
Correlation of pN Stage and Hypoechogenicity with Tumour Encapsulation and Vascular Invasion in Thyroid Cancer (TC): A Comprehensive Analysis and Clinical Outcomes



Abstract
Simple Summary
Abstract
1. Introduction
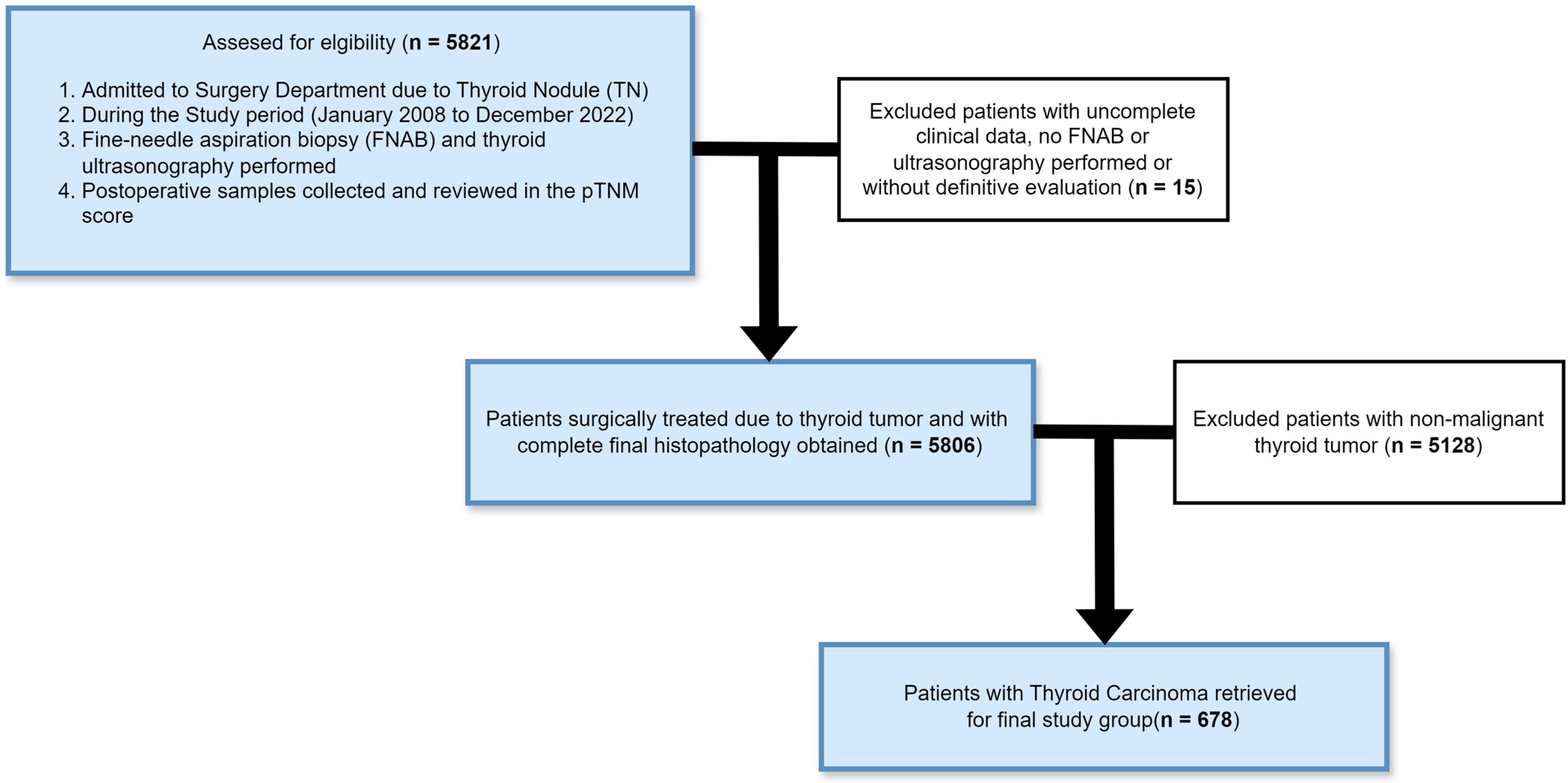
2. Materials and Methods
Statistical Analysis
3. Results
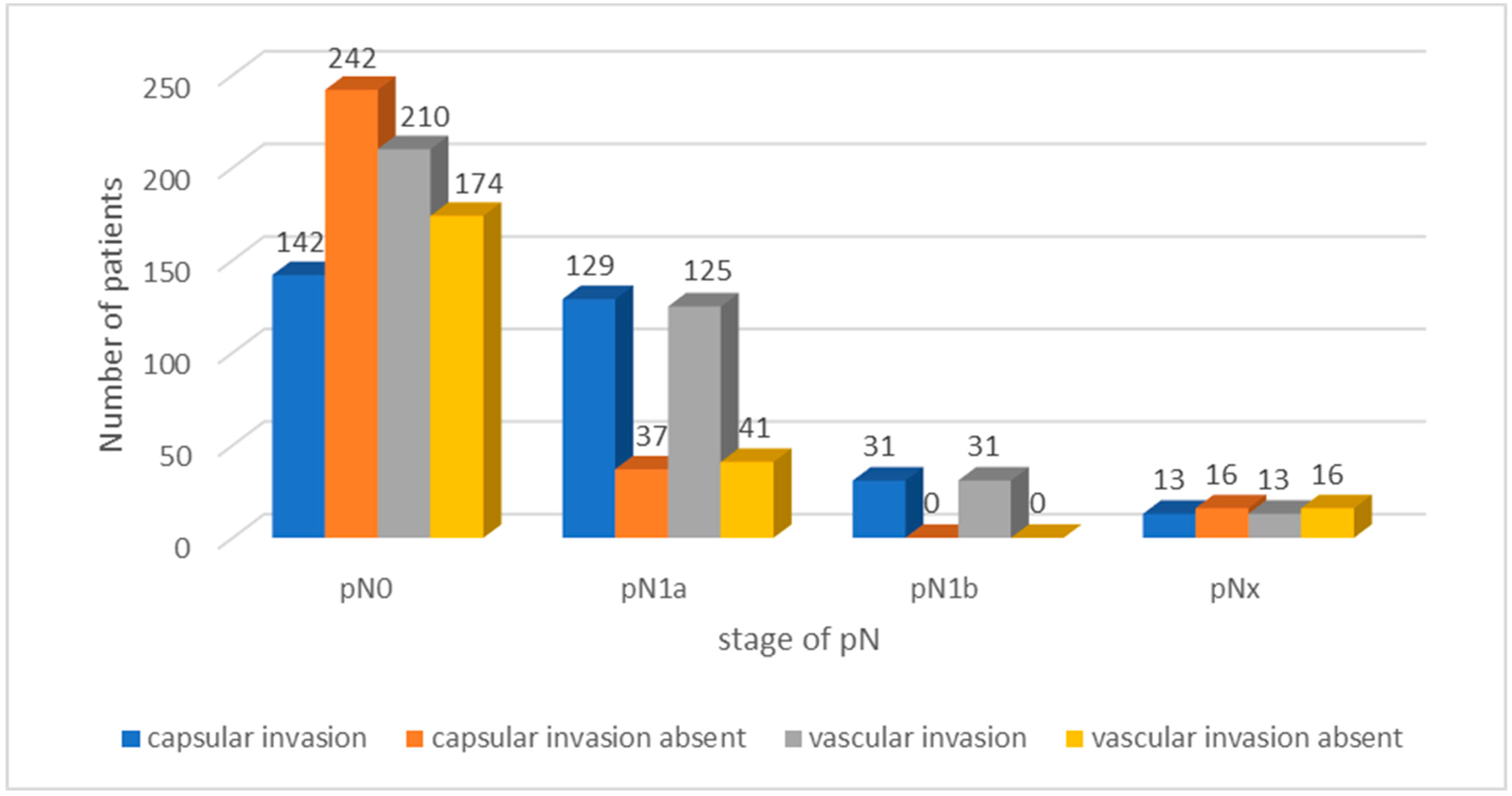
3.1. Tumour Encapsulation and Vascular Invasion
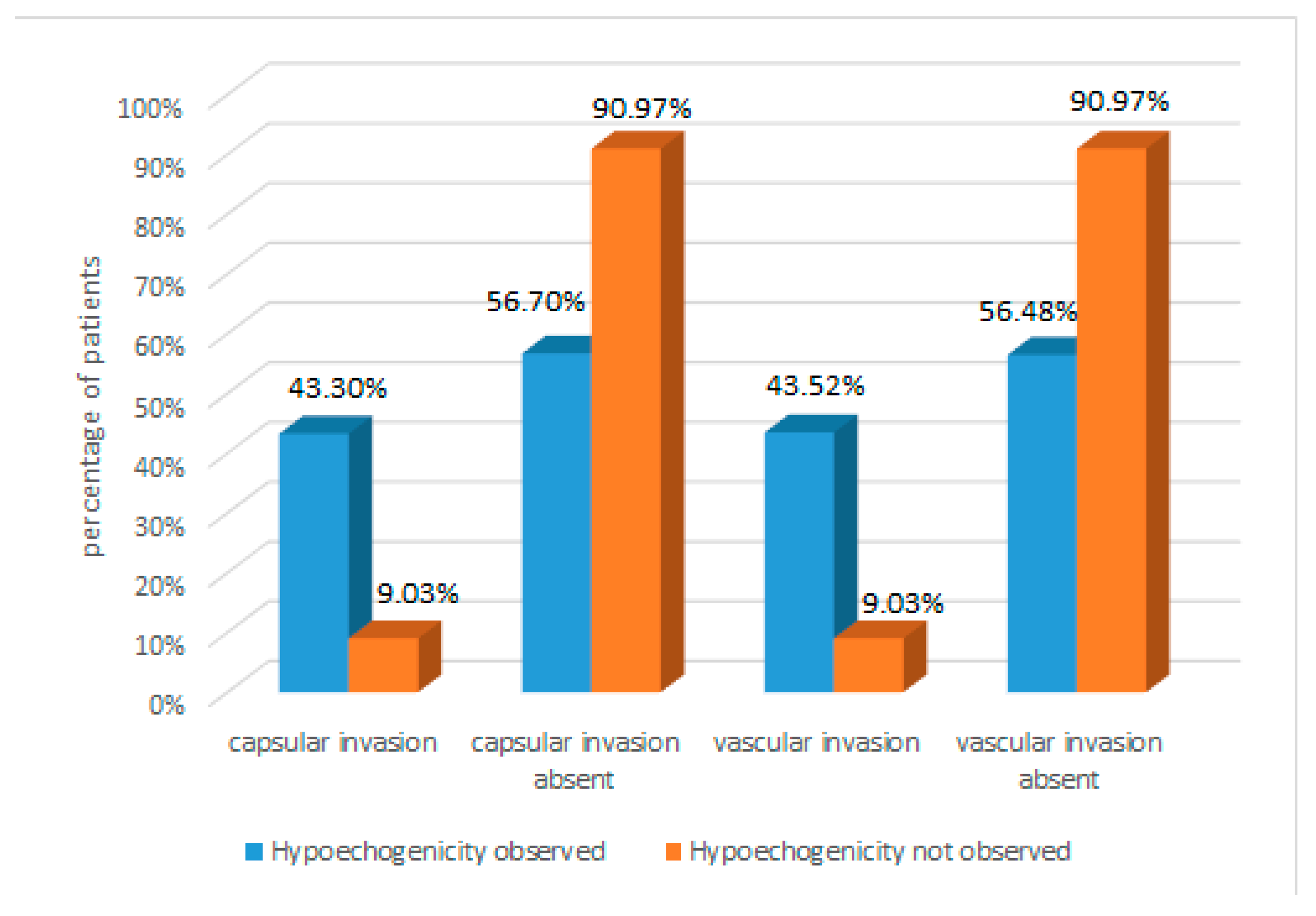
3.2. Hypoechogenicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nabhan, F.; Dedhia, P.H.; Ringel, M.D. Thyroid cancer, recent advances in diagnosis and therapy. Int. J. Cancer 2021, 149, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Haymart, M.R. Progress and Challenges in Thyroid Cancer Management. Endocr. Pract. 2021, 27, 1260–1263. [Google Scholar] [CrossRef] [PubMed]
- Scheller, B.; Culié, D.; Poissonnet, G.; Dassonville, O.; D’Andréa, G.; Bozec, A. Recent Advances in the Surgical Management of Thyroid Cancer. Curr. Oncol. 2023, 30, 4787–4804. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Filho, A.; Lortet-Tieulent, J.; Bray, F.; Cao, B.; Franceschi, S.; Vaccarella, S.; Dal Maso, L. Thyroid cancer incidence trends by histology in 25 countries: A population-based study. Lancet Diabetes Endocrinol. 2021, 9, 225–234. [Google Scholar] [PubMed]
- Paschke, R.; Lincke, T.; Müller, S.P.; Kreissl, M.C.; Dralle, H.; Fassnacht, M. The Treatment of Well-Differentiated Thyroid Carcinoma. Dtsch. Arztebl. Int. 2015, 112, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Kim, I.J. Recent Updates on the Management of Medullary Thyroid Carcinoma. Endocrinol. Metab. 2016, 31, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Schüle, S.; Darr, A.; Anneken, A.; Hahn, T. Diagnose und Therapie von Schilddrüsenkrebs [Diagnosis and therapy of thyroid cancer]. MMW Fortschr. Med. 2023, 165, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Ushakov, A.V. Principles and features of ultrasound hypoechogenicity in diffuse thyroid pathology. Quant. Imaging Med. Surg. 2024, 14, 2655–2670. [Google Scholar] [CrossRef] [PubMed]
