
Metastatic Lymph Node Detection on Ultrasound Images Using YOLOv7 in Patients with Head and Neck Squamous Cell Carcinoma

Abstract
Simple Summary
Abstract
1. Introduction
- Incorporates a trainable bag-of-freebies to improve real-time object detection performance without increasing inference costs;
- Integrates extended and composite scaling to effectively reduce model parameters and calculations for faster detection; and
2. Materials and Methods
2.1. Patients
- Both axial-oriented B- and D-mode US images were available;
- Short-axis diameter >2 mm (the longest nodal axis perpendicular to the long axis of the node with the maximal nodal area in an axially oriented US image);
- Identifiable on dissection specimens; and
- Histologically proven metastasis or non-metastasis.
2.2. US Image Acquisition
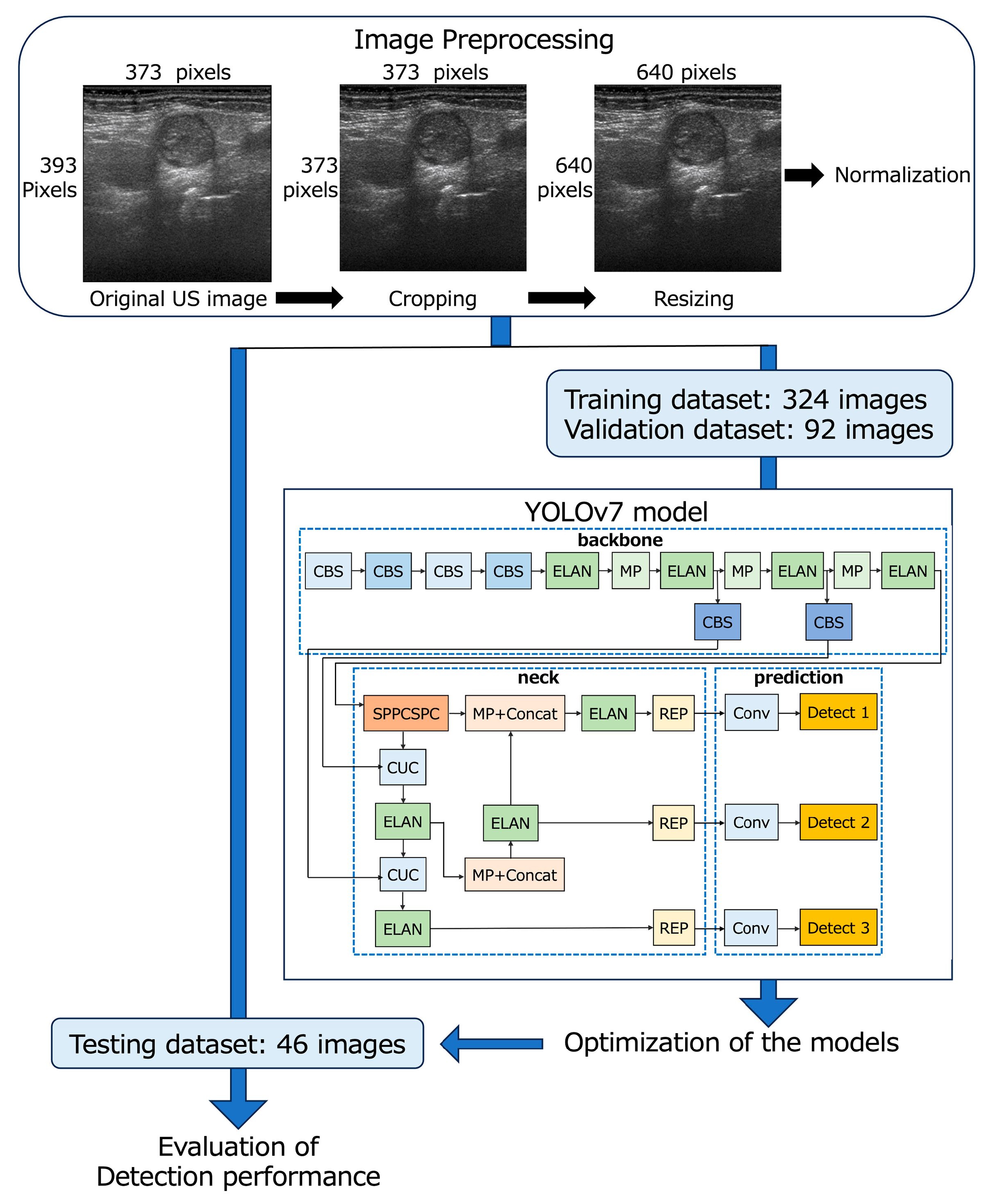
2.3. Preparation of US Datasets
2.4. YOLOv7 Model Procedure
- A low threshold (confidence score ≥ 0.1) to obtain a higher recall (B-mode model-1 and D-mode model-1), and
- An investigated threshold to obtain the largest area under the receiver operating characteristic curve (AUC) for the test images (B-mode model-2 and D-mode model-2).
