

Intraoperative Techniques That Define the Mucosal Margins of Oral Cancer In-Vivo: A Systematic Review


 and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Data Extraction
2.4. Critical Appraisal
3. Results
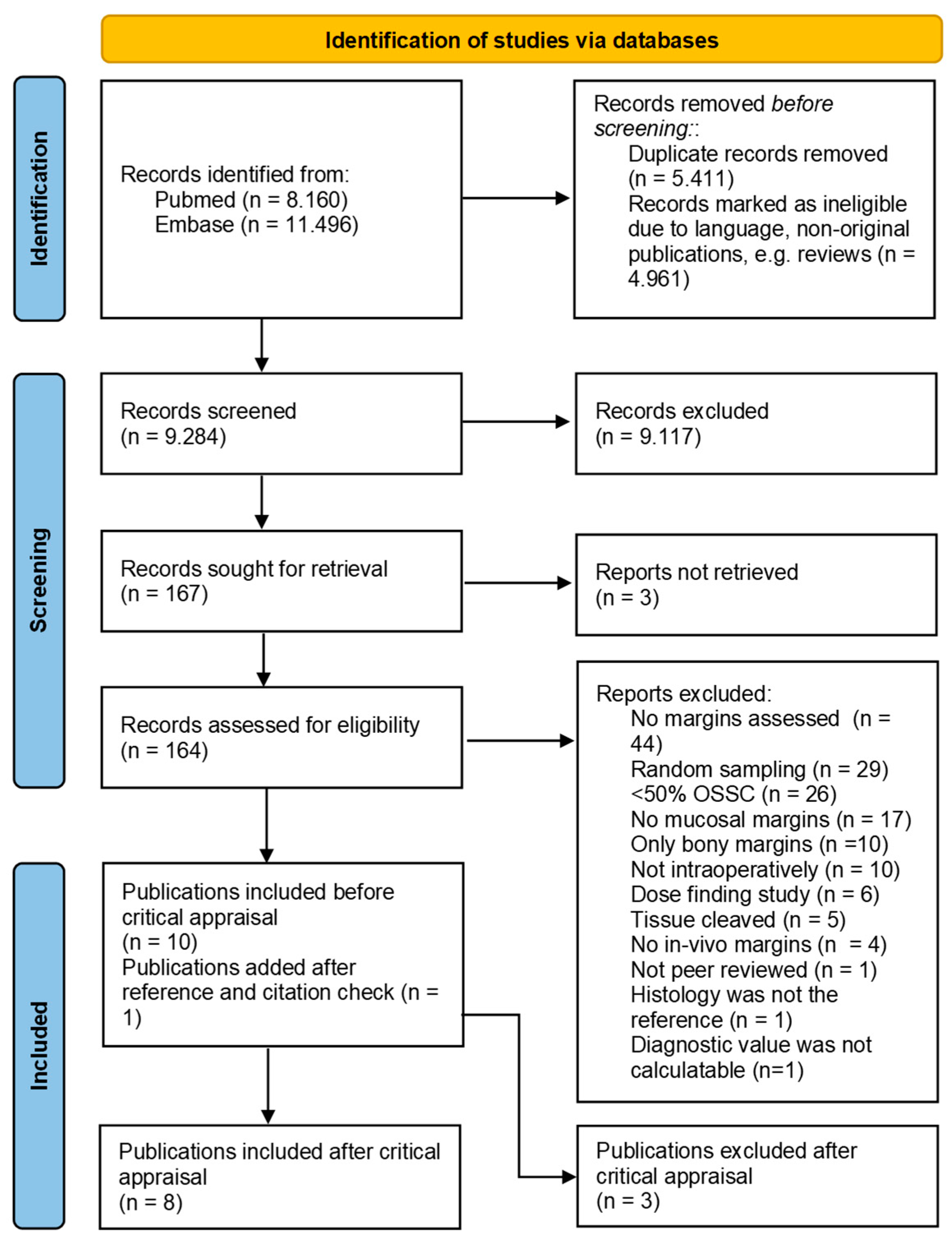
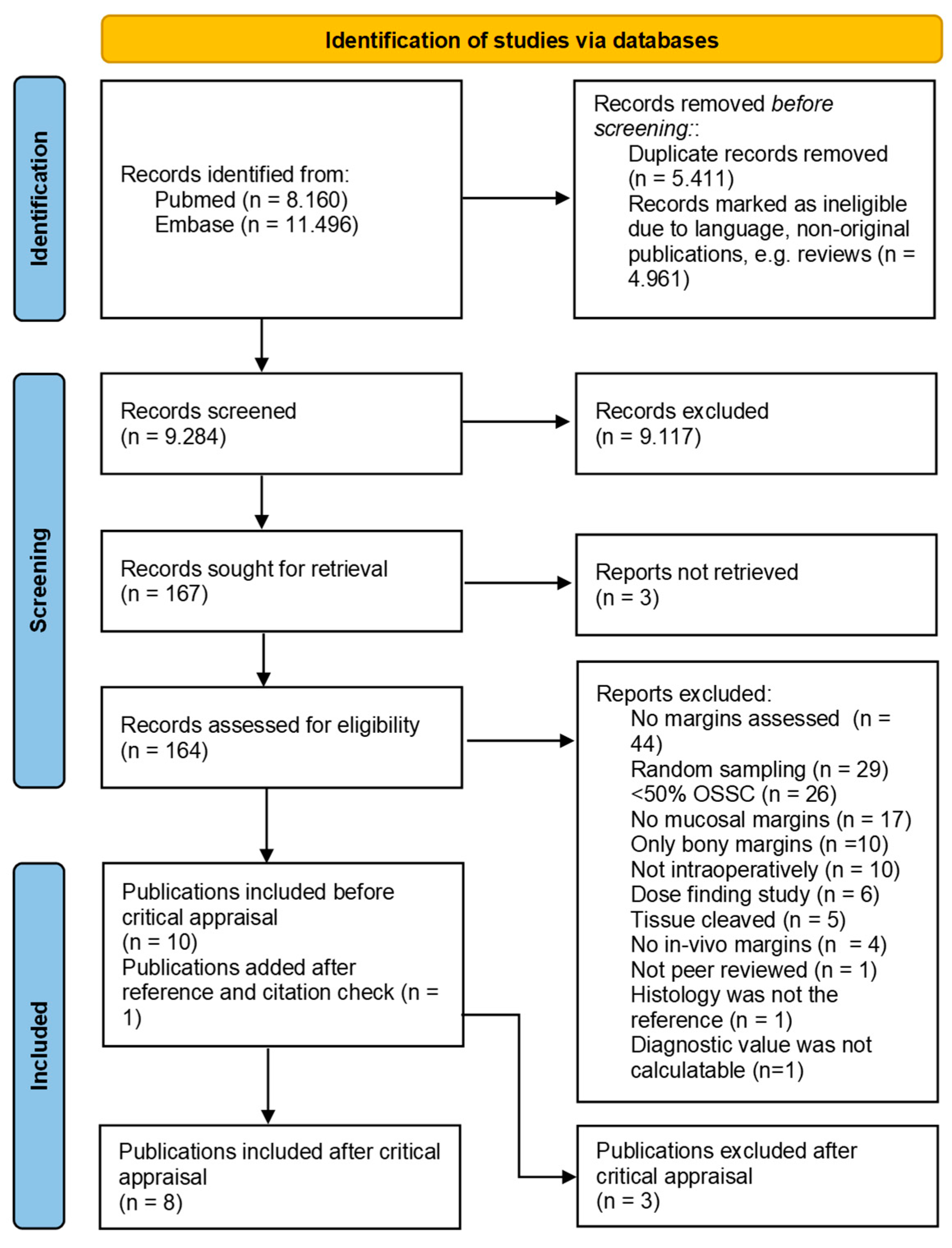
3.1. Search Strategy and Article Selection
3.2. Critical Appraisal
3.3. Margin Visualization Techniques
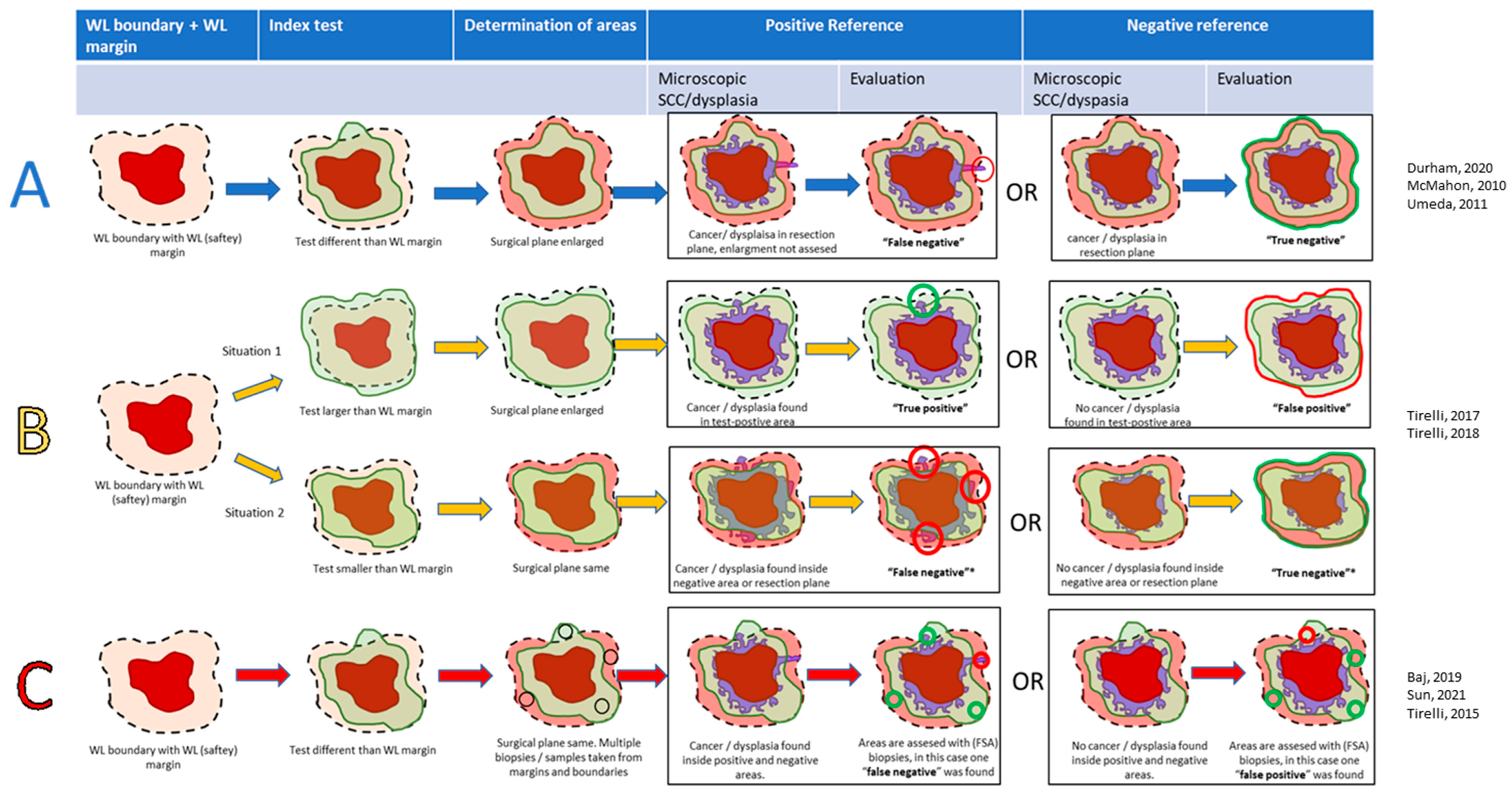
- Method A: Interventional studies (with or without a WL-safety margin control group). Surgical margins were enlarged when the index-positive area exceeded the WL-safety margin. SCC and/or dysplasia determined the TN or FN in the index-negative areas surrounding the index-positive areas. Index-positive areas were not analyzed; hence, only the NPV could be calculated. Three studies used this methodology [36,38,39].