- Alexander, L.F.; Patel, N.J.; Caserta, M.P.; Robbin, M.L. Thyroid Ultrasound: Diffuse and Nodular Disease. Radiol. Clin. N. Am. 2020, 58, 1041–1057. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Ding, K.; Mu, L.; Huang, J.; Ye, F.; Peng, Y.; Guo, C.; Ren, C. Hashimoto’s Thyroiditis: A “Double-Edged Sword” in Thyroid Carcinoma. Front. Endocrinol. 2022, 13, 801925. [Google Scholar] [CrossRef] [PubMed]
- Weetman, A.P. An update on the pathogenesis of Hashimoto’s thyroiditis. J. Endocrinol. Investig. 2021, 44, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, J.X.; Shi, J.; Yu, Y.; Yuan, Z.F.; Lu, G.Z.; Gao, Y.; Gao, Y.M.; Guo, X.H. A retrospective analysis of 12 cases of primary thyroid lymphoma. J. Peking. Univ. Health Sci. 2019, 51, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, C.Y.; Hwang, I.; You, S.H.; Park, S.W.; Lee, B.; Yoon, R.G.; Yim, Y.; Kim, J.H.; Na, D.G. Malignancy risk stratification of thyroid nodules according to echotexture and degree of hypoechogenicity: A retrospective multicenter validation study. Sci. Rep. 2022, 12, 16587. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Du, L.-Y.; Sun, J.-W.; Hou, X.-J.; Wang, H.; Wu, J.-Q.; Zhou, X.-L. Evaluation of thyroid nodules with coexistent Hashimoto’s thyroiditis according to various ultrasound-based risk stratification systems a retrospective research. Eur. J. Radiol. 2020, 131, 109059. [Google Scholar] [CrossRef] [PubMed]
- Huy, G.; Tetsuo, K.; Uyen, D.; Thong, P.; Naoki, O.; Kunio, M.; Tadao, N.; Lewis, H.; Ryohei, K. Prognostic impact of vascular invasion in differentiated thyroid carcinoma: A systematic review and meta-analysis. Eur. J. Endocrinol. 2017, 177, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Rao, M.; Zheng, C.; Huang, J.; Fang, D.; Xiong, Y.; Yuan, G. Analysis of factors influencing the clinical outcome after surgery and 131I therapy in patients with moderate-risk thyroid papillary carcinoma. Front. Endocrinol. 2022, 13, 1015798. [Google Scholar] [CrossRef]
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in Thyroid Cancer Incidence and Mortality in the United States. JAMA 2017, 4, 317. [Google Scholar]
