
Presence of CD44v9-Expressing Cancer Stem Cells in Circulating Tumor Cells and Effects of Carcinoembryonic Antigen Levels on the Prognosis of Colorectal Cancer


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Sample Collection
2.2. Reverse Transcription-Polymerase Chain Reaction (RT-PCR)
2.3. Clinical Assessment
2.4. Statistical Analysis
3. Results
3.1. Association between CD44v9 Expression and Clinicopathologic Features
3.2. Association between Expression of CD44v9 mRNA in CTCs and Survival Rate
3.3. Association between CEA Values and Survival Rates
3.4. Multivariate Cox Analysis for DSS
3.5. Comparison of DSS between Cases with Negative CD44v9 mRNA Expression and CEA Level
3.6. Comparison of DSS between Cases with Negative CD44v9 mRNA Expression and Low CEA < 5 ng/mL) and Other Cases
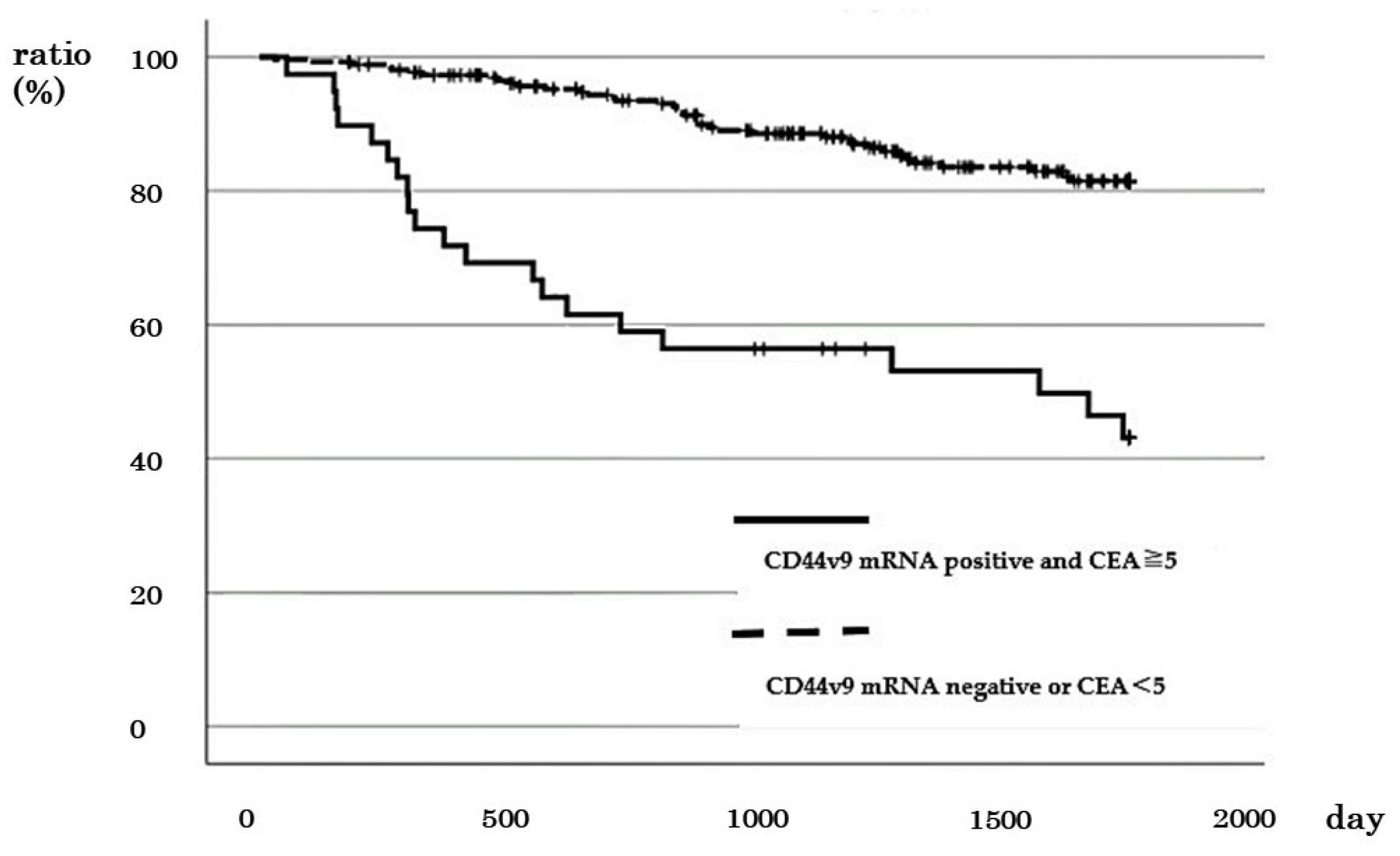
3.7. Comparison of DSS between Cases with Positive CD44v9 mRNA Expression and High CEA (≥5 ng/mL) and Other Cases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baidoun, F.; Elshiwy, K.; Elkeraie, Y.; Merjaneh, Z.; Khoudari, G.; Sarmini, M.T.; Gad, M.; Al-Husseini, M.; Saad, A. Colorectal Cancer Epidemiology: Recent Trends and Impact on Outcomes. Curr. Drug Targets 2021, 22, 998–1009. [Google Scholar] [CrossRef]
- Underwood, P.W.; Ruff, S.M.; Pawlik, T.M. Update on Targeted Therapy and Immunotherapy for Metastatic Colorectal Cancer. Cells 2024, 13, 245. [Google Scholar] [CrossRef]
- Duffy, M.J.; van Dalen, A.; Haglund, C.; Hansson, L.; Holinski-Feder, E.; Klapdor, R.; Lamerz, R.; Peltomaki, P.; Sturgeon, C.; Topolcan, O. Tumour markers in colorectal cancer: European Group on Tumour Markers (EGTM) guidelines for clinical use. Eur. J. Cancer 2007, 43, 1348–1360. [Google Scholar] [CrossRef]
- Locker, G.Y.; Hamilton, S.; Harris, J.; Jessup, J.M.; Kemeny, N.; Macdonald, J.S.; Somerfield, M.R.; Hayes, D.F.; Bast, R.C. ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J. Clin. Oncol. 2006, 24, 5313–5327. [Google Scholar] [CrossRef]
- Benson, A.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Ward, U.; Primrose, J.N.; Finan, P.J.; Perren, T.J.; Selby, P.; Purves, D.A.; Cooper, E.H. The use of tumour markers CEA, CA-195 and CA-242 in evaluating the response to chemotherapy in patients with advanced colorectal cancer. Br. J. Cancer 1993, 67, 1132–1135. [Google Scholar] [CrossRef]
- Preketes, A.P.; King, J.; Caplehorn, J.R.M.; Clingan, P.R.; Ross, W.B.; Morris, D.L. Cea reduction after cryotherapy for liver metastases from colon-cancer predicts survival. Aust. N. Z. J. Surg. 1994, 64, 612–614. [Google Scholar] [CrossRef]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef]
