
Management of Patients with Hypersensitivity to Platinum Salts and Taxane in Gynecological Cancers: A Cross-Sectional Study by the European Network of Young Gynaecologic Oncologists (ENYGO)

 , , ,
, , ,  , , , , , ,
, , , , , ,  , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Variables
2.3. Data Sources/Measurement
2.4. Statistical Analyses
3. Results
3.1. Demographic Data
3.2. HSR and Platinum-Based Chemotherapy
3.3. HSR and Taxane-Based Chemotherapy
3.4. Desensitization of HSRs in Gynecological Cancers
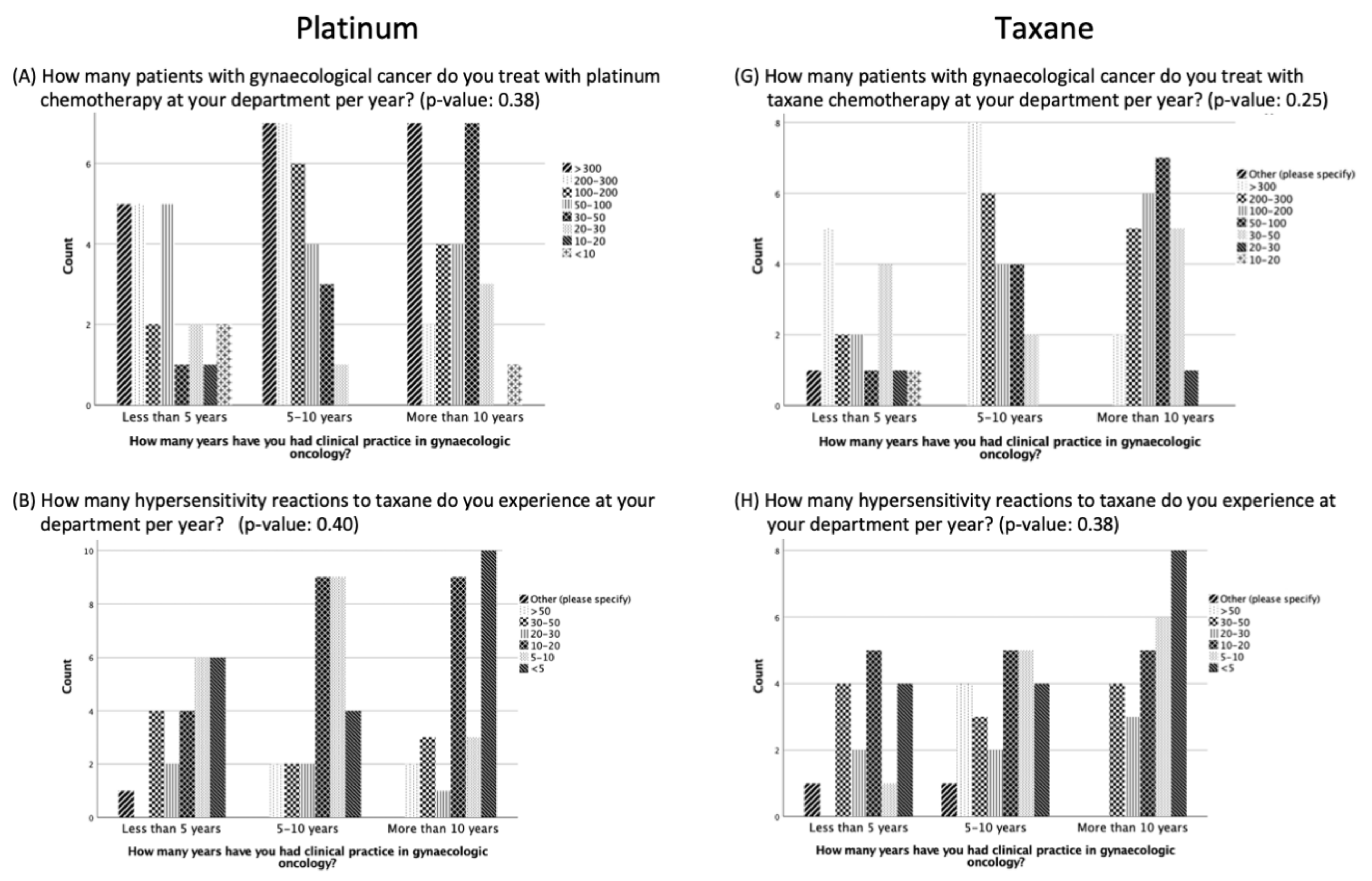
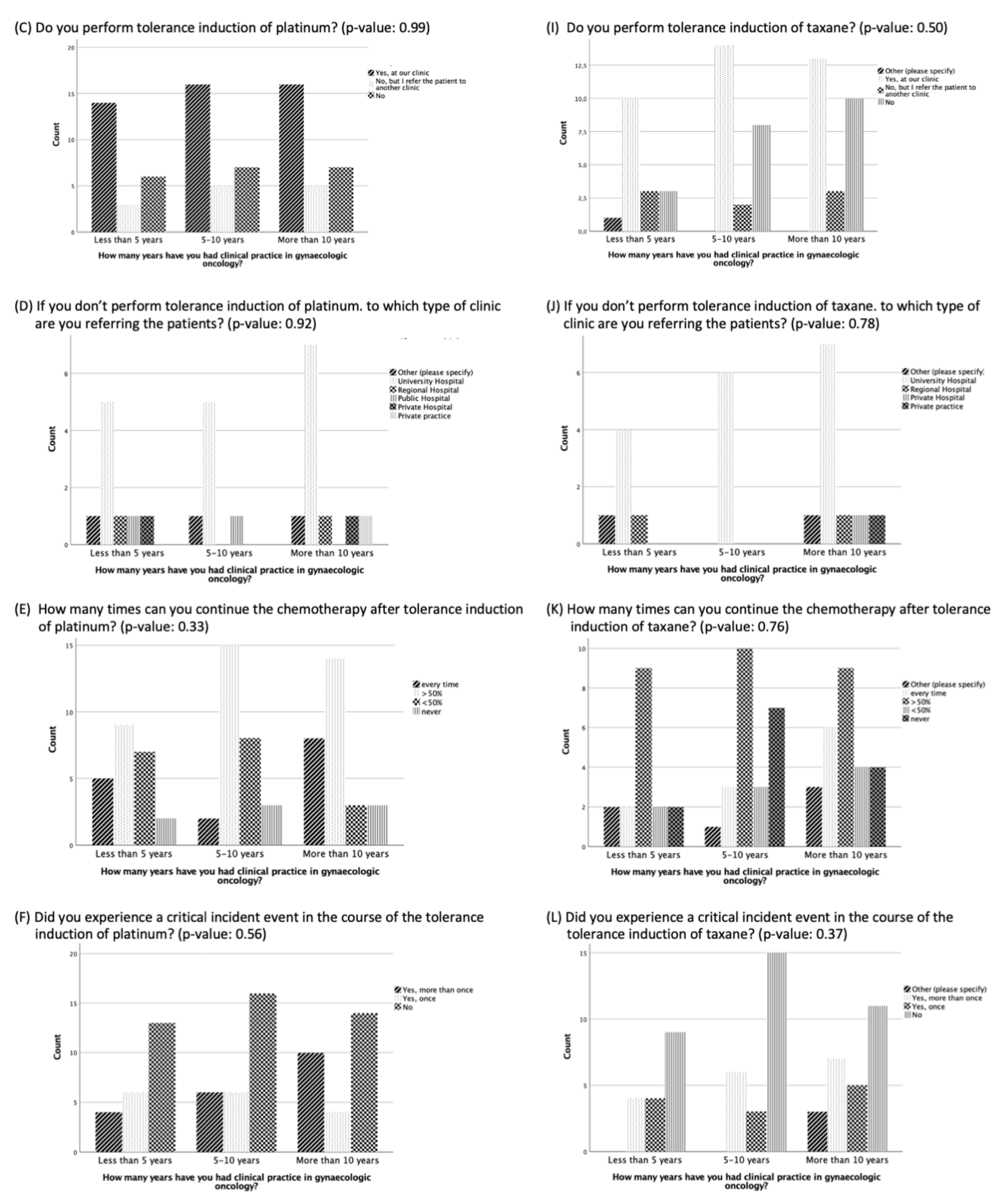
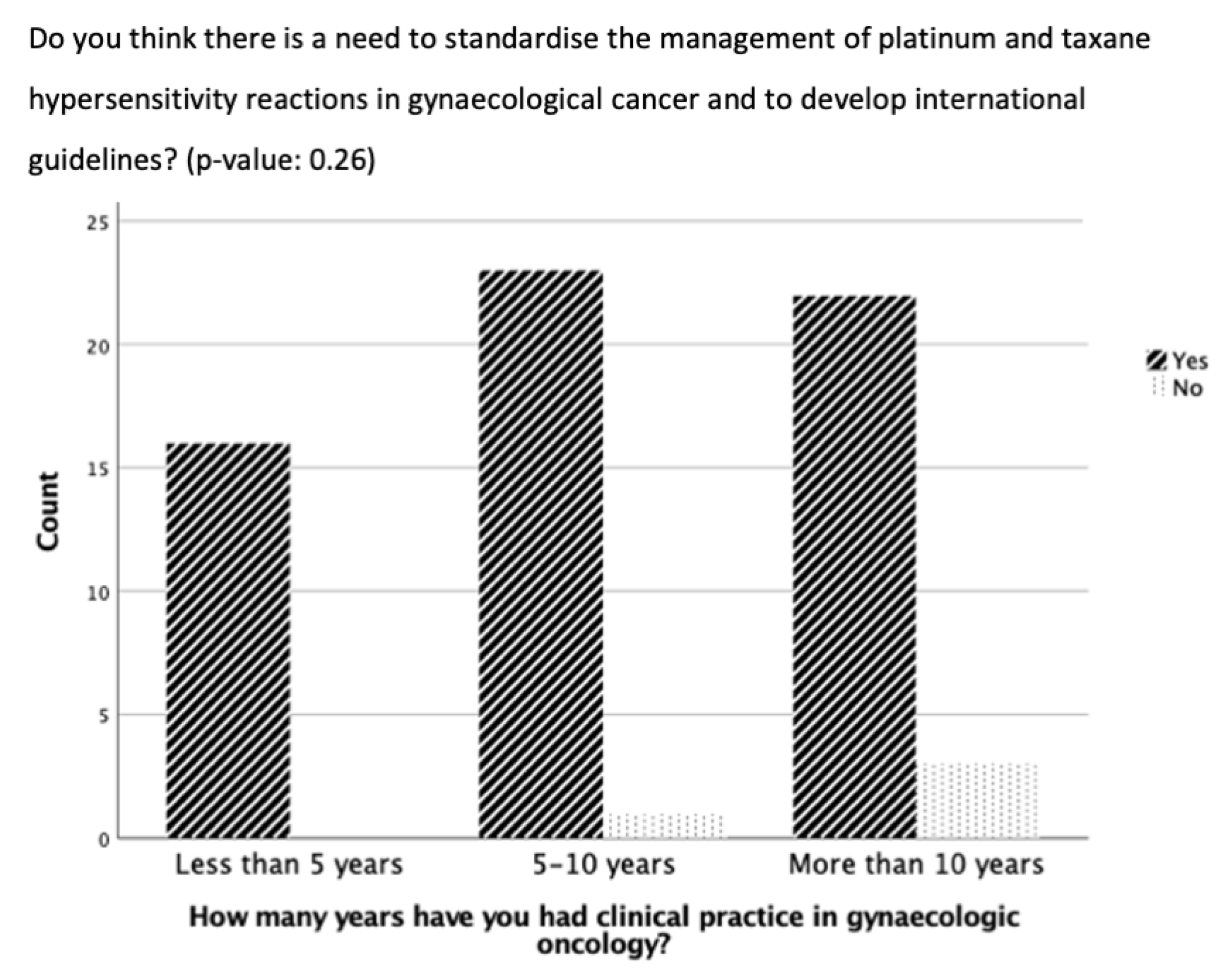
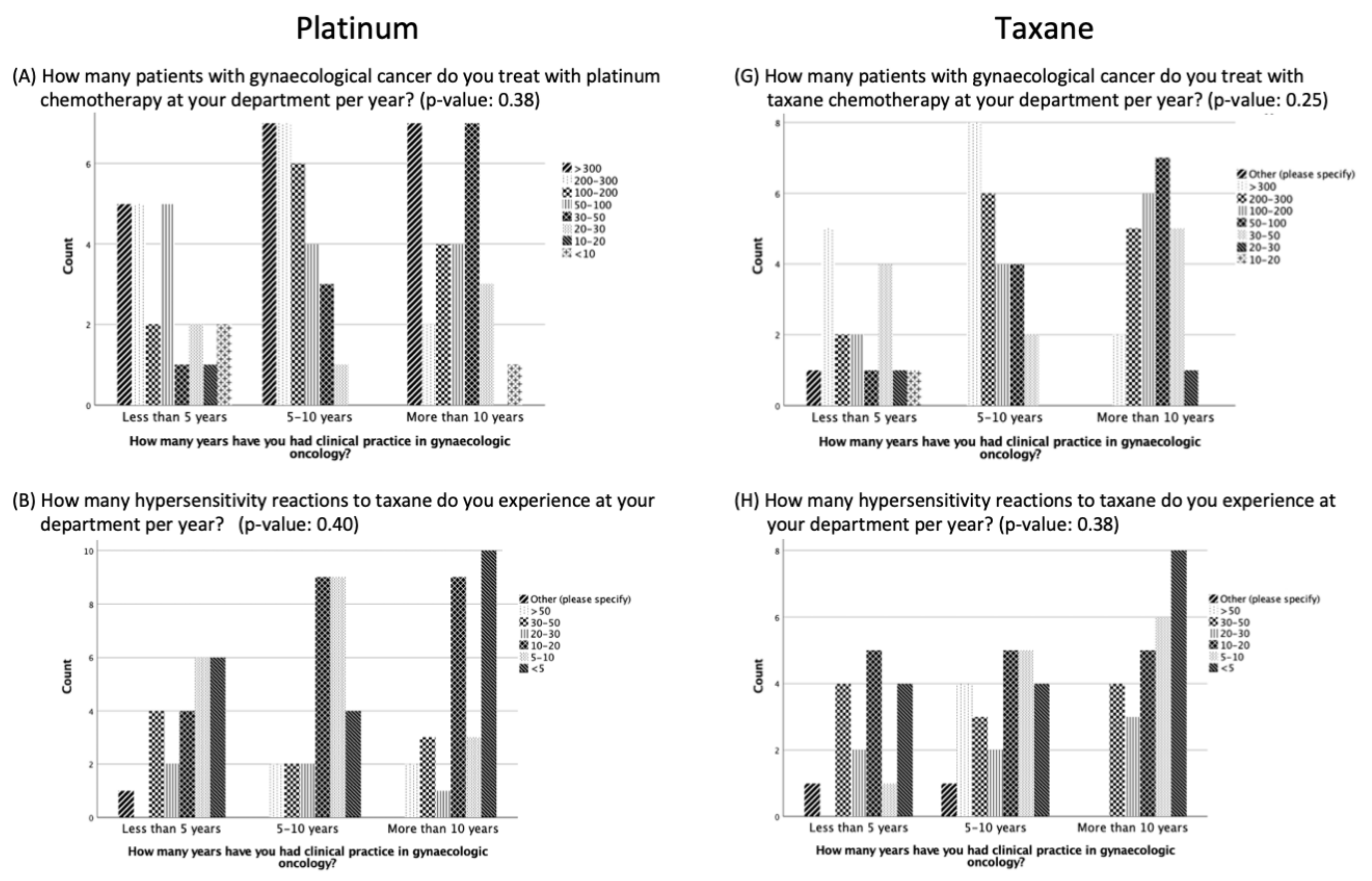
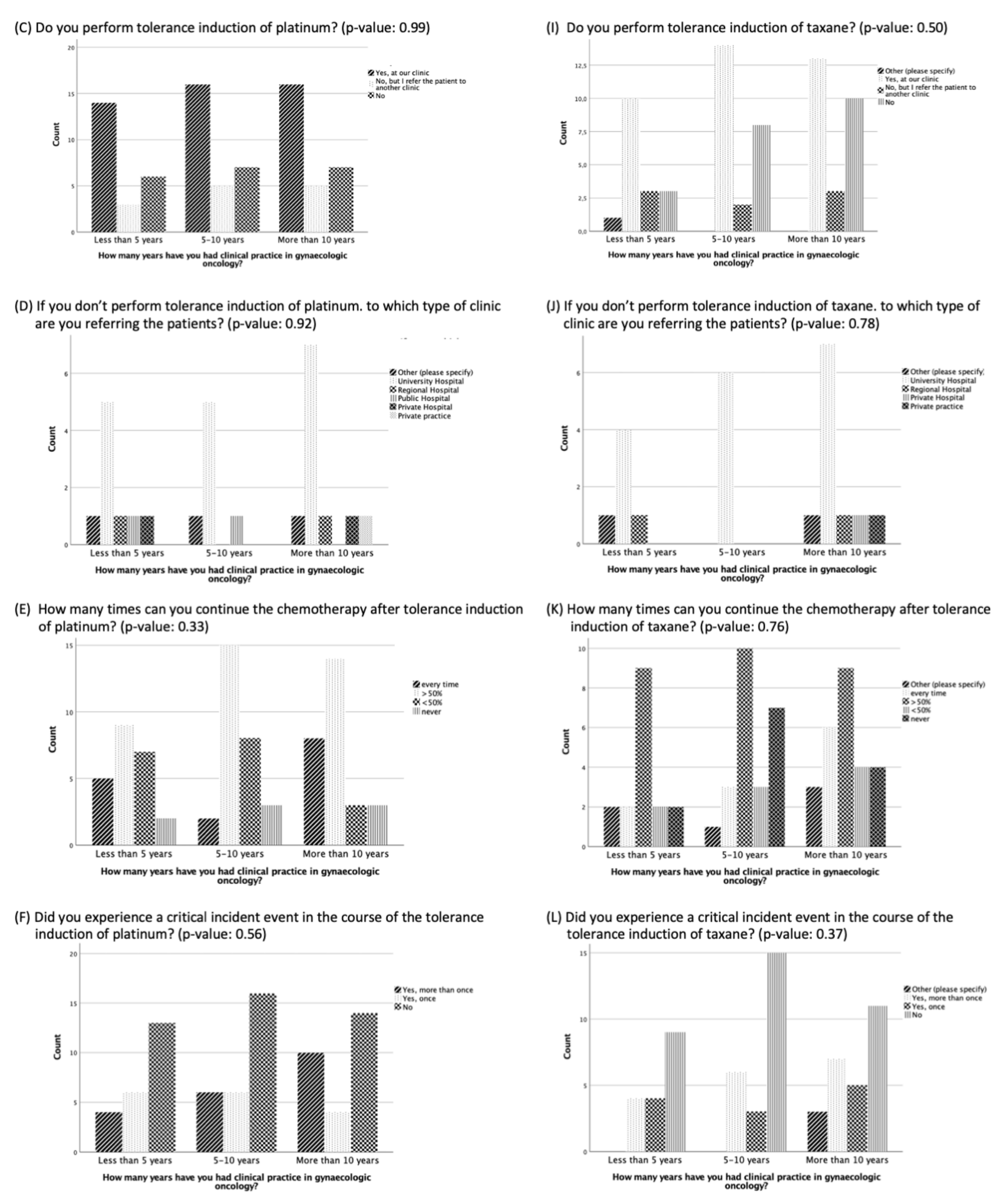
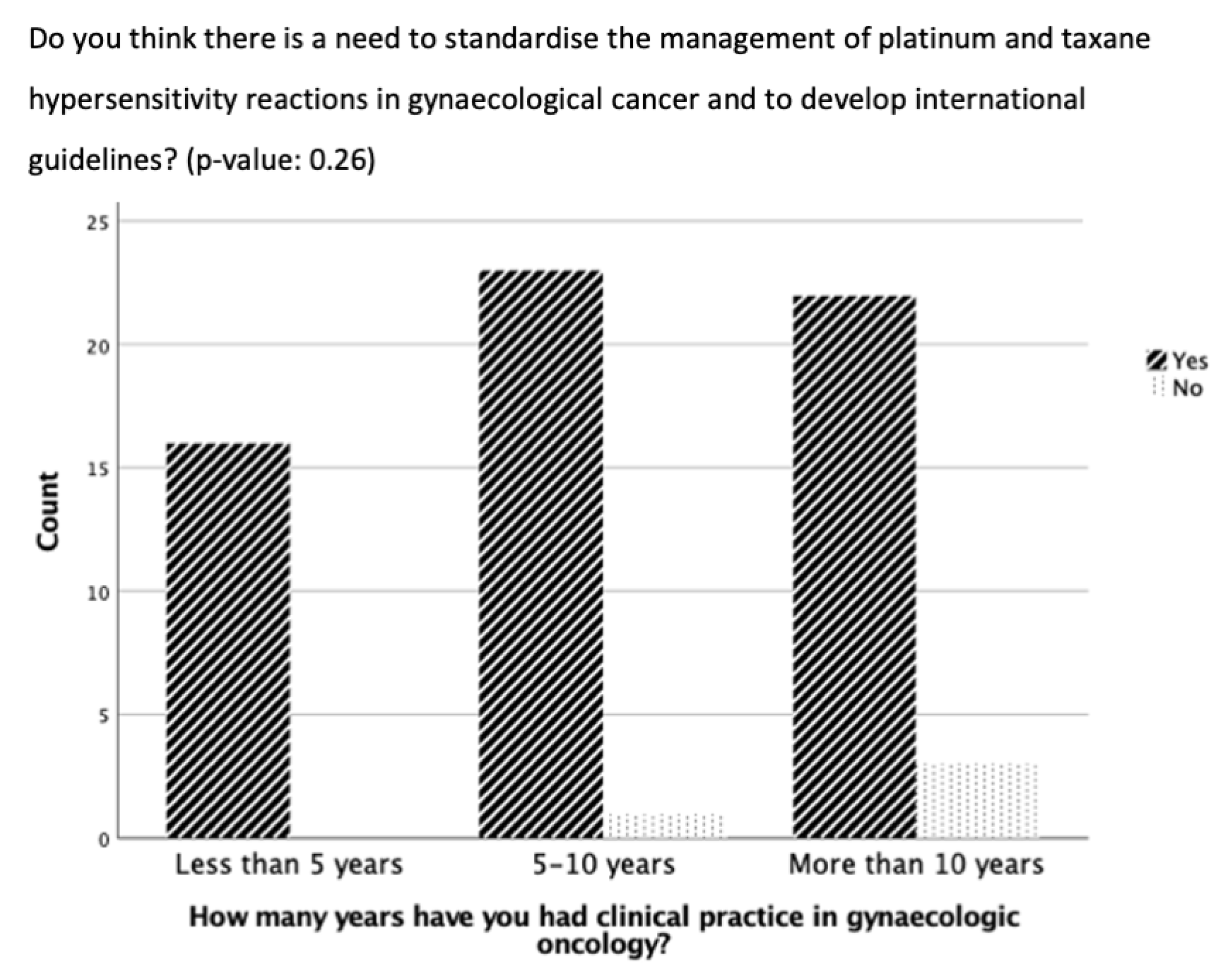
3.5. Management of Hypersensitivity Reactions Based on Length of Clinical Practice Experience
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oaknin, A.; Bosse, T.; Creutzberg, C.; Giornelli, G.; Harter, P.; Joly, F.; Lorusso, D.; Marth, C.; Makker, V.; Mirza, M.; et al. Endometrial cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 860–877. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Matias-Guiu, X.; Amant, F.; Concin, N.; Davidson, B.; Fotopoulou, C.; González-Martin, A.; Gourley, C.; Leary, A.; Lorusso, D.; et al. ESGO-ESMO-ESP consensus conference recommendations on ovarian cancer: Pathology and molecular biology and early, advanced and recurrent disease. Ann. Oncol. 2024, 35, 248–266. [Google Scholar] [CrossRef]
- González-Martín, A.; Harter, P.; Leary, A.; Lorusso, D.; Miller, R.; Pothuri, B.; Ray-Coquard, I.; Tan, D.; Bellet, E.; Oaknin, A.; et al. Newly diagnosed and relapsed epithelial ovarian cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 833–848. [Google Scholar] [CrossRef]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N.; Committee, E.G. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. S4), iv262. [Google Scholar] [CrossRef]
- Falzone, L.; Bordonaro, R.; Libra, M. SnapShot: Cancer chemotherapy. Cell 2023, 186, 1816.e1. [Google Scholar] [CrossRef]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [PubMed]