- Cho, S.J.; Suh, C.H.; Baek, J.H.; Chung, S.R.; Choi, Y.J.; Chung, K.W.; Shong, Y.K.; Lee, J.H. Active Surveillance for Small Papillary Thyroid Cancer: A Systematic Review and Meta-Analysis. Thyroid 2019, 29, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- Ashorobi, D.; Lopez, P.P. Follicular Thyroid Cancer. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Gršić, K.; Bumber, B.; Curić-Radivojević, R.; Leović, D. Prophylactic Central Neck Dissection in Well-differentiated Thyroid Cancer. Acta Clin. Croat. 2020, 59, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Boucai, L.; Zafereo, M.; Cabanillas, M.E. Thyroid Cancer: A Review. JAMA 2024, 331, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Nixon, I.J. Well-differentiated thyroid cancer—Are you overtreating your patients? Endokrynol. Pol. 2016, 67, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Jayasinghe, R.; Basnayake, O.; Jayarajah, U.; Seneviratne, S. Management of medullary carcinoma of the thyroid: A review. J. Int. Med. Res. 2022, 50. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, R.V.; Osamura, R.Y.; Klöppel, G.; Rosai, J. (Eds.) WHO Classification of Tumours of Endocrine Organs, 4th ed.; IARC Publications: Lyon, France, 2017; Volume 10. [Google Scholar]
- Vianello, F.; Censi, S.; Watutantrige-Fernando, S.; Barollo, S.; Zhu, Y.H.; Albiger, N.; Bertazza, L.; Manso, J.; Carducci, S.; Benna, C.; et al. The role of the size in thyroid cancer risk stratification. Sci. Rep. 2021, 11, 7303. [Google Scholar] [CrossRef] [PubMed]
- Magra, V.; Boulogeorgou, K.; Paschou, E.; Sevva, C.; Manaki, V.; Mpotani, I.; Mantalovas, S.; Laskou, S.; Kesisoglou, I.; Koletsa, T.; et al. Frequency of Thyroid Microcarcinoma in Patients Who Underwent Total Thyroidectomy with Benign Indication-A 5-Year Retrospective Review. Medicina 2024, 60, 468. [Google Scholar] [CrossRef]
- Akbulut, D.; Kuz, E.D.; Kursun, N.; Dizbay Sak, S. Capsular Invasion Matters Also in “Papillary Patterned” Tumors: A Study on 121 Cases of Encapsulated Conventional Variant of Papillary Thyroid Carcinoma. Endocr. Pathol. 2021, 32, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Carcangiu, M.L.; Zampi, G.; Pupi, A.; Castagnoli, A.; Rosai, J. Papillary carcinoma of the thyroid. A clinicopathologic study of 241 cases treated at the University of Florence, Italy. Cancer 1985, 55, 805–828. [Google Scholar] [CrossRef] [PubMed]