- Konishi, T.; Shimada, Y.; Hsu, M.; Tufts, L.; Jimenez-Rodriguez, R.; Cercek, A.; Yaeger, R.; Saltz, L.; Smith, J.J.; Nash, G.M.; et al. Association of Preoperative and Postoperative Serum Carcinoembryonic Antigen and Colon Cancer Outcome. JAMA Oncol. 2018, 4, 309–315. [Google Scholar] [CrossRef]
- Kim, G.; Jung, E.J.; Ryu, C.G.; Hwang, D.Y. Usefulness of Carcinoembryonic Antigen for Monitoring Tumor Progression during Palliative Chemotherapy in Metastatic Colorectal Cancer. Yonsei Med. J. 2013, 54, 116–122. [Google Scholar] [CrossRef]
- Kim, I.H.; Lee, J.E.; Yang, J.H.; Jeong, J.W.; Ro, S.; Lee, M.A. Clinical significance of changes in systemic inflammatory markers and carcinoembryonic antigen levels in predicting metastatic colorectal cancer prognosis and chemotherapy response. Asia Pac. J. Clin. Oncol. 2018, 14, 239–246. [Google Scholar] [CrossRef]
- Kim, I.H.; Lee, J.E.; Yang, J.H.; Jeong, J.W.; Ro, S.; Oh, S.T.; Kim, J.G.; Choi, M.H.; Lee, M.A. Clinical Significance of Discordance between Carcinoembryonic Antigen Levels and RECIST in Metastatic Colorectal Cancer. Cancer Res. Treat. 2018, 50, 283–292. [Google Scholar] [CrossRef]
- de Haas, R.J.; Wicherts, D.A.; Flores, E.; Ducreux, M.; Levi, F.; Paule, B.; Azoulay, D.; Castaing, D.; Lemoine, A.; Adam, R. Tumor Marker Evolution: Comparison with Imaging for Assessment of Response to Chemotherapy in Patients with Colorectal Liver Metastases. Ann. Surg. Oncol. 2010, 17, 1010–1023. [Google Scholar] [CrossRef]
- Masuda, T.; Hayashi, N.; Iguchi, T.; Ito, S.; Eguchi, H.; Mimori, K. Clinical and biological significance of circulating tumor cells in cancer. Mol. Oncol. 2016, 10, 408–417. [Google Scholar] [CrossRef]
- Aggarwal, C. Relationship among circulating tumor cells, CEA and overall survival in patients with metastatic colorectal cancer. Ann. Oncol. 2013, 24, 2708–2710. [Google Scholar] [CrossRef]
- Bork, U.; Rahbari, N.N.; Schölch, S.; Reissfelder, C.; Kahlert, C.; Büchler, M.W.; Weitz, J.; Koch, M. Circulating tumour cells and outcome in non-metastatic colorectal cancer: A prospective study. Br. J. Cancer 2015, 112, 1306–1313. [Google Scholar] [CrossRef]
- Cohen, S.J.; Punt, C.J.A.; Iannotti, N.; Saidman, B.H.; Sabbath, K.D.; Gabrail, N.Y.; Picus, J.; Morse, M.A.; Mitchell, E.; Miller, M.C.; et al. Prognostic significance of circulating tumor cells in patients with metastatic colorectal cancer. Ann. Oncol. 2009, 20, 1223–1229. [Google Scholar] [CrossRef]
- Cohen, S.J. Relationship of Circulating Tumor Cells to Tumor Response, Progression-Free Survival, and Overall Survival in Patients with Metastatic Colorectal Cancer. J. Clin. Oncol. 2009, 27, 1923. [Google Scholar] [CrossRef]
