
In Silico Comparison of Three Different Beam Arrangements for Intensity-Modulated Proton Therapy for Postoperative Whole Pelvic Irradiation of Prostate Cancer
 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Simulation
2.2. Volume Delineation
2.3. Treatment Planning
2.4. Statistical Analysis
3. Results
3.1. Target Coverage
3.2. Organ at Risk Objectives
3.3. Genitourinary Organs at Risk
3.4. Gastrointestinal Organs at Risk
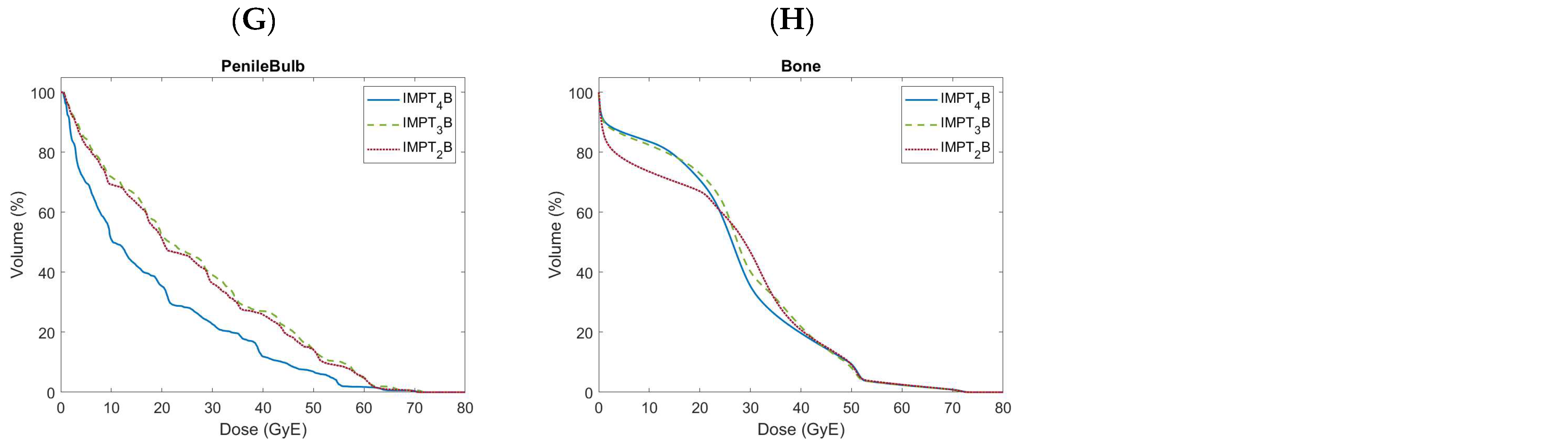
3.5. Bony Organs at Risk
3.6. Other Organs at Risk
4. Discussion
4.1. Beam Arrangements
4.2. Correlation between Dosimetric Outcomes and Toxicity
4.3. Robustness
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RP | Radical prostatectomy |
| RT | Radiation therapy |
| ADT | Androgen deprivation therapy |
| IMRT | Intensity-modulated photon radiation therapy |
| IMPT | Intensity-modulated proton therapy |
| CTV | Clinical target volume |
| OAR | Organ at risk |
| MRI | Magnetic resonance imaging |