2.5. Evaluation of Detection Performance and Comparison with Observers
2.6. Statistical Analysis
3. Results
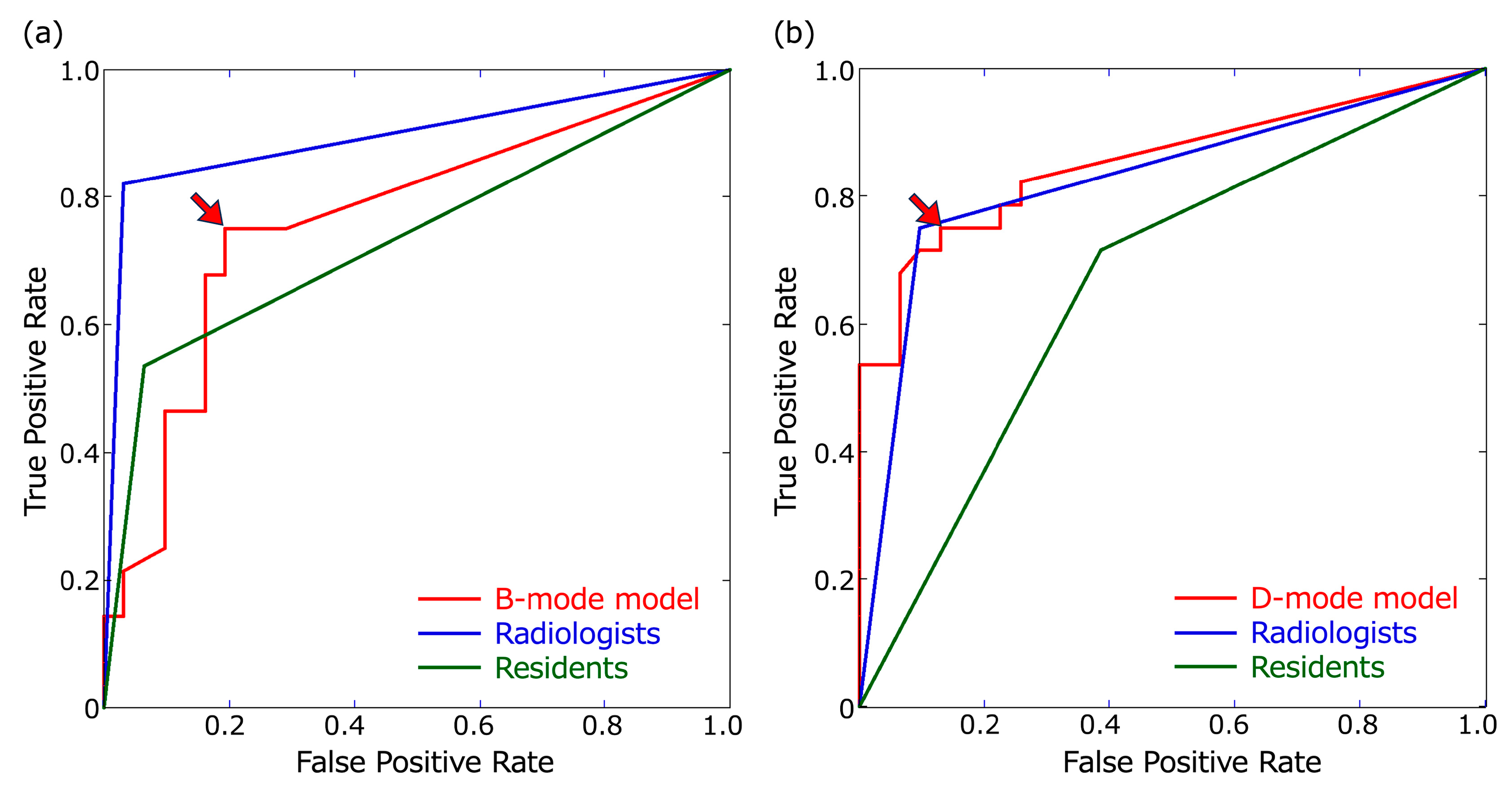
3.1. Detection Performance for Metastatic LNs
3.2. Recall at Each Cervical Level
3.3. Agreement on the Identification of Metastatic LNs between the Models and Observers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Cebeci, S.; Aydos, U.; Yeniceri, A.; Pula, D.; Duzlu, M.; Atay, L.O.; Yilmaz, M. Diagnostic performance of FDG PET/MRI for cervical lymph node metastasis in patients with clinically N0 head and neck cancer. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 4528–4535. [Google Scholar]
- Caldonazzi, N.; Rizzo, P.C.; Eccher, A.; Girolami, I.; Fanelli, G.N.; Naccarato, A.G.; Bonizzi, G.; Fusco, N.; d’Amati, G.; Scarpa, A.; et al. Value of Artificial Intelligence in Evaluating Lymph Node Metastases. Cancers 2023, 15, 2491. [Google Scholar] [CrossRef] [PubMed]
- Sumi, M.; Sato, S.; Nakamura, T. Extranodal spread of primary and secondary metastatic nodes: The dominant risk factor of survival in patients with head and neck squamous cell carcinoma. PLoS ONE 2017, 12, e0183611. [Google Scholar] [CrossRef] [PubMed]
- New Garcia, J.; Lopez, M.; Lopez, L.; Bague, S.; Granell, E.; Quer, M.; Leon, X. Validation of the pathological classification of lymph node metastasis for head and neck tumors according to the 8th edition of the TNM Classification of Malignant Tumors. Oral Oncol. 2017, 70, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Sumi, M. Nodal imaging in the neck: Recent advances in US, CT and MR imaging of metastatic nodes. Eur. Radiol. 2007, 17, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Kelly, H.R.; Curtin, H.D. Chapter 2 Squamous Cell Carcinoma of the Head and Neck—Imaging Evaluation of Regional Lymph Nodes and Implications for Management. Semin. Ultrasound CT MRI 2017, 38, 466–478. [Google Scholar] [CrossRef]
- Junn, J.C.; Soderlund, K.A.; Glastonbury, C.M. Imaging of Head and Neck Cancer With CT, MRI, and US. Semin. Nucl. Med. 2021, 51, 3–12. [Google Scholar] [CrossRef]
- Dong, F.; Tao, C.; Wu, J.; Su, Y.; Wang, Y.; Wang, Y.; Guo, C.; Lyu, P. Author correction: Detection of cervical lymph node metastasis from oral cavity cancer using a non-radiating, noninvasive digital infrared thermal imaging system. Sci. Rep. 2018, 8, 7219. [Google Scholar] [CrossRef]
- Luo, Y.H.; Mei, X.L.; Liu, Q.R.; Jiang, B.; Zhang, S.; Zhang, K.; Wu, X.; Luo, Y.M.; Li, Y.J. Diagnosing cervical lymph node metastasis in oral squamous cell carcinoma based on third-generation dual-source, dual-energy computed tomography. Eur. Radiol. 2023, 33, 162–171. [Google Scholar] [CrossRef]
- Baik, S.H.; Seo, J.W.; Kim, J.H.; Lee, S.K.; Choi, E.C.; Kim, J. Prognostic value of cervical nodal necrosis observed in preoperative CT and MRI of patients with tongue squamous cell carcinoma and cervical node metastases: A retrospective study. Am. J. Roentgenol. 2019, 213, 437–443. [Google Scholar] [CrossRef]