- Rivera, M.; Tuttle, R.M.; Patel, S.; Shaha, A.; Shah, J.P.; Ghossein, R.A. Encapsulated papillary thyroid carcinoma: A clini-co-pathologic study of 106 cases with emphasis on its morphologic subtypes (histologic growth pattern). Thyroid 2009, 19, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.Y.; Lee, C.H.; Park, S.Y.; Park, H.J.; Min, H.S.; Won, J.K.; Kim, B.S.; Ryu, H.S. Characteristic tumor growth patterns as novel histomorphologic predictors for lymph node metastasis in papillary thyroid carcinoma. Hum. Pathol. 2013, 44, 2620–2627. [Google Scholar] [CrossRef] [PubMed]
- Campennì, A.; Barbaro, D.; Guzzo, M.; Capoccetti, F.; Giovanella, L. Personalized management of differentiated thyroid cancer in real life—Practical guidance from a multidisciplinary panel of experts. Endocrine 2020, 70, 280–291. [Google Scholar] [CrossRef] [PubMed]
- Ardito, G.; Revelli, L.; Giustozzi, E.; Salvatori, M.; Fadda, G.; Ardito, F.; Avenia, N.; Ferretti, A.; Rampin, L.; Chondrogiannis, S.; et al. Aggressive papillary thyroid microcarcinoma: Prognostic factors and therapeutic strategy. Clin. Nucl. Med. 2013, 38, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Mete, O.; Asa, S.L. Thyroid Tumor Capsular Invasion: The Bottom Line or Much Ado About Nothing? Endocr. Pathol. 2020, 31, 141–142. [Google Scholar] [CrossRef] [PubMed]
- Kaliszewski, K.; Wojtczak, B.; Strutyńska-Karpińska, M.; Łukieńczuk, T.; Forkasiewicz, Z.; Domosławski, P. Incidental and non-incidental thyroid microcarcinoma. Oncol. Lett. 2016, 12, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Li, Y.; Jung, C.K.; Song, D.E.; Hang, J.F.; Liu, Z.; Jain, D.; Lai, C.R.; Hirokawa, M.; Kakudo, K.; et al. Histopathologic Assessment of Capsular Invasion in Follicular Thyroid Neoplasms-an Observer Variation Study. Endocr. Pathol. 