
Influence of Certification Program on Treatment Quality and Survival for Rectal Cancer Patients in Germany: Results of 13 Certified Centers in Collaboration with AN Institute

 , , ,
, , ,  ,
,  and
and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Perioperative Parameters
3.3. Postoperative Parameters
3.4. Histopathology
3.5. Follow-Up and Survival
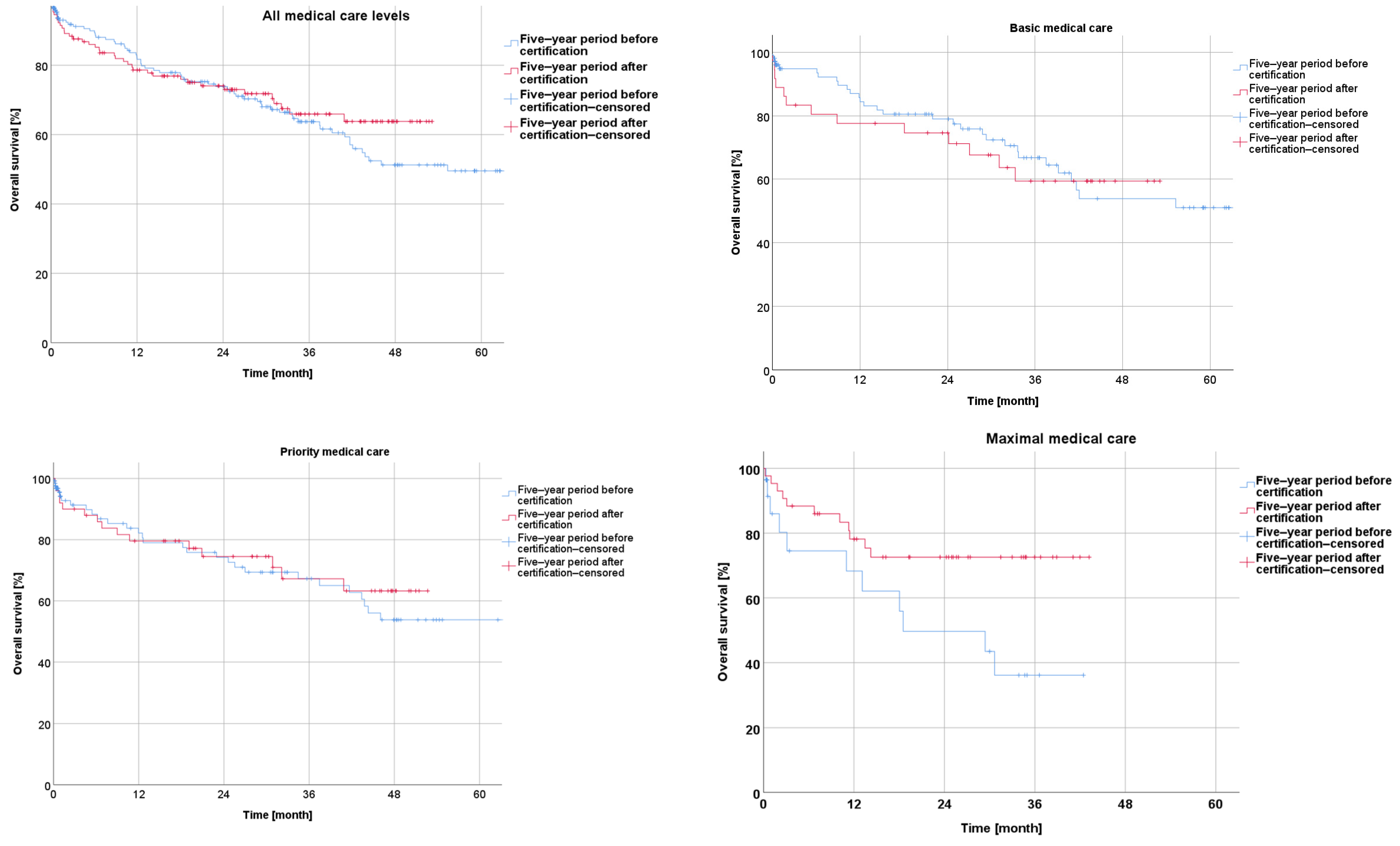