- Ariji, Y.; Fukuda, M.; Nozawa, M.; Kuwada, C.; Goto, M.; Ishibashi, K.; Nakayama, A.; Sugita, Y.; Nagao, T.; Ariji, E. Automatic detection of cervical lymph nodes in patients with oral squamous cell carcinoma using a deep learning technique: A preliminary study. Oral Radiol. 2021, 37, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Tang, X.; Yang, Y.; Zhang, C. 18FDG-PET/CT for the detection of regional nodal metastasis in patients with head and neck cancer: A meta-analysis. Oral Oncol. 2015, 51, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Roh, J.L.; Park, J.P.; Kim, J.S.; Lee, J.H.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. 18F fluorodeoxyglucose PET/CT in head and neck squamous cell carcinoma with negative neck palpation findings: A prospective study. Radiology 2014, 271, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Bianchini, C.; Caracciolo, M.; Urso, L.; Ciorba, A.; Bonsembiante, A.; Migliorelli, A.; Corazzi, V.; Carandina, I.; Ortolan, N.; Cittanti, C.; et al. Role of 18F-FDG PET/CT in evaluating lymph node status in patients with head and neck squamous cell carcinoma. Acta Otorhinolaryngol. Ital. 2023, 43, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Szyszko, T.A.; Cook, G.J.R. PET/CT and PET/MRI in head and neck malignancy. Clin. Radiol. 2018, 73, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Samolyk-Kogaczewska, N.; Sierko, E.; Dziemianczyk-Pakiela, D.; Nowaszewska, K.B.; Lukasik, M.; Reszec, J. Usefulness of hybrid PET/MRI in clinical evaluation of head and neck cancer patients. Cancers 2020, 12, 511. [Google Scholar] [CrossRef]
- Sumi, M.; Ohki, M.; Nakamura, T. Comparison of Sonography and CT for Differentiating Benign from Malignant Cervical Lymph Nodes in Patients with Squamous Cell Carcinoma of the Head and Neck. Am. J. Roentgenol. 2001, 176, 1019–1024. [Google Scholar] [CrossRef]
- Kawashima, Y.; Miyakoshi, M.; Kawabata, Y.; Indo, H. Efficacy of texture analysis of ultrasonographic images in the differentiation of metastatic and non-metastatic cervical lymph nodes in patients with squamous cell carcinoma of the tongue. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2023, 136, 247–254. [Google Scholar] [CrossRef]
- Zhu, Y.; Meng, Z.; Fan, X.; Duan, Y.; Jia, Y.; Dong, T.; Wang, Y.; Song, J.; Tian, J.; Wang, K.; et al. Deep learning radiomics of dual-modality ultrasound images for hierarchical diagnosis of unexplained cervical lymphadenopathy. BMC Med. 2022, 20, 269. [Google Scholar] [CrossRef]
- Richards, P.S.; Peacock, T.E. The role of ultrasound in the detection of cervical lymph node metastases in clinically N0 squamous cell carcinoma of the head and neck. Cancer Imag. 2007, 7, 167–178. [Google Scholar] [CrossRef]