2020, 31, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wei, Y.; Zhao, Z.L.; Peng, L.L.; Li, Y.; Lu, N.C.; Yu, M.A. A preliminary study of microwave ablation for solitary T1N0M0 papillary thyroid carcinoma with capsular invasion. Int. J. Hyperthermia 2022, 39, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.; Faridmoayer, E.; Lapkus, M.; Pastewski, J.; Sun, F.; Elassar, H.; Studzinski, D.M.; Callahan, R.E.; Czako, P.; Nagar, S. Vascular invasion predicts advanced tumor characteristics in papillary thyroid carcinoma. Am. J. Surg. 2022, 223, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Jacob, J. Invasion in thyroid cancer: Controversies and best practices. Semin. Diagn. Pathol. 2020, 37, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, L.; Borges Duarte, D.; Ricardo Brandão, J.; Alves Pereira, C.; Amado, A.; Gouveia, P.; Couto Carvalho, A.; Borges, F.; Freitas, C. Papillary thyroid carcinoma: The impact of histologic vascular invasion. Minerva Endocrinol. 2022, 49, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Wang, L.; Tuttle, R.M.; Ganly, I.; Ghossein, R. Prognostic impact of extent of vascular invasion in low-grade encapsu-lated follicular cell-derived thyroid carcinomas: A clinicopathologic study of 276 cases. Hum. Pathol. 2015, 46, 1789–1798. [Google Scholar] [CrossRef] [PubMed]
- Ghossein, R.A.; Hiltzik, D.H.; Carlson, D.L.; Patel, S.; Shaha, A.; Shah, J.P.; Tuttle, R.M.; Singh, B. Prognostic factors of recur-rence in encapsulated Hurthle cell carcinoma of the thyroid gland: A clinicopathologic study of 50 cases. Cancer 2006, 106, 1669–1676. [Google Scholar] [CrossRef]
- Ito, Y.; Hirokawa, M.; Masuoka, H.; Higashiyama, T.; Kihara, M.; Onoda, N.; Miya, A.; Miyauchi, A. Prognostic factors for follicular thyroid carcinoma: The importance of vascular invasion. Endocr. J. 2022, 69, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, H.; Katoh, R.; Sugino, K.; Matsuzu, K.; Masaki, C.; Akaishi, J.; Hames, K.Y.; Tomoda, C.; Suzuki, A.; Ohkuwa, K.; et al. Correction: Encapsulated Angioinvasive Follicular Thyroid Carcinoma: Prognostic Impact of the Extent of Vascular Invasion. Ann. Surg. Oncol. 2022, 29, 8213. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, D.; Ganly, I. New Insights on the Importance of the Extent of Vascular Invasion in Encapsulated Angio-invasive Follicular Thyroid Carcinoma. Ann. Surg. Oncol. 2022, 29, 4024–4025. [Google Scholar] [CrossRef] [PubMed]
