2. Methods
2.1. Data Source/Study Population
We used the California Cancer Registry (CCR) Research File of July 2023 to identify thyroid cancer cases diagnosed from 2010 to 2020 among California (CA) residents in a SEER*Stat readable format along with statewide mortality data with causes of death information.
We examined demographic characteristics by sex (male, female), age at diagnosis (0–39, 40–49, 50–59, 60–69, 70+ years old), race/ethnicity (Hispanic, non-Hispanic (NH) White, NH Black, and Asian Pacific Islander (API)), and socioeconomic status (lowest, lower middle, middle, upper middle, highest). Socioeconomic status was derived from United States census data based on the patient’s address at the time of initial diagnosis while factoring in the following census variables using a principal components analysis: the proportion of people with a blue collar job, the proportion older than 16 years without a job, the median household income, the proportion of the population living below the 200% Federal Poverty Level, the median gross rent, the median value of owner-occupied houses, and the median education index [
13,
14]. Socioeconomic status was split into quartiles—lowest, lower middle, middle, upper middle, and highest.
The cases of thyroid cancer from 2010 to 2020 were identified using the International Classification of Disease for Oncology, Third Edition (ICD-O-3), with site code C73.9—thyroid gland. Tumor histotypes included follicular (ICD-O-3 codes 8290, 8330, 8331, 8332, 8333, 8335, 8337, 8339, 8346), papillary (ICD-O-3 codes 8050, 8260, 8261, 8262, 8263, 8340, 8341, 8342, 8343, 8344, 8347), medullary (ICD-O-3 codes 8345, 8510, 8346, 8347), and anaplastic (ICD-O-3 codes 8020, 8021, 8022).
We studied tumor behavior by evaluating the TNM stage (I-IV) along with the specific tumor size (T0–T4) and lymph node involvement (N0, N1) in cases from 2010 to 2020 using the American Joint Committee on Cancer (AJCC) staging 7th–8th editions [
15,
16]. We also looked at the Charlson comorbidity score from 2010 to 2020, categorizing them by 0 for no health comorbidities and 1+ for 1 or more health comorbidities.
The CCR collects limited treatment information within the first 6 months after a cancer diagnosis. Data specific to thyroid surgery (no surgery, lobectomy/local surgery, subtotal or near total thyroidectomy, total thyroidectomy, thyroidectomy/surgery, NOS, and unknown) were available from 2010 to 2020, along with radiation treatment data (no radiation, isotopes, radiation/combination/other, and unknown) from 2010 to 2020.
2.2. Statistical Analysis
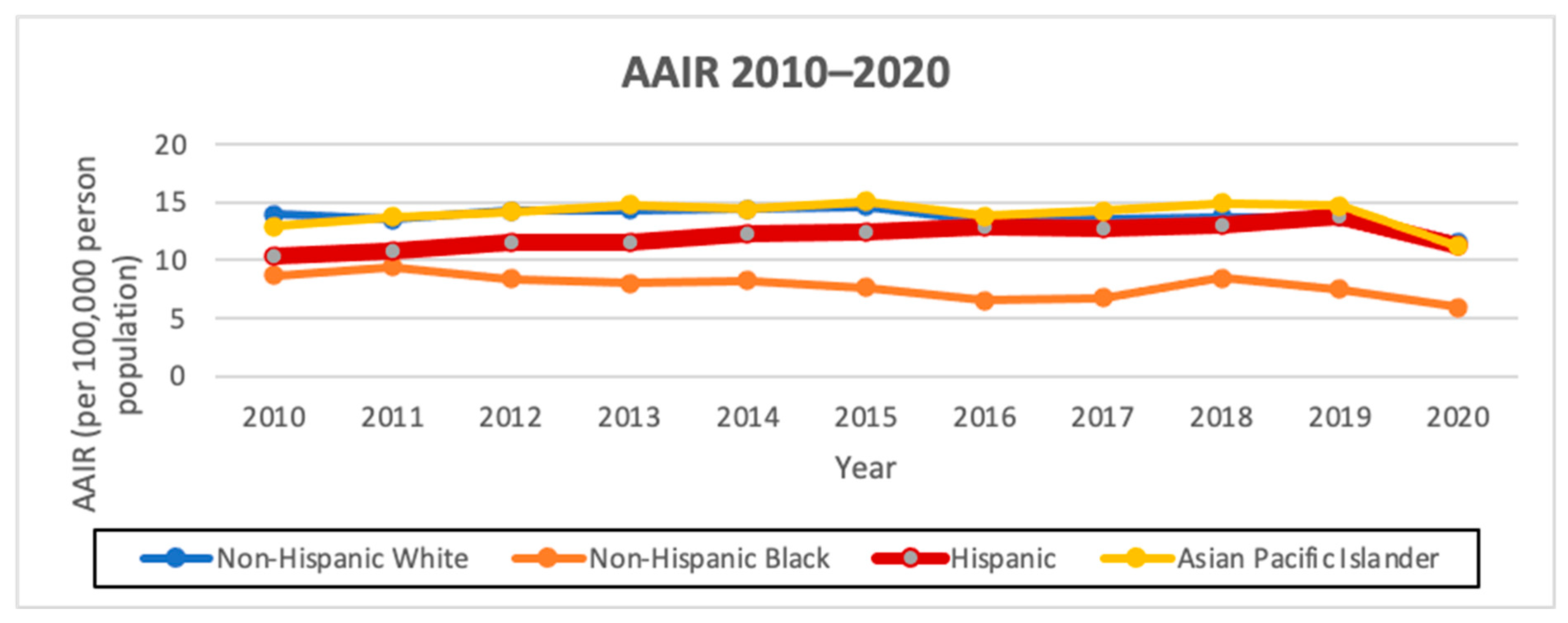
To compare cancer risk levels among different groups, we calculated and presented the age-adjusted incidence rates and age-adjusted mortality rates by considering the number of cancer occurrences and cancer-related deaths, respectively, in relation to the size of a group’s at-risk