- Chawla, S.; Loevner, L.; Mohan, S.; Lin, A.; Sehgal, C.M.; Poptani, H. Dynamic contrast-enhanced MRI and Doppler sonography in patients with squamous cell carcinoma of head and neck treated with induction chemotherapy. J. Clin. Ultrasound 2022, 50, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Kong, D.; Xu, X.; Hu, S.; Li, Z.; Tian, J. Deep learning-based classification of breast lesions using dynamic ultrasound video. Eur. J. Radiol. 2023, 165, 110885. [Google Scholar] [CrossRef] [PubMed]
- Chikui, T.; Yonetsu, K.; Nakamura, T. Multivariate feature analysis of sonographic findings of metastatic cervical lymph nodes: Contribution of blood flow features revealed by power Doppler sonography for predicting metastasis. Am. J. Neuroradiol. 2000, 21, 561–567. [Google Scholar]
- Tomita, H.; Yamashiro, T.; Heianna, J.; Nakasone, T.; Kobayashi, T.; Mishiro, S.; Hirahara, D.; Takaya, E.; Mimura, H.; Murayama, S.; et al. Deep Learning for the Preoperative Diagnosis of Metastatic Cervical Lymph Nodes on Contrast-Enhanced Computed ToMography in Patients with Oral Squamous Cell Carcinoma. Cancers 2021, 13, 600. [Google Scholar] [CrossRef]
- Santer, M.; Kloppenburg, M.; Gottfried, T.M.; Runge, A.; Schmutzhard, J.; Vorbach, S.M.; Mangesius, J.; Riedl, D.; Mangesius, S.; Widmann, G.; et al. Current Applications of Artificial Intelligence to Classify Cervical Lymph Nodes in Patients with Head and Neck Squamous Cell Carcinoma-A Systematic Review. Cancers 2022, 14, 5397. [Google Scholar] [CrossRef] [PubMed]
- Ariji, Y.; Kise, Y.; Fukuda, M.; Kuwada, C.; Ariji, E. Segmentation of metastatic cervical lymph nodes from CT images of oral cancers using deep-learning technology. Dentomaxillofac. Radiol. 2022, 51, 20210515. [Google Scholar] [CrossRef] [PubMed]
- Ariji, Y.; Fukuda, M.; Kise, Y.; Nozawa, M.; Yanashita, Y.; Fujita, H.; Katsumata, A.; Ariji, E. Contrast-enhanced computed tomography image assessment of cervical lymph node metastasis in patients with oral cancer by using a deep learning system of artificial intelligence. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Choi, E.J.; Choi, Y.; Zhang, H.; Jin, G.Y.; Ko, S.B. Breast Cancer Classification in Automated Breast Ultrasound Using Multiview Convolutional Neural Network with Transfer Learning. Ultrasound Med. Biol. 2020, 46, 1119–1132. [Google Scholar] [CrossRef]
- Hejduk, P.; Marcon, M.; Unkelbach, J.; Ciritsis, A.; Rossi, C.; Borkowski, K.; Boss, A. Fully automatic classification of automated breast ultrasound (ABUS) imaging according to BI-RADS using a deep convolutional neural network. Eur. Radiol. 2022, 32, 4868–4878. [Google Scholar] [CrossRef]
- Zhang, J.; Tao, X.; Jiang, Y.; Wu, X.; Yan, D.; Xue, W.; Zhuang, S.; Chen, L.; Luo, L.; Ni, D. Application of Convolution Neural Network Algorithm Based on Multicenter ABUS Images in Breast Lesion Detection. Front. Oncol. 2022, 12, 938413. [Google Scholar] [CrossRef]