- Fang, C.; Fan, C.W.; Wang, C.; Huang, Q.R.; Meng, W.T.; Yu, Y.Y.; Yang, L.; Hu, J.K.; Li, Y.; Mo, X.M.; et al. Prognostic value of CD133+CD54+CD44+ circulating tumor cells in colorectal cancer with liver metastasis. Cancer Med. 2017, 6, 2850–2857. [Google Scholar] [CrossRef]
- Plaks, V.; Koopman, C.D.; Werb, Z. Circulating Tumor Cells. Science 2013, 341, 1186–1188. [Google Scholar] [CrossRef]
- Chaffer, C.L.; Weinberg, R.A. A Perspective on Cancer Cell Metastasis. Science 2011, 331, 1559–1564. [Google Scholar] [CrossRef]
- Nguyen, D.X.; Bos, P.D.; Massague, J. Metastasis: From dissemination to organ-specific colonization. Nat. Rev. Cancer 2009, 9, U265–U274. [Google Scholar] [CrossRef]
- Ishimoto, T.; Nagano, O.; Yae, T.; Tamada, M.; Motohara, T.; Oshima, H.; Oshima, M.; Ikeda, T.; Asaba, R.; Yagi, H.; et al. CD44 Variant Regulates Redox Status in Cancer Cells by Stabilizing the xCT Subunit of System xc- and Thereby Promotes Tumor Growth. Cancer Cell 2011, 19, 387–400. [Google Scholar] [CrossRef]
- Ren, F.; Sheng, W.Q.; Du, X. CD133: A cancer stem cells marker, is used in colorectal cancers. World J. Gastroenterol. 2013, 19, 2603–2611. [Google Scholar] [CrossRef]
- Suwannakul, N.; Ma, N.; Midorikawa, K.; Oikawa, S.; Kobayashi, H.; He, F.; Kawanishi, S.; Murata, M. CD44v9 Induces Stem Cell-Like Phenotypes in Human Cholangiocarcinoma. Front. Cell Dev. Biol. 2020, 8, 417. [Google Scholar] [CrossRef]
- Phi, L.T.H.; Sari, I.N.; Yang, Y.G.; Lee, S.H.; Jun, N.; Kim, K.S.; Lee, Y.K.; Kwon, H.Y. Cancer Stem Cells (CSCs) in Drug Resistance and their Therapeutic Implications in Cancer Treatment. Stem Cells Int. 2018, 2018, 5416923. [Google Scholar] [CrossRef]
- Dalerba, P.; Dylla, S.J.; Park, I.K.; Liu, R.; Wang, X.H.; Cho, R.W.; Hoey, T.; Gurney, A.; Huang, E.H.; Simeone, D.M.; et al. Phenotypic characterization of human colorectal cancer stem cells. Proc. Natl. Acad. Sci. USA 2007, 104, 10158–10163. [Google Scholar] [CrossRef]
- Ricci-Vitiani, L.; Lombardi, D.G.; Pilozzi, E.; Biffoni, M.; Todaro, M.; Peschle, C.; De Maria, R. Identification and expansion of human colon-cancer-initiating cells. Nature 2007, 445, 111–115. [Google Scholar] [CrossRef]
- Barker, N.; Ridgway, R.A.; van Es, J.H.; van de Wetering, M.; Begthel, H.; van den Born, M.; Danenberg, E.; Clarke, A.R.; Sansom, O.J.; Clevers, H. Crypt stem cells as the cells-of-origin of intestinal cancer. Nature 2009, 457, U119–U608. [Google Scholar] [CrossRef]
- Pilati, P.; Mocellin, S.; Bertazza, L.; Galdi, F.; Briarava, M.; Mammano, E.; Tessari, E.; Zavagno, G.; Nitti, D. Prognostic Value of Putative Circulating Cancer Stem Cells in Patients Undergoing Hepatic Resection for Colorectal Liver Metastasis. Ann. Surg. Oncol. 2012, 19, 402–408. [Google Scholar] [CrossRef]
