
Talking about Familial Breast and Ovarian Cancer Risk—Evaluation of a Psychosocial Training Module for Gynecologists in Germany
 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Phase 1: Needs Assessment
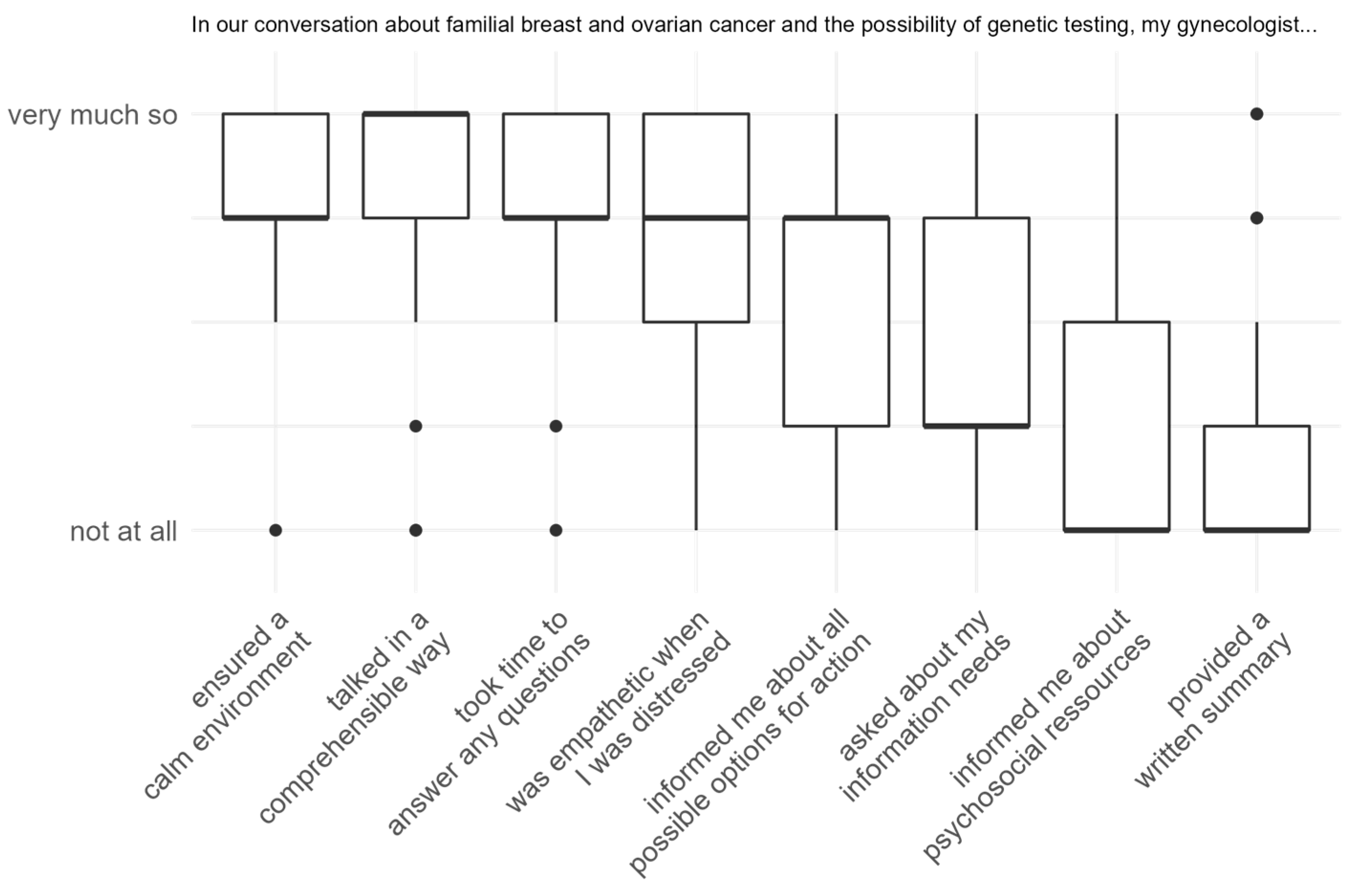
Results from the Pilot Study on Patients’ Experiences and Needs
2.2. Phase 2: Development of the Training Curriculum
2.2.1. Description of the Training Intervention
2.2.2. The Situation before Genetic Testing—Part A
2.2.3. Relevant Aspects When Discussing the Topic ‘Familial Cancer Burden’ with Women after Genetic Testing—Part B
2.3. Phase 3: Evaluation of the Training Curriculum
Methods of Evaluation of the Training
3. Main Results—Evaluating the Training
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beard, C.; Monohan, K.; Cicciarelli, L.; James, P.A. Mainstream genetic testing for breast cancer patients: Early experiences from the Parkville Familial Cancer Centre. Eur. J. Hum. Genet. 2021, 29, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Schmidtke, J.; Pabst, B.; Nippert, I. DNA-based Genetic Testing Is Rising Steeply in a National Health Care System with Open Access to Services: A Survey of Genetic Test Use in Germany, 1996–2002. Genet. Test. 2005, 9, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Kne, A.; Zierhut, H.; Baldinger, S.; Swenson, K.K.; Mink, P.; Veach, P.M.; Tsai, M.L. Why Is Cancer Genetic Counseling Underutilized by Women Identified as at Risk for Hereditary Breast Cancer? Patient Perceptions of Barriers Following a Referral Letter. J. Genet. Couns. 2017, 26, 697–715. [Google Scholar] [CrossRef] [PubMed]
- Meyer, L.A.; Anderson, M.E.; Lacour, R.A.; Suri, A.; Daniels, M.S.; Urbauer, D.L.; Nogueras-Gonzalez, G.M.; Schmeler, K.M.; Gershenson, D.M.; Lu, K.H. Evaluating Women with Ovarian Cancer for BRCA1 and BRCA2 Mutations: Missed Opportunities. Obstet. Gynecol. 2010, 115, 945–952. [Google Scholar] [CrossRef] [PubMed]
- van Riel, E.; van Dulmen, S.; Ausems, M.G.E.M. Who is being referred to cancer genetic counseling? Characteristics of counselees and their referral. J. Community Genet. 2012, 3, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Van Riel, E.; Wárlám-Rodenhuis, C.C.; Verhoef, S.; Rutgers, E.J.T.H.; Ausems, M.G.E.M. BRCA testing of breast cancer patients: Medical specialists’ referral patterns, knowledge and attitudes to genetic testing. Eur. J. Cancer Care 2010, 19, 369–376. [Google Scholar] [CrossRef] [PubMed]