- Gulcelik, N.E.; Akin, S.; Aydin, K.; Aydin, C.; Guler, Y.G.; Usman, A. The role of vascular endothelial growth factor in the development of papillary thyroid carcinoma in patients with lymphocytic thyroiditis. Minerva Endocrinol. 2023, 48, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Cong, M.; Zhou, W.; Zhu, J.; Liu, Q. Relationship between protein expression of VEGF-C, MMP-2 and lymph node metastasis in papillary thyroid cancer. J. Int. Med. Res. 2008, 36, 699–703. [Google Scholar] [CrossRef] [PubMed]
- Kaliszewski, K.; Diakowska, D.; Rzeszutko, M.; Nowak, Ł.; Aporowicz, M.; Wojtczak, B.; Sutkowski, K.; Rudnicki, J. Risk factors of papillary thyroid microcarcinoma that predispose patients to local recurrence. PLoS ONE 2020, 15, e0244930. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.S.; Lee, Y.S.; Lee, J.C.; Son, S.M.; Shin, D.H.; Kim, S.S.; Kim, I.J.; Lee, B.J. Ultrasound Echogenicity of Papillary Thyroid Cancer Is Affected by Tumor Growth Patterns and Tumor Fibrosis. In Vivo 2021, 35, 1633–1640. [Google Scholar] [CrossRef] [PubMed]
- Jiwang, L.; Yahong, L.; Kai, L.; Bo, H.; Yuejiao, Z.; Haotian, W.; Tao, Y. Clinicopathologic factors and preoperative ultraso-nographic characteristics for predicting central lymph node metastasis in papillary thyroid microcarcinoma: A single center retrospective study. Braz. J. Otorhinolaryngol. 2022, 88, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Prieditis, P.; Radzina, M.; Mikijanska, M.; Liepa, M.; Stepanovs, K.; Grani, G.; Durante, C.; Lamartina, L.; Trimboli, P.; Cantisani, V. Non-Marked Hypoechogenic Nodules: Multicenter Study on the Thyroid Malignancy Risk Stratification and Accuracy Based on TIRADS Systems Comparison. Medicina 2022, 58, 257. [Google Scholar] [CrossRef] [PubMed]
- Hacim, N.A.; Akbaş, A.; Ulgen, Y.; Aktokmakyan, T.V.; Meric, S.; Tokocin, M.; Karabay, O.; Altinel, Y. Impact of Ultraso-nographic Features for Thyroid Malignancy in Patients With Bethesda Categories III, IV, and V: A Retrospective Observational Study in a Tertiary Center. Cureus 2021, 13, 16708. [Google Scholar] [CrossRef] [PubMed]
