Alone or with Radium-223 in Patients with Castration Resistant Prostate Cancer

 ,
,  ,
,
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Immunophenotyping by Mass Cytometry Time-of-Flight (CyTOF)
2.2. Immunohistochemistry (IHC)
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Piulats, J.M.; Gross-Goupil, M.; Goh, J.; Ojamaa, K.; Hoimes, C.J.; Vaishampayan, U.; Berger, R.; Sezer, A.; Alanko, T.; et al. Pembrolizumab for Treatment-Refractory Metastatic Castration-Resistant Prostate Cancer: Multicohort, Open-Label Phase II KEYNOTE-199 Study. J. Clin. Oncol. 2019, 38, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Slovin, S.F.; Higano, C.S.; Hamid, O.; Tejwani, S.; Harzstark, A.; Alumkal, J.J.; Scher, H.I.; Chin, K.; Gagnier, P.; McHenry, M.B.; et al. Ipilimumab alone or in combination with radiotherapy in metastatic castration-resistant prostate cancer: Results from an open-label, multicenter phase I/II study. Ann. Oncol. 2013, 24, 1813–1821. [Google Scholar] [CrossRef]
- Graff, J.N.; Beer, T.M.; Alumkal, J.J.; Slottke, R.E.; Redmond, W.L.; Thomas, G.V.; Thompson, R.F.; Wood, M.A.; Koguchi, Y.; Chen, Y.; et al. A phase II single-arm study of pembrolizumab with enzalutamide in men with metastatic castration-resistant prostate cancer progressing on enzalutamide alone. J. Immunother. Cancer 2020, 8, e000642. [Google Scholar] [CrossRef]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fosså, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef]
- Confino, H.; Hochman, I.; Efrati, M.; Schmidt, M.; Umansky, V.; Kelson, I.; Keisari, Y. Tumor ablation by intratumoral Ra-224-loaded wires induces anti-tumor immunity against experimental metastatic tumors. Cancer Immunol. Immunother. 2015, 64, 191–199. [Google Scholar] [CrossRef]