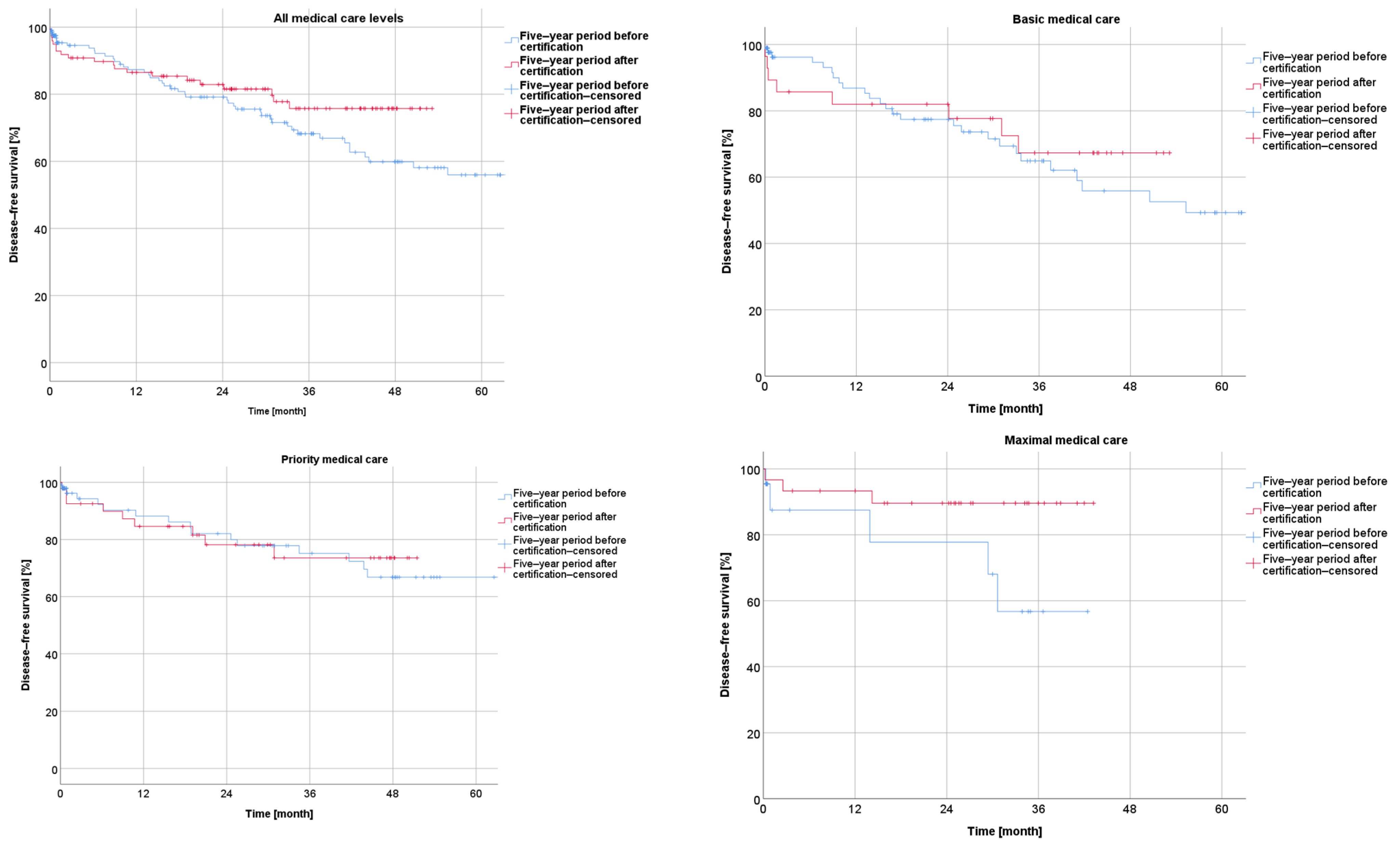
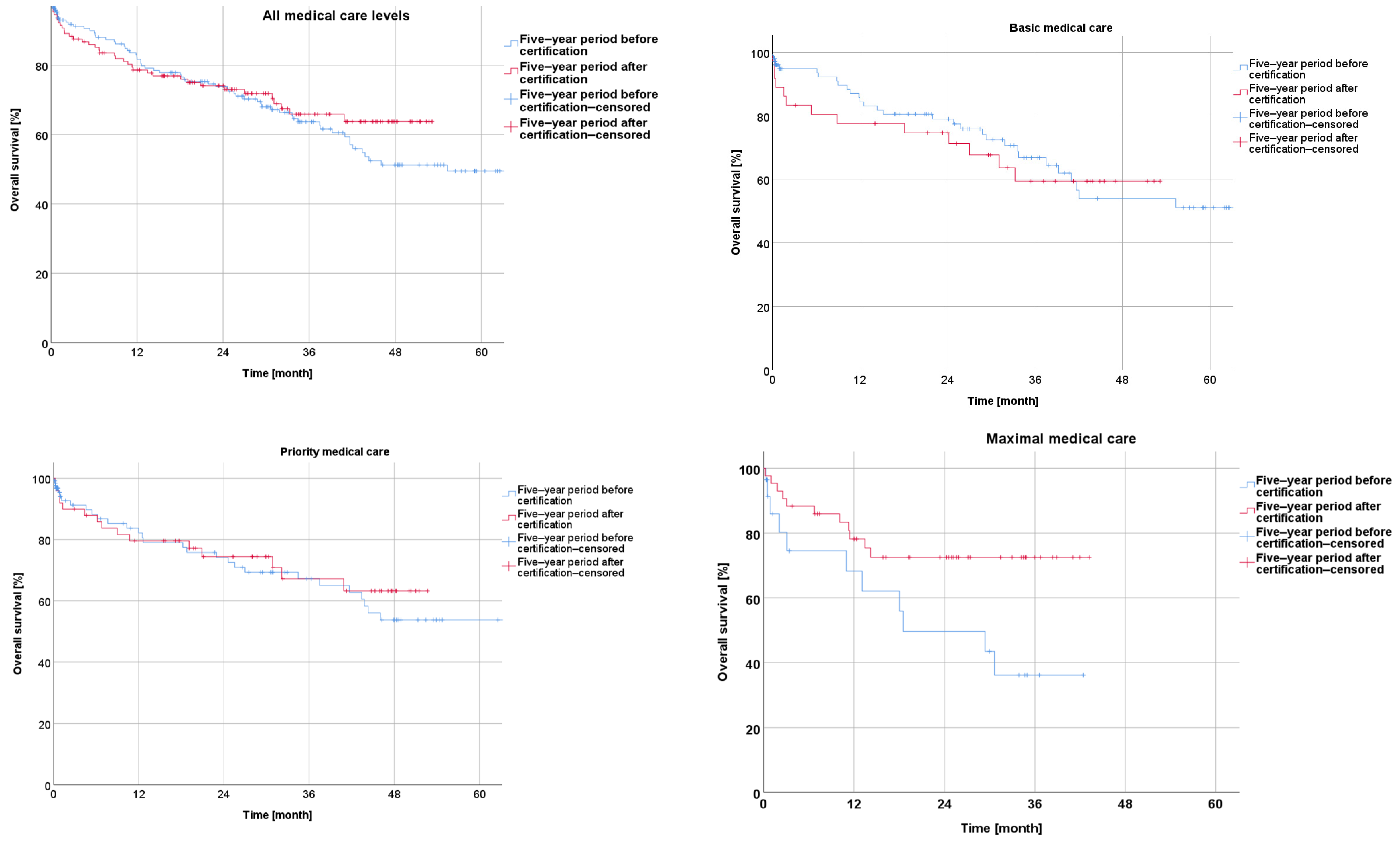
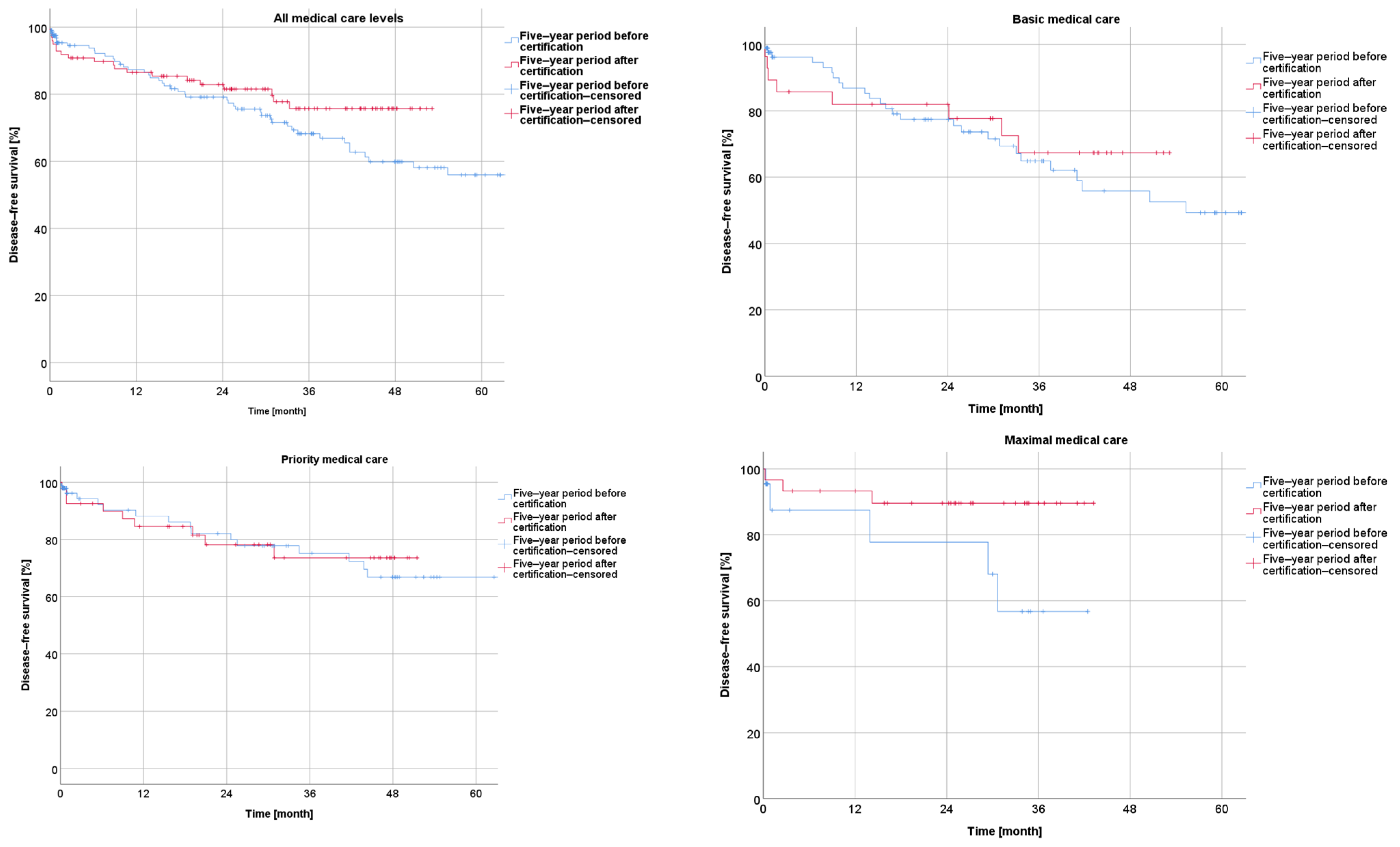
3.5.1. Survival before and after Certification for the Entire Collective and According to the Medical Care Level
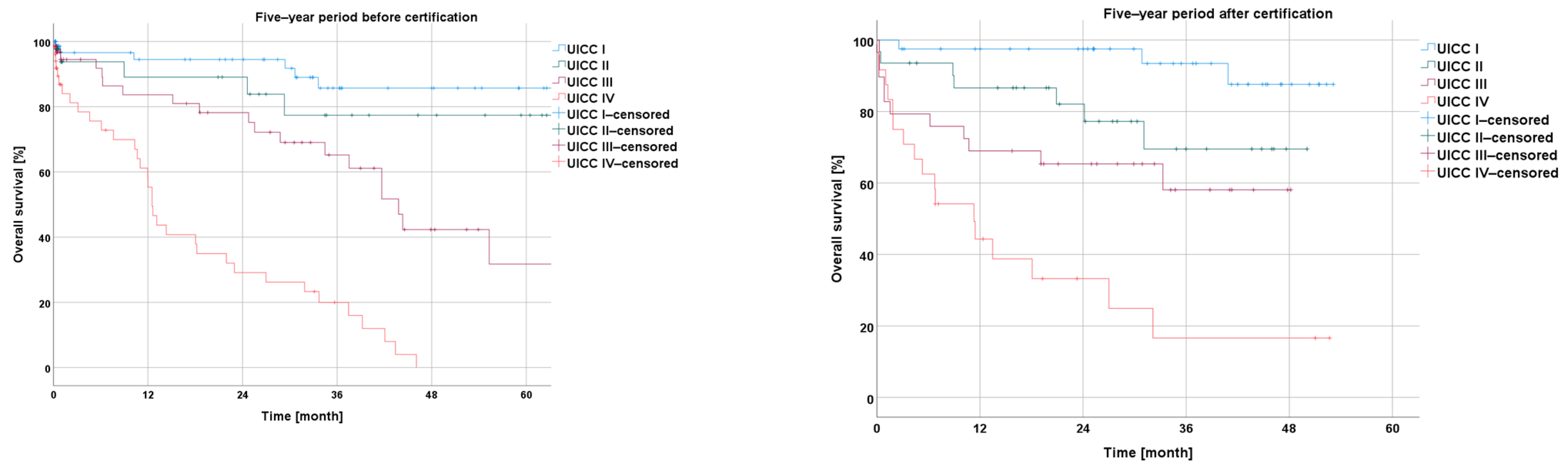
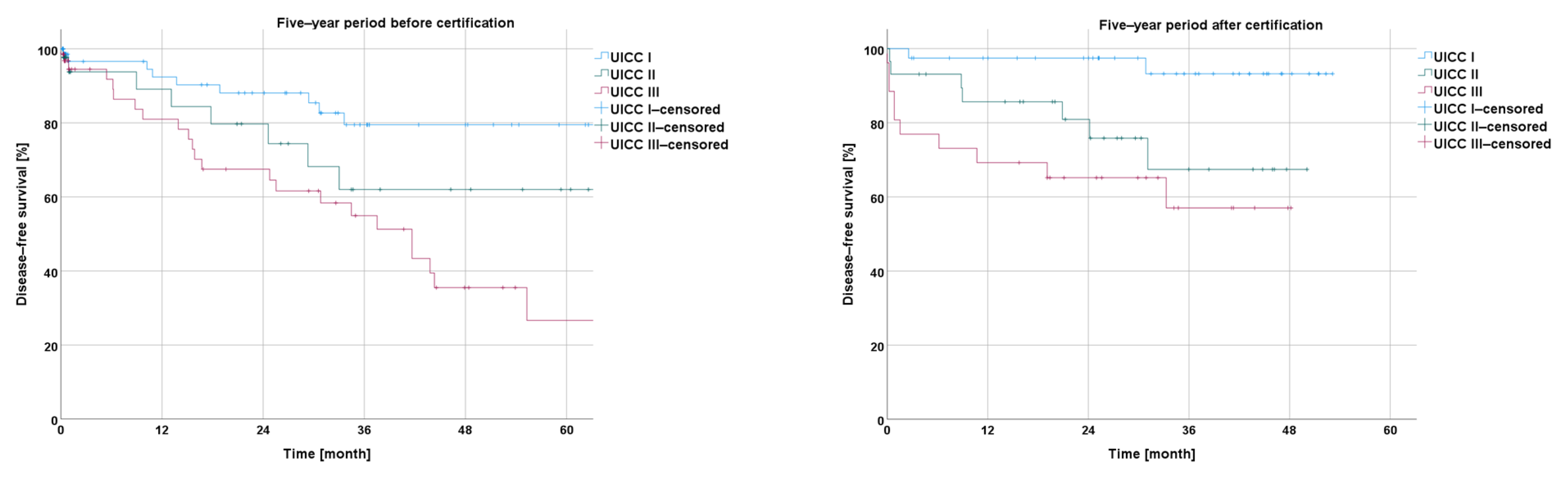
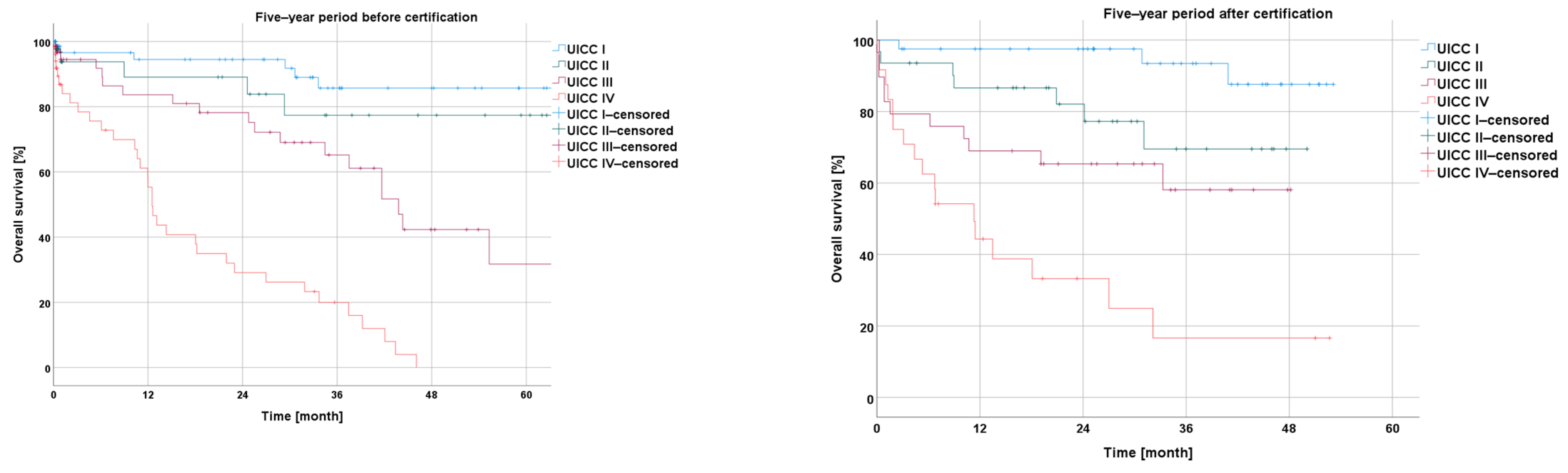