- Maloney, S.M.; Hoover, C.A.; Morejon-Lasso, L.V.; Prosperi, J.R. Mechanisms of Taxane Resistance. Cancers 2020, 12, 3323. [Google Scholar] [CrossRef]
- Zhang, C.; Xu, C.; Gao, X.; Yao, Q. Platinum-based drugs for cancer therapy and anti-tumor strategies. Theranostics 2022, 12, 2115–2132. [Google Scholar] [CrossRef]
- Castells, M.; Sancho-Serra Mdel, C.; Simarro, M. Hypersensitivity to antineoplastic agents: Mechanisms and treatment with rapid desensitization. Cancer Immunol. Immunother. 2012, 61, 1575–1584. [Google Scholar] [CrossRef]
- O’Malley, D.M.; Vetter, M.H.; Cohn, D.E.; Khan, A.; Hays, J.L. Outpatient desensitization in selected patients with platinum hypersensitivity reactions. Gynecol. Oncol. 2017, 145, 603–610. [Google Scholar] [CrossRef]
- Moon, D.H.; Lee, J.M.; Noonan, A.E.; Annunziata, C.M.; Minasian, L.; Houston, N.; Hays, J.L.; Kohn, E.C. Deleterious BRCA1/2 mutation is an independent risk factor for carboplatin hypersensitivity reactions. Br. J. Cancer 2013, 109, 1072–1078. [Google Scholar] [CrossRef]
- Pagani, M.; Bavbek, S.; Alvarez-Cuesta, E.; Dursun, A.B.; Bonadonna, P.; Castells, M.; Cernadas, J.; Chiriac, A.; Sahar, H.; Madrigal-Burgaleta, R.; et al. Hypersensitivity reactions to chemotherapy: An EAACI Position Paper. Allergy 2022, 77, 388–403. [Google Scholar] [CrossRef] [PubMed]
- Boulanger, J.; Boursiquot, J.N.; Cournoyer, G.; Lemieux, J.; Masse, M.S.; Almanric, K.; Guay, M.P. Management of hypersensitivity to platinum- and taxane-based chemotherapy: Cepo review and clinical recommendations. Curr. Oncol. 2014, 21, e630–e641. [Google Scholar] [CrossRef] [PubMed]
- Pagani, M. The complex clinical picture of presumably allergic side effects to cytostatic drugs: Symptoms, pathomechanism, reexposure, and desensitization. Med. Clin. N. Am. 2010, 94, 835–852, xiii. [Google Scholar] [CrossRef] [PubMed]