- Method B: Interventional studies with diagnostic accuracy. In these studies, the index test was either smaller or larger than the WL-safety margin, and a specimen was either considered index test negative (index ≤ WL) or positive (index > WL). Tumors were excised according to the largest area. Histopathology determined the diagnostic accuracy in these areas. In contrast to Method A, the TP and FP could also be evaluated. In case the index-positive area was as large as the WL-safety margin, the case was considered negative. Two studies used this methodology [41,42].
- Method C: Diagnostic accuracy studies. In these studies, all tumors were excised according to the WL-safety margin. Index-positive areas extending beyond the WL-safety margin were sampled and assessed on the TP or FP. Areas not extending further than the WL-safety margin were also sampled, indicating either the TN or FN. The overlap between the WL-safety margin and positive index test was considered a plausible situation, in contrast to ‘Method C’. Three studies used this methodology [33,34,40].
3.3.1. Autofluorescence
3.3.2. Iodine Staining
3.3.3. Narrow Band Imaging
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The Global Burden of Cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef]
- Chinn, S.B.; Myers, J.N. Oral cavity carcinoma: Current management, controversies, and future directions. Am. Soc. Clin. Oncol. 2015, 33, 3269–3276. [Google Scholar] [CrossRef]
- Daniell, J.; Udovicich, C.; Rowe, D.; McDowell, L.; Vital, D.; Bressel, M.; Magarey, M.; Iseli, T.; Wong, T.; Lekgabe, E.; et al. Impact of histological Oral Tongue Cancer margins on locoregional recurrence: A multi-centre retrospective analysis. Oral Oncol. 2020, 111, 105004. [Google Scholar] [CrossRef]
- Lee, D.Y.; Kang, S.H.; Kim, J.H.; Kim, M.; Oh, K.H.; Woo, J.; Kwon, S.; Jung, K.; Baek, S. Survival and recurrence of resectable tongue cancer: Resection margin cutoff value by T classification. Head Neck 2018, 40, 283–291. [Google Scholar] [CrossRef]
- Brinkman, D.; Callanan, D.; O’Shea, R.; Jawad, H.; Feeley, L.; Sheahan, P. Impact of 3 mm margin on risk of recurrence and survival in oral cancer. Oral Oncol. 2020, 110, 104883. [Google Scholar] [CrossRef]
- Singh, A.; Mishra, A.; Singhvi, H.; Sharin, F.; Bal, M.; Laskar, S.; Prabhash, K.; Chaturvedi, P. Optimum surgical margins in squamous cell carcinoma of the oral tongue: Is the current definition adequate? Oral Oncol. 2020, 111, 10948. [Google Scholar] [CrossRef] [PubMed]
- Bajwa, M.S.; Houghton, D.; Java, K.; Triantafyllou, A.; Khattak, O.; Bekiroglu, F.; Schache, A.G.; Brown, J.S.; McCaul, J.A.; Rogers, S.N.; et al. The relevance of surgical margins in clinically early oral squamous cell carcinoma. Oral Oncol. 2020, 110, 104913. [Google Scholar] [CrossRef] [PubMed]
- Dik, E.A.; Willems, S.M.; Ipenburg, N.A.; Adriaansens, S.O.; Rosenberg, A.J.W.P.; Van Es, R.J.J. Resection of early oral squamous cell carcinoma with positive or close margins: Relevance of adjuvant treatment in relation to local recurrence: Margins of 3 mm as safe as 5 mm. Oral Oncol. 2014, 50, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Haddad, R.; Hicks, W.; Hitchcock, Y.; Jimeno, A.; Leizman, D.; Pinto, H.; Rocco, J.; Rodriguez, C.; Schwartz, D.; Shah, J.; et al. NCCN Guidelines Version 2.2023 Head and Neck Cancers. 2023. Available online: https://www.nccn.org/home/member- (accessed on 2 February 2023).