- Lin, E.H.; Hassan, M.; Li, Y.N.; Zhao, H.; Nooka, A.; Sorenson, E.; Xie, K.P.; Champlin, R.; Wu, X.F.; Li, D.H. Elevated circulating endothelial progenitor marker CD133 messenger RNA levels predict colon cancer recurrence. Cancer 2007, 110, 534–542. [Google Scholar] [CrossRef]
- Kakehashi, A.; Ishii, N.; Sugihara, E.; Gi, M.; Saya, H.; Wanibuchi, H. CD44 variant 9 is a potential biomarker of tumor initiating cells predicting survival outcome in hepatitis C virus-positive patients with resected hepatocellular carcinoma. Cancer Sci. 2016, 107, 609–618. [Google Scholar] [CrossRef]
- Nagano, O.; Saya, H. Mechanism and biological significance of CD44 cleavage. Cancer Sci. 2004, 95, 930–935. [Google Scholar] [CrossRef]
- Chen, C.; Zhao, S.J.; Karnad, A.; Freeman, J.W. The biology and role of CD44 in cancer progression: Therapeutic implications. J. Hematol. Oncol. 2018, 11, 64. [Google Scholar] [CrossRef]
- Katoh, S.; Goi, T.; Naruse, T.; Ueda, Y.; Kurebayashi, H.; Nakazawa, T.; Kimura, Y.; Hirono, Y.; Yamaguchi, A. Cancer Stem Cell Marker in Circulating Tumor Cells: Expression of CD44 Variant Exon 9 Is Strongly Correlated to Treatment Refractoriness, Recurrence and Prognosis of Human Colorectal Cancer. Anticancer Res. 2015, 35, 239–244. [Google Scholar]
- Ziranu, P.; Aimola, V.; Pretta, A.; Dubois, M.; Murru, R.; Liscia, N.; Cau, F.; Persano, M.; Deias, G.; Palmas, E.; et al. New Horizons in Metastatic Colorectal Cancer: Prognostic Role of CD44 Expression. Cancers 2023, 15, 1212. [Google Scholar] [CrossRef]
- Kimura, Y.; Goi, T.; Nakazawa, T.; Hirono, Y.; Katayama, K.; Urano, T.; Yamaguchi, A. CD44variant exon 9 plays an important role in colon cancer initiating cells. Oncotarget 2013, 4, 785–791. [Google Scholar] [CrossRef][Green Version]
- Sawai, K.; Goi, T.; Sakamoto, S.; Matsunaka, T.; Maegawa, N.; Koneri, K. Oxidative stress as a biomarker for predicting the prognosis of patients with colorectal cancer. Oncology 2022, 100, 612–619. [Google Scholar] [CrossRef]
- Jogo, T.; Oki, E.; Nakanishi, R.; Ando, K.; Nakashima, Y.; Kimura, Y.; Saeki, H.; Oda, Y.; Maehara, Y.; Mori, M. Expression of CD44 variant 9 induces chemoresistance of gastric cancer by controlling intracellular reactive oxygen spices accumulation. Gastric Cancer 2021, 24, 1100–1101. [Google Scholar] [CrossRef]
- Yamaguchi, A.; Urano, T.; Goi, T.; Saito, M.; Takeuchi, K.; Hirose, K.; Nakagawara, G.; Shiku, H.; Furukawa, K. Expression of a CD44 variant containing exons 8 to 10 is a useful independent factor for the prediction of prognosis in colorectal cancer patients. J. Clin. Oncol. 1996, 14, 1122–1127. [Google Scholar] [CrossRef]