- Dizon, D.S.; Sabbatini, P.J.; Aghajanian, C.; Hensley, M.L.; Spriggs, D.R. Analysis of patients with epithelial ovarian cancer or fallopian tube carcinoma retreated with cisplatin after the development of a carboplatin allergy. Gynecol. Oncol. 2002, 84, 378–382. [Google Scholar] [CrossRef]
- Cernadas, J.R.; Brockow, K.; Romano, A.; Aberer, W.; Torres, M.J.; Bircher, A.; Campi, P.; Sanz, M.L.; Castells, M.; Demoly, P.; et al. General considerations on rapid desensitization for drug hypersensitivity—A consensus statement. Allergy 2010, 65, 1357–1366. [Google Scholar] [CrossRef]
- Vetter, M.H.; Khan, A.; Backes, F.J.; Bixel, K.; Cohn, D.E.; Copeland, L.J.; Fowler, J.M.; Salani, R.; Li, Q.; O’Malley, D.M. Outpatient desensitization of patients with moderate (high-risk) to severe platinum hypersensitivity reactions. Gynecol. Oncol. 2019, 152, 316–321. [Google Scholar] [CrossRef]
- Scherer, K.; Brockow, K.; Aberer, W.; Gooi, J.H.C.; Demoly, P.; Romano, A.; Schnyder, B.; Whitaker, P.; Cernadas, J.S.R.; Bircher, A.J.; et al. Desensitization in delayed drug hypersensitivity reactions—An EAACI position paper of the Drug Allergy Interest Group. Allergy 2013, 68, 844–852. [Google Scholar] [CrossRef]
- Zwimpfer, T.A.; Scherer, K.; Schotzau, A.; Heinzelmann-Schwarz, V.; Hartmann, K.; Vetter, M.; Montavon, C. Desensitization in patients with hypersensitivity to platinum and taxane in gynecological cancers. Cancer Med. 2023, 13, e6840. [Google Scholar] [CrossRef]
- Rosello, S.; Blasco, I.; Garcia Fabregat, L.; Cervantes, A.; Jordan, K.; Committee, E.G. Management of infusion reactions to systemic anticancer therapy: ESMO Clinical Practice Guidelines. Ann. Oncol. 2017, 28 (Suppl. S4), iv100–iv118. [Google Scholar] [CrossRef]
- Tsao, L.R.; Young, F.D.; Otani, I.M.; Castells, M.C. Hypersensitivity Reactions to Platinum Agents and Taxanes. Clin. Rev. Allergy Immunol. 2022, 62, 432–448. [Google Scholar] [CrossRef]
- Sloane, D.; Govindarajulu, U.; Harrow-Mortelliti, J.; Barry, W.; Hsu, F.I.; Hong, D.; Laidlaw, T.; Palis, R.; Legere, H.; Bunyavanich, S.; et al. Safety, Costs, and Efficacy of Rapid Drug Desensitizations to Chemotherapy and Monoclonal Antibodies. J. Allergy Clin. Immunol. Pract. 2016, 4, 497–504. [Google Scholar] [CrossRef]