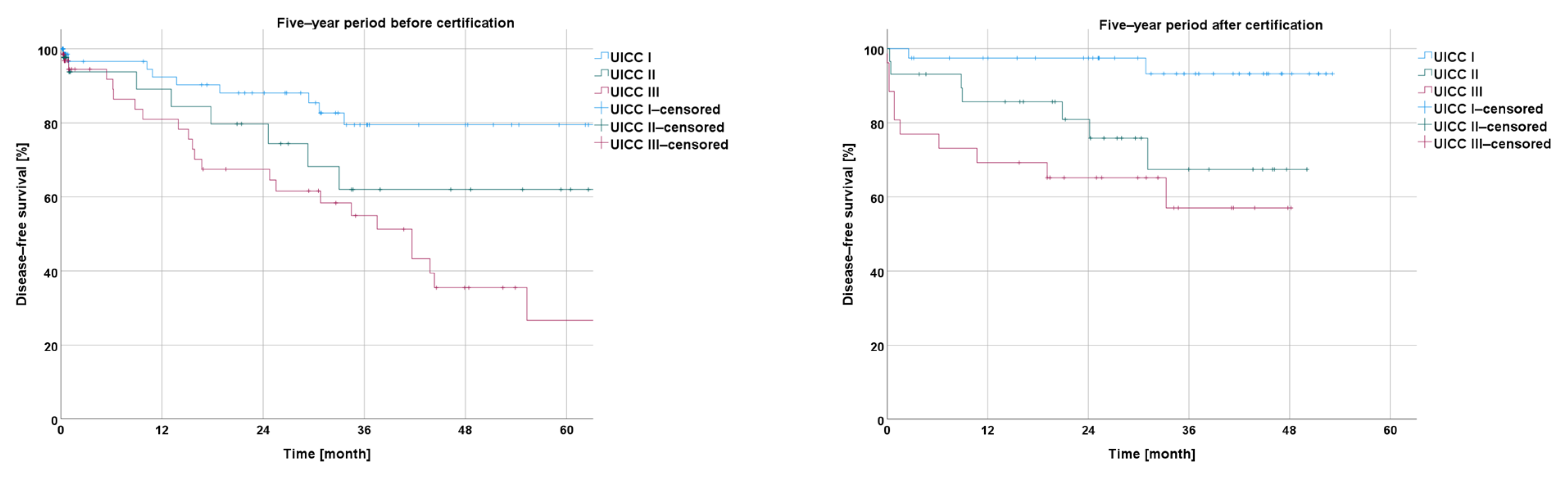
3.5.2. Survival According to UICC Stage
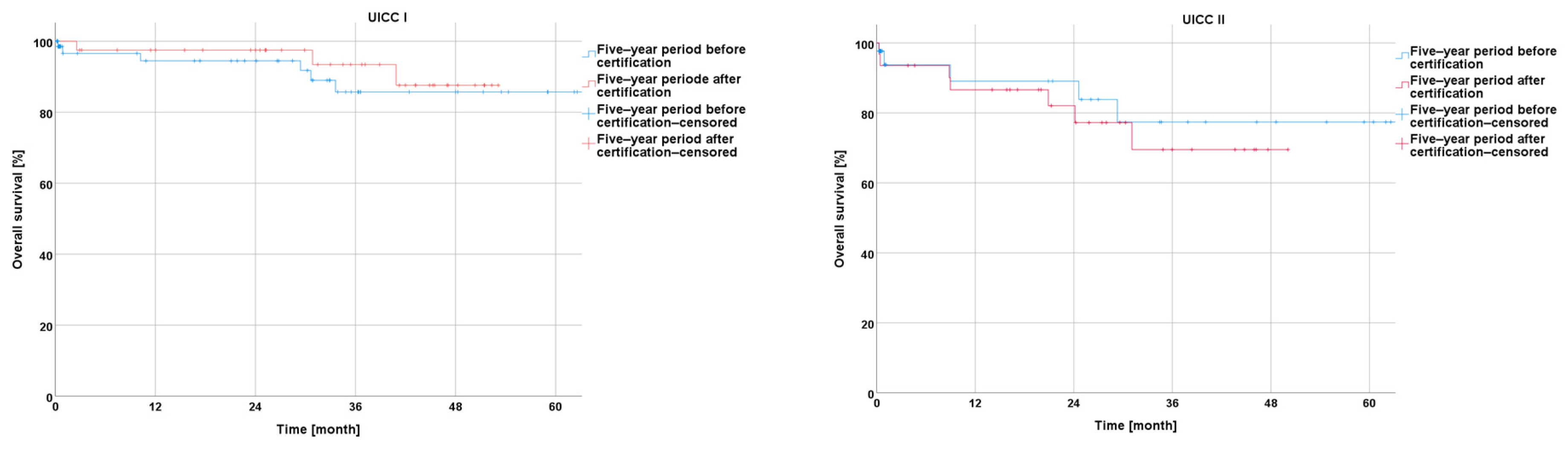
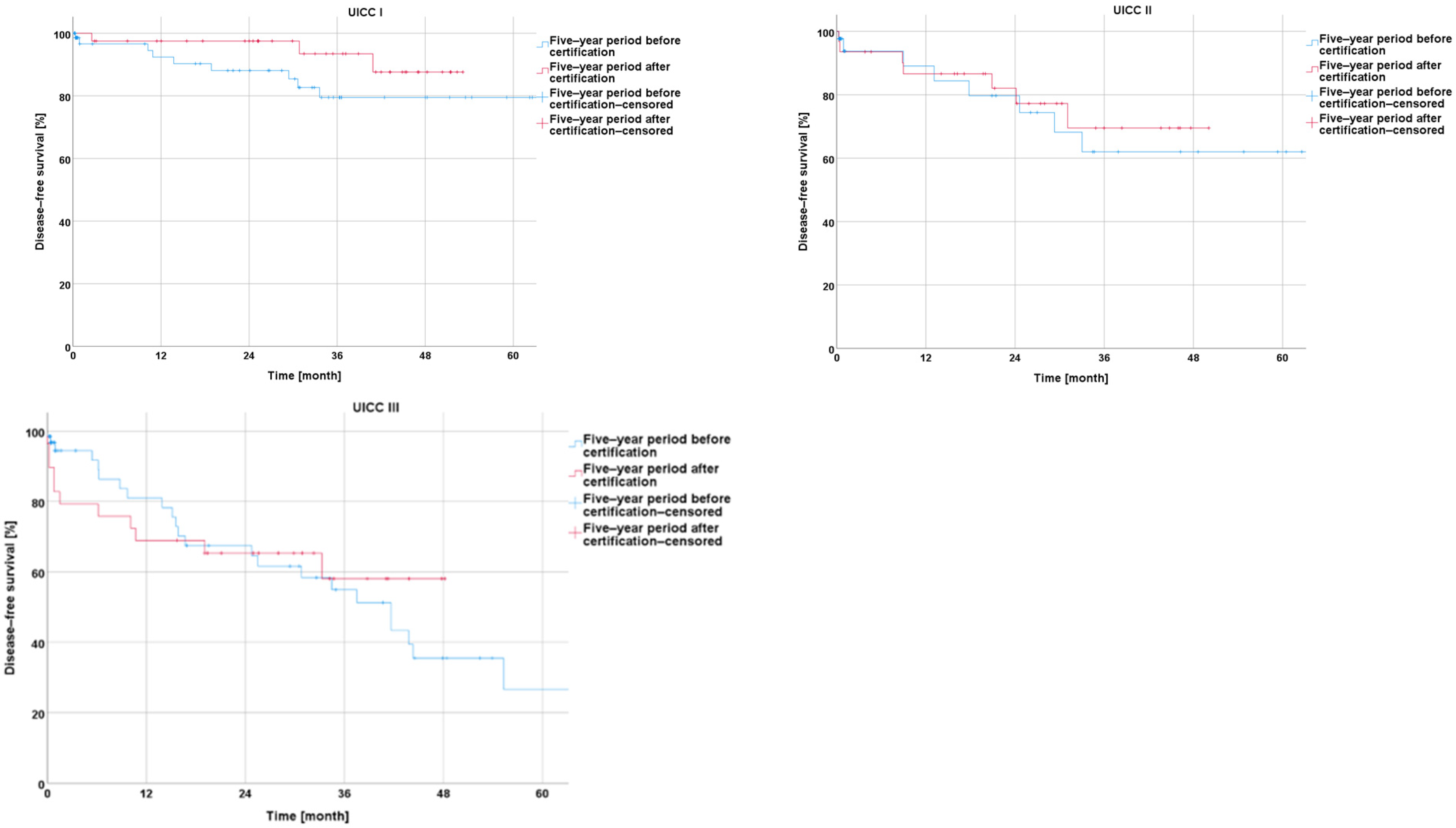
Survival before and after Certification According to UICC Stage
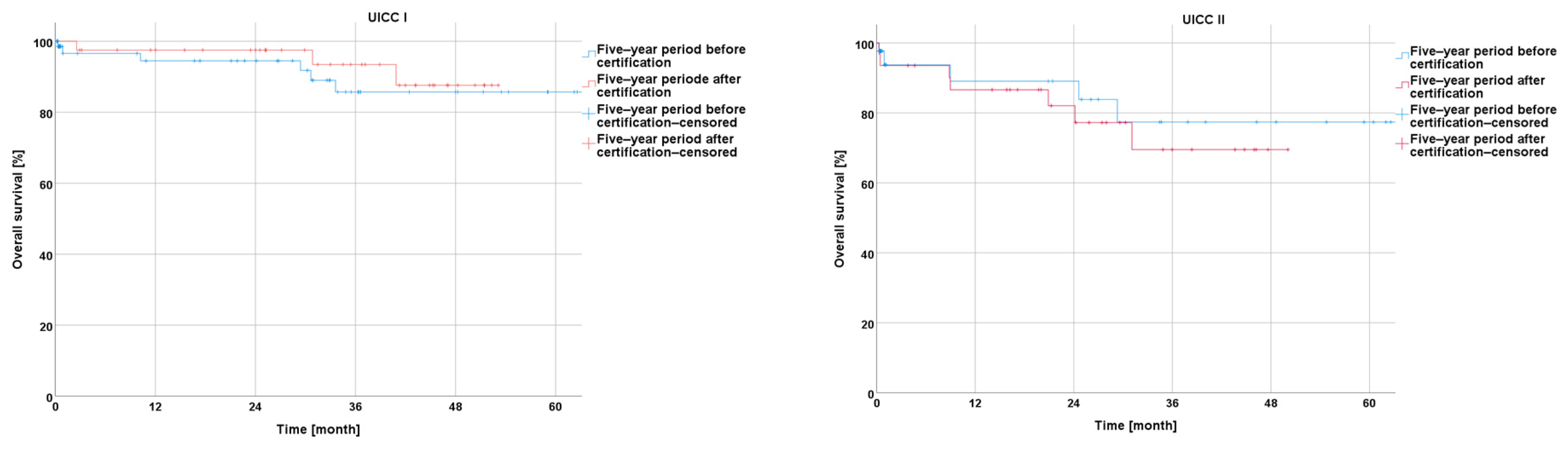
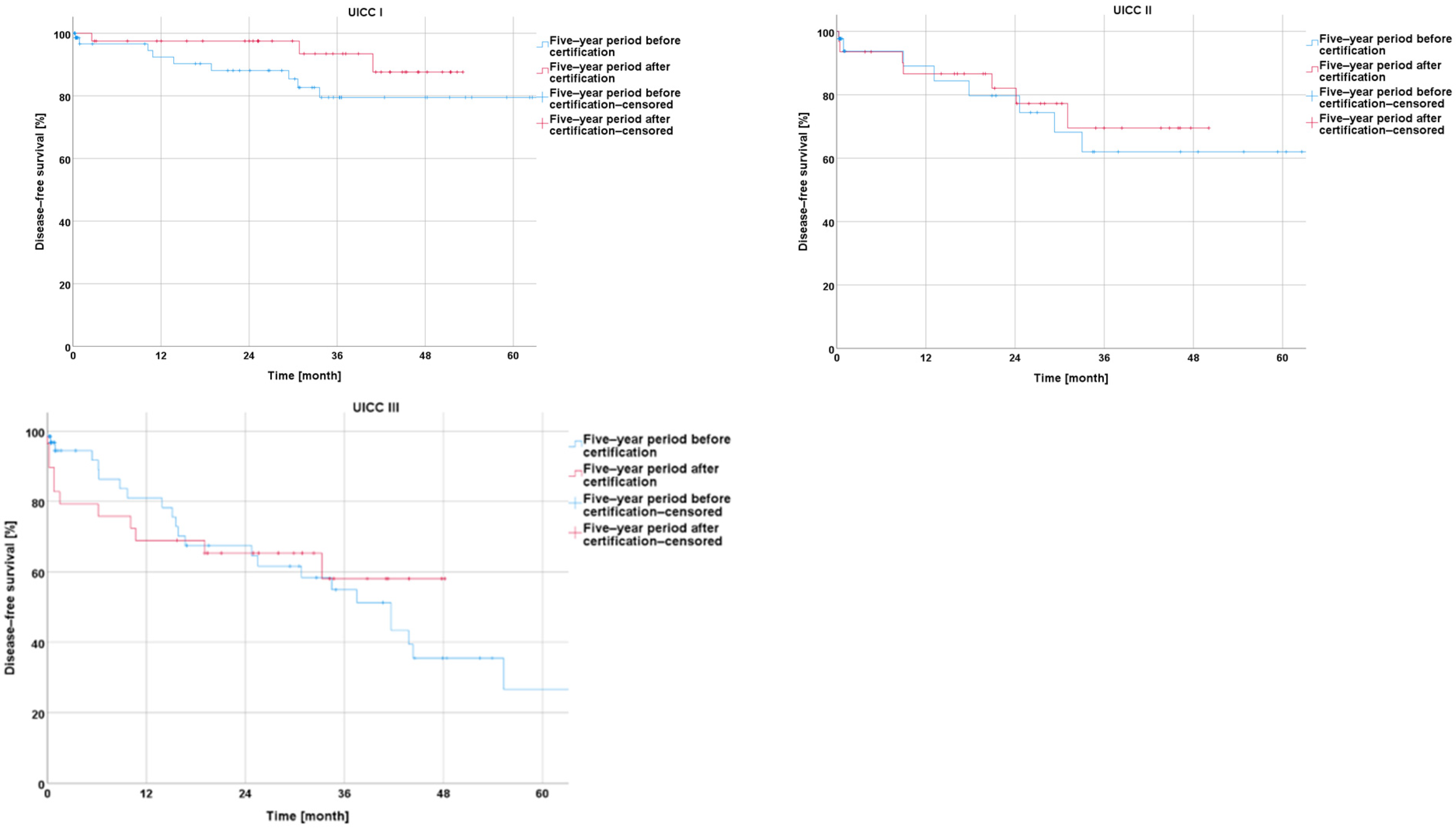
Survival before and after Certification According to Particular UICC Stage
3.5.3. Neoadjuvant and Adjuvant Treatment
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CrCC | colorectal cancer center |
| CRC | colorectal cancer |
| ARR | anterior rectal resection |
| LARR | low anterior rectal resection |
| APE | abdominoperineal excision |
| Min. | minutes |
| Preop. LOS | preoperative length of stay |
| Postop. LOS | postoperative length of stay |
| oLOS | overall length of stay |
| UICC | Union International Contra Cancer |
| TME | total mesorectal excision |
References
- Erdmann, F.; Spix, C.; Katalinic, A.; Christ, M.; Folkerts, J.; Hansmann, J.; Kranzhöfer, K.; Kunz, B.; Manegold, K.; Penzkofer, A.; et al. Robert Koch-Intitute: Cancer in Germany 2017/2018, 13th ed.; 2022; Available online: https://edoc.rki.de/handle/176904/9042 (accessed on 15 November 2023).