population. The age-adjusted incidence rates (AAIRs) per 100,000 person-years of incidence and histology (papillary, follicular, medullary, anaplastic), along with the average annual percent change (AAPC) from 2010 to 2020, were calculated by sex and race/ethnicity using the CCR SEER*Stat database file of January 2023 [
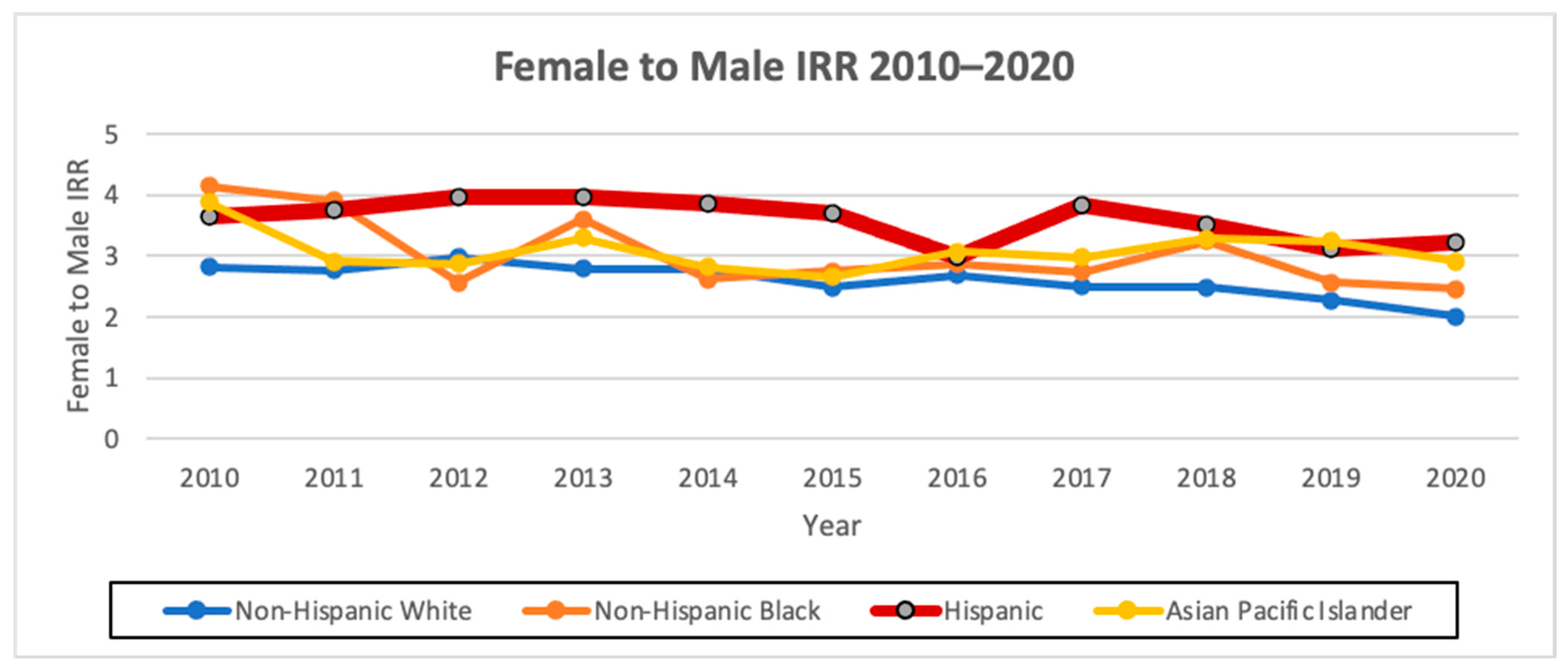
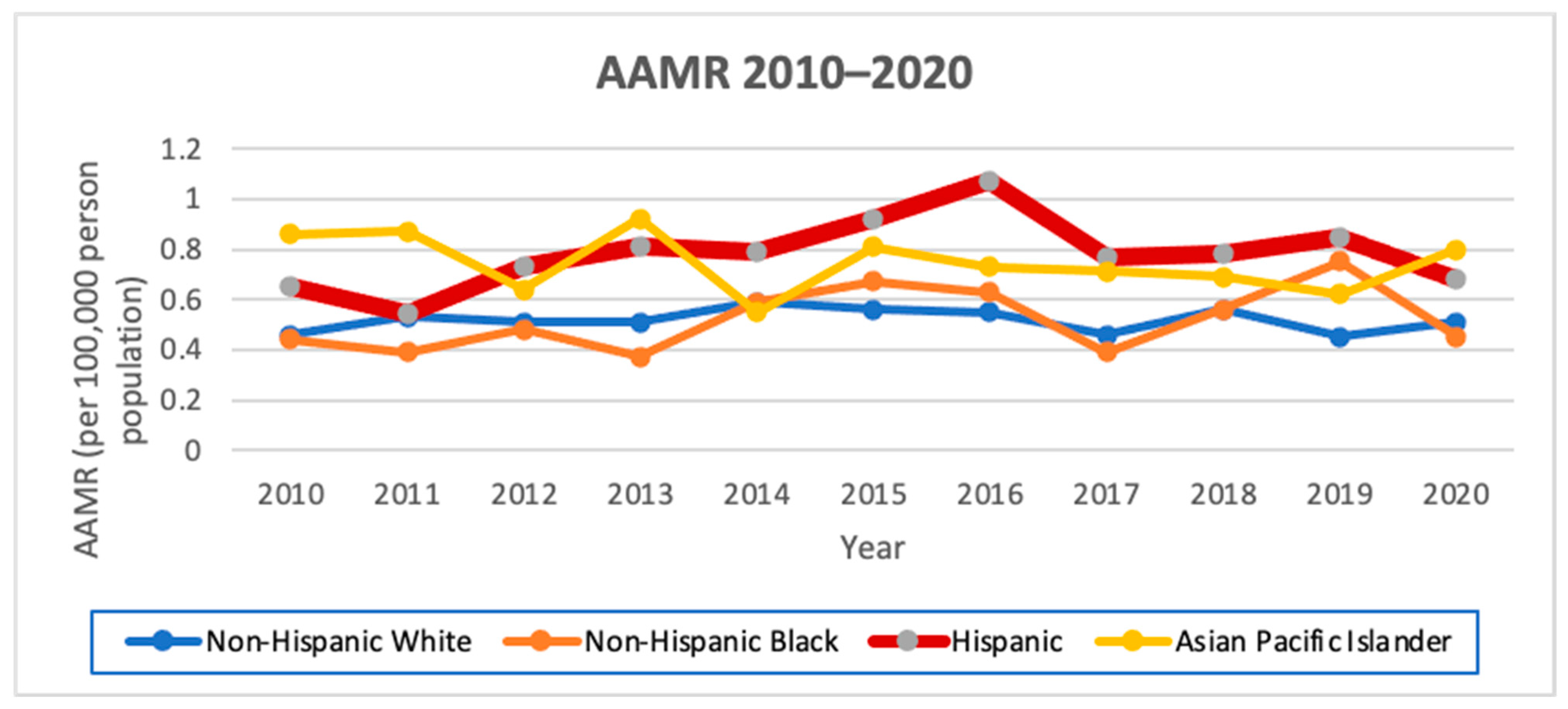
17]. In addition, we calculated the incidence rate ratio (IRR) of females to males. Additionally, age-adjusted mortality rates (AAMRs) for all causes of death were calculated by sex and race, with the AAPC measured from 2010 to 2020 using the California Department of Public Health’s Center for Health Statistics Death Master Files from 1970 to 2020 [
18].
To evaluate the mortality risk from all causes of death by race/ethnicity in thyroid cancer cases, we performed a univariate analysis of race/ethnicity (Hispanic, NH White, NH Black, and API) and a multivariate hazard cox ratio regression analysis consisting of race/ethnicity (Hispanic, NH White, NH Black, and API), age (0–39, 40–64, 65+), sex (female, male), socioeconomic status (lowest, lower middle, middle, upper middle, highest), Charlson score (0, 1+), surgery (surgery, no surgery), radiation (isotopes, radiation/combination/other, no radiation), stage (I, II, III, IV), and lymphovascular invasion (present, not present). Given the mixed-race/ethnicity group, we excluded the American Indian/Other/Unknown race/ethnicity group from the univariate and multivariate analyses.
Tests for statistical significance were two-sided and considered statistically significant at p < 0.1. The statistical analysis was performed using SAS software, release 9.4. (SAS Institute, Cary, NC, USA).
4. Discussion
In our analysis of Hispanic thyroid cancer patients in California from 2010 to 2020, we show that the more than 3.5:1 ratio of female to male was the largest compared to all the other races/ethnicities, and that Hispanics had the greatest AAIR AAPC, with Hispanic males (3.4; 95% CI 1.4–5.5, p < 0.1) having a significantly positive AAIR AAPC that no other male or female racial/ethnic group demonstrated. Furthermore, a greater proportion of Hispanics were diagnosed with advanced disease features, including larger tumor sizes, positive nodal sizes, and lymphovascular invasion. Hispanic ethnicity had the highest AAMR among both males and females, with Hispanic males having a significantly increased AAPC (4.2; 95% CI −6.9–16.6, p < 0.1). This finding persisted after adjusting for different variables, including both socioeconomic and tumor-related variables; Hispanic ethnicity in California (HR: 1.21, 95% CI 1.18–1.24, p < 0.0001) persistently remained a significantly independent variable in mortality risk in thyroid cancer. Thus, our findings are consistent with studies from past years but also show a significant mortality risk among Hispanics.