- Koshiba, H.; Hosokawa, K.; Kubo, A.; Miyagi, Y.; Oda, T.; Watanabe, A.; Honjo, H. Incidence of Carboplatin-related hypersensitivity reactions in Japanese patients with gynecologic malignancies. Int. J. Gynecol. Cancer 2009, 19, 460–465. [Google Scholar] [CrossRef]
- Sendo, T.; Sakai, N.; Itoh, Y.; Ikesue, H.; Kobayashi, H.; Hirakawa, T.; Nakano, H.; Oishi, R. Incidence and risk factors for paclitaxel hypersensitivity during ovarian cancer chemotherapy. Cancer Chemother. Pharmacol. 2005, 56, 91–96. [Google Scholar] [CrossRef]
- Kessous, R.; Wissing, M.D.; Laskov, I.; Abitbol, J.; Bitharas, J.; Agnihotram, V.R.; Yasmeen, A.; Salvador, S.; Lau, S.; Gotlieb, W.H. Multiple lines of chemotherapy for patients with high-grade ovarian cancer: Predictors for response and effect on survival. Int. J. Cancer 2021, 148, 2304–2312. [Google Scholar] [CrossRef]
- Shepherd, G.M. Hypersensitivity reactions to chemotherapeutic drugs. Clin. Rev. Allergy Immunol. 2003, 24, 253–262. [Google Scholar] [CrossRef]
- Altwerger, G.; Florsheim, E.B.; Menderes, G.; Black, J.; Schwab, C.; Gressel, G.M.; Nelson, W.K.; Carusillo, N.; Passante, T.; Huang, G.; et al. Impact of carboplatin hypersensitivity and desensitization on patients with recurrent ovarian cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 2449–2456. [Google Scholar] [CrossRef] [PubMed]
- Falzone, L.; Scandurra, G.; Lombardo, V.; Gattuso, G.; Lavoro, A.; Distefano, A.B.; Scibilia, G.; Scollo, P. A multidisciplinary approach remains the best strategy to improve and strengthen the management of ovarian cancer (Review). Int. J. Oncol. 2021, 59, 53. [Google Scholar] [CrossRef] [PubMed]
- Berardi, R.; Morgese, F.; Rinaldi, S.; Torniai, M.; Mentrasti, G.; Scortichini, L.; Giampieri, R. Benefits and Limitations of a Multidisciplinary Approach in Cancer Patient Management. Cancer Manag. Res. 2020, 12, 9363–9374. [Google Scholar] [CrossRef] [PubMed]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef] [PubMed]