- Barsegian, V.; Müller, S.P.; Möckel, D.; Horn, P.A.; Bockisch, A.; Lindemann, M. Lymphocyte function following radium-223 therapy in patients with metastasized, castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 242–246. [Google Scholar] [CrossRef]
- Vardaki, I.; Corn, P.; Gentile, E.; Song, J.H.; Madan, N.; Hoang, A.; Parikh, N.; Guerra, L.; Lee, Y.C.; Lin, S.C.; et al. Radium-223 Treatment Increases Immune Checkpoint Expression in Extracellular Vesicles from the Metastatic Prostate Cancer Bone Microenvironment. Clin. Cancer Res. 2021, 27, 3253–3264. [Google Scholar] [CrossRef]
- Kim, J.W.; Shin, M.S.; Kang, Y.; Kang, I.; Petrylak, D.P. Immune Analysis of Radium-223 in Patients With Metastatic Prostate Cancer. Clin. Genitourin. Cancer 2018, 16, e469–e476. [Google Scholar] [CrossRef]
- Mercader, M.; Bodner, B.K.; Moser, M.T.; Kwon, P.S.; Park, E.S.; Manecke, R.G.; Ellis, T.M.; Wojcik, E.M.; Yang, D.; Flanigan, R.C.; et al. T cell infiltration of the prostate induced by androgen withdrawal in patients with prostate cancer. Proc. Natl. Acad. Sci. USA 2001, 98, 14565–14570. [Google Scholar] [CrossRef]
- Morse, M.D.; McNeel, D.G. Prostate cancer patients on androgen deprivation therapy develop persistent changes in adaptive immune responses. Hum. Immunol. 2010, 71, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Page, S.T.; Plymate, S.R.; Bremner, W.J.; Matsumoto, A.M.; Hess, D.L.; Lin, D.W.; Amory, J.K.; Nelson, P.S.; Wu, J.D. Effect of medical castration on CD4+ CD25+ T cells, CD8+ T cell IFN-gamma expression, and NK cells: A physiological role for testosterone and/or its metabolites. Am. J. Physiol. Endocrinol. Metab. 2006, 290, E856–E863. [Google Scholar] [CrossRef]
- Smith, M.; Parker, C.; Saad, F.; Miller, K.; Tombal, B.; Ng, Q.S.; Boegemann, M.; Matveev, V.; Piulats, J.M.; Zucca, L.E.; et al. Addition of radium-223 to abiraterone acetate and prednisone or prednisolone in patients with castration-resistant prostate cancer and bone metastases (ERA 223): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 408–419. [Google Scholar] [CrossRef]
