

Estimation of Mediastinal Toxicities after Radiotherapy for Hodgkin Lymphoma—A Normal Tissue Complication Analysis of the HD16/17 Trial by the German Hodgkin Study Group
 , , ,
, , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design of GHSG HD16 and HD17
2.1.1. HD16
2.1.2. HD17
2.2. Patient Data and RT Analysis
2.3. NTCP Calculations
2.4. Statistics and Analysis
3. Results
3.1. Patient Collective
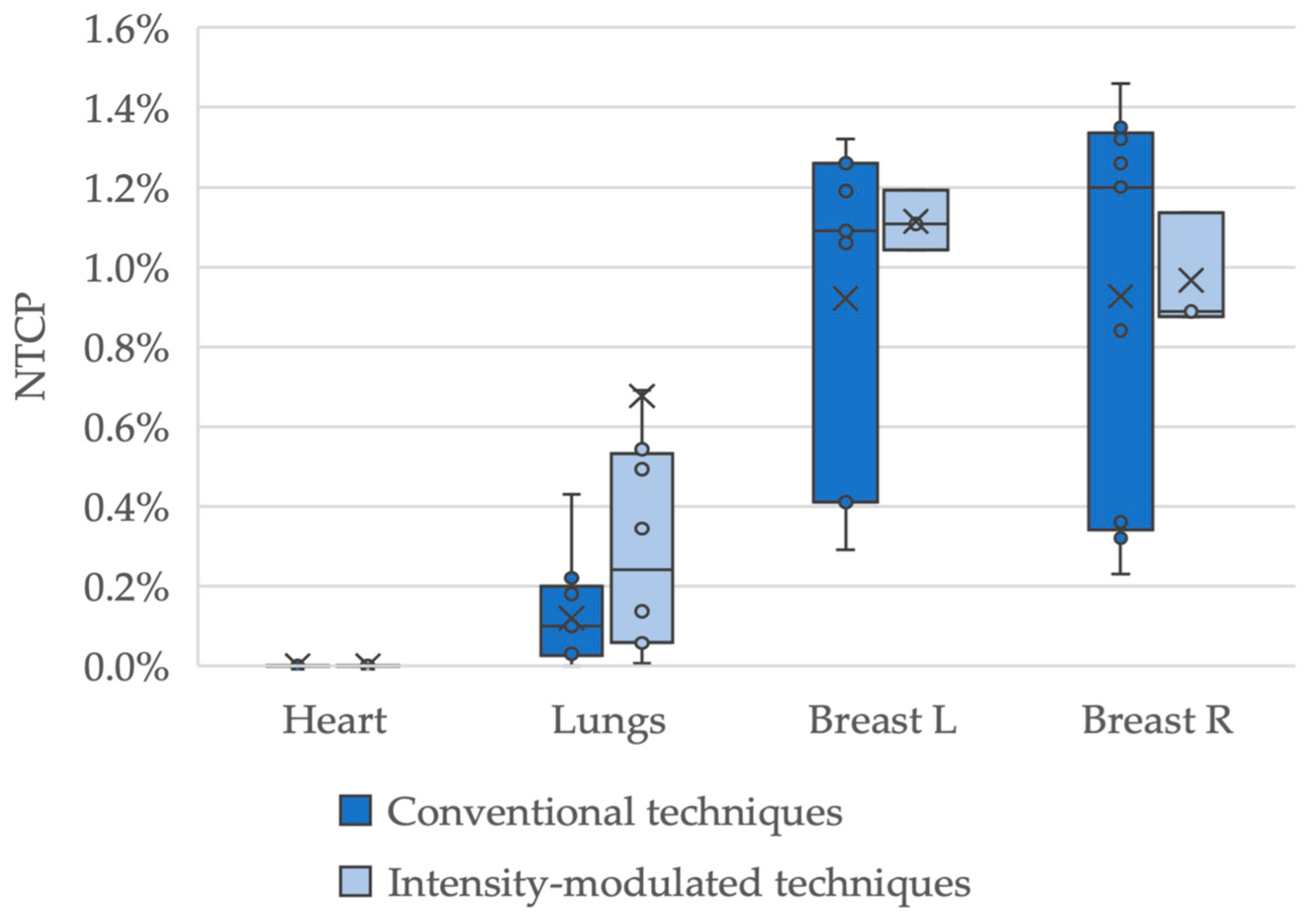
3.2. NTCP Calculations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fuchs, M.; Borchmann, P.; Greil, R.; Hitz, F.; Naumann, R.; Sasse, S.; Engert, A. Hodgkin Lymphom—Onkopedia. Available online: https://www.onkopedia.com/de/onkopedia/guidelines/hodgkin-lymphom/@@guideline/html/index.html (accessed on 16 August 2023).