- Quan, M.Y.; Huang, Y.X.; Wang, C.Y.; Zhang, Q.; Chang, C.; Zhou, S.C. Deep learning radiomics model based on breast ultrasound video to predict HER2 expression status. Front. Endocrinol. 2023, 14, 1144812. [Google Scholar] [CrossRef] [PubMed]
- Kise, Y.; Kuwada, C.; Ariji, Y.; Naitoh, M.; Ariji, E. Preliminary Study on the Diagnostic Performance of a Deep Learning System for Submandibular Gland Inflammation Using Ultrasonography Images. J. Clin. Med. 2021, 10, 4508. [Google Scholar] [CrossRef] [PubMed]
- Kise, Y.; Shimizu, M.; Ikeda, H.; Fujii, T.; Kuwada, C.; Nishiyama, M.; Funakoshi, T.; Ariji, Y.; Fujita, H.; Katsumata, A.; et al. Usefulness of a deep learning system for diagnosing Sjogren’s syndrome using ultrasonography images. Dentomaxillofac. Radiol. 2020, 49, 20190348. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Tan, G.; Zhu, N.; Chen, Z.; Yang, Y.; Wen, H.; Li, K. CacheTrack-YOLO: Real-Time Detection and Tracking for Thyroid Nodules and Surrounding Tissues in Ultrasound Videos. IEEE J. Biomed. Health Inform. 2021, 25, 3812–3823. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Qiu, Y.; Han, L.; Liao, G.; Zhuang, Y.; Ma, B.; Luo, Y.; Lin, J.; Chen, K. A lightweight network for automatic thyroid nodules location and recognition with high speed and accuracy in ultrasound images. J. Xray Sci. Technol. 2022, 30, 967–981. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Mutasa, S.; Liu, M.Z.; Nemer, J.; Sun, M.; Siddique, M.; Desperito, E.; Jambawalikar, S.; Ha, R.S. Deep learning prediction of axillary lymph node status using ultrasound images. Comput. Biol. Med. 2022, 143, 105250. [Google Scholar] [CrossRef]
- Lee, J.H.; Baek, J.H.; Kim, J.H.; Shim, W.H.; Chung, S.R.; Choi, Y.J.; Lee, J.H. Deep Learning-Based Computer-Aided Diagnosis System for Localization and Diagnosis of Metastatic Lymph Nodes on Ultrasound: A Pilot Study. Thyroid 2018, 28, 1332–1338. [Google Scholar] [CrossRef]
- Kann, B.H.; Aneja, S.; Loganadane, G.V.; Kelly, J.R.; Smith, S.M.; Decker, R.H.; Yu, J.B.; Park, H.S.; Yarbrough, W.G.; Malhotra, A.; et al. Pretreatment identification of head and neck cancer nodal metastasis and extranodal extension using deep learning neural networks. Sci. Rep. 2018, 8, 14036. [Google Scholar] [CrossRef]
- Jiang, P.; Ergu, D.; Liu, F.; Cai, Y.; Ma, B. A Review of Yolo Algorithm Developments. Proc. Comput. Sci. 2022, 199, 1066–1073. [Google Scholar] [CrossRef]
- Wang, C.Y.; Bochkovskiy, A.; Liao, H.Y.M. YOLOv7: Trainable bag-of-freebies sets new state-of-the-art for real-time object detectors. arXiv 2022, arXiv:2207.02696v1. [Google Scholar]
- Soeb, M.J.A.; Jubayer, M.F.; Tarin, T.A.; Al Mamun, M.R.; Ruhad, F.M.; Parven, A.; Mubarak, N.M.; Karri, S.L.; Meftaul, I.M. Tea leaf disease detection and identification based on YOLOv7 (YOLO-T). Sci. Rep. 2023, 13, 6078. [Google Scholar] [CrossRef] [PubMed]