- Gillessen, S.; Choudhury, A.; Saad, F.; Gallardo, E.; Soares, A.; Loriot, Y.; McDermott, R.S.; Rodriguez-Vida, A.; Isaacson, P.; Nolè, F.; et al. LBA1 A randomized multicenter open label phase III trial comparing enzalutamide vs a combination of Radium-223 (Ra223) and enzalutamide in asymptomatic or mildly symptomatic patients with bone metastatic castration-resistant prostate cancer (mCRPC): First results of EORTC-GUCG 1333/PEACE-3. Ann. Oncol. 2024, 35, S1254. [Google Scholar]
- Golden, E.B.; Apetoh, L. Radiotherapy and immunogenic cell death. Semin. Radiat. Oncol. 2015, 25, 11–17. [Google Scholar] [CrossRef]
- Marshall, C.H.; Fu, W.; Wang, H.; Park, J.C.; DeWeese, T.L.; Tran, P.T.; Song, D.Y.; King, S.; Afful, M.; Hurrelbrink, J.; et al. Randomized Phase II Trial of Sipuleucel-T with or without Radium-223 in Men with Bone-metastatic Castration-resistant Prostate Cancer. Clin. Cancer Res. 2021, 27, 1623–1630. [Google Scholar] [CrossRef]
- Moreira, D.; Sampath, S.; Won, H.; White, S.V.; Su, Y.L.; Alcantara, M.; Wang, C.; Lee, P.; Maghami, E.; Massarelli, E.; et al. Myeloid cell-targeted STAT3 inhibition sensitizes head and neck cancers to radiotherapy and T cell-mediated immunity. J. Clin. Investig. 2021, 131, e137001. [Google Scholar] [CrossRef]
- Su, Y.-L.; Banerjee, S.; White, S.V.; Kortylewski, M. STAT3 in Tumor-Associated Myeloid Cells: Multitasking to Disrupt Immunity. Int. J. Mol. Sci. 2018, 19, 1803. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, X.; Qiu, C.; Yang, N. STAT3 Contributes to Radioresistance in Cancer. Front. Oncol. 2020, 10, 1120. [Google Scholar] [CrossRef]
- Chen, H.J.; Yu, M.M.; Huang, J.C.; Lan, F.Y.; Liao, H.H.; Xu, Z.H.; Yu, Y.J.; Huang, Y.C.; Chen, F. SLC4A4 is a novel driver of enzalutamide resistance in prostate cancer. Cancer Lett. 2024, 597, 217070. [Google Scholar] [CrossRef]