| CT | Computed tomography |
| PTV | Planning target volume |
| GyE | Gy radiobiologic equivalent |
| RBE | Relative biological effectiveness |
| DVH | Dose-volume histogram |
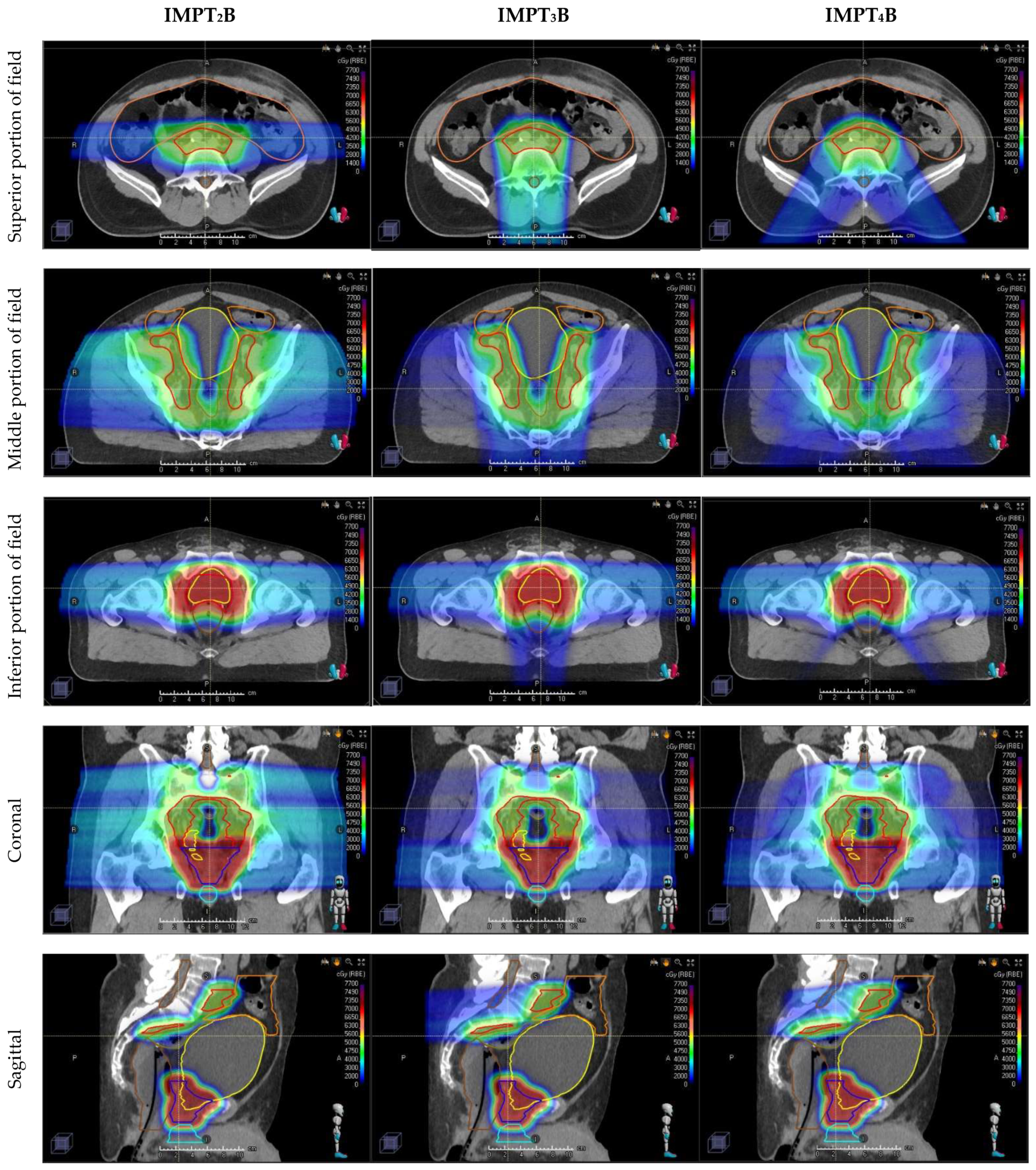
| IMPT2B | two-field IMPT beam arrangement using opposed laterals |
| IMPT3B | three-field IMPT beam arrangement using opposed laterals inferiorly matched to a Posterior–anterior beam superiorly |
| PA | Posterior–anterior |
| IMPT4B | four-field IMPT beam arrangement using opposed laterals inferiorly matched to 2 Posterior oblique beams superiorly |
| PO | Posterior oblique |
| SFO | Single-field optimization |
| GPU | Graphics processing units |
| AO | Anterior oblique |
| WPRT | Whole pelvis radiation therapy |
| GI | Gastrointestinal |
| GU | Genitourinary |
| HR | Hazard ratio |
References
- American Cancer Society. Cancer Facts and Figures 2021. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf (accessed on 11 October 2021).