- Li, X.D.; Ji, M.; Wu, J.; Jiang, J.T.; Wu, C.P. Clinical significance of CD44 variants expression in colorectal cancer. Tumori 2013, 99, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Suzuki, H.; Imaeda, H.; Matsuzaki, J.; Tsugawa, H.; Nagano, O.; Asakura, K.; Saya, H.; Hibi, T. CD44 variant 9 expression in primary early gastric cancer as a predictive marker for recurrence. Br. J. Cancer 2013, 109, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Chen, K.; Jiang, P.; Zhang, X.; Li, X. CD44v/CD44s expression patterns are associated with the survival of pancreatic carcinoma patients. Diagn. Pathol. 2014, 9, 79. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Fan, C.W.; Wang, C.; Huang, Q.R.; Meng, W.T.; Yu, Y.Y.; Yang, L.; Peng, Z.H.; Hu, J.K.; Li, Y.; et al. CD133+CD54+CD44+ circulating tumor cells as a biomarker of treatment selection and liver metastasis in patients with colorectal cancer. Oncotarget 2016, 7, 77389–77403. [Google Scholar] [CrossRef] [PubMed]
- Grover, P.K.; Cummins, A.G.; Price, T.J.; Roberts-Thomson, I.C.; Hardingham, J.E. Circulating tumour cells: The evolving concept and the inadequacy of their enrichment by EpCAM-based methodology for basic and clinical cancer research. Ann. Oncol. 2014, 25, 1506–1516. [Google Scholar] [CrossRef] [PubMed]
- Bednarz-Knoll, N.; Alix-Panabières, C.; Pantel, K. Plasticity of disseminating cancer cells in patients with epithelial malignancies. Cancer Metastasis Rev. 2012, 31, 673–687. [Google Scholar] [CrossRef] [PubMed]
- van de Stolpe, A.; Pantel, K.; Sleijfer, S.; Terstappen, L.W.; den Toonder, J.M.J. Circulating Tumor Cell Isolation and Diagnostics: Toward Routine Clinical Use. Cancer Res. 2011, 71, 5955–5960. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Folkman, J. Patterns and emerging mechanisms of the angiogenic switch during tumorigenesis. Cell 1996, 86, 353–364. [Google Scholar] [CrossRef]
- Bellizzi, A.; Sebastian, S.; Ceglia, P.; Centonze, M.; Divella, R.; Manzillo, E.F.; Azzariti, A.; Silvestris, N.; Montemurro, S.; Caliandro, C.; et al. Co-expression of CD133(+)/CD44(+) in human colon cancer and liver metastasis. J. Cell. Physiol. 2013, 228, 408–415. [Google Scholar] [CrossRef]
- Goi, T.; Yamaguchi, A.; Takeuchi, K.; Nakagawa, G.; Yamashiro, S.; Furukawa, K.; Urano, T.; Shiku, H. CD44 with variant exons 8-10 in colorectal tumors: Expression analysis by a variant exon 9-specific monoclonal antibody. Int. J. Oncol. 1996, 8, 657–662. [Google Scholar]