- Liu, Q.; Tong, D.; Liu, G.; Xu, J.; Do, K.; Geary, K.; Zhang, D.; Zhang, J.; Zhang, Y.; Li, Y.; et al. Metformin reverses prostate cancer resistance to enzalutamide by targeting TGF-β1/STAT3 axis-regulated EMT. Cell Death Dis. 2017, 8, e3007. [Google Scholar] [CrossRef] [PubMed]
- Hellsten, R.; Stiehm, A.; Palominos, M.; Persson, M.; Bjartell, A. The STAT3 inhibitor GPB730 enhances the sensitivity to enzalutamide in prostate cancer cells. Transl. Oncol. 2022, 24, 101495. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liakou, C.I.; Kamat, A.; Pettaway, C.; Ward, J.F.; Tang, D.N.; Sun, J.; Jungbluth, A.A.; Troncoso, P.; Logothetis, C.; et al. Anti-CTLA-4 therapy results in higher CD4+ICOShi T cell frequency and IFN-gamma levels in both nonmalignant and malignant prostate tissues. Proc. Natl. Acad. Sci. USA 2009, 106, 2729–2734. [Google Scholar] [CrossRef]
- Fan, X.; Quezada, S.A.; Sepulveda, M.A.; Sharma, P.; Allison, J.P. Engagement of the ICOS pathway markedly enhances efficacy of CTLA-4 blockade in cancer immunotherapy. J. Exp Med. 2014, 211, 715–725. [Google Scholar] [CrossRef]
- Zhao, S.G.; Lehrer, J.; Chang, S.L.; Das, R.; Erho, N.; Liu, Y.; Sjöström, M.; Den, R.B.; Freedland, S.J.; Klein, E.A.; et al. The Immune Landscape of Prostate Cancer and Nomination of PD-L2 as a Potential Therapeutic Target. J. Natl. Cancer Inst. 2019, 111, 301–310. [Google Scholar] [CrossRef]
- Armstrong, A.J.; Gupta, S.; Healy, P.; Kemeny, G.; Leith, B.; Zalutsky, M.R.; Spritzer, C.; Davies, C.; Rothwell, C.; Ware, K.; et al. Pharmacodynamic study of radium-223 in men with bone metastatic castration resistant prostate cancer. PLoS ONE 2019, 14, e0216934. [Google Scholar] [CrossRef]