- Cosme, I.; Nobre, E.; Bugalho, M.J. Factors for second non-diagnostic ultrasound-guided fine-needle aspiration cytology in thyroid nodules. Ann. Endocrinol. 2023, 84, 734–738. [Google Scholar] [CrossRef]
- Borowczyk, M.; Woliński, K.; Więckowska, B.; Jodłowska-Siewert, E.; Szczepanek-Parulska, E.; Verburg, F.A.; Ruchała, M. Sonographic Features Differentiating Follicular Thyroid Cancer from Follicular Adenoma-A Meta-Analysis. Cancers 2021, 13, 938. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Feature | Number of Patients | p Value | |
|---|---|---|---|
| Sex | Male | 97 (14.31%) | 0.133 |
| Female | 581 (85.69%) | ||
| Age (years) | <55 | 385 (56.78%) | <0.0001 |
| >55 | 293 (43.22%) | ||
| Type of surgery | Total | 474 (69.91%) | |
| No total | 204 (30.09%) | ||
| Reoperation needed | Yes | 176 (25.95%) | 0.002 |
| No | 502 (74.04%) | ||
| Histological type | Papillary | 579 (85.39%) | - |
| Follicular | 31 (4.57%) | ||
| Medullary | 24 (3.53%) | ||
| Undifferentiated | 14 (2.06%) | ||
| Lymphoma | 12 (1.76%) | ||
| Secondary | 10 (1.47%) | ||
| Squamous cell | 4 (0.58%) | ||
| Sarcoma | 3 (0.44%) | ||
| Myeloma | 1 (0.14%) | ||
| pTNM stage | I | 501 (73.89%) | <0.0001 |
| II | 90 (13.27%) | ||
| III | 42 (6.19%) | ||
| IV | 45 (6.63%) | ||
| pT | pT1a | 256 (37.75%) | |
| pT1b | 276 (40.70%) | ||
| pT2 | 78 (11.50%) | ||
| pT3 | 24 (3.54%) | ||
| pT4a | 16 (2.36%) | ||
| pT4b | 26 (3.83%) | ||
| pTm | 2 (0.29%) | ||
| pN | pN0 | 427 (62.97%) | |
| pN1a | 184 (27.14%) | ||
| pN1b | 35 (5.16%) | ||
| pNx | 32 (4.72%) | ||
| pM | pM0 | 568 (83.78%) | |
| pM1 | 46 (6.78%) | ||
| pMx | 64 (9.43%) | ||
| Feature | Number of Patients | p Value |
|---|---|---|
| pN0 | 384 (62.95%) | |
| Capsular invasion | 142 (36.98%) | <0.0001 |
| Capsular invasion absent | 242 (63.02%) | |
| Vascular invasion | 210 (54.69%) | |
| Vascular invasion absent | 174 (45.31%) | |
| pN1a | 166 (27.21%) | |
| Capsular invasion | 129 (77.71%) | <0.0001 |
| Capsular invasion absent | 37 (22.29%) | |
| Vascular invasion | 125 (75.30%) | |
| Vascular invasion absent | 41 (24.70%) | |
| pN1b | 31 (5.09%) | |