- Helliwell, T.; Woolgar, J. Standards and Datasets for Reporting Cancers. 2013. Available online: www.nice.org.uk/accreditation (accessed on 2 February 2023).
- Varvares, M.A.; Poti, S.; Kenyon, B.; Christopher, K.; Walker, R.J. Surgical margins and primary site resection in achieving local control in oral cancer resections. Laryngoscope 2015, 125, 2298–2307. [Google Scholar] [CrossRef]
- Ettl, T.; El-Gindi, A.; Hautmann, M.; Gosau, M.; Weber, F.; Rohrmeier, C.; Gerken, M.; Müller, S.; Reichert, T.; Klingelhöffer, C. Positive frozen section margins predict local recurrence in R0-resected squamous cell carcinoma of the head and neck. Oral Oncol. 2016, 55, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Jehn, P.; Stier, R.; Tavassol, F.; Dittmann, J.; Zimmerer, R.; Gellrich, N.; Krüskemper, G. Spalthoff SPhysical and Psychological Impairments Associated with Mucositis after Oral Cancer Treatment and Their Impact on Quality of Life. Oncol Res. Treat. 2019, 42, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Kubik, M.; Sridharan, S.; Varvares, M.; Zandberg, D.; Skinner, H.; Seethala, R.; Chiosea, S. Intraoperative Margin Assessment in Head and Neck Cancer: A Case of Misuse and Abuse? Head Neck Pathol. 2020, 14, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, D.P.; Southwick, H.W.; Smejkal, W. “Field cancerization” in oral stratified squamous epithelium. Clinical implications of multicentric origin. Cancer 1953, 6, 963–968. [Google Scholar] [CrossRef]
- Gokavarapu, S.; Parvataneni, N.; Pavagada, S.; Rao, L.C.; Raju, K.; Rao, T.S. Mild to moderate dysplasia at surgical margin is a significant indicator of survival in patients with oral cancer. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 330–337. [Google Scholar] [CrossRef]
- Singh, A.; Mair, M.; Singhvi, H.; Ramalingam, N.; Bal, M.; Lamba, K.; Nair, D.; Nair, S.; Chaturvedi, P. Incidence and impact of dysplasia at final resection margins in cancers of the oral cavity. Acta Oto-Laryngol. 2020, 140, 963–969. [Google Scholar] [CrossRef]
- Mogedas-Vegara, A.; Hueto-Madrid, J.-A.; Chimenos-Küstner, E.; Bescós-Atín, C. Oral leukoplakia treatment with the carbon dioxide laser: A systematic review of the literature. J. Cranio-Maxillofac. Surg. 2016, 44, 331–336. [Google Scholar] [CrossRef]
- Smits, R.W.H.; Koljenović, S.; Hardillo, J.A.; Hove, I.T.; Meeuwis, C.A.; Sewnaik, A.; Dronkers, E.A.; Schut, T.C.B.; Langeveld, T.P.M.; Molenaar, J.; et al. Resection margins in oral cancer surgery: Room for improvement. Head Neck 2016, 38 (Suppl. S1), E2197–E2203. [Google Scholar] [CrossRef] [PubMed]
- DiNardo, L.J.; Lin, J.; Karageorge, L.S.; Powers, C.N. Accuracy, Utility, and Cost of Frozen Section Margins in Head and Neck Cancer Surgery. Laryngoscope 2000, 110, 1773–1776. [Google Scholar] [CrossRef]
- Bulbul, M.G.; Tarabichi, O.; Sethi, R.K.; Parikh, A.S.; Varvares, M.A. Does Clearance of Positive Margins Improve Local Control in Oral Cavity Cancer? A Meta-analysis. Otolaryngol. Head Neck Surg. 2019, 161, 235–244. [Google Scholar] [CrossRef]
- de Koning, K.J.; van Es, R.J.; Klijn, R.J.; Breimer, G.E.; Dankbaar, J.W.; Braunius, W.W.; van Cann, E.M.; Dieleman, F.J.; Rijken, J.A.; Tijink, B.M.; et al. Application and accuracy of ultrasound-guided resections of tongue cancer. Oral Oncol. 2022, 133, 106023. [Google Scholar] [CrossRef]
- Adriaansens, C.M.E.M.; de Koning, K.J.; de Bree, R.; Dankbaar, J.W.; Breimer, G.E.; van Es, R.J.J.; Noorlag, R. Ultrasound-guided resection for squamous cell carcinoma of the buccal mucosa: A feasibility study. Head Neck 2023, 45, 647–657. [Google Scholar] [CrossRef]
- Heidkamp, J.; Weijs, W.L.J.; Grunsven, A.C.H.v.E.; Vries, I.d.L.; Maas, M.C.; Rovers, M.M.; Fütterer, J.J.; Steens, S.C.A.; Takes, R.P. Assessment of surgical tumor-free resection margins in fresh squamous-cell carcinoma resection specimens of the tongue using a clinical MRI system. Head Neck 2020, 42, 2039–2049. [Google Scholar] [CrossRef] [PubMed]
- Brouwer de Koning, S.G.; Schaeffers, A.W.M.A.; Schats, W.; van den Brekel, M.W.M.; Ruers, T.J.M.; Karakullukcu, M.B. As-sessment of the deep resection margin during oral cancer surgery: A systematic review. Eur. J. Surg. Oncol. 2021, 47, 2220–2232. [Google Scholar] [CrossRef]