- Ylitalo, E.B.; Thysell, E.; Jernberg, E.; Lundholm, M.; Crnalic, S.; Egevad, L.; Stattin, P.; Widmark, A.; Bergh, A.; Wikström, P. Subgroups of Castration-resistant Prostate Cancer Bone Metastases Defined Through an Inverse Relationship Between Androgen Receptor Activity and Immune Response. Eur. Urol. 2017, 71, 776–787. [Google Scholar] [CrossRef]
- Gillessen, S.; Tombal, B.; Turco, F.; Choudhury, A.; Rodriguez-Vida, A.; Gallardo, E.; Velho, P.I.; Nolè, F.; Cruz, F.; Loriot, Y.; et al. Decrease in Fracture Rate with Mandatory Bone-protecting Agents in the EORTC 1333/PEACE-3 Trial Comparing Radium-223 Combined with Enzalutamide Versus Enzalutamide Alone: A Safety Analysis. Eur. Urol. 2025, 87, 285–288. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Patients | Arm A Enzalutamide + Rad233 | Arm B Enzalutamide | |
|---|---|---|---|
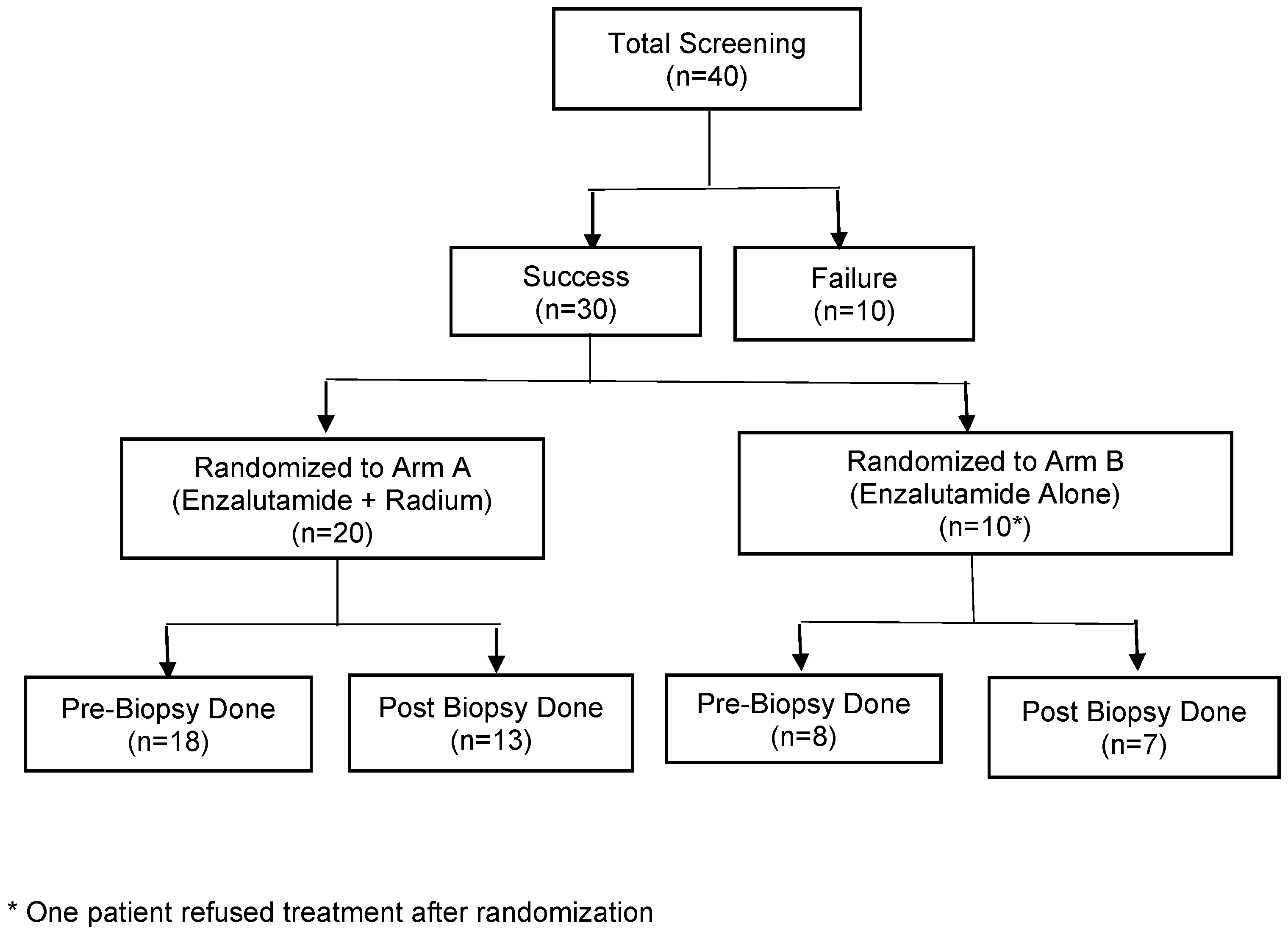
| Total Patient Randomized and Treated | 29 * | 20 | 9 * |
| Age | |||
| Median (Range) | 68 (53–87) | 67 (57–87) | 68 (53–78) |
| Race/Ethnicity | |||
| White | 19 (66%) | 13 (65%) | 6 (67%) |
| Hispanic | 6 (21%) | 3 (15%) | 3 (33%) |
| Black or African American | 2 (7%) | 2 (10%) | 0 |
| Asian | 2 (7%) | 2 (10%) | 0 |
| ECOG Performance Status | |||
| 0 | 27 (93%) | 18 (90%) | 9 (100%) |
| 1 | 2 (7%) | 2 (10%) | 0 |
| Gleason Score | |||
| 7 | 6 (24%) | 4 (25%) | 2 (22%) |
| >7 | 19 (76%) | 12 (75%) | 7 (78%) |
| Median (Range) | 8 (7–10) | 8.5 (7–10) | 8 (7–9) |
| Unknown | 4 | 4 | |
| Visceral Mets Involved at Study Entry | |||
| No | 16 (62%) | 12 (67%) | 4 (50%) |
| Yes | 10 (38%) | 6 (33%) | 4 (50%) |
| Unknown | 3 | 2 | 1 |
| Received Prior Chemotherapy | |||
| No | 15 (52%) | 9 (45%) | 6 (67%) |
| Yes | 14 (48%) | 11 (55%) | 3 (33%) |
| Baseline Testosterone Level | |||
| Median (Range) | 10.9 (2.5–65.5) | 11.0 (2.5–65.5) | 10.0 (7.0–22.0) |
| Missing | 5 | 3 | 2 |
| Baseline PSA Level | |||
| Median (Range) | 13.3 (0.5–1760) | 12.3 (0.5–1760) | 30.5 (2.7–142.1) |