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef]
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer Incidence and Mortality Rates and Trends—An Update. Cancer Epidemiol. Biomark. Prev. 2016, 25, 16–27. [Google Scholar] [CrossRef]
- Tzelepi, V. Prostate Cancer: Pathophysiology, Pathology and Therapy. Cancers 2022, 15, 281. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, S.; Vourda, A.; Syggelos, S.; Gyftopoulos, K. Cell Plasticity and Prostate Cancer: The Role of Epithelial-Mesenchymal Transition in Tumor Progression, Invasion, Metastasis and Cancer Therapy Resistance. Cancers 2021, 13, 2795. [Google Scholar] [CrossRef]
- Sanda, M.G.; Dunn, R.L.; Michalski, J.; Sandler, H.M.; Northouse, L.; Hembroff, L.; Lin, X.; Greenfield, T.K.; Litwin, M.S.; Saigal, C.S.; et al. Quality of life and satisfaction with outcome among prostate-cancer survivors. N. Engl. J. Med. 2008, 358, 1250–1261. [Google Scholar] [CrossRef]
- Donovan, J.L.; Hamdy, F.C.; Lane, J.A.; Mason, M.; Metcalfe, C.; Walsh, E.; Blazeby, J.M.; Peters, T.J.; Holding, P.; Bonnington, S.; et al. Patient-Reported Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N. Engl. J. Med. 2016, 375, 1425–1437. [Google Scholar] [CrossRef]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [PubMed]
- Tendulkar, R.D.; Agrawal, S.; Gao, T.; Efstathiou, J.A.; Pisansky, T.M.; Michalski, J.M.; Koontz, B.F.; Hamstra, D.A.; Feng, F.Y.; Liauw, S.L.; et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy After Radical Prostatectomy. J. Clin. Oncol. 2016, 34, 3648–3654. [Google Scholar] [CrossRef]
- Thompson, I.M.; Tangen, C.M.; Paradelo, J.; Lucia, M.S.; Miller, G.; Troyer, D.; Messing, E.; Forman, J.; Chin, J.; Swanson, G.; et al. Adjuvant radiotherapy for pathologically advanced prostate cancer: A randomized clinical trial. JAMA 2006, 296, 2329–2335. [Google Scholar] [CrossRef]
- Thompson, I.M.; Tangen, C.M.; Paradelo, J.; Lucia, M.S.; Miller, G.; Troyer, D.; Messing, E.; Forman, J.; Chin, J.; Swanson, G.; et al. Adjuvant radiotherapy for pathological T3N0M0 prostate cancer significantly reduces risk of metastases and improves survival: Long-term followup of a randomized clinical trial. J. Urol. 2009, 181, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Bolla, M.; van Poppel, H.; Collette, L.; van Cangh, P.; Vekemans, K.; Da Pozzo, L.; de Reijke, T.M.; Verbaeys, A.; Bosset, J.F.; van Velthoven, R.; et al. Postoperative radiotherapy after radical prostatectomy: A randomised controlled trial (EORTC trial 22911). Lancet 2005, 366, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Bolla, M.; van Poppel, H.; Tombal, B.; Vekemans, K.; Da Pozzo, L.; de Reijke, T.M.; Verbaeys, A.; Bosset, J.F.; van Velthoven, R.; Colombel, M.; et al. Postoperative radiotherapy after radical prostatectomy for high-risk prostate cancer: Long-term results of a randomised controlled trial (EORTC trial 22911). Lancet 2012, 380, 2018–2027. [Google Scholar] [CrossRef] [PubMed]