- White, S.; Jacobs, C.; Phillips, J. Mainstreaming genetics and genomics: A systematic review of the barriers and facilitators for nurses and physicians in secondary and tertiary care. Genet. Med. 2020, 22, 1149–1155. [Google Scholar] [CrossRef]
- Douma, K.F.L.; Smets, E.M.A.; Allain, D.C. Non-genetic health professionals’ attitude towards, knowledge of and skills in discussing and ordering genetic testing for hereditary cancer. Fam. Cancer 2016, 15, 341–350. [Google Scholar] [CrossRef]
- Watson, M.; Foster, C.; Eeles, R.; Eccles, D.; Ashley, S.; Davidson, R.; Mackay, J.; Morrison, P.J.; Hopwood, P.; Evans, D.G.R.; et al. Psychosocial impact of breast/ovarian (BRCA 1/2) cancer-predictive genetic testing in a UK multi-centre clinical cohort. Br. J. Cancer 2004, 91, 1787–1794. [Google Scholar] [CrossRef]
- Speiser, D.; Kendel, F.; Fechner, K.; Olbrich, C.; Stegen, S.; Haering, S.; Rörig, A.; Feufel, M.A. iKNOWgynetics—A web-based learning concept to empower primary care gynecologists to participate in the care of patients with a family history of breast and ovarian cancer. J. Genet. Couns. 2023, 1–8. [Google Scholar] [CrossRef]
- Schmutzler, R.K.; Schmitz-Luhn, B.; Borisch, B.; Devilee, P.; Eccles, D.; Hall, P.; Balmana, J.; Boccia, S.; Dabrock, P.; Emons, G.; et al. Risk-Adjusted Cancer Screening and Prevention (RiskAP): Complementing Screening for Early Disease Detection by a Learning Screening Based on Risk Factors. Breast Care 2022, 17, 208–223. [Google Scholar] [CrossRef] [PubMed]
- Speiser, D.; Rebitschek, F.G.; Feufel, M.A.; Brand, H.; Besch, L.; Kendel, F. Accuracy in risk understanding among BRCA1/2-mutation carriers. Patient Educ. Couns. 2019, 102, 1925–1931. [Google Scholar] [CrossRef]
- King, A.; Hoppe, R.B. “Best Practice” for Patient-Centered Communication: A Narrative Review. J. Grad. Med. Educ. 2013, 5, 385–393. [Google Scholar] [CrossRef]
- Fallowfield, L.; Jenkins, V. Effective communication skills are the key to good cancer care. Eur. J. Cancer 1999, 35, 1592–1597. [Google Scholar] [CrossRef] [PubMed]