| Disease Involvement | |||
| Bone | 29 (100%) | 20 (100%) | 9 (100%) |
| Non-regional Lymph Nodes | 5 (17%) | 3 (15%) | 2 (22%) |
| Pelvis | 3 (10%) | 2 (10%) | 1 (11%) |
| Visceral | 4 (13%) | 2 (10%) | 2 (22%) |
| Number Patients | ||||
|---|---|---|---|---|
| Total Patients (n = 29) | Arm A Enzalutamide + Rad233 (n = 20) | Arm B Enzalutamide (n = 9) | p-Value | |
| Number of Cycles Given | ||||
| 1 or 2 Cycles | 1 (3%) | 1 (5%) | 0 | |
| ≥3 Cycles | 28 (97%) | 19 (95%) | 9 (100%) | |
| Median (Range) | 6 (1–6) | 6 (1–6) | 6 (4–6) | |
| PSA Maximum Changed from Baseline | 0.30 ^ | |||
| Median (Range) | −57% (−100–62%) | −53% (−100–62%) | −61% (−99–−15%) | |
| PSA Changed from Baseline at 12 Weeks since Treatment Start | 0.30 ^ | |||
| Median (Range) | −39% (−100–140%) | −28% (−100–140%) | −61% (−97–79%) | |
| Not available | 2 | |||
| PSA30 Response | 0.11 * | |||
| No | 10 (34%) | 9 (45%) | 1 (11%) | |
| Yes | 19 (66%) | 11 (55%) | 8 (89%) | |
| Best Clinical Overall Response | 0.56 * | |||
| PR | 2 (7%) | 1 (5%) | 1 (11%) | |
| SD | 19 (62%) | 14 (70%) | 5 (56%) | |
| PD | 8 (28%) | 5 (25%) | 3 (33%) | |
| Off Treatment Reason | ||||
| Complete Treatment | 21 (72%) | 16 (80%) | 5 (56%) | |
| Disease Progression | 7 (24%) | 4 (20%) | 3 (33%) | |
| Unacceptable Toxicity | 1 (3%) # | 0 | 1 (11%) | |
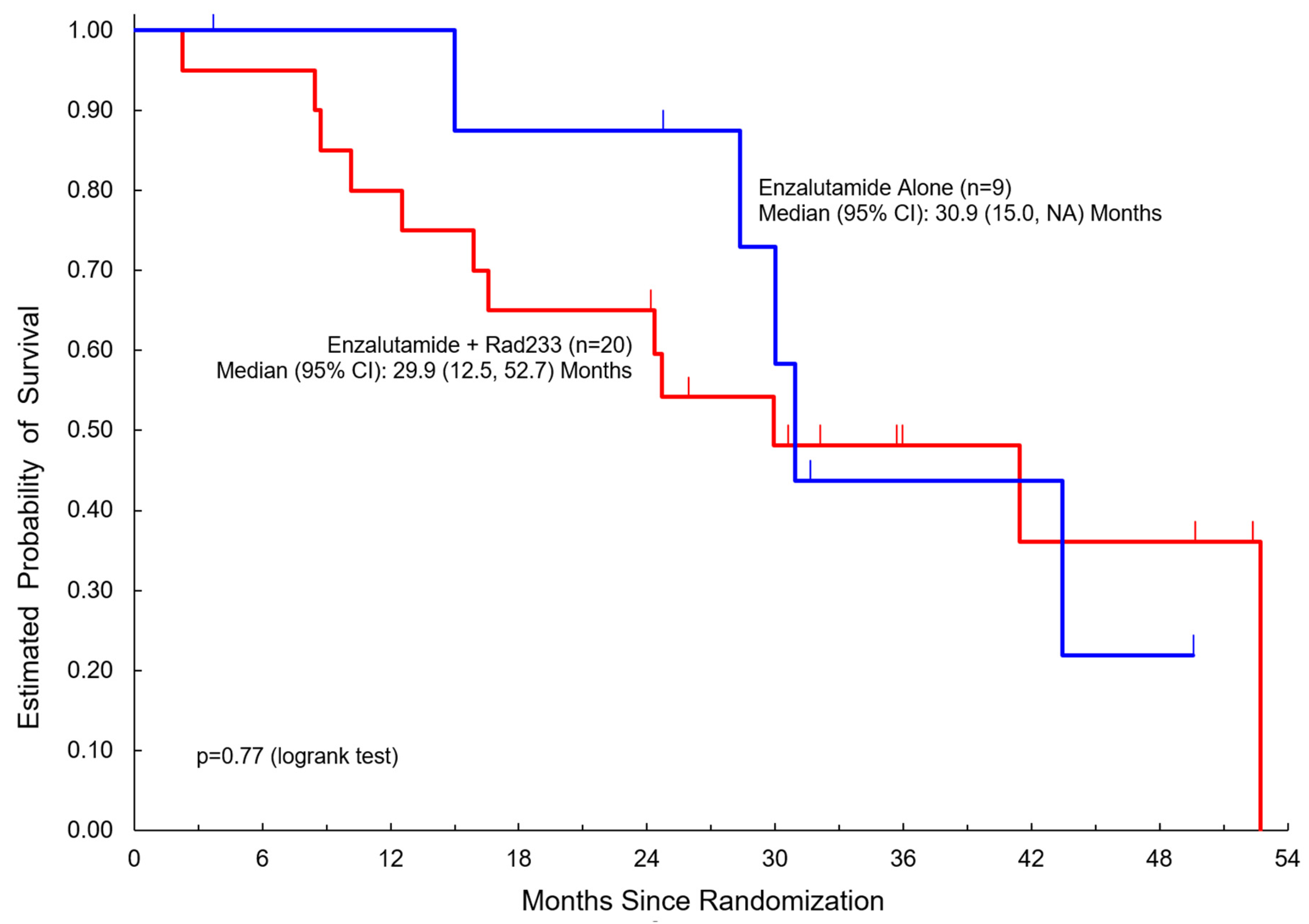
| Overall Survival | ||||
| Median (95% CI) | 30.9 (24.3, 52.7) Mo. | 29.9 (12.5, 52.7) Mo. | 30.9 (15.0, NA) Mo. | 0.77 ~ |
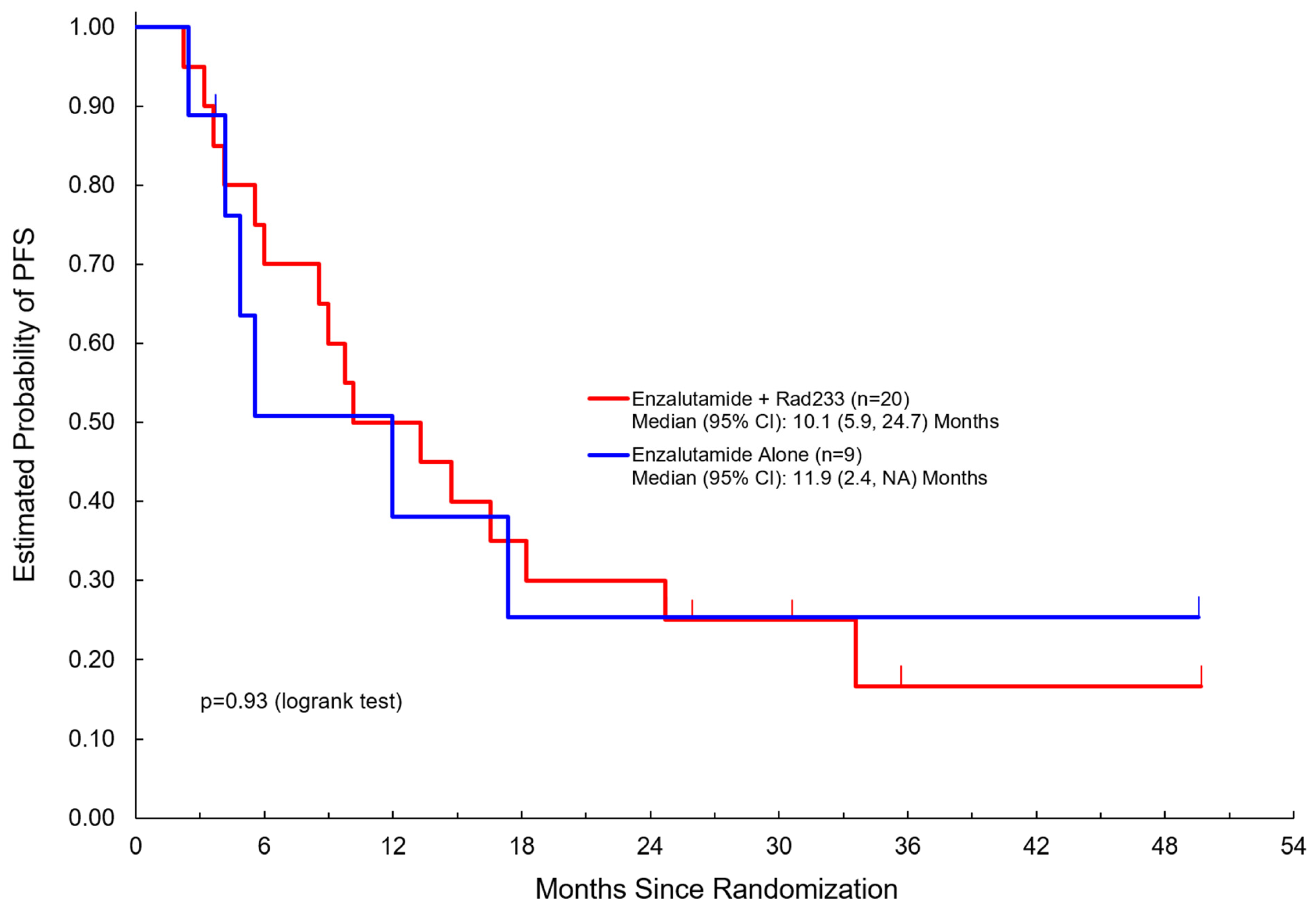
| Progression Free Survival | ||||
| Median (95% CI) | 11.9 (5.5, 17.4) Mo. | 10.1 (5.9, 24.7) Mo. | 11.9 (2.4, NA) Mo. | 0.93 ~ |
| Duration of Follow-Up | ||||
| Median (Range) | 36.0 (3.7–52.4) Mo. | 36.0 (24.2–52.4) Mo. | 49.6 (3.7–49.6) Mo. | |
| Arm A: Radium223 + Enzalutamide (n = 20) | Arm B: Enzalutamide (n = 9) | |||||
|---|---|---|---|---|---|---|