- Ghadban, T.; Reeh, M.; Bockhorn, M.; Grotelueschen, R.; Bachmann, K.; Grupp, K.; Uzunoglu, F.G.; Izbicki, J.R.; Perez, D.R. Decentralized colorectal cancer care in Germany over the last decade is associated with high in-hospital morbidity and mortality. Cancer Manag. Res. 2019, 11, 2101–2107. [Google Scholar] [CrossRef]
- Coleman, M.P.; Quaresma, M.; Berrino, F.; Lutz, J.-M.; De Angelis, R.; Capocaccia, R.; Baili, P.; Rachet, B.; Gatta, G.; Hakulinen, T.; et al. Cancer survival in five continents: A worldwide population-based study (CONCORD). Lancet Oncol. 2008, 9, 730–756. [Google Scholar] [CrossRef] [PubMed]
- Sahm, M.; Schneider, C.; Gretschel, S.; Kube, R.; Becker, A.; Gunther, M.; Loew, A.; Jahnke, K.; Mantke, R. Reality of care of colorectal cancer in the State of Brandenburg: With special consideration of the number of hospital cases and certification as a colorectal cancer center. Chirurg 2022, 93, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Richter, M.; Sonnow, L.; Mehdizadeh-Shrifi, A.; Richter, A.; Koch, R.; Zipprich, A. German oncology certification system for colorectal cancer—Relative survival rates of a single certified centre vs. national and international registry data. Innov. Surg. Sci. 2021, 6, 67–73. [Google Scholar] [CrossRef]
- German S3 Guideline for Treatment of Colorectal Cancer Online. S3-Leitlinie Kolorektales Karzinom. 2019. Available online: https://register.awmf.org/assets/guidelines/021-007OLl_S3_Kolorektales-Karzinom-KRK_2019-01.pdf (accessed on 15 November 2023).
- Hohenberger, W.; Bittorf, B.; Papadopoulos, T.; Merkel, S. Survival after surgical treatment of cancer of the rectum. Langenbeck’s Arch. Surg. 2005, 390, 363–372. [Google Scholar] [CrossRef]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef]
- Fleischmann, M.; Diefenhardt, M.; Nicolas, A.M.; Rodel, F.; Ghadimi, M.; Hofheinz, R.D.; Greten, F.R.; Rodel, C.; Fokas, E.; German Rectal Cancer Study Group. ACO/ARO/AIO-21—Capecitabine-based chemoradiotherapy in combination with the IL-1 receptor antagonist anakinra for rectal cancer Patients: A phase I trial of the German rectal cancer study group. Clin. Transl. Radiat. Oncol. 2022, 34, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Diefenhardt, M.; Fleischmann, M.; Martin, D.; Hofheinz, R.D.; Piso, P.; Germer, C.T.; Hambsch, P.; Grutzmann, R.; Kirste, S.; Schlenska-Lange, A.; et al. Clinical outcome after total neoadjuvant treatment (CAO/ARO/AIO-12) versus intensified neoadjuvant and adjuvant treatment (CAO/ARO/AIO-04) a comparison between two multicenter randomized phase II/III trials. Radiother. Oncol. 2023, 179, 109455. [Google Scholar] [CrossRef]
- Kowalski, C.; Graeven, U.; von Kalle, C.; Lang, H.; Beckmann, M.W.; Blohmer, J.U.; Burchardt, M.; Ehrenfeld, M.; Fichtner, J.; Grabbe, S.; et al. Shifting cancer care towards Multidisciplinarity: The cancer center certification program of the German cancer society. BMC Cancer 2017, 17, 850. [Google Scholar] [CrossRef]
- Rückher, J.; Bokemeyer, C.; Fehm, T.; Graeven, U.; Wesselmann, S. Das Zertifizierungssystem der Deutschen Krebsgesellschaft. Nutzen und Weiterentwicklung. Onkologe 2021, 27, 969–979. [Google Scholar] [CrossRef]
- Benz, S.; Wesselmann, S.; Seufferlein, T. Stellenwert von zertifizierten Darmkrebszentren in der Behandlung des kolorektalen Karzinoms. Gastroenterologe 2020, 15, 310–316. [Google Scholar] [CrossRef]
- Archampong, D.; Borowski, D.; Wille-Jorgensen, P.; Iversen, L.H. Workload and surgeon’s specialty for outcome after colorectal cancer surgery. Cochrane Database Syst. Rev. 2012, CD005391. [Google Scholar] [CrossRef]
- Aquina, C.T.; Probst, C.P.; Becerra, A.Z.; Iannuzzi, J.C.; Kelly, K.N.; Hensley, B.J.; Rickles, A.S.; Noyes, K.; Fleming, F.J.; Monson, J.R. High volume improves outcomes: The argument for centralization of rectal cancer surgery. Surgery 2016, 159, 736–748. [Google Scholar] [CrossRef] [PubMed]
- Trautmann, F.; Reissfelder, C.; Pecqueux, M.; Weitz, J.; Schmitt, J. Evidence-based quality standards improve prognosis in colon cancer care. Eur. J. Surg. Oncol. 2018, 44, 1324–1330. [Google Scholar] [CrossRef] [PubMed]
- Klaue, H.J.C. Certification of Colorectal Cancer Units—A Critical Overview on the Basis of Unsettled Aspects. Zentralblatt Chir. 2013, 138, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Hermanek, P.; Hermanek, P.; Hohenberger, W.; Klimpfinger, M.; Kockerling, F.; Papadopoulos, T. The pathological assessment of mesorectal excision: Implications for further treatment and quality management. Int. J. Color. Dis. 2003, 18, 335–341. [Google Scholar] [CrossRef] [PubMed]
- West, N.P.; Finan, P.J.; Anderin, C.; Lindholm, J.; Holm, T.; Quirke, P. Evidence of the oncologic superiority of cylindrical abdominoperineal excision for low rectal cancer. J. Clin. Oncol. 2008, 26, 3517–3522. [Google Scholar] [CrossRef] [PubMed]
- Leite, J.S.; Martins, S.C.; Oliveira, J.; Cunha, M.F.; Castro-Sousa, F. Clinical significance of macroscopic completeness of mesorectal resection in rectal cancer. Color. Dis. 2011, 13, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Salerno, G.; Daniels, I.R.; Moran, B.J.; Wotherspoon, A.; Brown, G. Clarifying margins in the multidisciplinary management of rectal cancer: The MERCURY experience. Clin. Radiol. 2006, 61, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Göhl, J.; Dörfer, J.; Hohenberger, W.; Merkel, S. Bedeutung der TME im operativen Therapiekonzept des Rektumkarzinoms. Onkologe 2007, 13, 365–374. [Google Scholar] [CrossRef]