- Yamaguchi, A.; Goi, T.; Yu, J.R.; Hirono, Y.; Ishida, M.; Iida, A.; Kimura, T.; Takeuchi, K.; Katayama, K.; Hirose, K. Expression of CD44v6 in advanced gastric cancer and its relationship to hematogenous metastasis and long-term prognosis. J. Surg. Oncol. 2002, 79, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Jang, B.I.; Li, Y.; Graham, D.Y.; Cen, P.T. The Role of CD44 in the Pathogenesis, Diagnosis, and Therapy of Gastric Cancer. Gut Liver 2011, 5, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Seki, K.; Yamaguchi, A.; Goi, T.; Nakagawara, G.; Matsukawa, S.; Urano, T.; Furukawa, K. Inhibition of liver metastasis formation by anti-CD44 variant exon 9 monoclonal antibody. Int. J. Oncol. 1997, 11, 1257–1261. [Google Scholar] [CrossRef] [PubMed]
- Jia, S.Y.; Zhang, R.; Li, Z.Y.; Li, J.M. Clinical and biological significance of circulating tumor cells, circulating tumor DNA, and exosomes as biomarkers in colorectal cancer. Oncotarget 2017, 8, 55632–55645. [Google Scholar] [CrossRef] [PubMed]
- Wanebo, H.J.; Rao, B.; Pinsky, C.M.; Hoffman, R.G.; Stearns, M.; Schwartz, M.K.; Oettgen, H.F. Preoperative carcinoembryonic antigen level as a prognostic indicator in colorectal cancer. N. Engl. J. Med. 1978, 299, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Grem, J. The prognostic importance of tumor markers in adenocarcinomas of the gastrointestinal tract. Curr. Opin. Oncol. 1997, 9, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Iinuma, H.; Watanabe, T.; Mimori, K.; Adachi, M.; Hayashi, N.; Tamura, J.; Matsuda, K.; Fukushima, R.; Okinaga, K.; Sasako, M.; et al. Clinical Significance of Circulating Tumor Cells, Including Cancer Stem-Like Cells, in Peripheral Blood for Recurrence and Prognosis in Patients with Dukes’ Stage B and C Colorectal Cancer. J. Clin. Oncol. 2011, 29, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.Y.; Yang, C.Y.; Yeh, P.H.; Hsu, C.J.; Chang, L.W.; Chan, W.J.; Lin, C.P.; Lyu, Y.Y.; Wu, W.C.; Lee, C.W.; et al. Highly Correlated Recurrence Prognosis in Patients with Metastatic Colorectal Cancer by Synergistic Consideration of Circulating Tumor Cells/Microemboli and Tumor Markers CEA/CA19-9. Cells 2021, 10, 1149. [Google Scholar] [CrossRef]
- Chu, H.Y.; Lu, L.S.; Cho, W.; Wu, S.Y.; Chang, Y.C.; Lin, C.P.; Yang, C.Y.; Lin, C.H.; Jiang, J.K.; Tseng, F.G. Enumerating Circulating Tumor Cells with a Self-Assembled Cell Array (SACA) Chip: A Feasibility Study in Patients with Colorectal Cancer. Cancers 2019, 11, 56. [Google Scholar] [CrossRef]
- Yamaguchi, A.; Goi, T.; Seki, K.; Ohtaki, N.; Maehara, M.; Kobayashi, T.; Niimoto, S.; Katayama, K.; Hirose, K.; Nakagawara, G.; et al. Clinical significance of combined immunohistochemical detection of CD44v and sialyl lex expression for colorectal cancer patients undergoing curative resection. Oncology 1998, 55, 400–404. [Google Scholar] [CrossRef]