| Treatment-Related Adverse Event (TRAE) | Any Grade TRAE (%) | Grade 1 | Grade 2 | Any Grade TRAE (%) | Grade 1 | Grade 2 |
| Leukopenia | 6 (30%) | 4 (20%) | 2 (10%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Hyponatremia | 6 (30%) | 6 (30%) | 0 (0%) | 1 (11%) | 1 (11%) | 0 (0%) |
| Neutropenia | 5 (25%) | 2 (10%) | 3 (15%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Fatigue | 5 (25%) | 4 (20%) | 1 (5%) | 4 (44%) | 4 (44%) | 0 (0%) |
| Anemia | 3 (15%) | 3 (15%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Hot Flashes | 3 (15%) | 3 (15%) | 0 (0%) | 1 (11%) | 1 (11%) | 0 (0%) |
| Nausea | 3 (15%) | 3 (15%) | 0 (0%) | 1 (11%) | 0 (0%) | 1 (11%) |
| Dizziness | 3 (15%) | 3 (15%) | 0 (0%) | 3 (33%) | 2 (22%) | 1 (11%) |
| Thrombocytopenia | 2 (10%) | 2 (10%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Diarrhea | 2 (10%) | 2 (10%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Myalgias | 2 (10%) | 2 (10%) | 0 (0%) | 1 (11%) | 1 (11%) | 0 (0%) |
| Constipation | 1 (5%) | 0 (0%) | 1 (5%) | 1 (11%) | 1 (11%) | 0 (0%) |
| Elevated Alkaline Phosphatase | 1 (5%) | 1 (5%) | 0 (0%) | 1 (11%) | 1 (11%) | 0 (0%) |
| Hyperglycemia | 1 (5%) | 1 (5%) | 0 (0%) | 2 (22%) | 2 (22%) | 0 (0%) |
| Dysgeusia | 1 (5%) | 1 (5%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Hypertension | 1 (5%) | 0 (0%) | 1 (5%) | 3 (33%) | 0 (0%) | 3 (33%) |
| Immune Analyte | Arm A Enzalutamide + Rad233 | Arm B Enzalutamide | ||
|---|---|---|---|---|
| Mean Expression (End of Treatment vs. Baseline in pg/mL) | p-Value | Mean Expression (End of Treatment vs. Baseline in pg/mL) | p-Value | |
| PDL-2 | 17,817 vs. 16474 | p = 0.0026 | 1787 vs. 1641 | p = 0.57 |
| BTLA | 2246 vs. 2063 | p = 0.57 | 1787 vs. 1641 | p = 0.8 |
| TIM-3 | 3233 vs. 3072 | p = 0.57 | 3239 vs. 3350 | p = 1 |
| HVEM | 2310 vs. 2163 | p = 0.078 | 2868 vs. 2861 | p = 1 |