- Fuchs, M.; Goergen, H.; Kobe, C.; Kuhnert, G.; Lohri, A.; Greil, R.; Sasse, S.; Topp, M.S.; Schäfer, E.; Hertenstein, B.; et al. Positron Emission Tomography-Guided Treatment in Early-Stage Favorable Hodgkin Lymphoma: Final Results of the International, Randomized Phase III HD16 Trial by the German Hodgkin Study Group. J. Clin. Oncol. 2019, 37, 2835–2845. [Google Scholar] [CrossRef]
- Borchmann, P.; Plütschow, A.; Kobe, C.; Greil, R.; Meissner, J.; Topp, M.S.; Ostermann, H.; Dierlamm, J.; Mohm, J.; Thiemer, J.; et al. PET-Guided Omission of Radiotherapy in Early-Stage Unfavourable Hodgkin Lymphoma (GHSG HD17): A Multicentre, Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2021, 22, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Borchmann, P.; Goergen, H.; Kobe, C.; Lohri, A.; Greil, R.; Eichenauer, D.A.; Zijlstra, J.M.; Markova, J.; Meissner, J.; Feuring-Buske, M.; et al. PET-Guided Treatment in Patients with Advanced-Stage Hodgkin’s Lymphoma (HD18): Final Results of an Open-Label, International, Randomised Phase 3 Trial by the German Hodgkin Study Group. Lancet 2017, 390, 2790–2802. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.; Schaapveld, M.; Janus, C.P.M.; Daniëls, L.A.; Petersen, E.J.; Van Der Maazen, R.W.M.; Zijlstra, J.M.; Beijert, M.; Nijziel, M.R.; Verschueren, K.M.S.; et al. Long-Term Cause-Specific Mortality in Hodgkin Lymphoma Patients. J. Natl. Cancer Inst. 2021, 113, 760–769. [Google Scholar] [CrossRef]
- Aleman, B.M.P.; van den Belt-Dusebout, A.W.; Klokman, W.J.; van’t Veer, M.B.; Bartelink, H.; van Leeuwen, F.E. Long-Term Cause-Specific Mortality of Patients Treated for Hodgkin’s Disease. J. Clin. Oncol. 2003, 21, 3431–3439. [Google Scholar] [CrossRef]
- Leitlinienprogramm Onkologie: Hodgkin-Lymphom (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): Diagnostik, Therapie Und Nachsorge Des Hodgkin Lymphoms Bei Erwachsenen Patienten, Langversion 3.2, 2022; AWMF Registernummer: 018/029 OL. Available online: https://www.leitlinienprogramm-onkologie.de/fileadmin/user_upload/Downloads/Leitlinien/Hodgkin/Version_3/LL_Hodgkin_Lymphom_Langversion_3.2.pdf (accessed on 20 December 2023).