- Langewitz, W. Physician-patient communication in medical education: Can it be learned? Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2012, 55, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Bokkers, K.; Vlaming, M.; Engelhardt, E.G.; Zweemer, R.P.; van Oort, I.M.; Kiemeney, L.A.L.M.; Bleiker, E.M.A.; Ausems, M.G.E.M. The Feasibility of Implementing Mainstream Germline Genetic Testing in Routine Cancer Care—A Systematic Review. Cancers 2022, 14, 1059. [Google Scholar] [CrossRef]
- Fallowfield, L.; Solis-Trapala, I.; Starkings, R.; May, S.; Matthews, L.; Eccles, D.; Evans, D.G.; Turnbull, C.; Crawford, G.; Jenkins, V. Talking about Risk, UncertaintieS of Testing IN Genetics (TRUSTING): Development and evaluation of an educational programme for healthcare professionals about BRCA1 & BRCA2 testing. Br. J. Cancer 2022, 127, 1116–1122. [Google Scholar] [CrossRef]
- Meiser, B.; Gaff, C.; Julian-Reynier, C.; Biesecker, B.B.; Esplen, M.J.; Vodermaier, A.; Tibben, A. International Perspectives on Genetic Counseling and Testing for Breast Cancer Risk. Breast Dis. 2007, 27, 109–125. [Google Scholar] [CrossRef]
- McClaren, B.J.; Crellin, E.; Janinski, M.; Nisselle, A.E.; Ng, L.; Metcalfe, S.A.; Gaff, C.L. Preparing Medical Specialists for Genomic Medicine: Continuing Education Should Include Opportunities for Experiential Learning. Front. Genet. 2020, 11, 151. [Google Scholar] [CrossRef]
- Fallowfield, L.; Jenkins, V.; Farewell, V.; Saul, J.; Duffy, A.; Eves, R. Efficacy of a Cancer Research UK communication skills training model for oncologists: A randomised controlled trial. Lancet 2002, 359, 650–656. [Google Scholar] [CrossRef]
- Fallowfield, L.; Jenkins, V.; Farewell, V.; Solis-Trapala, I. Enduring impact of communication skills training: Results of a 12-month follow-up. Br. J. Cancer 2003, 89, 1445–1449. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, V.; Fallowfield, L. Can Communication Skills Training Alter Physicians’ Beliefs and Behavior in Clinics? J. Clin. Oncol. 2002, 20, 765–769. [Google Scholar]
- Ernst, J.; Friedrich, M.; Lehmann, C.; Vehling, S.; Oechsle, K.; Koch, U.; Mehnert, A. Die Mitteilung schlechter Nachrichten durch den Arzt: Die deutsche Version des MPP-(Measure of Patients’ Preferences) Fragebogens zu den kommunikativen Präferenzen von Krebspatienten. Das Gesundheitswesen 2015, 78, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Mayring, P. Qualitative Inhaltsanalyse. In Grundlagen und Techniken; Beltz Juventa: Weinheim, Germany; Basel, Switzerland, 2010. [Google Scholar]