- Wiegel, T.; Bottke, D.; Steiner, U.; Siegmann, A.; Golz, R.; Störkel, S.; Willich, N.; Semjonow, A.; Souchon, R.; Stöckle, M.; et al. Phase III postoperative adjuvant radiotherapy after radical prostatectomy compared with radical prostatectomy alone in pT3 prostate cancer with postoperative undetectable prostate-specific antigen: ARO 96-02/AUO AP 09/95. J. Clin. Oncol. 2009, 27, 2924–2930. [Google Scholar] [CrossRef] [PubMed]
- Wiegel, T.; Bartkowiak, D.; Bottke, D.; Bronner, C.; Steiner, U.; Siegmann, A.; Golz, R.; Störkel, S.; Willich, N.; Semjonow, A.; et al. Adjuvant radiotherapy versus wait-and-see after radical prostatectomy: 10-year follow-up of the ARO 96-02/AUO AP 09/95 trial. Eur. Urol. 2014, 66, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Morgan, S.C.; Waldron, T.S.; Eapen, L.; Mayhew, L.A.; Winquist, E.; Lukka, H.; Genitourinary Cancer Disease Site Group of the Cancer Care Ontario Program in Evidence-based Care. Adjuvant radiotherapy following radical prostatectomy for pathologic T3 or margin-positive prostate cancer: A systematic review and meta-analysis. Radiother. Oncol. 2008, 88, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Daly, T.; Hickey, B.E.; Lehman, M.; Francis, D.P.; See, A.M. Adjuvant radiotherapy following radical prostatectomy for prostate cancer. Cochrane Database Syst. Rev. 2011, CD007234. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.; Karrison, T.G.; Balogh, A.G.; Gomella, L.G.; Low, D.A.; Bruner, D.W.; Wefel, J.S.; Martin, A.G.; Michalski, J.M.; Angyalfi, S.J.; et al. The addition of androgen deprivation therapy and pelvic lymph node treatment to prostate bed salvage radiotherapy (NRG Oncology/RTOG 0534 SPPORT): An international, multicentre, randomised phase 3 trial. Lancet 2022, 399, 1886–1901. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.R. Radiological use of fast protons. Radiology 1946, 47, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, T.J.; Routman, D.M.; Schultz, H.; Harmsen, W.S.; Corbin, K.S.; Wong, W.W.; Choo, R. IMPT versus VMAT for Pelvic Nodal Irradiation in Prostate Cancer: A Dosimetric Comparison. Int. J. Part. Ther. 2019, 5, 11–23. [Google Scholar] [CrossRef]
- Santos, P.M.G.; Barsky, A.R.; Hwang, W.T.; Deville, C.; Wang, X.; Both, S.; Bekelman, J.E.; Christodouleas, J.P.; Vapiwala, N. Comparative toxicity outcomes of proton-beam therapy versus intensity-modulated radiotherapy for prostate cancer in the postoperative setting. Cancer 2019, 125, 4278–4293. [Google Scholar] [CrossRef] [PubMed]
- Gogineni, E.; Cruickshank, I.K.; Chen, H.; Halthore, A.; Li, H.; Deville, C. In silico comparison of whole pelvis intensity-modulated photon versus proton therapy for the postoperative management of prostate cancer. Acta Oncol. 2023, 62, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.A.; Paulson, E.; Davis, B.J.; Spratt, D.E.; Morgan, T.M.; Dearnaley, D.; Tree, A.C.; Efstathiou, J.A.; Harisinghani, M.; Jani, A.B.; et al. NRG Oncology Updated International Consensus Atlas on Pelvic Lymph Node Volumes for Intact and Postoperative Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.; Bluett, J.; Amos, R.; Levy, L.; Choi, S.; Nguyen, Q.N.; Zhu, X.R.; Gillin, M.; Lee, A. Spot scanning proton beam therapy for prostate cancer: Treatment planning technique and analysis of consequences of rotational and translational alignment errors. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Kirk, M.L.; Tang, S.; Zhai, H.; Vapiwala, N.; Deville, C.; James, P.; Bekelman, J.E.; Christodouleas, J.P.; Tochner, Z.; Both, S. Comparison of prostate proton treatment planning technique, interfraction robustness, and analysis of single-field treatment feasibility. Pract. Radiat. Oncol. 2015, 5, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Fang, P.; Mick, R.; Deville, C.; Both, S.; Bekelman, J.E.; Christodouleas, J.P.; Guzzo, T.J.; Tochner, Z.; Hahn, S.M.; Vapiwala, N. A case-matched study of toxicity outcomes after proton therapy and intensity-modulated radiation therapy for prostate cancer. Cancer 2015, 121, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Both, S.; Bentefour, H.; Paly, J.J.; Tochner, Z.; Efstathiou, J.; Lu, H.M. Improvement of prostate treatment by anterior proton fields. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Underwood, T.; Giantsoudi, D.; Moteabbed, M.; Zietman, A.; Efstathiou, J.; Paganetti, H.; Lu, H.M. Can We Advance Proton Therapy for Prostate? Considering Alternative Beam Angles and Relative Biological Effectiveness Variations When Comparing Against Intensity Modulated Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Chera, B.S.; Vargas, C.; Morris, C.G.; Louis, D.; Flampouri, S.; Yeung, D.; Duvvuri, S.; Li, Z.; Mendenhall, N.P. Dosimetric study of pelvic proton radiotherapy for high-risk prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 994–1002. [Google Scholar] [CrossRef]
- Kuban, D.A.; Tucker, S.L.; Dong, L.; Starkschall, G.; Huang, E.H.; Cheung, M.R.; Lee, A.K.; Pollack, A. Long-term results of the M. D. Anderson randomized dose-escalation trial for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 67–74. [Google Scholar] [CrossRef]
- Tucker, S.L.; Cheung, R.; Dong, L.; Liu, H.H.; Thames, H.D.; Huang, E.H.; Kuban, D.; Mohan, R. Dose-volume response analyses of late rectal bleeding after radiotherapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.H.; Pollack, A.; Levy, L.; Starkschall, G.; Dong, L.; Rosen, I.; Kuban, D.A. Late rectal toxicity: Dose-volume effects of conformal radiotherapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 1314–1321. [Google Scholar] [CrossRef]
- Deville, C.; Jain, A.; Hwang, W.T.; Woodhouse, K.D.; Both, S.; Wang, S.; Gabriel, P.E.; Christodouleas, J.P.; Bekelman, J.; Tochner, Z.; et al. Initial report of the genitourinary and gastrointestinal toxicity of post-prostatectomy proton therapy for prostate cancer patients undergoing adjuvant or salvage radiotherapy. Acta Oncol. 2018, 57, 1506–1514. [Google Scholar] [CrossRef]
- Kavanagh, B.D.; Pan, C.C.; Dawson, L.A.; Das, S.K.; Li, X.A.; Ten Haken, R.K.; Miften, M. Radiation dose-volume effects in the stomach and small bowel. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S101–S107. [Google Scholar] [CrossRef]
- Bryant, C.; Smith, T.L.; Henderson, R.H.; Hoppe, B.S.; Mendenhall, W.M.; Nichols, R.C.; Morris, C.G.; Williams, C.R.; Su, Z.; Li, Z.; et al. Five-Year Biochemical Results, Toxicity, and Patient-Reported Quality of Life After Delivery of Dose-Escalated Image Guided Proton Therapy for Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 422–434. [Google Scholar] [CrossRef]