- Herzog, T.; Belyaev, O.; Chromik, A.M.; Weyhe, D.; Mueller, C.A.; Munding, J.; Tannapfel, A.; Uhl, W.; Seelig, M.H. TME quality in rectal cancer surgery. Eur. J. Med. Res. 2010, 15, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Draeger, T.; Volkel, V.; Gerken, M.; Klinkhammer-Schalke, M.; Furst, A. Long-term oncologic outcomes after laparoscopic versus open rectal cancer resection: A high-quality population-based analysis in a Southern German district. Surg. Endosc. 2018, 32, 4096–4104. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, C.; Sibert, N.T.; Breidenbach, C.; Hagemeier, A.; Roth, R.; Seufferlein, T.; Benz, S.; Post, S.; Siegel, R.; Wiegering, A.; et al. Outcome Quality After Colorectal Cancer Resection in Certified Colorectal Cancer Centers—Patient-Reported and Short-Term Clinical Outcomes. Dtsch. Arztebl. Int. 2022, 119, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Klinkhammer-Schalke, M.; Bierbaum, V.; Gerken, M.; Bobeth, C.; Rößler, M.; Dröge, P.; Ruhnke, T.; Günster, C.; Kleihues-van Tol, K.; et al. Initial Cancer Treatment in Certified Versus Non-Certified Hospitals. Dtsch. Ärzteblatt Int. 2023, 120, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Conticchio, M.; Papagni, V.; Notarnicola, M.; Delvecchio, A.; Riccelli, U.; Ammendola, M.; Curro, G.; Pessaux, P.; Silvestris, N.; Memeo, R. Laparoscopic vs. open mesorectal excision for rectal cancer: Are these approaches still comparable? A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235887. [Google Scholar] [CrossRef] [PubMed]
- Acuna, S.A.; Chesney, T.R.; Ramjist, J.K.; Shah, P.S.; Kennedy, E.D.; Baxter, N.N. Laparoscopic Versus Open Resection for Rectal Cancer: A Noninferiority Meta-analysis of Quality of Surgical Resection Outcomes. Ann. Surg. 2019, 269, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Schnitzbauer, V.; Gerken, M.; Benz, S.; Volkel, V.; Draeger, T.; Furst, A.; Klinkhammer-Schalke, M. Laparoscopic and open surgery in rectal cancer patients in Germany: Short and long-term results of a large 10-year population-based cohort. Surg. Endosc. 2020, 34, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Hanna, G.B.; Mackenzie, H.; Miskovic, D.; Ni, M.; Wyles, S.; Aylin, P.; Parvaiz, A.; Cecil, T.; Gudgeon, A.; Griffith, J.; et al. Laparoscopic Colorectal Surgery Outcomes Improved After National Training Program (LAPCO) for Specialists in England. Ann. Surg. 2022, 275, 1149–1155. [Google Scholar] [CrossRef]
- Hong, S.W.; Byeon, J.S. Endoscopic diagnosis and treatment of early colorectal cancer. Intest. Res. 2022, 20, 281–290. [Google Scholar] [CrossRef]
- Okolica, D.; Bishawi, M.; Karas, J.R.; Reed, J.F.; Hussain, F.; Bergamaschi, R. Factors influencing postoperative adverse events after Hartmann’s reversal. Color. Dis. 2012, 14, 369–373. [Google Scholar] [CrossRef]
- Zarnescu Vasiliu, E.C.; Zarnescu, N.O.; Costea, R.; Rahau, L.; Neagu, S. Morbidity after reversal of Hartmann operation: Retrospective analysis of 56 patients. J. Med. Life 2015, 8, 488–491. [Google Scholar] [PubMed]
- Hallam, S.; Mothe, B.S.; Tirumulaju, R. Hartmann’s procedure, reversal and rate of stoma-free survival. Ann. R. Coll. Surg. Engl. 2018, 100, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Whitney, S.; Gross, B.D.; Mui, A.; Hahn, S.; Read, B.; Bauer, J. Hartmann’s reversal: Factors affecting complications and outcomes. Int. J. Color. Dis. 2020, 35, 1875–1880. [Google Scholar] [CrossRef] [PubMed]
- Aravani, A.; Samy, E.F.; Thomas, J.D.; Quirke, P.; Morris, E.J.A.; Finan, P.J. A retrospective observational study of length of stay in hospital after colorectal cancer surgery in England (1998–2010). Medicine 2016, 95, e5064. [Google Scholar] [CrossRef] [PubMed]
- Koch, F.; Hohenstein, S.; Bollmann, A.; Kuhlen, R.; Ritz, J.P. Dissemination of fast-track concepts in Germany. Chirurgie 2022, 93, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Koch, F.; Green, M.; Dietrich, M.; Pontau, F.; Moikow, L.; Ulmer, S.; Dietrich, N.; Ritz, J.P. First 18 months as certified ERAS® center for colorectal cancer: Lessons learned and results of the first 261 patients. Chirurgie 2022, 93, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Koch, F.; Dietrich, M.; Green, M.; Moikow, L.; Schmidt, M.; Ristig, M.; Meier-Hellmann, A.; Ritz, J.P. The Usefulness of ERAS Concepts for Colorectal Resections—An Economic Analysis under DRG Conditions. Zentralblatt Chir. 2023, 148, 454–459. [Google Scholar] [CrossRef]
- Harnsberger, C.R.; Maykel, J.A.; Alavi, K. Postoperative Ileus. Clin. Colon Rectal Surg. 2019, 32, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Tittel, A.; Schippers, E.; Anurov, M.; Titkova, S.; Ottinger, A.; Schumpelick, V. Shorter postoperative atony after laparoscopic-assisted colonic resection? An animal study. Surg. Endosc. 2001, 15, 508–512. [Google Scholar] [CrossRef]
- Schwenk, E.S.; Grant, A.E.; Torjman, M.C.; McNulty, S.E.; Baratta, J.L.; Viscusi, E.R. The Efficacy of Peripheral Opioid Antagonists in Opioid-Induced Constipation and Postoperative Ileus: A Systematic Review of the Literature. Reg. Anesth. Pain Med. 2017, 42, 767–777. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CrCC Certification | |||||