| Capsular invasion | 31 (100%) | <0.0001 |
| Capsular invasion absent | 0 (0%) | |
| Vascular invasion | 31 (100%) | |
| Vascular invasion absent | 0 (0%) | |
| pNx | 29 (4.75%) | |
| Capsular invasion | 13 (44.83%) | <0.0001 |
| Capsular invasion absent | 16 (55.17%) | |
| Vascular invasion | 13 (44.83%) | |
| Vascular invasion absent | 16 (55.17%) |
| Feature | Number of Patients | p Value |
|---|---|---|
| Hypoechogenicity observed | 455 (74.59%) | |
| Capsular invasion | 197 (43.30%) | <0.0001 |
| Capsular invasion absent | 258 (56.70%) | |
| Vascular invasion | 198 (43.52%) | |
| Vascular invasion absent | 257 (56.48%) | |
| Hypoechogenicity not observed | 155 (25.41%) | |
| Capsular invasion | 14 (9.03%) | <0.0001 |
| Capsular invasion absent | 141 (90.97%) | |
| Vascular invasion | 14 (9.03%) | |
| Vascular invasion absent | 141 (90.97%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurkiewicz, K.; Miciak, M.; Biernat, S.; Wojtczak, B.; Kaliszewski, K. Correlation of pN Stage and Hypoechogenicity with Tumour Encapsulation and Vascular Invasion in Thyroid Cancer (TC): A Comprehensive Analysis and Clinical Outcomes. Cancers 2024, 16, 2019. https://doi.org/10.3390/cancers16112019
Jurkiewicz K, Miciak M, Biernat S, Wojtczak B, Kaliszewski K. Correlation of pN Stage and Hypoechogenicity with Tumour Encapsulation and Vascular Invasion in Thyroid Cancer (TC): A Comprehensive Analysis and Clinical Outcomes. Cancers. 2024; 16(11):2019. https://doi.org/10.3390/cancers16112019
Chicago/Turabian StyleJurkiewicz, Krzysztof, Michał Miciak, Szymon Biernat, Beata Wojtczak, and Krzysztof Kaliszewski. 2024. "Correlation of pN Stage and Hypoechogenicity with Tumour Encapsulation and Vascular Invasion in Thyroid Cancer (TC): A Comprehensive Analysis and Clinical Outcomes" Cancers 16, no. 11: 2019. https://doi.org/10.3390/cancers16112019
APA StyleJurkiewicz, K., Miciak, M., Biernat, S., Wojtczak, B., & Kaliszewski, K. (2024). Correlation of pN Stage and Hypoechogenicity with Tumour Encapsulation and Vascular Invasion in Thyroid Cancer (TC): A Comprehensive Analysis and Clinical Outcomes. Cancers, 16(11), 2019. https://doi.org/10.3390/cancers16112019