- Yoon, M.; Kim, D.; Shin, D.H.; Park, S.Y.; Lee, S.B.; Kim, D.Y.; Kim, J.Y.; Pyo, H.R.; Cho, K.H. Inter- and intrafractional movement-induced dose reduction of prostate target volume in proton beam treatment. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1091–1102. [Google Scholar] [CrossRef]
- Yoon, M.; Shin, D.; Kwak, J.; Park, S.; Lim, Y.K.; Kim, D.; Park, S.Y.; Lee, S.B.; Shin, K.H.; Kim, T.H.; et al. Characteristics of movement-induced dose reduction in target volume: A comparison between photon and proton beam treatment. Med. Dosim. 2009, 34, 191–201. [Google Scholar] [CrossRef]
- Trofimov, A.; Nguyen, P.L.; Efstathiou, J.A.; Wang, Y.; Lu, H.M.; Engelsman, M.; Merrick, S.; Cheng, C.W.; Wong, J.R.; Zietman, A.L. Interfractional variations in the setup of pelvic bony anatomy and soft tissue, and their implications on the delivery of proton therapy for localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 928–937. [Google Scholar] [CrossRef]
- Soukup, M.; Söhn, M.; Yan, D.; Liang, J.; Alber, M. Study of robustness of IMPT and IMRT for prostate cancer against organ movement. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Efstathiou, J.A.; Sharp, G.C.; Lu, H.M.; Ciernik, I.F.; Trofimov, A.V. Evaluation of the dosimetric impact of interfractional anatomical variations on prostate proton therapy using daily in-room CT images. Med. Phys. 2011, 38, 4623–4633. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Chen, H.; Gogineni, E.; Halthore, A.; Floreza, B.; Esho-Voltaire, T.; Weaver, A.; Alcorn, S.; Ladra, M.; Li, H.; et al. Comparing Ultra-hypofractionated Proton versus Photon Therapy in Extremity Soft Tissue Sarcoma. Int. J. Part. Ther. 2023, 9, 30–39. [Google Scholar] [CrossRef]
- Vargas, C.; Fryer, A.; Mahajan, C.; Indelicato, D.; Horne, D.; Chellini, A.; McKenzie, C.; Lawlor, P.; Henderson, R.; Li, Z.; et al. Dose-volume comparison of proton therapy and intensity-modulated radiotherapy for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 744–751. [Google Scholar] [CrossRef]
- Vees, H.; Dipasquale, G.; Nouet, P.; Zilli, T.; Cozzi, L.; Miralbell, R. Pelvic Lymph Node Irradiation Including Pararectal Sentinel Nodes for Prostate Cancer Patients: Treatment Optimization Comparing Intensity Modulated X-rays, Volumetric Modulated Arc Therapy, and Intensity Modulated Proton Therapy. Technol. Cancer Res. Treat. 2015, 14, 181–189. [Google Scholar] [CrossRef]
- Widesott, L.; Pierelli, A.; Fiorino, C.; Lomax, A.J.; Amichetti, M.; Cozzarini, C.; Soukup, M.; Schneider, R.; Hug, E.; Di Muzio, N.; et al. Helical tomotherapy vs. intensity-modulated proton therapy for whole pelvis irradiation in high-risk prostate cancer patients: Dosimetric, normal tissue complication probability, and generalized equivalent uniform dose analysis. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1589–1600. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Target/OAR | Clinical Goal | IMPT2B | IMPT3B | IMPT4B | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | St-Dev | Mean | St-Dev | Mean | St-Dev | 2B vs 3B | 2B vs 4B | 3B vs 4B | ||