- Heudel, P.E.; Devouassoux-Shisheboran, M.; Taieb, S.; Genestie, C.; Selle, F.; Morice, P.; Rouzier, R.; Ray-Coquard, I. Multidisciplinary management of advanced ovarian cancer for an optimal therapeutic strategy. Eur. J. Gynaecol. Oncol. 2017, 38, 175–180. [Google Scholar] [PubMed]
- Bjorn, S.F.; Schnack, T.H.; Lajer, H.; Christensen, I.J.; Lundvall, L.; Thomsen, L.N.; Hogdall, C. Classification of Ovarian Cancer Surgery Facilitates Treatment Decisions in a Gynecological Multidisciplinary Team. Int. J. Gynecol. Cancer 2017, 27, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Moterani, V.C.; Tiezzi, D.G.; de Andrade, J.M.; Candido Dos Reis, F.J. Analysis of the relationship between hospital characteristics and survival in ovarian cancer: A historical cohort. J. Surg. Oncol. 2020, 122, 1802–1807. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.D.; Chen, L.; Hou, J.Y.; Burke, W.M.; Tergas, A.I.; Ananth, C.V.; Neugut, A.I.; Hershman, D.L. Association of Hospital Volume and Quality of Care With Survival for Ovarian Cancer. Obstet. Gynecol. 2017, 130, 545–553. [Google Scholar] [CrossRef]
- Vernooij, F.; Heintz, A.P.; Coebergh, J.W.; Massuger, L.F.; Witteveen, P.O.; van der Graaf, Y. Specialized and high-volume care leads to better outcomes of ovarian cancer treatment in the Netherlands. Gynecol. Oncol. 2009, 112, 455–461. [Google Scholar] [CrossRef]
- Scott, R.; Hawarden, A.; Russell, B.; Edmondson, R.J. Decision-Making in Gynaecological Oncology Multidisciplinary Team Meetings: A Cross-Sectional, Observational Study of Ovarian Cancer Cases. Oncol. Res. Treat. 2020, 43, 70–77. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Number (n = 133, %) |
|---|---|
| Gender | |
| Female | 73 (54.9) |
| Male | 60 (45.1) |
| Age (years) (median, IQR) | 38 (35, 43) |
| Country | |
| Switzerland | 14 (10.5) |
| Italy | 12 (9.0) |
| Germany | 11 (8.3) |
| India | 9 (6.8) |
| Azerbaijan | 8 (6.0) |
| Slovenia | 8 (6.0) |
| Setting * | |
| University Hospital | 76 (57.1) |
| Regional Hospital | 16 (12.0) |