- Eich, H.T.; Kriz, J.; Müller, R.P. Evolution of Radiation Therapy within the German Hodgkin Study Group Trials. J. Natl. Compr. Canc. Netw. 2011, 9, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, R.T. Evolution of the Techniques of Radiation Therapy in the Management of Lymphoma. Int. J. Clin. Oncol. 2013, 18, 359–363. [Google Scholar] [CrossRef]
- Pepper, N.B.; Oertel, M.; Kittel, C.; Kröger, K.J.; Elsayad, K.; Haverkamp, U.; Eich, H.T. Impact of Radiation Techniques on Lung Toxicity in Patients with Mediastinal Hodgkin’s Lymphoma. Strahlenther. Onkol. 2021, 197, 56–62. [Google Scholar] [CrossRef]
- Oertel, M.; Hering, D.; Nacke, N.; Kittel, C.; Kröger, K.; Kriz, J.; Fuchs, M.; Baues, C.; Vordermark, D.; Engenhart-Cabillic, R.; et al. Radiation Therapy in the German Hodgkin Study Group HD 16 and HD 17 Trials: Quality Assurance and Dosimetric Analysis for Hodgkin Lymphoma in the Modern Era. Adv. Radiat. Oncol. 2023, 8, 101169. [Google Scholar] [CrossRef]
- Lyman, J.T. Complication Probability as Assessed from Dose-Volume Histograms. Radiat. Res. Suppl. 1985, 8, 13–19. [Google Scholar] [CrossRef]
- Burman, C.; Kutcher, G.J.; Emami, B.; Goitein, M. Fitting of Normal Tissue Tolerance Data to an Analytic Function. Int. J. Radiat. Oncol. Biol. Phys. 1991, 21, 123–135. [Google Scholar] [CrossRef]
- Mukesh, M.B.; Harris, E.; Collette, S.; Coles, C.E.; Bartelink, H.; Wilkinson, J.; Evans, P.M.; Graham, P.; Haviland, J.; Poortmans, P.; et al. Normal Tissue Complication Probability (NTCP) Parameters for Breast Fibrosis: Pooled Results from Two Randomised Trials. Radiother. Oncol. 2013, 108, 293–298. [Google Scholar] [CrossRef]
- Galper, S.L.; Yu, J.B.; Mauch, P.M.; Strasser, J.F.; Silver, B.; LaCasce, A.; Marcus, K.J.; Stevenson, M.A.; Chen, M.H.; Ng, A.K. Clinically Significant Cardiac Disease in Patients with Hodgkin Lymphoma Treated with Mediastinal Irradiation. Blood 2011, 117, 412–418. [Google Scholar] [CrossRef]
- Van Leeuwen, F.E.; Ng, A.K. Long-Term Risk of Second Malignancy and Cardiovascular Disease after Hodgkin Lymphoma Treatment. Hematology Am. Soc. Hematol. Educ. Program 2016, 2016, 323–330. [Google Scholar] [CrossRef]
- Mulrooney, D.A.; Hyun, G.; Ness, K.K.; Ehrhardt, M.J.; Yasui, Y.; Duprez, D.; Howell, R.M.; Leisenring, W.M.; Constine, L.S.; Tonorezos, E.; et al. Major Cardiac Events for Adult Survivors of Childhood Cancer Diagnosed between 1970 and 1999: Report from the Childhood Cancer Survivor Study Cohort. BMJ 2020, 368, l6794. [Google Scholar] [CrossRef]
- Hoeller, U.; Borgmann, K.; Oertel, M.; Haverkamp, U.; Budach, V.; Eich, H.T. Late Sequelae of Radiotherapy: The Effect of Technical and Conceptual Innovations in Radiation Oncology. Dtsch. Arztebl. Int. 2021, 118, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Siaravas, K.C.; Katsouras, C.S.; Sioka, C. Radiation Treatment Mechanisms of Cardiotoxicity: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 6272. [Google Scholar] [CrossRef] [PubMed]
- Hull, M.C.; Morris, C.G.; Pepine, C.J.; Mendenhall, N.P. Valvular Dysfunction and Carotid, Subclavian, and Coronary Artery Disease in Survivors of Hodgkin Lymphoma Treated with Radiation Therapy. JAMA 2003, 290, 2831–2837. [Google Scholar] [CrossRef]
- National Heart Lung and Blood Institute. Coronary Heart Disease-Causes and Risk Factors|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health/coronary-heart-disease/causes (accessed on 16 February 2024).