- Kain, J.J.; Birkeland, A.C.; Udayakumar, N.; Morlandt, A.B.; Stevens, T.M.; Carroll, W.R.; Rosenthal, E.L.; Warram, J.M. Surgical margins in oral cavity squamous cell carcinoma: Current practices and future directions. Laryngoscope 2020, 130, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Young, K.; Ma, E.; Kejriwal, S.; Nielsen, T.; Aulakh, S.S.; Birkeland, A.C. Intraoperative In Vivo Imaging Modalities in Head and Neck Cancer Surgical Margin Delineation: A Systematic Review. Cancers 2022, 14, 3416. [Google Scholar] [CrossRef]
- Carnicelli, G.; Disconzi, L.; Cerasuolo, M.; Casiraghi, E.; Costa, G.; De Virgilio, A.; Esposito, A.A.; Ferreli, F.; Fici, F.; Casto, A.L.; et al. Image-Guided Intraoperative Assessment of Surgical Margins in Oral Cavity Squamous Cell Cancer: A Diagnostic Test Accuracy Review. Diagnostics 2023, 13, 1846. [Google Scholar] [CrossRef]
- de Koning, S.G.B.; Karakullukcu, M.B.; Lange, C.A.; Ruers, T.J. The oral cavity tumor thickness: Measurement accuracy and consequences for tumor staging. Eur. J. Surg. Oncol. 2019, 45, 2131–2136. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Bramer, W.M.; Giustini, D.; De Jong, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in endnote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef]
- Whiting, P.; Rutjes, A.; Westwood, M.; Mallett, S.; Deeks, J.; Reitsma, J.; Leeflang, M.; Sterne, J.; Bossuyt, M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. 2011. Available online: https://annals.org (accessed on 1 September 2023).
- Baj, A.; Fusco, N.; Bolzoni, A.; Carioli, D.; Mazzucato, C.; Faversani, A.; Bresciani, L.; Maggioni, M.; Capaccio, P. A novel inte-grated platform for the identification of surgical margins in oral squamous cell carcinoma: Results from a prospective single-institution series. BMC Cancer 2019, 19, 467. [Google Scholar] [CrossRef]
- Sun, L.-F.; Wang, C.-X.; Cao, Z.-Y.; Han, W.; Guo, S.-S.; Wang, Y.-Z.; Meng, Y.; Hou, C.-X.; Zhu, Q.-H.; Tang, Y.-T.; et al. Evaluation of autofluorescence visualization system in the delineation of oral squamous cell carcinoma surgical margins. Photodiagnosis Photodyn. Ther. 2021, 36, 102487. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, T.; Bessho, H.; Nomura, T.; Kozakai, A.; Kosugi, A.; Shibahara, T. Setting of the surgical margin using optical in-strument for treatment of early tongue squamous cell carcinoma. J. Oral Maxillofac. Surg. Med. Pathol. 2019, 31, 8–12. [Google Scholar] [CrossRef]
- Durham, J.; Brasher, P.; Anderson, D.; Yoo, J.; Hart, R.; Dort, J.; Seikaly, H.; Kerr, P.; Rosin, M.; Poh, C. Effect of Fluorescence Visualization-Guided Surgery on Local Recurrence of Oral Squamous Cell Carcinoma: A Randomized Clinical Trial. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, T.; Shibahara, T.; Takano, M. Combination of fluorescence visualization and iodine solution-guided surgery for local control of early tongue cancer. Int. J. Oral Maxillofac. Surg. 2023, 52, 161–167. [Google Scholar] [CrossRef] [PubMed]
- McMahon, J.; Devine, J.C.; McCaul, J.A.; McLellan, D.R.; Farrow, A. Use of Lugol’s iodine in the resection of oral and oropha-ryngeal squamous cell carcinoma. Br. J. Oral Maxillofac. Surg. 2010, 48, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Umeda, M.; Shigeta, T.; Takahashi, H.; Minamikawa, T.; Komatsubara, H.; Oguni, A.; Shibuya, Y.; Komori, T. Clinical evaluation of Lugol’s iodine staining in the treatment of stage I–II squamous cell carcinoma of the tongue. Int. J. Oral Maxillofac. Surg. 2011, 40, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Tirelli, G.; Piovesana, M.; Gatto, A.; Tofanelli, M.; Biasotto, M.; Nata, F.B. Narrow band imaging in the intra-operative definition of resection margins in oral cavity and oropharyngeal cancer. Oral Oncol. 2015, 51, 908–913. [Google Scholar] [CrossRef]
- Tirelli, G.; Piovesana, M.; Gatto, A.; Torelli, L.; Di Lenarda, R.; Nata, F.B. NBI utility in the pre-operative and intra-operative assessment of oral cavity and oropharyngeal carcinoma. Am. J. Otolaryngol. 2017, 38, 65–71. [Google Scholar] [CrossRef]
- Tirelli, G.; Piovesana, M.; Marcuzzo, A.V.; Gatto, A.; Biasotto, M.; Bussani, R.; Zandonà, L.; Giudici, F.; Nata, F.B. Tailored resections in oral and oropharyngeal cancer using narrow band imaging. Am. J. Otolaryngol. 2018, 39, 197–203. [Google Scholar] [CrossRef]
- Tirelli, G.; Nata, F.B.; Gatto, A.; Bussani, R.; Spinato, G.; Zacchigna, S.; Piovesana, M. Intraoperative Margin Control in Transoral Approach for Oral and Oropharyngeal Cancer. Laryngoscope 2019, 129, 1810–1815. [Google Scholar] [CrossRef]