- Mortada, M.J.; Tomassini, S.; Anbar, H.; Morettini, M.; Burattini, L.; Sbrollini, A. Segmentation of Anatomical Structures of the Left Heart from Echocardiographic Images Using Deep Learning. Diagnostics 2023, 13, 1683. [Google Scholar] [CrossRef] [PubMed]
- Oka, S.; Nozaki, K.; Hayashi, M. An efficient annotation method for image recognition of dental instruments. Sci. Rep. 2023, 13, 169. [Google Scholar] [CrossRef] [PubMed]
- Abdusalomov, A.B.; Mukhiddinov, M.; Whangbo, T.K. Brain tumor detection based on deep learning approaches and magnetic resonance imaging. Cancers 2023, 15, 4172. [Google Scholar] [CrossRef] [PubMed]
- Chang, B.R.; Tsai, H.F.; Hsieh, C.W. Accelerating the response of self-driving control by using rapid object detection and steering angle prediction. Electronics 2023, 12, 2161. [Google Scholar] [CrossRef]
- Hu, Q.; Whitney, H.M.; Li, H.; Ji, Y.; Liu, P.; Giger, M.L. Improved Classification of Benign and Malignant Breast Lesions Using Deep Feature Maximum Intensity Projection MRI in Breast Cancer Diagnosis Using Dynamic Contrast-enhanced MRI. Radiol. Artif. Intell. 2021, 3, e200159. [Google Scholar] [CrossRef]
- Shi, Y.; Tang, H.; Baine, M.J.; Hollingsworth, M.A.; Du, H.; Zheng, D.; Zhang, C.; Yu, H. 3DGAUnet: 3D generative adversarial networks with a 3D U-net based generator to achieve the accurate and effective synthesis of clinical tumor image data for pancreatic cancer. Cancers 2023, 15, 5496. [Google Scholar] [CrossRef]
- Zhang, Z.; Ma, L.; Wei, C.; Yang, M.; Qin, S.; Lv, X.; Ze Zhang, Z. Cotton Fusarium wilt diagnosis based on generative adversarial networks in small samples. Front. Plant Sci. 2023, 14, 1290774. [Google Scholar] [CrossRef]
- Hu, P.; Cai, C.; Yi, H.; Zhao, J.; Feng, Y.; Wang, Q. Aiding airway obstruction diagnosis with computational fluid dynamics and convolutional neural network: A new perspective and numerical case study. J. Fluids Eng. 2022, 144, 081206. [Google Scholar] [CrossRef]
- Rutkowski, D.R.; Roldán-Alzate, A.; Johnson, K.M. Enhancement of cerebrovascular 4D flow MRI velocity fields using machine learning and computational fluid dynamics simulation data. Sci. Rep. 2021, 11, 10240. [Google Scholar] [CrossRef]
- Hao, W.; Ren, C.; Han, M.; Zhang, L.; Li, F.; Liu, Z. Cattle body detection based on YOLOv5-EMA for precision livestock farming. Animals 2023, 13, 3535. [Google Scholar] [CrossRef] [PubMed]
- Suri, J.S.; Agarwal, S.; Chabert, G.L.; Carriero, A.; Paschè, A.; Danna, P.S.C.; Saba, L.; Mehmedovic, A.; Faa, G.; Singh, I.M.; et al. COVLIAS 2.0-cXAI: Cloud-based explainable deep learning system for COVID-19 lesion localization in computed tomography scans. Diagnostics 2022, 12, 1482. [Google Scholar] [CrossRef] [PubMed]