- van Nimwegen, F.A.; Schaapveld, M.; Cutter, D.J.; Janus, C.P.M.; Krol, A.D.G.; Hauptmann, M.; Kooijman, K.; Roesink, J.; van der Maazen, R.; Darby, S.C.; et al. Radiation Dose-Response Relationship for Risk of Coronary Heart Disease in Survivors of Hodgkin Lymphoma. J. Clin. Oncol. 2016, 34, 235–243. [Google Scholar] [CrossRef]
- Cutter, D.J.; Schaapveld, M.; Darby, S.C.; Hauptmann, M.; Van Nimwegen, F.A.; Krol, A.D.G.; Janus, C.P.M.; Van Leeuwen, F.E.; Aleman, B.M.P. Risk for Valvular Heart Disease After Treatment for Hodgkin Lymphoma. J. Natl. Cancer Inst. 2015, 107, djv008. [Google Scholar] [CrossRef] [PubMed]
- Specht, L.; Yahalom, J. The Concept and Evolution of Involved Site Radiation Therapy for Lymphoma. Int. J. Clin. Oncol. 2015, 20, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Eich, H.T.; Müller, R.P.; Engenhart-Cabillic, R.; Lukas, P.; Schmidberger, H.; Staar, S.; Willich, N. Involved-Node Radiotherapy in Early-Stage Hodgkin’s Lymphoma. Definition and Guidelines of the German Hodgkin Study Group (GHSG). Strahlenther. Onkol. 2008, 184, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, D.C.; Koh, E.S.; Tran, T.H.; Heydarian, M.; Tsang, R.; Pintilie, M.; Xu, T.; Huang, L.; Sachs, R.K.; Brenner, D.J. Individualized Estimates of Second Cancer Risks after Contemporary Radiation Therapy for Hodgkin Lymphoma. Cancer 2007, 110, 2576–2586. [Google Scholar] [CrossRef] [PubMed]
- McKay, M.J.; Taubman, K.L.; Lee, S.; Scott, A.M. Radiotherapy Planning of Lymphomas: Role of Metabolic Imaging with PET/CT. Ann. Nucl. Med. 2022, 36, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Goodman, K.A.; Toner, S.; Hunt, M.; Wu, E.J.; Yahalom, J. Intensity-Modulated Radiotherapy for Lymphoma Involving the Mediastinum. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Cella, L.; Conson, M.; Pressello, M.C.; Molinelli, S.; Schneider, U.; Donato, V.; Orecchia, R.; Salvatore, M.; Pacelli, R. Hodgkin’s Lymphoma Emerging Radiation Treatment Techniques: Trade-Offs between Late Radio-Induced Toxicities and Secondary Malignant Neoplasms. Radiat. Oncol. 2013, 8, 22. [Google Scholar] [CrossRef]
- Oertel, M.; Hering, D.; Baues, C.; Kittel, C.; Fuchs, M.; Kriz, J.; Kröger, K.; Vordermark, D.; Herfarth, K.; Engenhart-Cabillic, R.; et al. Radiation Doses to Mediastinal Organs at Risk in Early-Stage Unfavorable Hodgkin Lymphoma– a Risk Stratified Analysis of the GHSG HD17 Trial. Front. Oncol. 2023, 13, 1183906. [Google Scholar] [CrossRef]
- Cutter, D.J.; Ramroth, J.; Diez, P.; Buckle, A.; Ntentas, G.; Popova, B.; Clifton-Hadley, L.; Hoskin, P.J.; Darby, S.C.; Radford, J.; et al. Predicted Risks of Cardiovascular Disease Following Chemotherapy and Radiotherapy in the UK NCRI RAPID Trial of Positron Emission Tomography–Directed Therapy for Early-Stage Hodgkin Lymphoma. J. Clin. Oncol. 2021, 39, 3591–3601. [Google Scholar] [CrossRef]
- Marks, L.B.; Yorke, E.D.; Jackson, A.; Ten Haken, R.K.; Constine, L.S.; Eisbruch, A.; Bentzen, S.M.; Nam, J.; Deasy, J.O. Use of Normal Tissue Complication Probability Models in the Clinic. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S10–S19. [Google Scholar] [CrossRef]
- Hanania, A.N.; Mainwaring, W.; Ghebre, Y.T.; Hanania, N.A.; Ludwig, M. Radiation-Induced Lung Injury: Assessment and Management. Chest 2019, 156, 150–162. [Google Scholar] [CrossRef]
- Sud, A.; Thomsen, H.; Sundquist, K.; Houlston, R.S.; Hemminki, K. Risk of Second Cancer in Hodgkin Lymphoma Survivors and Influence of Family History. J. Clin. Oncol. 2017, 35, 1584–1590. [Google Scholar] [CrossRef] [PubMed]
- De Gonzalez, A.B.; Curtis, R.E.; Kry, S.F.; Gilbert, E.; Lamart, S.; Berg, C.D.; Stovall, M.; Ron, E. Proportion of Second Cancers Attributable to Radiotherapy Treatment in Adults: A Cohort Study in the US SEER Cancer Registries. Lancet Oncol. 2011, 12, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Swerdlow, A.J.; Barber, J.A.; Hudson, G.V.; Cunningham, D.; Gupta, R.K.; Hancock, B.W.; Horwich, A.; Lister, T.A.; Linch, D.C. Risk of Second Malignancy After Hodgkin’s Disease in a Collaborative British Cohort: The Relation to Age at Treatment. J. Clin. Oncol. 2000, 18, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Viviani, S.; Zinzani, P.L.; Rambaldi, A.; Brusamolino, E.; Levis, A.; Bonfante, V.; Vitolo, U.; Pulsoni, A.; Liberati, A.M.; Specchia, G.; et al. ABVD versus BEACOPP for Hodgkin’s Lymphoma When High-Dose Salvage Is Planned. N. Engl. J. Med. 2011, 365, 203–212. [Google Scholar] [CrossRef]
- Robert Koch-Institut Krebs in Deutschland. Zentrum für Krebsregisterdaten Krebs in Deutschland Für 2019/2020. Available online: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebs_in_Deutschland/krebs_in_deutschland_2023.pdf?__blob=publicationFile (accessed on 20 December 2023).