- Schmid Mast, M.; Kindlimann, A.; Langewitz, W. Recipients’ perspective on breaking bad news: How you put it really makes a difference. Patient Educ. Couns. 2005, 58, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Baile, W.F.; Buckman, R.; Lenzi, R.; Glober, G.; Beale, E.A.; Kudelka, A.P. SPIKES—A Six-Step Protocol for Delivering Bad News: Application to the Patient with Cancer. Oncologist 2000, 5, 302–311. [Google Scholar] [CrossRef]
- Harvie, M.; Howell, A.; Evans, G.D. Can Diet and Lifestyle Prevent Breast Cancer: What Is the Evidence? Am. Soc. Clin. Oncol. Educ. Book 2015, 35, e66–e73. [Google Scholar] [CrossRef]
- Porciello, G.; Montagnese, C.; Crispo, A.; Grimaldi, M.; Libra, M.; Vitale, S.; Palumbo, E.; Pica, R.; Calabrese, I.; Cubisino, S.; et al. Mediterranean diet and quality of life in women treated for breast cancer: A baseline analysis of DEDiCa multicentre trial. PLoS ONE 2020, 15, e0239803. [Google Scholar] [CrossRef]
- R Core Team R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020.
- Schwarzer, R.; Jerusalem, M. The General Self-Efficacy Scale (GSE). In Measures in Health Psychology: A User’s Portfolio; Causal and Control Beliefs; NFER-NELSON: Windsor, UK, 1995. [Google Scholar]
- Berger-Höger, B.; Vitinius, F.; Fischer, H.; Beifus, K.; Köberlein-Neu, J.; Isselhard, A.; Töpper, M.; Wiedemann, R.; Rhiem, K.; Schmutzler, R.; et al. Nurse-led decision coaching by specialized nurses for healthy BRCA1/2 gene mutation carriers-adaptation and pilot testing of a curriculum for nurses: A qualitative study. BMC Nurs. 2022, 21, 42. [Google Scholar] [CrossRef]
- Meiser, B.; Woodward, P.; Gleeson, M.; Kentwell, M.; Fan, H.M.; Antill, Y.; Butow, P.N.; Boyle, F.; Best, M.; Taylor, N.; et al. Pilot study of an online training program to increase genetic literacy and communication skills in oncology healthcare professionals discussing BRCA1/2 genetic testing with breast and ovarian cancer patients. Fam. Cancer 2022, 21, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Bellcross, C.A.; Peipins, L.A.; McCarty, F.A.; Rodriguez, J.L.; Hawkins, N.A.; Hensley Alford, S.; Leadbetter, S. Characteristics associated with genetic counseling referral and BRCA1/2 testing among women in a large integrated health system. Genet. Med. 2015, 17, 43–50. [Google Scholar] [CrossRef]