- Chen, R.S.; Song, Y.M.; Zhou, Z.Y.; Tong, T.; Li, Y.; Fu, M.; Guo, X.L.; Dong, L.J.; He, X.; Qiao, H.X.; et al. Disruption of xCT inhibits cancer cell metastasis via the caveolin-1/beta-catenin pathway. Oncogene 2009, 28, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Doi, T.; Nagano, O.; Imamura, C.K.; Ozeki, T.; Ishii, Y.; Tsuchihashi, K.; Takahashi, S.; Nakajima, T.E.; Hironaka, S.; et al. Dose-escalation study for the targeting of CD44v(+) cancer stem cells by sulfasalazine in patients with advanced gastric cancer (EPOC1205). Gastric Cancer 2017, 20, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Doi, T.; Nagano, O.; Fukutani, M.; Hasegawa, H.; Nomura, S.; Sato, A.; Kuwata, T.; Asai, K.; Einaga, Y.; et al. Phase 1 study of sulfasalazine and cisplatin for patients with CD44v-positive gastric cancer refractory to cisplatin (EPOC1407). Gastric Cancer 2017, 20, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Otsubo, K.; Nosaki, K.; Imamura, C.K.; Ogata, H.; Fujita, A.; Sakata, S.; Hirai, F.; Toyokawa, G.; Iwama, E.; Harada, T.; et al. Phase I study of salazosulfapyridine in combination with cisplatin and pemetrexed for advanced non-small-cell lung cancer. Cancer Sci. 2017, 108, 1843–1849. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CD44v9 mRNA | |||||
|---|---|---|---|---|---|
| No. of Cases | Negative Cases (%) | Positive Cases (%) | p-Value | ||
| All cases (%) | 300 | 206 (68.7) | 94 (31.3) | ||
| Age (average years) | 66.8 | 69.5 | 0.068 | ||
| Gender | Male | 177 | 122 (68.9) | 55 (31.1) | 0.907 |
| Female | 123 | 84 (68.3) | 39 (31.7) | ||
| Location | Right colon | 110 | 71 (64.6) | 39 (35.5) | 0.242 |
| Left colon | 190 | 135 (71.5) | 55 (28.6) | ||
| Size (average mm) | 45.08 | 47.00 | 0.462 | ||
| Histological type | Differentiated | 278 | 189 (68.0) | 89 (32.0) | 0.366 |
| Undifferentiated | 22 | 17 (77.3) | 5 (22.7) | ||
| Serosa invasion | Negative | 85 | 64 (75.3) | 21 (24.7) | 0.120 |
| Positive | 215 | 142 (66.0) | 73 (34.0) | ||
| Lymph node metastasis | Negative | 160 | 119 (74.4) | 41 (25.6) | 0.023 |
| Positive | 140 | 87 (62.1) | 53 (37.9) | ||
| Liver metastasis | Negative | 263 | 187 (71.1) | 76 (28.9) | 0.015 |
| Positive | 37 | 19 (51.4) | 18 (48.6) | ||
| Lung metastasis | Negative | 265 | 189 (71.3) | 76 (28.7) | 0.043 |
| Positive | 15 | 7 (46.7) | 8 (53.3) | ||
| Stage | I, II | 154 | 114 (74.0) | 40 (26.0) | 0.040 |
| III, IV | 146 | 92 (63.0) | 54 (37.0) | ||
| CEA | 5.0> | 172 | 117 (68.0) | 55 (32.0) | 0.781 |
| 5.0≤ | 128 | 89 (69.5) | 39 (30.5) | ||
| Multivariate | ||||
|---|---|---|---|---|
| Variable | Odds Ration | 95% CI | p-Value | |
| Age (years) | 0.977 | 0.955–1.000 | 0.48 | |
| Gender | Male vs. Female | 1.040 | 0.587–1.843 | 0.893 |
| Size | 0.998 | 0.982–1.014 | 0.775 | |