- Vrinceanu, D.; Dumitru, M.; Cergan, R.; Anghel, A.G.; Patrascu, E.T.; Caius Codrut Sarafoleanu, C.C.; Costache, A. Correlations between ultrasonography performed by the ENT specialist and pathologic findings in the management of three cases with thyroglossal duct cyst. Med. Ultrason. 2018, 20, 524–526. [Google Scholar] [CrossRef] [PubMed]
- Moshtaghi, O.; Haidar, Y.M.; Mahmoodi, A.; Tjoa, T.; Armstrong, W.B. The role of in-office ultrasound in the diagnosis of neck masses. Otolaryngol. Head Neck Surg. 2017, 157, 58–61. [Google Scholar] [CrossRef]
- Pang, D.; Guan, Z.; Luo, T.; Su, W.; Dou, R. Real-time detection of road manhole covers with a deep learning model. Sci. Rep. 2023, 13, 16479. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Training Datasets | Validation Datasets | Testing Datasets | Total | |
|---|---|---|---|---|
| No. of images | 324 | 92 | 46 | 462 |
| No. of LNs | 365 | 116 | 59 | 540 |
| No. of metastatic LNs | 183 | 50 | 28 | 261 |
| No. of non-metastatic LNs | 182 | 66 | 31 | 279 |
| Detection Result | ||||
|---|---|---|---|---|
| Detected as Metastatic LNs | Not Detected as Metastatic LNs | |||
| Pathology | Metastatic LNs | N (A + B) = 28 | True positive: A | False negative: B |
| Non-metastatic LNs | N (C + D) = 31 | False positive: C | True negative: D | |
| Non-LN areas detected as metastatic LNs | False positive for non-LN area: E | |||
| B-mode images | B-mode model-1 | B-mode model-2 | Radiologists | Residents |
| Recall | 0.75 | 0.75 | 0.821 | 0.536 |
| Precision | 0.618 | 0.724 | 0.958 | 0.517 |
| F1-score | 0.677 | 0.737 | 0.885 | 0.526 |
| False-positive rate for non-LN area | 0.087 | 0.043 | 0 | 0.261 |
| Accuracy | 0.729 | 0.78 | 0.898 | 0.746 |
| AUC (95% CI) | 0.73 (0.601–0.829) | 0.778 (0.652–0.868) | 0.895 (0.786–0.951) | 0.736 (0.62–0.826) |
| D-mode images | D-mode model-1 | D-mode model-2 | Radiologists | Residents |
| Recall | 0.821 | 0.75 | 0.75 | 0.714 |
| Precision | 0.719 | 0.84 | 0.875 | 0.606 |
| F1-score | 0.767 | 0.792 | 0.808 | 0.656 |
| False-positive rate for non-LN area | 0.022 | 0 | 0 | 0.022 |
| Accuracy | 0.78 | 0.814 | 0.831 | 0.661 |
| AUC (95% CI) | 0.782 (0.657–0.870) | 0.81 (0.689–0.892) | 0.827 (0.707–0.904) | 0.664 (0.533–0.773) |
| Comparison of accuracy, recall, and AUC between B-mode and D-mode images | ||||
| p value for recall * | 0.687 | 1 | 0.687 | 0.063 |
| p value for accuracy * | 0.549 | 0.727 | 0.289 | 0.359 |
| p value for AUC ** | 0.365 | 0.518 | 0.169 | 0.270 |
| B-mode images | B-mode model-1 | B-mode model-2 | Radiologists | Residents | ||||
| B-mode model-1 | Recall | 1 | 0.727 | 0.146 | ||||
| Accuracy/AUC | ||||||||
| B-mode model-2 | 0.250/0.073 | Recall | 0.727 | 0.146 | ||||
| Accuracy/AUC | ||||||||
| Radiologists | 0.031/0.0166 | 0.118/0.0747 | Recall | 0.008 | ||||
| Accuracy/AUC | ||||||||