| Public Hospital | 24 (18.0) |
| Private Hospital | 22 (16.5) |
| Private practice | 4 (3.0) |
| Other | 3 (2.3) |
| Specialty | |
| Gynecologic oncologist | 58 (43.6) |
| Gynecologist | 18 (13.5) |
| Medical oncologist | 45 (33.8) |
| Radiation oncologist | 8 (6.0) |
| Other (please specify) | 4 (3.0) |
| Types of gynecological cancer treated * | |
| Ovarian | 123 (92.5) |
| Cervical | 126 (94.7) |
| Vulvar | 104 (78.2) |
| Vaginal | 100 (75.2) |
| Corpus/Endometrium | 114 (85.7) |
| Breast | 62 (46.6) |
| Other | 5 (3.8) |
| Clinical practice in gynecologic oncology | |
| Less than 5 years | 43 (32.3) |
| 5–10 years | 45 (33.8) |
| More than 10 years | 45 (33.8) |
| Involved in chemotherapy treatment | |
| Yes | 103 (77.4) |
| No | 30 (22.6) |
| Questions | Platinum n = 79 (n, %) | Taxane n = 67 (n, %) |
|---|---|---|
| Gynecological cancers treated with platinum/taxane per year | ||
| >300 | 19 (24.1) | 15 (22.4) |
| 200–300 | 14 (17.7) | 13 (19.4) |
| 100–200 | 12 (15.2) | 12 (17.9) |
| 50–100 | 13 (16.5) | 12 (17.9) |
| 30–50 | 11 (13.9) | 11 (16.4) |
| 20–30 | 6 (7.6) | 2 (3.0) |
| 10–20 | 1 (1.3) | 1 (1.5) |
| <10 | 3 (3.8) | 1 (1.5) |
| HSRs to platinum/taxane per year | ||
| >50 | 4 (5.1) | 4 (6.0) |
| 30–50 | 9 (11.4) | 11 (16.4) |
| 20–30 | 5 (6.3) | 7 (10.4) |
| 10–20 | 22 (27.8) | 15 (22.4) |
| 5–10 | 18 (22.8) | 12 (17.9) |
| <5 | 20 (25.3) | 16 (23.9) |
| Other | 1 (1.3) | 2 (3.0) |
| HSRs to platinum/taxane CTCAE Grade 1–2 * | ||
| Premedication with antihistamines/steroids and new attempt with standard infusion | 67 (84.8) | 62 (92.5) |
| Suspension of the chemotherapy | 12 (15.2) | 11 (16.4) |
| Change the chemotherapy to, e.g., Oxaliplatin | 7 (8.9) | 11 (16.4) |
| Tolerance induction (stepwise increase of infusion rate of highly diluted platinum dilution) | 33 (41.8) | 14 (20.9) |
| Other | 3 (3.8) | 2 (2.9) |
| HSR to platinum/taxane CTCAE Grade 3–4 * | ||
| Premedication with antihistamines/steroids and new attempt with standard infusion | 25 (31.6) | 30 (44.8) |
| Suspension of the chemotherapy | 28 (35.4) | 25 (37.3) |