|---|---|---|---|---|---|
| −5y | +5y | p | |||
| Parameter | N (Mean) | % (SD) | N (Mean) | % (SD) | |
| Number of patients | 267 | 47.42% | 296 | 52.58% | |
| Sex | 0.925 | ||||
| Female | 109 | 41% | 122 | 41% | |
| Male | 158 | 59% | 174 | 59% | |
| Age | 68 | 10.51 | 68 | 12.67 | 0.712 |
| BMI | 26 | 4.36 | 27 | 4.83 | 0.467 |
| ASA | |||||
| ASA I | 24 | 9% | 27 | 9% | 0.234 |
| ASA II | 153 | 57% | 145 | 49% | |
| ASA III | 87 | 33% | 120 | 41% | |
| ASA IV | 3 | 1% | 3 | 1% | |
| CrCC Certification | |||||
|---|---|---|---|---|---|
| −5y | +5y | p | |||
| Parameter | N (Mean) | % (SD) | N (Mean) | % (SD) | |
| Number of patients | 267 | 47.42% | 296 | 52.57% | |
| Surgical approach | |||||
| Laparotomy | 226 | 86% | 114 | 39% | <0.001 |
| Laparoscopy | 14 | 5% | 160 | 55% | <0.001 |
| Conversion | 2 | 6% | 16 | 9% | 0.504 |
| Trans-anal | 20 | 8% | 3 | 1% | <0.001 |
| Surgery type | |||||
| ARR | 47 | 18% | 47 | 17% | 0.753 |
| LARR | 113 | 43% | 112 | 40% | 0.505 |
| APE | 43 | 16% | 62 | 22% | 0.084 |
| Hartmann | 3 | 1% | 23 | 8% | <0.001 |
| Anastomosis type | |||||
| Stapler | 167 | 63% | 178 | 61% | 0.572 |
| Intraoperative complications | 14 | 5% | 15 | 5,17% | 0.93 |
| Duration of surgery (Min.) | 161 | 74.21 | 192 | 79.33 | <0.001 |
| CrCC Certification | |||||
|---|---|---|---|---|---|
| −5y | +5y | p | |||
| Parameter | N (Mean) | % (SD) | N (Mean) | % (SD) | |
| Number of patients | 267 | 47.42% | 296 | 52.57% | |
| LOS | |||||
| Preop. LOS (days) | 4.71 | 4.55 | 4.13 | 17.95 | <0.001 |
| Postop. LOS (days) | 16.65 | 14.88 | 15.15 | 10.40 | 0.151 |
| Overall LOS (days) | 20.32 | 16.11 | 19.54 | 20.97 | 0.065 |
| Case dismissal | |||||
| Discharge | 237 | 89% | 278 | 94% | 0.060 |
| Transfer | 16 | 6% | 8 | 3% | |
| Death | 14 | 5% | 9 | 3% | |
| Morbidity | 85 | 32% | 112 | 38% | 0.174 |
| Non-surgical complications | 52 | 20% | 52 | 18% | 0.552 |
| Surgical complications | 61 | 23% | 78 | 27% | 0.284 |
| Bleeding | 5 | 2% | 2 | 1% | 0.208 |
| Sepsis | 6 | 2% | 7 | 2% | 0.904 |
| Aseptic wound healing disorder | 6 | 2% | 9 | 3% | 0.539 |
| Wound infection | 8 | 3% | 10 | 3% | 0.771 |
| Abdominal wall dehiscence | 5 | 2% | 4 | 1% | 0.639 |
| Ileus | 5 | 2% | 2 | 1% | 0.208 |
| Atonia (>3 days) | 5 | 2% | 16 | 6% | 0.025 |
| Abscess | 2 | 1% | 4 | 1% | 0.475 |
| Stool fistula | 4 | 2% | 0 | 0% | 0.036 |
| Presacral infection | 4 | 2% | 9 | 3% | 0.213 |
| Peritonitis | 3 | 1% | 1 | 0% | 0.275 |
| Colostomy complication | 1 | 0% | 4 | 1% | 0.211 |
| Multiple organ failure | 2 | 1% | 3 | 1% | 0.725 |
| Anastomotic leakage | 21 | 12% | 21 | 11% | 0.940 |
| CrCC Certification | |||||
|---|---|---|---|---|---|
| −5y | +5y | p | |||
| Parameter | N (Mean) | % (SD) | N (Mean) | % (SD) | |
| Number of patients | 267 | 47.42% | 296 | 52.57% | |
| Histological verification before treatment | 224 | 84% | 272 | 93% | 0.001 |
| pT | |||||
| pT0 | 4 | 2% | 7 | 3% | 0.490 |
| pT1 | 36 | 15% | 28 | 10% | |
| pT2 | 64 | 26% | 83 | 30% | |
| pT3 | 117 | 48% | 133 | 48% | |
| pT4 | 22 | 9% | 26 | 9% | |
| pN | |||||
| pN0 | 124 | 48% | 170 | 59% | 0.001 |
| pN1 | 45 | 17% | 57 | 20% | |
| pN2 | 58 | 22% | 50 | 17% | |
| pNX | 21 | 8% | 5 | 2% | |
| Missing | 12 | 5% | 7 | 2% | |
| L | |||||
| L0 | 120 | 46% | 168 | 58% | <0.001 |
| L+ | 83 | 32% | 105 | 36% | |
| Not examined | 56 | 22% | 19 | 7% | |
| V | |||||
| V0 | 148 | 57% | 207 | 71% | |
| V+ | 47 | 18% | 63 | 22% | <0.001 |
| Not examined | 63 | 24% | 22 | 8% | |
| UICC | |||||
| I | 4 | 2% | 7 | 2% | <0.001 |
| II | 75 | 29% | 82 | 28% | |
| III | 43 | 16% | 65 | 22% | |
| IV | 67 | 25% | 62 | 21% | |
| Missing | 53 | 20% | 58 | 20% | |
| M.E.R.C.U.R.Y. | |||||
| I | / | / | 251 | 94% | / |
| II | / | / | 10 | 4% | / |
| III | / | / | 5 | 2% | / |
| Coning | / | / | 6 | 2% | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andric, M.; Stockheim, J.; Rahimli, M.; Al-Madhi, S.; Acciuffi, S.; Dölling, M.; Croner, R.S.; Perrakis, A. Influence of Certification Program on Treatment Quality and Survival for Rectal Cancer Patients in Germany: Results of 13 Certified Centers in Collaboration with AN Institute. Cancers 2024, 16, 1496. https://doi.org/10.3390/cancers16081496
Andric M, Stockheim J, Rahimli M, Al-Madhi S, Acciuffi S, Dölling M, Croner RS, Perrakis A. Influence of Certification Program on Treatment Quality and Survival for Rectal Cancer Patients in Germany: Results of 13 Certified Centers in Collaboration with AN Institute. Cancers. 2024; 16(8):1496. https://doi.org/10.3390/cancers16081496
Chicago/Turabian StyleAndric, Mihailo, Jessica Stockheim, Mirhasan Rahimli, Sara Al-Madhi, Sara Acciuffi, Maximilian Dölling, Roland Siegfried Croner, and Aristotelis Perrakis. 2024. "Influence of Certification Program on Treatment Quality and Survival for Rectal Cancer Patients in Germany: Results of 13 Certified Centers in Collaboration with AN Institute" Cancers 16, no. 8: 1496. https://doi.org/10.3390/cancers16081496
APA StyleAndric, M., Stockheim, J., Rahimli, M., Al-Madhi, S., Acciuffi, S., Dölling, M., Croner, R. S., & Perrakis, A. (2024). Influence of Certification Program on Treatment Quality and Survival for Rectal Cancer Patients in Germany: Results of 13 Certified Centers in Collaboration with AN Institute. Cancers, 16(8), 1496. https://doi.org/10.3390/cancers16081496