In thyroid cancer, estrogen receptor-alpha cells are overexpressed, while estrogen receptor-beta cells reduce tumor growth, and the fact that the ratio of estrogen receptor-alpha is greater than estrogen receptor-beta in thyroid cancer contributes to the high female-to-male ratio. Hispanics have been shown to have similar estrogen levels to non-Hispanic White people but lower levels than non-Hispanic Black people [
19,
20]. But, obesity appears to be associated with the development of differentiated thyroid cancer, particularly with leptin, a hormone produced primarily by adipose tissue; leptin and its receptor (OB-R) have been implicated to be overexpressed in thyroid carcinomas, particularly papillary thyroid cancer, as multiple studies of PTC tissues have shown an expression of 50–80% of PTC tissue expressing OB-R and leptin [
21,
22,
23,
24]. Hispanics (44.8%) do have higher rates of obesity compared to non-Hispanic White people (42.2%) and Asian Pacific Islanders (17.4%), but similar rates of obesity exist between Hispanic males (45.7%) and females (43.7%) [
25]. Much of the sex disparity lies in the fact that many of the cases among women were small, early-stage papillary thyroid cancer cases [
26]. Yet, in our data, we see that Hispanics have a greater prevalence of large tumor sizes. We note that thyroid cancer is the second most common cancer diagnosis during pregnancy, and there have been links to recent pregnancy and infertility problems causing thyroid cancer [
27,
28,
29]. Compared to Non-Hispanic women, Hispanic women with Medicaid insurance had 22% higher rates of severe pregnancy complications in 2020 and Hispanic women with private insurance had a 28% increase in severe pregnancy complications in 2021 [
30]. The sex ratio in thyroid cancer may also be genetic, as six single-nucleotide polymorphisms (SNPs) identified in Colombia have been tied to an increased female-to-male ratio (5:1) along with larger tumor sizes [
31]. As such, further investigations are needed to understand the greater sex disparity in thyroid cancer incidence among Hispanics.
Hispanics were also found to have the highest AAIR AAPC (1.0; 95% CI −0.3–2.4,
p < 0.1), with Hispanic males having a significantly positive AAIR AAPC (3.4; 95% CI 1.4–5.5,
p < 0.1) that no other male or female racial group demonstrated. This could be multifactorial; first, Hispanic presence in California has been increasing, as the percentage of Hispanics has increased from 19.8% in 1980 to 32.4% in 2000 to 37.6% in 2010 to 40.4% in 2020 [
12,
32]. Furthermore, as mentioned prior, Hispanics have higher percentages of obesity than non-Hispanic White people, which may be contributing to the AAPC [
25]. In addition, it has been suggested that metabolic syndrome and its subsequent abnormal metabolism can place the body in a state of chronic inflammation, leading to thyroid-stimulating hormones inducing tumorigenesis [
33]. Hispanics have been shown to have a higher prevalence of cardiovascular disease, Type II diabetes, non-alcoholic fatty liver disease, and dyslipidemia, which may indirectly play into the higher increases in thyroid cancer incidence [
34].
Our data also demonstrated that Hispanics had a higher prevalence of larger tumor sizes and positive nodal sizes compared to other races/ethnicities, consistent with previous studies [
3,
4,
5,
6,
7,
8]. An SEER analysis from 2017 to 2018 showed that Hispanics had a greater percentage of nodal disease at initial surgery compared to non-Hispanic White people and a greater incidence of recurrent disease, while another SEER analysis showed that Hispanics were more likely to present with distant disease than non-Hispanic White people [
5]. Meanwhile, a meta-analysis has shown that Hispanics have the greatest proportion among all races/ethnicities of having tumors > 4 cm in size at diagnosis [
4]. Finally, another SEER analysis from 1992 to 2006 showed that Hispanics had the highest rate of anaplastic thyroid cancer diagnosed [
35]. This was also seen among papillary thyroid cancer patients in an SEER analysis from 2011 to 2013 receiving adjuvant radiation, in which Hispanics and Asian Pacific Islanders had greater odds of T4, N1, or M1 disease [
36].