- Lane, P.M.; Gilhuly, T.; Whitehead, P.; Zeng, H.; Poh, C.F.; Ng, S.; Williams, P.M.; Zhang, L.; Rosin, M.P.; MacAulay, C.E. Simple device for the direct visualization of oral-cavity tissue fluorescence. J. Biomed. Opt. 2006, 11, 024006. [Google Scholar] [CrossRef]
- Yang, Z.-H.; Chen, W.-L.; Huang, H.-Z.; Pan, C.-B.; Li, J.-S. Quality of Life of Patients With Tongue Cancer 1 Year After Surgery. J. Oral Maxillofac. Surg. 2010, 68, 2164–2168. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, F.; Abbaci, M.; Casiraghi, O.; Ben Lakhdar, A.; Alfaro, A.; Breuskin, I.; Laplace-Builhé, C. Value of Full-Field Optical Coherence Tomography Imaging for the Histological Assessment of Head and Neck Cancer. Lasers Surg. Med. 2020, 52, 768–778. [Google Scholar] [CrossRef] [PubMed]
- Hamdoon, Z.; Jerjes, W.; McKenzie, G.; Jay, A.; Hopper, C. Optical coherence tomography in the assessment of oral squamous cell carcinoma resection margins. Photodiagnosis Photodyn. Ther. 2016, 13, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Sunny, S.P.; Agarwal, S.; James, B.L.; Heidari, E.; Muralidharan, A.; Yadav, V.; Pillai, V.; Shetty, V.; Chen, Z.; Hedne, N.; et al. Intra-operative point-of-procedure delineation of oral cancer margins using optical coherence tomography. Oral Oncol. 2019, 92, 12–19. [Google Scholar] [CrossRef]
- De Wit, J.; Vonk, J.; Voskuil, F.; de Visscher, S.; Schepman, K.; Hooghiemstra, W.; Linssen, M.; Elias, S.; Halmos, G.; Plaat, B.; et al. EGFR-targeted fluorescence molecular imaging for in-traoperative margin assessment in oral cancer patients: A phase II trial. Nat. Commun. 2023, 14, 4952. [Google Scholar] [CrossRef]
- Van Keulen, S.; Nishio, N.; Birkeland, A.; Fakurnejad, S.; Martin, B.; Forouzanfar, T.; Cunanan, K.; Colevas, A.; Van Den Berg, N.; Rosenthal, E. The sentinel margin: Intraoperative ex vivo specimen mapping using relative fluorescence intensity. Clin. Cancer Res. 2019, 25, 4656–4662. [Google Scholar] [CrossRef]
- Junaid, M.; Choudhary, M.M.; A Sobani, Z.; Murtaza, G.; Qadeer, S.; Ali, N.S.; Khan, M.J.; Suhail, A. A comparative analysis of toluidine blue with frozen section in oral squamous cell carcinoma. World J. Surg. Oncol. 2012, 10, 57. [Google Scholar] [CrossRef]
- Algadi, H.H.; Abou-Bakr, A.A.-E.; Jamali, O.M.; Fathy, L.M. Toluidine blue versus frozen section for assessment of mucosal tumor margins in oral squamous cell carcinoma. BMC Cancer 2020, 20, 1147. [Google Scholar] [CrossRef]
- Kerawala, C.J.; Beale, V.; Reed, M.; Martin, C. The role of vital tissue staining the marginal control of oral squamous cell carcinoma Oncology. Int. J. Oral Maxillofac. Surg. 2000, 29, 32–35. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Risk of Bias | Applicability | ||||||
|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference | Flow and Timing | Patient Selection | Index Test | Reference | |
| Morikawa, 2019 [35] |  |  | | | | |  |
| Durham, 2020 [36] | | | | | | | |
| Sun, 2021 [34] | | | | | | | |
| Morikawa, 2023 [37] | | | | | | | |
| McMahon, 2010 [38] | | | | | | | |
| Umeda, 2011 [39] | | | | | | | |
| Tirelli, 2015 [40] | | | | | | | |
| Tirelli, 2017 [41] | | | | | | | |
| Tirelli, 2018 [42] | | | | | | | |
| Tirelli, 2019 [43] | | | | | | | |
| Baj, 2019 [33] | | | | | | | |
| Author | Method | Technique | Cohorts/Survival Analysis | No. of Tumors/No. of Margin Samples | Consistency | Demarcation of Safety-Margin | Positive Margin Defined by Publication | Definition of Free Margin by Authors | Acquisition Time | Technique Influence on the Final Histopathology | Free Margin Status on the Final Histopathology |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Durham, 2020 [36] | A | Autofluorescence | Autofluorescence (R) vs. WL-guided surgery (R)/survival analysis | 443 | Autofluorescence: 277 OSCC + HGL, control: 216 OSCC + HGL | At least 10 mm from the boundary of the WL-positive and FVL-positive areas | “Positive margin for severe dysplasia or greater histologic change”. | Not given | Undefined | Yes | Undefined, only the “first pass margin” is given, defined as the positive margin before re-resections are taken from the tumor bed. |
| Sun, 2021 [34] | C | Autofluorescence | Diagnostic accuracy of autofluorescence (P) | 30/126 | 30 OSCC | 15-20 mm from the boundary of the WL-positive area, no resections based on the FVL-positive area | Carcinoma in situ, invasive carcinoma, and severe dysplasia in mucosal samples | Normal epithelium in mucosal samples | Undefined | No | Undefined, only margins within random samples were reported |