| Residents | 1/0.9351 | 0.804/0.5242 | 0.012/0.0022 | Recall | ||||
| Accuracy/AUC | ||||||||
| D-mode images | D-mode model-1 | D-mode model-2 | Radiologists | Residents | ||||
| D-mode model-1 | Recall | 0.5 | 0.727 | 0.508 | ||||
| Accuracy/AUC | ||||||||
| D-mode model-2 | 0.687/0.4645 | Recall | 1 | 1 | ||||
| Accuracy/AUC | ||||||||
| Radiologists | 0.607/0.4914 | 1/0.7951 | Recall | 1 | ||||
| Accuracy/AUC | ||||||||
| Residents | 0.230/0.1591 | 0.093/0.0615 | 0.064/0.0419 | Recall | ||||
| Accuracy/AUC | ||||||||
| B-mode images | B-mode model-1 | B-mode model-2 | Radiologists | Residents |
| Level I | 0.909 | 0.909 | 0.909 | 0.364 |
| Level II | 0.8 | 0.8 | 0.9 | 0.7 |
| Level III + IV | 0.429 | 0.429 | 0.571 | 0.571 |
| D-mode images | D-mode model-1 | D-mode model-2 | Radiologists | Residents |
| Level I | 0.727 | 0.636 | 0.727 | 0.636 |
| Level II | 1 | 1 | 1 | 0.7 |
| Level III + IV | 0.714 | 0.571 | 0.429 | 0.857 |
| B-Mode Images | Kappa Value | D-Mode Images | Kappa Value |
|---|---|---|---|
| B-mode model-1 vs. B-mode model-2 | 0.898 | D-mode model-1 vs. D-mode model-2 | 0.798 |
| B-mode model-1 vs. Radiologists | 0.392 | D-mode model-1 vs. Radiologists | 0.496 |
| B-mode model-1 vs. Residents | 0.361 | D-mode model-1 vs. Residents | 0.149 |
| B-mode model-2 vs. Radiologists | 0.483 | D-mode model-2 vs. Radiologists | 0.546 |
| B-mode mode-2 vs. Residents | 0.437 | D-mode model-2 vs. Residents | 0.230 |
| Radiologists vs. Residents | 0.595 | Radiologists vs. Residents | 0.199 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eida, S.; Fukuda, M.; Katayama, I.; Takagi, Y.; Sasaki, M.; Mori, H.; Kawakami, M.; Nishino, T.; Ariji, Y.; Sumi, M. Metastatic Lymph Node Detection on Ultrasound Images Using YOLOv7 in Patients with Head and Neck Squamous Cell Carcinoma. Cancers 2024, 16, 274. https://doi.org/10.3390/cancers16020274
Eida S, Fukuda M, Katayama I, Takagi Y, Sasaki M, Mori H, Kawakami M, Nishino T, Ariji Y, Sumi M. Metastatic Lymph Node Detection on Ultrasound Images Using YOLOv7 in Patients with Head and Neck Squamous Cell Carcinoma. Cancers. 2024; 16(2):274. https://doi.org/10.3390/cancers16020274
Chicago/Turabian StyleEida, Sato, Motoki Fukuda, Ikuo Katayama, Yukinori Takagi, Miho Sasaki, Hiroki Mori, Maki Kawakami, Tatsuyoshi Nishino, Yoshiko Ariji, and Misa Sumi. 2024. "Metastatic Lymph Node Detection on Ultrasound Images Using YOLOv7 in Patients with Head and Neck Squamous Cell Carcinoma" Cancers 16, no. 2: 274. https://doi.org/10.3390/cancers16020274
APA StyleEida, S., Fukuda, M., Katayama, I., Takagi, Y., Sasaki, M., Mori, H., Kawakami, M., Nishino, T., Ariji, Y., & Sumi, M. (2024). Metastatic Lymph Node Detection on Ultrasound Images Using YOLOv7 in Patients with Head and Neck Squamous Cell Carcinoma. Cancers, 16(2), 274. https://doi.org/10.3390/cancers16020274