| Change the chemotherapy to, e.g., Oxaliplatin | 27 (34.1) | 30 (44.8) |
| Tolerance induction (stepwise increase of infusion rate of highly diluted platinum dilution) | 39 (49.4) | 28 (41.8) |
| Other | 0 (0.0) | 3 (4.5) |
| Performing tolerance induction of platinum/taxane | ||
| Yes †, at our clinic | 46 (58.2) | 37 (55.2) |
| No, but I referred the patient to another clinic | 13 (16.5) | 8 (11.9) |
| No | 20 (25.3) | 21 (31.3) |
| Other | 0 (0.0) | 1 (1.5) |
| † If yes, who performs the tolerance induction of platinum/taxane * | ||
| Allergologist | 22 (47.8) | 16 (43.2) |
| Medical oncologist | 32 (69.56) | 23 (62.12) |
| Specialist for internal medicine | 2 (4.3) | 0 (0.0) |
| Gynecologic oncologist | 12 (26.1) | 7 (18.9) |
| Other | 5 (10.8) | 4 (10.8) |
| How many times can you continue the chemotherapy after tolerance induction of platinum/taxane | ||
| every time | 15 (19.0) | 11 (16.4) |
| >50% | 38 (48.1) | 28 (41.8) |
| <50% | 18 (22.8) | 9 (13.4) |
| never | 8 (10.1) | 13 (19.4) |
| Other | 0 (0.0) | 6 (9.0) |
| Experience of a critical incident event in the course of the tolerance induction of platinum/taxane | ||
| Yes §, more than once | 20 (25.3) | 17 (25.4) |
| Yes §, once | 16 (20.3) | 12 (17.9) |
| No | 43 (54.4) | 35 (52.2) |
| Other (please specify) | 0 (0.0) | 3 (4.5) |
| § If yes, the reason(s) * | ||
| HSR to platinum/taxane CTCAE Grade 1–2 | 17 (47.2) | 10 (34.5) |
| HSR to platinum/taxane CTCAE Grade 3–4 | 24 (66.7) | 18 (62.1) |
| Death | 2 (5.6) | 1 (3.4) |
| Patient not informed about the risks of tolerance induction | 2 (5.6) | 1 (3.4) |
| Other | 4 (11.1) | 2 (6.9) |
| Question | Not Involved in Chemotherapy Treatment n = 30 (%) | Involved in Chemotherapy Treatment n = 103 (%) |
|---|---|---|
| Aware of the possibility of desensitization of patients with HSRs to platinum/taxane prior to this survey | ||
| Yes | 12 (40.0) | 57 (55.3) |
| No | 16 (53.3) | 7 (6.8) |
| Other | 0 (0) | 2 (1.9) |
| No answer | 2 (2.7) | 37 (35.9) |