- Toltz, A.; Shin, N.; Mitrou, E.; Laude, C.; Freeman, C.R.; Seuntjens, J.; Parker, W.; Roberge, D. Late Radiation Toxicity in Hodgkin Lymphoma Patients: Proton Therapy’s Potential. J. Appl. Clin. Med. Phys. 2015, 16, 167–178. [Google Scholar] [CrossRef]
- Edvardsson, A.; Kügele, M.; Alkner, S.; Enmark, M.; Nilsson, J.; Kristensen, I.; Kjellén, E.; Engelholm, S.; Ceberg, S. Comparative Treatment Planning Study for Mediastinal Hodgkin’s Lymphoma: Impact on Normal Tissue Dose Using Deep Inspiration Breath Hold Proton and Photon Therapy. Acta. Oncol. 2019, 58, 95–104. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| n | ||
|---|---|---|
| HD16 | HD17 | |
| Number of patients | 20 | 25 |
| Sex * | ||
| Female | 11 (55) | 12 (48) |
| Male | 8 (40) | 12 (48) |
| Median age at RT | 35 | 26.5 ** |
| IQR | 22 | 17.5 |
| Risk factors | ||
| ≥3 nodal areas | 0 | 15 (60) |
| Elevated erythrocyte sedimentation rate | 0 | 14 (56) |
| Mediastinal bulk | 0 | 8 (32) |
| Extranodal involvement | 0 | 1 (4) |
| Ann Arbor Stage | ||
| IA | 3 (15) | 2 (8) |
| IB | 1 (5) | 1 (4) |
| IIA | 14 (70) | 17 (68) |
| IIB | 2 (10) | 5 (20) |
| Radiation field | ||
| IFRT | 20 | 5 |
| INRT | 0 | 20 |
| Radiation dose | 20 Gy | 30 Gy |
| Deviation from protocol | ||
| None | 18 | 19 |
| Minor | 1 | 2 |
| Major | 1 | 4 |
| Grade 3 toxicities | ||
| Dysphagia | 0 | 1 |
| Nausea | 1 | 0 |
| Mucositis | 1 | 0 |
| HD16 | HD17 | ||
|---|---|---|---|
| Heart | Dmean | 7.6 | 19.6 |
| Dmedian | 6.4 | 20.6 | |
| DIQR | 15.9 | 4.7 | |
| Lungs | Dmean | 5.0 | 10.9 |
| Dmedian | 5.4 | 11.0 | |
| DIQR | 4.2 | 3.2 | |
| Breast L | Dmean | 15.3 | 22.4 |
| Dmedian | 18.4 | 26.2 | |
| DIQR | 5.8 | 14.5 | |
| Breast R | Dmean | 11.9 | 21.2 |
| Dmedian | 16.2 | 24.6 | |
| DIQR | 14.4 | 18.0 |
| Organ at Risk | Endpoint | Study | n | Median (%) | IQR | p |
|---|---|---|---|---|---|---|
| Heart | Pericarditis | HD16 | 20 | 0.0 | 0.0 | - |
| HD17 | 25 | 0.0 | 0.0 | |||
| Lungs | Pneumonitis | HD16 | 20 | 0.0 | 0.0 | <0.01 |
| HD17 | 25 | 0.1 | 0.4 | |||
| Left Breast | Breast Fibrosis | HD16 | 11 | 0.7 | 0.2 | 0.02 |
| HD17 | 12 | 1.1 | 0.7 | |||
| Right Breast | Breast fibrosis | HD16 | 11 | 0.6 | 0.4 | 0.01 |
| HD17 | 12 | 1.0 | 0.8 |
| Organ at Risk | Cohort | n | Median NTCP (%) | Median NTCP (HD16/HD17) | Median NTCP/PTV | Median NTCP/PTV (HD16/HD17) |
|---|---|---|---|---|---|---|
| Heart | HD16 | 20 | 0.0 | - | 2.12 × 10−21 | - |
| HD17 | 25 | 0.0 | 3.73 × 10−12 | |||
| Lungs | HD16 | 20 | 0.0 | - | 5.54 × 10−9 | - |
| HD17 | 25 | 0.1 | 8.29 × 10−7 | |||
| Breast L | HD16 | 11 | 0.7 | 0.6 | 4.21 × 10−6 | 0.5 |
| HD17 | 12 | 1.1 | 8.09 × 10−6 | |||
| Breast R | HD16 | 11 | 0.6 | 0.6 | 4.03 × 10−6 | 0.5 |
| HD17 | 12 | 1.0 | 8.15 × 10−6 |
| Author Year | Question | Endpoints | NTCP Model/ Risk Estimation | Results | Conclusion |
|---|---|---|---|---|---|