| McMahon, 2010 [38] | A | Iodine | Iodine (P) vs. WL-guided surgery ® | 100 | Iodine: 40 OSCC and 10 OPSCC, control: 42 OSCC, 8 OPSCC | 10 mm from the boundary of the WL-positive area and 0 mm from the IU-positive areas were included | “Intraepithelial neoplasia in mucosal margin”. | “Mucosal margins free from dysplasia, carcinoma in situ and invasive carcinoma” | Undefined | Yes | Iodine: 96% (48/50), WL 96% (34/50) |
| Umeda, 2011 [39] | A | Iodine | Iodine (R)/Survival analysis. | 93 | 93 OSCC of the tongue | At least 10 mm from the boundary of the WL-positive areas and at least 5 mm from the boundary of the IU-positive areas | “Positive for SCC” or ‘’positive for dysplasia”. | SCC ≥ 1 mm from the deep or mucosal margin | Undefined | Yes | 81/93 (87%) |
| Tirelli, 2015 [40] | C | NBI | NBI (P) | 16 | 8 OSCC, 8 OPSCC | 15 mm from the boundary of the WL-positive areas and including the boundary of the NBI-positive areas. | SCC < 0.1 mm from the mucosal margin | SCC > 3 mm from the mucosal margin | 5 min | Yes, technique-directed FSA did not influence diagnostic accuracy | 94% (15/16)/yes |
| Tirelli, 2017 [41] | B | NBI | NBI (P) | 31 | 20 OSCC, 11 OPSCC (of 2 the result of the reference test was not clear) | 15 mm from the boundary of the WL-positive areas and including the boundary of the NBI-positive areas. | SCC < 0.1 mm from the mucosal margin | SCC > 3 mm from the mucosal margin | 5 min | Yes, FSA, in addition to the technique, did not influence diagnostic accuracy | 77% (24/31)/yes |
| Tirelli, 2018 [42] | B | NBI | NBI (P) | 61 | 39 OSCC, 22 OPSCC | 15 mm from the boundary of the WL-positive areas and including the boundary of the NBI-positive areas. | SCC < 0.1 mm from the mucosal margin | SCC > 3 mm from the mucosal margin | 5 min | Yes, FSA, in addition to the technique, did not influence diagnostic accuracy | 85% (52/61)/yes |
| Baj, 2019 [33] | C | NBI | NBI (P) | 16/ 88 | 16 OSCC | 15-20 mm from the boundary of the WL-positive area, no resections based on the NBI-positive area | Tumor or dysplasia in the FSA biopsy | No tumor or dysplasia in FSA biopsy | Undefined | No | Undefined, only FSA biopsy status reported |
| Author | Evaluation | Reference Results Based on | Test Positive/Negative | Ref Positive/Negative | NPV SCC (Test/WL Control Group) | NPV SCC + Severe Dysplasia (Test/WL Control Group) | NPV SCC + Dysplasia (Test/WL Control Group) | Bias or Concern |
|---|---|---|---|---|---|---|---|---|
| Durham, 2020 [36] | Interventional (with WL-guided control group) | Full specimen (OSCC or HGL) | NA/10 mm from the WL-positive area and 10 mm from the FVL-positive area (whichever was wider) | “Severe dysplasia or greater histologic change” in the resection plane on the final histopathology/normal tissue in the resection plane on the final histopathology | Not given | Test: 70% (151/216) Control: 70% (159/227) | Not given | Unknown reason for certain exclusions; patients with small tumors and “High-grade lesions” were included as well. |
| Sun, 2021 [34] | Diagnostic accuracy | Samples from margin | Sample within the FVL-positive area exceeding the WL-positive area/sample within the FVL-positive area inside the WL-positive area | SCC or dysplasia (all types) in the sample of the FVL-positive area/normal tissue in the sample of the FVL-positive area | 100% (126/126) | 82% (103/126) | 61% (77/126) | 126 samples were taken and analyzed from random locations between the boundary of the FVL-positive area and the surgical margin of 30 tumors |
| Author | Evaluation | Reference Results Based on | Test Positive/Negative | Ref Positive/Negative | NPV SCC (Test Group/WL Control Group) | NPV SCC + Severe Dysplasia or (Test/WL Control Group) | NPV SCC + Dysplasia (Test/WL Control Group) | Bias of Concern |
|---|---|---|---|---|---|---|---|---|
| McMahon, 2020 [38] | Interventional (with WL-guided control group) | Full specimen | NA/10 mm from the boundary of the WL-positive area, 0 mm from the IU-positive area | Dysplasia (all types)or SCC in the resection plane | Test: 100% (50/50) Control: 96% (48/50) | Test: 98% (49/50) Control: 96% (47/50) | Test: 96% (48/50) Control: 68% (34/50) | None. |
| Umeda, 2011 [39] | Interventional (no WL-guided surgery control group) | Full specimen | NA/ 10 mm from the boundary of the WL-positive area and 5 mm from the IU-positive area | Dysplasia or SCC in the resection plane | 99% (92/93) | Not given, only mild dysplasia in the resection plane | 92% (86/93) | None. |