| Histological type | Differentiated vs. Undifferentiated | 0.545 | 0.175–1.694 | 0.294 |
| Serosa invasion | Negative vs. Positive | 1.594 | 0.706–3.599 | 0.262 |
| Lymph node metastasis | Negative vs. Positive | 1.837 | 0.983–3.433 | 0.056 |
| Liver metastasis | Negative vs. Positive | 2.728 | 1.131–6.583 | 0.026 |
| Lung metastasis | Negative vs. Positive | 1.544 | 0.478–4.991 | 0.468 |
| CEA | 5.0> vs. 5.0≤ | 0.671 | 0.359–1.255 | 0.212 |
| Multivariate | ||||
|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | |
| Lymph node metastasis | Negative vs. positive | 5.430 | 2.068–14.049 | <0.001 |
| Distant metastasis | Negative vs. positive | 9.281 | 4.743–17.582 | <0.001 |
| Expression of CD44v9 | Negative vs. positive | 1.788 | 1.055–3.001 | 0.029 |
| CEA value | <5 vs. ≥5 | 1.888 | 1.066–3.356 | 0.030 |
| Multivariate | ||||
|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | |
| Lymph node metastasis | Negative vs. positive | 6.143 | 2.297–16.429 | <0.001 |
| Distant metastasis | Negative vs. positive | 9.733 | 5.073–18.672 | <0.001 |
| CD44v9 and CEA | CD44v9 (negative) and CEA < 5 vs. others | 0.314 | 0.137–0.717 | 0.011 |
| Multivariate | ||||
|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | |
| Lymph node metastasis | Negative vs. positive | 5.366 | 2.088–13.793 | <0.001 |
| Distant metastasis | Negative vs. positive | 9.864 | 5.160–18.857 | <0.001 |
| CD44v9 and CEA | CD44v9 (positive) and CEA ≥ 5 ng/mL vs. others | 1.822 | 1.045–3.177 | 0.035 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawai, K.; Goi, T.; Kimura, Y.; Koneri, K. Presence of CD44v9-Expressing Cancer Stem Cells in Circulating Tumor Cells and Effects of Carcinoembryonic Antigen Levels on the Prognosis of Colorectal Cancer. Cancers 2024, 16, 1556. https://doi.org/10.3390/cancers16081556
Sawai K, Goi T, Kimura Y, Koneri K. Presence of CD44v9-Expressing Cancer Stem Cells in Circulating Tumor Cells and Effects of Carcinoembryonic Antigen Levels on the Prognosis of Colorectal Cancer. Cancers. 2024; 16(8):1556. https://doi.org/10.3390/cancers16081556
Chicago/Turabian StyleSawai, Katsuji, Takanori Goi, Youhei Kimura, and Kenji Koneri. 2024. "Presence of CD44v9-Expressing Cancer Stem Cells in Circulating Tumor Cells and Effects of Carcinoembryonic Antigen Levels on the Prognosis of Colorectal Cancer" Cancers 16, no. 8: 1556. https://doi.org/10.3390/cancers16081556
APA StyleSawai, K., Goi, T., Kimura, Y., & Koneri, K. (2024). Presence of CD44v9-Expressing Cancer Stem Cells in Circulating Tumor Cells and Effects of Carcinoembryonic Antigen Levels on the Prognosis of Colorectal Cancer. Cancers, 16(8), 1556. https://doi.org/10.3390/cancers16081556