| CTV_50 | V 49.0 GyE > 98.0% | 100 | 0.1 | 100 | 0.0 | 100 | 0.0 | 0.348 | 0.215 | 0.162 |
| V 50.0 GyE > 98.0% | 99.6 | 0.6 | 99.6 | 0.6 | 99.8 | 0.2 | 0.864 | 0.117 | 0.136 | |
| CTV_70 | V 68.6 GyE > 99.0% | 100 | 0.0 | 100 | 0.0 | 100 | 0.0 | N/A | N/A | N/A |
| V 70.0 GyE > 99.0% | 99.8 | 0.4 | 99.8 | 0.5 | 99.7 | 0.5 | 0.519 | 0.282 | 0.375 | |
| Bladder | V 30.0 GyE < 50.0% | 46.5 | 9.6 | 45.8 | 10.6 | 43.7 | 9.2 | 0.337 | <0.001 | 0.004 |
| V 45.0 GyE < 40.0% | 37.7 | 9.5 | 37.7 | 10.0 | 36.3 | 9.1 | 0.887 | <0.001 | 0.001 | |
| V 50.0 GyE < 35.0% | 33.8 | 9.6 | 34.1 | 9.8 | 33.3 | 9.4 | 0.274 | 0.129 | 0.002 | |
| V 65.0 GyE < 20.0% | 25.5 | 9.1 | 25.5 | 9.2 | 25.4 | 9.0 | 0.973 | 0.933 | 0.927 | |
| V 70.0 GyE < 15.0% | 21.3 | 8.4 | 21.2 | 8.4 | 22.7 | 8.6 | 0.123 | <0.001 | <0.001 | |
| Mean Dose (GyE) | 31.3 | 6.4 | 31.0 | 6.8 | 29.9 | 6.4 | 0.453 | <0.001 | 0.003 | |
| Bladderless_CTV | V 30.0 GyE < 50.0% | 36.9 | 7.6 | 36.2 | 8.2 | 33.7 | 6.5 | 0.364 | <0.001 | 0.003 |
| V 45.0 GyE < 40.0% | 26.5 | 6.0 | 26.6 | 6.5 | 24.9 | 5.4 | 0.829 | <0.001 | 0.001 | |
| V 50.0 GyE < 35.0% | 21.9 | 5.5 | 22.3 | 5.8 | 21.4 | 5.1 | 0.227 | 0.145 | 0.003 | |
| V 65.0 GyE < 20.0% | 12.0 | 3.8 | 12.0 | 3.9 | 12.0 | 3.7 | 1.000 | 0.986 | 0.979 | |
| V 70.0 GyE < 15.0% | 7.1 | 2.4 | 6.9 | 2.5 | 8.7 | 2.9 | 0.123 | <0.001 | <0.001 | |
| D 0.03 cm3 < 73.5 GyE | 72.5 | 0.6 | 72.4 | 0.5 | 73.0 | 0.3 | 0.036 | 0.002 | <0.001 | |
| Mean Dose (GyE) | 24.1 | 4.4 | 23.9 | 4.8 | 22.6 | 4.1 | 0.494 | <0.001 | 0.002 | |
| Bowel Cavity | V 15.0 GyE < 830.0 cm3 | 530.0 | 202.7 | 219.8 | 92.8 | 200.0 | 83.7 | <0.001 | <0.001 | <0.001 |
| V 30.0 GyE < 300.0 cm3 | 170.1 | 71.7 | 140.8 | 61.1 | 131.4 | 57.9 | <0.001 | <0.001 | 0.002 | |
| V 40.0 GyE < 30.0% | 6.2 | 4.1 | 5.2 | 3.6 | 4.9 | 2.9 | <0.001 | <0.001 | 0.086 | |
| V 45.0 GyE < 195.0 cm3 | 81.2 | 37.6 | 68.8 | 32.2 | 70.5 | 33.9 | <0.001 | <0.001 | 0.298 | |
| V 55.0 GyE < 20.0 cm3 | 0.7 | 2.0 | 0.7 | 2.1 | 0.8 | 2.2 | 0.446 | 0.262 | 0.510 | |
| V 60.0 GyE < 5.0 cm3 | 0.4 | 1.3 | 0.4 | 1.4 | 0.5 | 1.5 | 0.445 | 0.224 | 0.489 | |
| Mean Dose (GyE) | 8.8 | 3.3 | 4.9 | 3.1 | 4.6 | 2.6 | <0.001 | <0.001 | 0.013 | |
| Sigmoid | D 0.03 cm3 < 66.0 GyE | 59.0 | 7.1 | 58.8 | 6.9 | 56.7 | 7.0 | 0.599 | <0.001 | <0.001 |
| Rectum (anatomic) | V 40.0 GyE < 40.0% | 33.7 | 8.2 | 34.7 | 9.7 | 28.9 | 6.8 | 0.160 | <0.001 | <0.001 |
| V 50.0 GyE < 30.0% | 26.8 | 7.3 | 26.9 | 8.4 | 22.3 | 5.8 | 0.822 | <0.001 | <0.001 | |
| V 60.0 GyE < 20.0% | 19.5 | 6.0 | 19.0 | 6.5 | 15.8 | 4.6 | 0.209 | <0.001 | <0.001 | |
| V 70.0 GyE < 10.0% | 5.5 | 2.2 | 4.7 | 2.0 | 4.0 | 1.9 | <0.001 | <0.001 | 0.009 | |
| V 72.1 GyE < 0.5 cm3 | 0.1 | 0.2 | 0.1 | 0.2 | 0.0 | 0.0 | 0.102 | 0.038 | 0.266 | |
| D 0.03 cm3 < 72.1 GyE | 72.1 | 0.6 | 71.6 | 0.6 | 71.2 | 0.3 | <0.001 | <0.001 | 0.005 | |
| Mean Dose (GyE) | 27.3 | 5.2 | 29.4 | 6.0 | 24.6 | 4.5 | 0.001 | <0.001 | <0.001 | |
| Rectum (in-field) | V 40.0 GyE < 40.0% | 34.7 | 8.8 | 35.8 | 10.4 | 30.2 | 7.4 | 0.162 | <0.001 | <0.001 |