| Hodgson et al. 2007 [26] | Estimated risk difference in secondary malignancies for RT mantle 35 Gy, 35 Gy IFRT and 20 Gy IFRT | Lung cancer breast cancer | Radio- biological modeling of carcinogenesis | Compared to mantle RT, 35 Gy IFRT reduced 20-year ERR of breast cancer and lung cancer by 63% and 21%, respectively, 20 Gy IFRT reduced ERR by 77% and 57% | IFRT is predicted to have a decreased risk compared to mantle RT, but considerable interindividual variations exist |
| Pepper et al. 2021 [10] | Impact of RT technique on radiation induced lung disease | Pneumonitis, pulmonary secondary malignancies | LKB QUANTEC EQD-based function | According to QUANTEC parameters, pneumonitis risk is increased by 1% for 5-field IMRT and 2.6% for 7-field IMRT, in comparison to APPA (smaller risk increase with LKB model). Secondary pulmonary malignancy risk is increased by 0.1% and 0.19% for 5-field IMRT and 7-field IMRT, in comparison to APPA | Mediastinal radiation holds a very low risk for lung toxicities with APPA showing the lowest estimated risk out of the examined radiation techniques |
| Cutter et al. 2021 [31] | Prediction of 30-year absolute excess risk of radiation-related cardiovascular disease in a post-hoc analysis of the RAPID trial | Cardiovascular morbidity and mortality (cardiac disease and stroke) | Estimated increase in mortality rate per unit dose | Average excess in cardiovascular mortality was predicted to be 0.56% (range 0.01–6.79%), average predicted excess in incidence was 6.24% (range 0.31–31.09%) due to RT | Low predicted risk for most patients. A minority of patients receiving high doses to cardiovascular structures might profit from advanced radiation techniques or omitting RT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oertel, M.; Hölscher, P.; Hering, D.; Kittel, C.; Fuchs, M.; Haverkamp, U.; Borchmann, P.; Eich, H.T. Estimation of Mediastinal Toxicities after Radiotherapy for Hodgkin Lymphoma—A Normal Tissue Complication Analysis of the HD16/17 Trial by the German Hodgkin Study Group. Cancers 2024, 16, 1168. https://doi.org/10.3390/cancers16061168
Oertel M, Hölscher P, Hering D, Kittel C, Fuchs M, Haverkamp U, Borchmann P, Eich HT. Estimation of Mediastinal Toxicities after Radiotherapy for Hodgkin Lymphoma—A Normal Tissue Complication Analysis of the HD16/17 Trial by the German Hodgkin Study Group. Cancers. 2024; 16(6):1168. https://doi.org/10.3390/cancers16061168
Chicago/Turabian StyleOertel, Michael, Priska Hölscher, Dominik Hering, Christopher Kittel, Michael Fuchs, Uwe Haverkamp, Peter Borchmann, and Hans Theodor Eich. 2024. "Estimation of Mediastinal Toxicities after Radiotherapy for Hodgkin Lymphoma—A Normal Tissue Complication Analysis of the HD16/17 Trial by the German Hodgkin Study Group" Cancers 16, no. 6: 1168. https://doi.org/10.3390/cancers16061168
APA StyleOertel, M., Hölscher, P., Hering, D., Kittel, C., Fuchs, M., Haverkamp, U., Borchmann, P., & Eich, H. T. (2024). Estimation of Mediastinal Toxicities after Radiotherapy for Hodgkin Lymphoma—A Normal Tissue Complication Analysis of the HD16/17 Trial by the German Hodgkin Study Group. Cancers, 16(6), 1168. https://doi.org/10.3390/cancers16061168