- Helms, M.; Kalmbach, N.; Neeb, C.; Kussmaul, J.; Speiser, D. 139 Centre of hereditary breast and ovarian cancer at charité—Who presents for counseling and why? In Proceedings of the ESGO SoA 2020 Conference, Virtual, 14–16 December 2020; pp. A109–A110. [Google Scholar]
- MacDonald, D.J.; Sarna, L.; Weitzel, J.N.; Ferrell, B. Women’s Perceptions of the Personal and Family Impact of Genetic Cancer Risk Assessment: Focus Group Findings. J. Genet. Couns. 2010, 19, 148–160. [Google Scholar] [CrossRef]
- Bonadona, V.; Saltel, P.; Desseigne, F.; Mignotte, H.; Saurin, J.-C.; Wang, Q.; Sinilnikova, O.; Giraud, S.; Freyer, G.; Plauchu, H.; et al. Cancer Patients Who Experienced Diagnostic Genetic Testing for Cancer Susceptibility: Reactions and Behavior after the Disclosure of a Positive Test Result. Cancer Epidemiol. Biomark. Prev. 2002, 11, 97–104. [Google Scholar]
- Listøl, W.; Høberg-Vetti, H.; Eide, G.E.; Bjorvatn, C. Anxiety and depression symptoms among women attending group-based patient education courses for hereditary breast and ovarian cancer. Hered. Cancer Clin. Pract. 2017, 15, 2. [Google Scholar] [CrossRef] [PubMed]
- Street, R.L., Jr.; Makoul, G.; Arora, N.K.; Epstein, R.M. How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ. Couns. 2009, 74, 295–301. [Google Scholar] [CrossRef]
- Cragun, D.; Bonner, D.; Kim, J.; Akbari, M.R.; Narod, S.A.; Gomez-Fuego, A.; Garcia, J.D.; Vadaparampil, S.T.; Pal, T. Factors associated with genetic counseling and BRCA testing in a population-based sample of young Black women with breast cancer. Breast Cancer Res. Treat. 2015, 151, 169–176. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Content | Learning Objective Participants Should… | Duration (Minutes) |
|---|---|---|
| Part A: the situation before genetic testing (45 min) | ||
| Psychosocial expectations and experiences of women with their gynecologists | … become aware of specific needs | 5 |
| Inclusion criteria for familial breast and ovarian cancer risk from a psychosocial perspective | … become aware of potential strains | 5 |
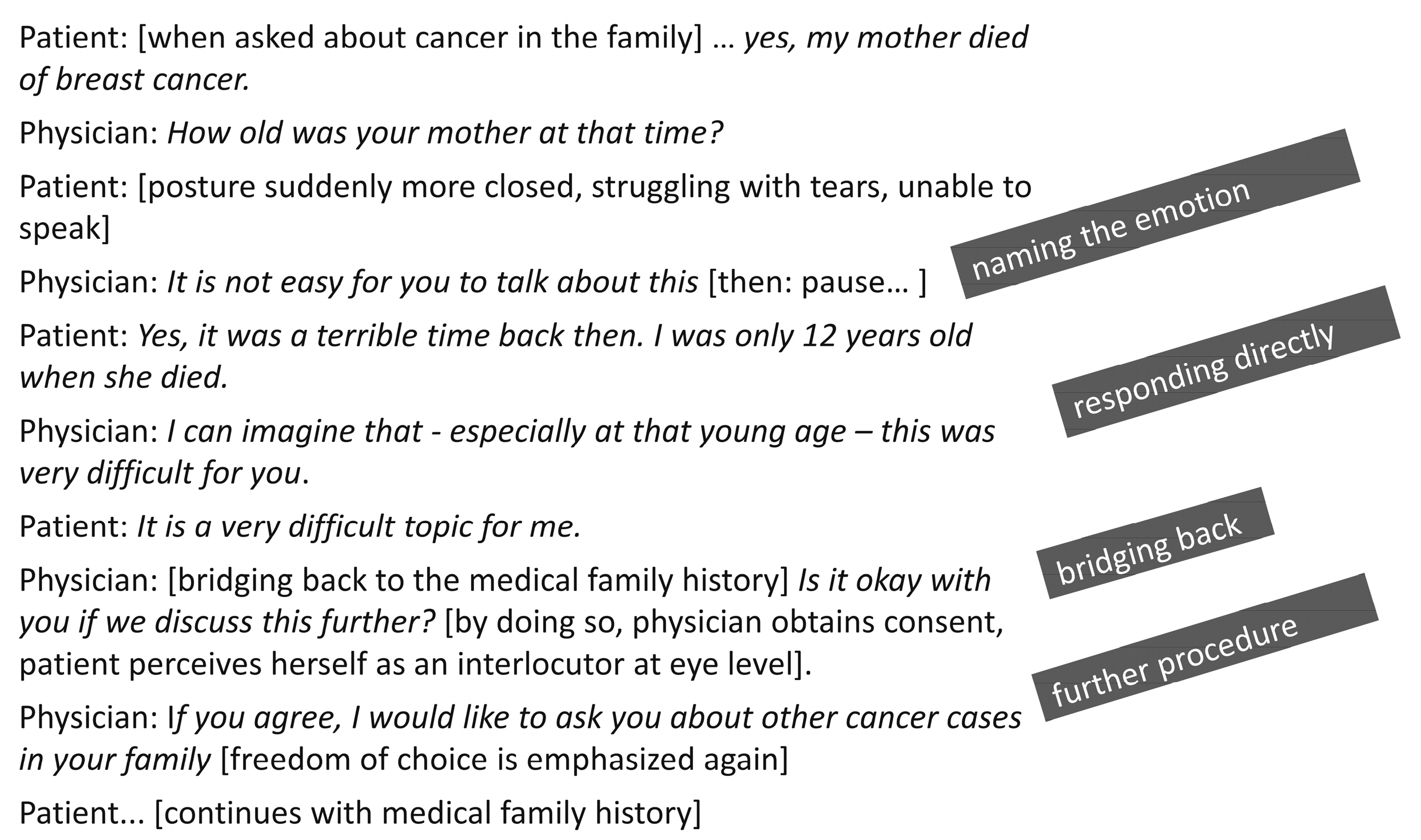
| Case examples | … be able to apply basic principles of communication in emotionally challenging situations | 25 |