| V 50.0 GyE < 30.0% | 27.7 | 7.8 | 27.8 | 9.0 | 23.3 | 6.3 | 0.825 | <0.001 | <0.001 | |
| V 60.0 GyE < 20.0% | 20.2 | 6.4 | 19.7 | 7.0 | 16.6 | 4.9 | 0.204 | <0.001 | <0.001 | |
| V 70.0 GyE < 10.0% | 5.7 | 2.2 | 4.8 | 2.0 | 4.1 | 1.9 | 0.001 | <0.001 | 0.009 | |
| V 72.1 GyE < 0.5 cm3 | 0.1 | 0.2 | 0.1 | 0.2 | 0.0 | 0.0 | 0.114 | 0.039 | 0.270 | |
| D 0.03 cm3 < 72.1 GyE | 72.1 | 0.6 | 71.6 | 0.6 | 71.2 | 0.3 | <0.001 | <0.001 | 0.005 | |
| Mean Dose (GyE) | 28.1 | 5.5 | 30.2 | 6.3 | 25.6 | 4.8 | 0.001 | <0.001 | <0.001 | |
| Left Femoral Head | V 37.0 GyE < 50.0% | 0.9 | 1.3 | 0.1 | 0.3 | 0.1 | 0.1 | 0.004 | 0.002 | 0.470 |
| V 40.0 GyE < 40.0% | 0.2 | 0.3 | 0.0 | 0.1 | 0.0 | 0.1 | 0.016 | 0.003 | 0.788 | |
| V 50.0 GyE < 10.0% | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | N/A | N/A | N/A | |
| D 0.03 cm3 < 53.0 GyE | 40.2 | 3.2 | 35.6 | 3.4 | 34.2 | 3.9 | <0.001 | <0.001 | 0.015 | |
| Right Femoral Head | V 37.0 GyE < 50.0% | 1.0 | 1.3 | 0.2 | 0.7 | 0.0 | 0.1 | 0.009 | 0.002 | 0.312 |
| V 40.0 GyE < 40.0% | 0.1 | 0.2 | 0.1 | 0.3 | 0.0 | 0.0 | 0.546 | 0.017 | 0.361 | |
| V 50.0 GyE < 10.0% | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | N/A | N/A | N/A | |
| D 0.03 cm3 < 53.0 GyE | 40.3 | 3.3 | 36.1 | 3.5 | 34.4 | 4.1 | <0.001 | <0.001 | 0.006 | |
| Bone | V 10.0 GyE < 90.0% | 73.5 | 5.1 | 82.4 | 5.0 | 83.4 | 3.4 | <0.001 | <0.001 | 0.027 |
| V 40.0 GyE < 37.0% | 20.8 | 4.9 | 21.8 | 3.9 | 19.6 | 3.3 | 0.163 | 0.060 | 0.000 | |
| Mean Dose (GyE) | 26.0 | 2.5 | 27.5 | 2.1 | 26.6 | 1.9 | 0.001 | 0.038 | 0.001 | |
| Penile Bulb | Mean < 52.5 GyE | 23.6 | 6.2 | 23.7 | 7.3 | 22.0 | 6.6 | 0.848 | 0.003 | <0.001 |
| Skin | D 0.03 cm3 < 56.0 GyE | 36.4 | 2.4 | 36.8 | 1.5 | 31.0 | 1.7 | 0.652 | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gogineni, E.; Chen, H.; Cruickshank, I.K., Jr.; Koempel, A.; Gogineni, A.; Li, H.; Deville, C., Jr. In Silico Comparison of Three Different Beam Arrangements for Intensity-Modulated Proton Therapy for Postoperative Whole Pelvic Irradiation of Prostate Cancer. Cancers 2024, 16, 2702. https://doi.org/10.3390/cancers16152702
Gogineni E, Chen H, Cruickshank IK Jr., Koempel A, Gogineni A, Li H, Deville C Jr. In Silico Comparison of Three Different Beam Arrangements for Intensity-Modulated Proton Therapy for Postoperative Whole Pelvic Irradiation of Prostate Cancer. Cancers. 2024; 16(15):2702. https://doi.org/10.3390/cancers16152702
Chicago/Turabian StyleGogineni, Emile, Hao Chen, Ian K. Cruickshank, Jr., Andrew Koempel, Aarush Gogineni, Heng Li, and Curtiland Deville, Jr. 2024. "In Silico Comparison of Three Different Beam Arrangements for Intensity-Modulated Proton Therapy for Postoperative Whole Pelvic Irradiation of Prostate Cancer" Cancers 16, no. 15: 2702. https://doi.org/10.3390/cancers16152702
APA StyleGogineni, E., Chen, H., Cruickshank, I. K., Jr., Koempel, A., Gogineni, A., Li, H., & Deville, C., Jr. (2024). In Silico Comparison of Three Different Beam Arrangements for Intensity-Modulated Proton Therapy for Postoperative Whole Pelvic Irradiation of Prostate Cancer. Cancers, 16(15), 2702. https://doi.org/10.3390/cancers16152702