Socioeconomic status and access to care may factor into the increased mortality risk of Hispanic ethnicity, as middle-to-low socioeconomic status was a significant independent variable in our multivariate analysis. A total of 47% of Hispanic women in Los Angeles with thyroid cancer reported financial hardship, along with 49% reporting low acculturation to the English language [
37]. While Hispanics have a lower AAIR of thyroid cancer compared to Asian Pacific Islanders and non-Hispanic White people, uninsured Hispanics had the highest AAIR compared to the other races/ethnicities [
1]. Hispanics have the lowest health insurance rate of any racial or ethnic group (34%), including more than twice that of non-Hispanic White people [
38,
39]. Hispanics also have a 25% lower median income than non-Hispanic White people [
39,
40]. Subsequently, the limitations of financial resources and access to care may affect Hispanics in terms of having adequate health literacy and limit their means to being able to have a well-balanced diet and places to carry out ample exercise, which are key factors in avoiding some possible triggers to thyroid cancer such as metabolic syndrome and obesity.
Despite factoring disease characteristics and socioeconomic variables into our multivariate analysis, Hispanic ethnicity (HR: 1.21, 95% CI 1.18–1.24,
p < 0.05) remains a significant risk factor. Some of this may have to do with genetic changes in Hispanics relative to other races/ethnicities. Hispanics have been shown to have an increased prevalence of
BRAF V600E, and this mutation has been linked in the past with increased mortality [
41,
42]. The
BRAF V600E mutation has been shown to be associated with more advanced clinical stages and decreased responsiveness to radioiodine [
43]. Even in smaller-size papillary thyroid cancer cases of <1.5 cm, a significantly higher percentage of
BRAF V600E cases demonstrate aggressive features such as extrathyroidal extension and lymph node metastasis compared to non-mutated cases [
44]. Among Hispanics, poorly differentiated
BRAF mutant cases are significantly increased compared to non-Hispanic White people [
43,
45]. Furthermore, a Colombian study investigating 141 papillary thyroid cancer cases showed that the
BRAF V600E and
TERT C228T or C250T mutations were associated with large tumors, lymph node metastasis, extra-thyroid extension, and advanced stages, and compared to published data on U.S. white people, Colombian patients had a higher prevalence of both severe pathologic features and double-mutant tumors [
46]. It has been thought that some of the key genes triggering this are related to several microRNAs targeting the TGF-beta–SMAD pathway [
43].
TERT promoter mutations have been shown in 95% of thyroid tumors that have transformed from papillary carcinoma to a more aggressive anaplastic thyroid carcinoma and so pose a greater risk of transformation to a more aggressive and rare thyroid cancer compared to other mutations [
47]. That being said, additional studies with larger sample sizes comparing
BRAF V600E-mutant thyroid cancer cases among Hispanics and non-Hispanics are merited to better characterize the effect of
BRAF V600E on the prevalence of advanced features and mortality risk.