| SPIKES model | … be able to use the SPIKES model to reflect on difficult situations | 10 |
| Part B: the situation after genetic testing (45 min) | ||
| Presentation of data on under- and overestimation of cancer risk in women with HBOC | … be able to recognize and address over- and underestimation | 25 |
| Peer networks, access to information | … become aware of the potential role of peer networks | 10 |
| Lifestyle changes | … be able to address the importance of lifestyle changes for health-related quality of life | 10 |
| Pre-Workshop M (SD) | Post-Workshop M (SD) | Cohen’s d | t (df) | p-Value | |
|---|---|---|---|---|---|
| I know how to communicate an increased risk for BRCA mutation in an empathic way | 3.16 (0.60) | 3.32 (0.53) | 0.22 | 2.31 (102) | 0.012 |
| It is easy for me to educate my patients about familial cancer in a comprehensible way. | 2.94 (0.65) | 3.28 (0.47) | 0.49 | 4.97 (102) | <0.001 |
| I am confident in dealing with different emotionally challenging patient reactions | 3.00 (0.54) | 3.20 (0.45) | 0.37 | 3.77 (102) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kendel, F.; Speiser, D.; Fechner, K.; Olbrich, C.; Stegen, S.; Rörig, A.; Feufel, M.A.; Haering, S. Talking about Familial Breast and Ovarian Cancer Risk—Evaluation of a Psychosocial Training Module for Gynecologists in Germany. Cancers 2024, 16, 310. https://doi.org/10.3390/cancers16020310
Kendel F, Speiser D, Fechner K, Olbrich C, Stegen S, Rörig A, Feufel MA, Haering S. Talking about Familial Breast and Ovarian Cancer Risk—Evaluation of a Psychosocial Training Module for Gynecologists in Germany. Cancers. 2024; 16(2):310. https://doi.org/10.3390/cancers16020310
Chicago/Turabian StyleKendel, Friederike, Dorothee Speiser, Karen Fechner, Christine Olbrich, Stephanie Stegen, Alina Rörig, Markus A. Feufel, and Stephanie Haering. 2024. "Talking about Familial Breast and Ovarian Cancer Risk—Evaluation of a Psychosocial Training Module for Gynecologists in Germany" Cancers 16, no. 2: 310. https://doi.org/10.3390/cancers16020310
APA StyleKendel, F., Speiser, D., Fechner, K., Olbrich, C., Stegen, S., Rörig, A., Feufel, M. A., & Haering, S. (2024). Talking about Familial Breast and Ovarian Cancer Risk—Evaluation of a Psychosocial Training Module for Gynecologists in Germany. Cancers, 16(2), 310. https://doi.org/10.3390/cancers16020310