| LAG-3 | 115,977 vs. 112,772 | p = 0.78 | 159,067 vs. 119,192 | p = 0.23 |
| GITRL | 1068 vs. 1046 | p = 0.42 | 759 vs. 711 | p = 0.83 |
| PD-1 | 1717 vs. 1690 | p = 0.65 | 1450 vs. 1423 | p = 1 |
| CTLA-4 | 164 vs. 155 | p = 0.87 | 119 vs. 102 | p = 0.57 |
| PDL-1 | 294 vs. 277 | p = 0.91 | 202 vs. 102 | p = 0.88 |
| ICOS | 3096 vs. 3116 | p = 0.91 | 1773 vs. 1885 | p = 0.88 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zang, P.D.; Da Silva, D.M.; Liu, Z.-X.; Kandukuri, S.; Tsao-Wei, D.; D’Souza, A.; Kast, W.M.; Pal, S.K.; Kefauver, C.; Juanqueira, M.; et al. Immune Modulation During Treatment with Enzalutamide Alone or with Radium-223 in Patients with Castration Resistant Prostate Cancer. Cancers 2025, 17, 1730. https://doi.org/10.3390/cancers17101730
Zang PD, Da Silva DM, Liu Z-X, Kandukuri S, Tsao-Wei D, D’Souza A, Kast WM, Pal SK, Kefauver C, Juanqueira M, et al. Immune Modulation During Treatment with Enzalutamide Alone or with Radium-223 in Patients with Castration Resistant Prostate Cancer. Cancers. 2025; 17(10):1730. https://doi.org/10.3390/cancers17101730
Chicago/Turabian StyleZang, Peter D., Diane M. Da Silva, Zhang-Xu Liu, Shivani Kandukuri, Denice Tsao-Wei, Anishka D’Souza, W. Martin Kast, Sumanta K. Pal, Cheryl Kefauver, Maribel Juanqueira, and et al. 2025. "Immune Modulation During Treatment with Enzalutamide Alone or with Radium-223 in Patients with Castration Resistant Prostate Cancer" Cancers 17, no. 10: 1730. https://doi.org/10.3390/cancers17101730
APA StyleZang, P. D., Da Silva, D. M., Liu, Z.-X., Kandukuri, S., Tsao-Wei, D., D’Souza, A., Kast, W. M., Pal, S. K., Kefauver, C., Juanqueira, M., Yang, L., Quinn, D. I., & Dorff, T. B. (2025). Immune Modulation During Treatment with Enzalutamide Alone or with Radium-223 in Patients with Castration Resistant Prostate Cancer. Cancers, 17(10), 1730. https://doi.org/10.3390/cancers17101730