There are clinical implications, as dabrafenib, a
BRAF-mutated tyrosine kinase inhibitor, has been shown to have efficacy in well-differentiated radioactive-iodine-resistant thyroid cancer patients and, in combination with trametinib, has been shown to improve overall survival in anaplastic thyroid cancer [
48,
49]. Other important mutations to note that it could be worth investigating the prevalence of among Hispanics given their associations with anaplastic transformation outside of
TERT-promoter mutations include subunits of the SWI/SNF complex such as
SMARCA4 and alterations of the
PIK3CA gene, which were found to be positive in 33% of thyroid tumor samples with a heterogenous pathology of papillary and anaplastic carcinoma components [
47]. Mutations in
RAS genes occur in 30–45% of follicular thyroid cancer, 30–45% of follicular-variant papillary thyroid cancer, and 20–40% of poorly differentiated thyroid cancer and are also worth investigation among Hispanics [
50]. Meanwhile,
RET proto-oncogene is found in medullary thyroid carcinoma, and while a small-case analysis of medullary thyroid carcinoma among Mexicans has been performed, larger studies could be conducted to evaluate any possible connection between any particularly Hispanic subgroups and medullary thyroid cancer/multiple endocrine neoplasia type 2 [
51,
52].
By studying additional molecular alterations in Hispanics relative to other races/ethnicities, this may help mitigate the mortality risk among the Hispanic race/ethnicity. With possible known mutations and associated targeted therapies, the need for equality in obtaining comprehensive genomic profiling of tumors and access to targeted therapy agents is critical. Hispanic ethnicity has been shown to be underrepresented among patients obtaining precision oncology assays [
53]. Moreover, Hispanics have had less access to targeted drugs and are severely underrepresented in clinical trials that could provide access to these drugs and help better understand biological differences in response to these drugs [
54].
The key limitations of this analysis and important considerations moving forward are that our analysis consists of Hispanics in the state of California in the United States, which means that it is not completely generalizable to Hispanic populations elsewhere. Hispanics in California consist of primarily those with Mexican descent (77%), while Hispanics in Florida consist of those with primarily Caribbean descent, notably Cuban (28%) and Puerto Rican (21%) [
55,
56]. Further analysis in other sectors of the U.S. may help better elucidate differences in tumor characteristics and socioeconomic challenges among different Hispanic subgroups. In addition, another limitation is the lack of genetic testing available. Comparing molecular testing for key mutations of thyroid cancer, such as
BRAF V600E and
RET, is important among Hispanics and other races/ethnicities and within Hispanic subgroups.
Another important aspect that is critical in future analysis is comparing differences in thyroid cancer among Hispanic immigrants from different origins and Hispanics who are U.S.-born. U.S.-born Hispanic women younger than 55 have been shown to have a significantly greater incidence of papillary thyroid cancer, while the opposite is true in older Hispanic women [
9]. In another study comparing Colombians and U.S. Hispanics, U.S.-born Hispanics had a smaller mean tumor size of 20 mm vs. 27 mm than Colombians and were half as likely to have regional disease (16.7% vs. 31.15%) [
31]. In another study comparing Puerto Ricans and U.S. mainland Hispanics, Puerto Rican women had an 83% increased risk of a papillary thyroid cancer diagnosis compared to U.S. Hispanics, and Puerto Rican men had a 2.2-fold increased risk compared to U.S. Hispanic men [
57]. This shows that disaggregated data among Hispanics both in the U.S. and outside the U.S. by origin will be important in helping describe mortality risk in thyroid cancer. Finally, 5% of the population in California is made up of undocumented immigrants, with Mexicans and Salvadorans constituting the largest share [
58]. Given that some of their data may not be identifiable in the cancer registry as a result, the magnitude of the risks involved in the incidence and mortality of thyroid cancer may be even greater.
Thus, our study highlights key important factors showing that greater attention needs to be paid to Hispanics in thyroid cancer moving forward due to the greater prevalence of large tumor sizes and positive nodal status at presentation, the greater sex disparities in women compared to men, and the increased mortality driven both by tumor characteristics and socioeconomic factors among Hispanics. As much of this could be tied to differences in the genetic makeup of thyroid cancer tumors, access to molecular testing, targeted therapies, clinical trials, and mitigating financial costs is paramount to helping bridge these disparities.


 ,
, 



{kind=link}
{kind=link}
{kind=link}