| Author | Evaluation | Reference Results Based on | Test Positive/Negative | Ref Positiv/Negative | Sens/Spec Cancer | PPV/NPV Cancer | Sens/Spec SCC + Sdys | PPV/NPV SCC + Sdys | Sens/Spec SCC + Dys (all Types) | PPV/NPV SCC + Dys (All Types) | Bias of Concern |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Tirelli, 2015 [40] | Diagnostic accuracy | FSA-samples | The NBI-positive area beyond the 15 mm WL-safety margin/NBI-positive area between the boundary of the WL-positive area and 15 mm WL-safety margin | SCC and/or dysplasia/no SCC and/or dysplasia in the NBI-positive or negative area | Sens: 100% (12/12) Spec: 0% (0/4) | PPV: 75% (12/16) NPV: undefined (0/0) | NA | NA | Sens: 100% (16/16) Spec: undefined (0/0) | PPV: 100% (16/16) NPV: undefined (0/0) | Only the NBI-positive areas were assessed with biopsies, while the NBI-negative areas, (mucosa within the 15 mm W-safety margin, but outside the boundary of the NBI-positive area) did not receive a biopsy. Also, the NBI-positive area seemed too small, since dysplasia and SCC were found in the resection plane. Possible overlap with Tirelli 2017 and Tirelli 2018. |
| Tirelli, 2017 [41] | Interventional with diagnostic accuracy | Final histopathology | NBI-positive area beyond the 15 mm WL-safety margin/ NBI-positive area between the boundary of the WL-positive area and 15 mm WL-safety margin | SCC and/or dysplasia/no SCC and/or dysplasia in the NBI-positive or negative area | Sens: 100% (12/12) Spec: 6% (1/17) | PPV: 43% (12/28) NPV: 100% (1/1) | Sens: 100% (16/16) Spec: 8% (1/13) | PPV: 57% (16/28) NPV: 100% (1/1) | Sens: 100% (20/20) Spec: 11% (1/9) | PPV: 71% (20/28) NPV: 100% (1/1) | Only one specimen with NBI-negative findings (specimen with the boundary of the NBI-positive area within the WL margin). Of two specimens, the NBI-positive areas were as large as the WL-safety margin, but it was unclear whether the resection planes were free from SCC/dysplasia. Hence, only 29 cases could be evaluated. Possible overlap with Tirelli 2015 and Tirelli 2018. |
| Tirelli, 2018 [42] | Interventional with diagnostic accuracy | Final histopathology | NBI-positive area beyond the 15 mm WL-safety margin/ NBI-positive area between the boundary of the WL-positive area and 15 mm WL-safety margin | SCC and/or dysplasia/no SCC and/or dysplasia in the NBI-positive or negative area | Sens: 96% (23/24) Spec: 46% (17/37) | PPV: 53% (23/43) NPV: 94% (17/18) | Sens: 93% (28/30) Spec: 52% (16/31) | PPV: 65% (28/43) NPV: 89% (16/18) | Sens: 94% (34/36) Spec: 64% (16/25) | PPV: 79% (34/43) NPV: 89% (16/18) | Possible overlap with Tirelli 2015 and Tirelli 2017. |
| Baj, 2019 [33] | Diagnostic accuracy | FSA-samples | NBI boundary outside 15–20 mm from the WL boundary/NBI-positive area between the boundary of WL-positive area and 15 mm WL-safety margin | Dysplasia or SCC in FSA biopsy from a positive test situation/no dysplasia or SCC in FSA biopsy | Not given | Not given | Not given | Not given | Sens: 38% (3/8) Spec: 70% (32/46) | PPV: 18% (3/17) NPV: 86% (32/37) | Only small biopsies were taken for certain areas. The WL-safety margin was not from a consistent distance from the WL-positive boundary (varying between 15 and 20 mm). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Koning, K.J.; Adriaansens, C.M.E.M.; Noorlag, R.; de Bree, R.; van Es, R.J.J. Intraoperative Techniques That Define the Mucosal Margins of Oral Cancer In-Vivo: A Systematic Review. Cancers 2024, 16, 1148. https://doi.org/10.3390/cancers16061148
de Koning KJ, Adriaansens CMEM, Noorlag R, de Bree R, van Es RJJ. Intraoperative Techniques That Define the Mucosal Margins of Oral Cancer In-Vivo: A Systematic Review. Cancers. 2024; 16(6):1148. https://doi.org/10.3390/cancers16061148
Chicago/Turabian Stylede Koning, Klijs J., Carleen M. E. M. Adriaansens, Rob Noorlag, Remco de Bree, and Robert J. J. van Es. 2024. "Intraoperative Techniques That Define the Mucosal Margins of Oral Cancer In-Vivo: A Systematic Review" Cancers 16, no. 6: 1148. https://doi.org/10.3390/cancers16061148
APA Stylede Koning, K. J., Adriaansens, C. M. E. M., Noorlag, R., de Bree, R., & van Es, R. J. J. (2024). Intraoperative Techniques That Define the Mucosal Margins of Oral Cancer In-Vivo: A Systematic Review. Cancers, 16(6), 1148. https://doi.org/10.3390/cancers16061148