| A need to standardize the management of platinum and taxane HSRs in gynecological cancer and to develop international guidelines? | ||
| Yes | 25 (83.3) | 61 (59.2) |
| No | 2 (6.7) | 4 (3.9) |
| No answer | 3 (10.0) | 38 (36.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwimpfer, T.A.; Bilir, E.; Gasimli, K.; Cokan, A.; Bizzarri, N.; Razumova, Z.; Kacperczyk-Bartnik, J.; Nikolova, T.; Pletnev, A.; Kahramanoglu, I.; et al. Management of Patients with Hypersensitivity to Platinum Salts and Taxane in Gynecological Cancers: A Cross-Sectional Study by the European Network of Young Gynaecologic Oncologists (ENYGO). Cancers 2024, 16, 1155. https://doi.org/10.3390/cancers16061155
Zwimpfer TA, Bilir E, Gasimli K, Cokan A, Bizzarri N, Razumova Z, Kacperczyk-Bartnik J, Nikolova T, Pletnev A, Kahramanoglu I, et al. Management of Patients with Hypersensitivity to Platinum Salts and Taxane in Gynecological Cancers: A Cross-Sectional Study by the European Network of Young Gynaecologic Oncologists (ENYGO). Cancers. 2024; 16(6):1155. https://doi.org/10.3390/cancers16061155
Chicago/Turabian StyleZwimpfer, Tibor A., Esra Bilir, Khayal Gasimli, Andrej Cokan, Nicolò Bizzarri, Zoia Razumova, Joanna Kacperczyk-Bartnik, Tanja Nikolova, Andrei Pletnev, Ilker Kahramanoglu, and et al. 2024. "Management of Patients with Hypersensitivity to Platinum Salts and Taxane in Gynecological Cancers: A Cross-Sectional Study by the European Network of Young Gynaecologic Oncologists (ENYGO)" Cancers 16, no. 6: 1155. https://doi.org/10.3390/cancers16061155
APA StyleZwimpfer, T. A., Bilir, E., Gasimli, K., Cokan, A., Bizzarri, N., Razumova, Z., Kacperczyk-Bartnik, J., Nikolova, T., Pletnev, A., Kahramanoglu, I., Shushkevich, A., Strojna, A., Theofanakis, C., Cicakova, T., Vetter, M., Montavon, C., Morgan, G., & Heinzelmann-Schwarz, V. (2024). Management of Patients with Hypersensitivity to Platinum Salts and Taxane in Gynecological Cancers: A Cross-Sectional Study by the European Network of Young Gynaecologic Oncologists (ENYGO). Cancers, 16(6), 1155. https://doi.org/10.3390/cancers16061155