

The Crosstalk between Nerves and Cancer—A Poorly Understood Phenomenon and New Possibilities

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials/Methods
3. Results
3.1. A Short Historical View of the Interaction between the NGF and Cancer
3.2. The NGF’s Receptors and Its Effect on Neurons
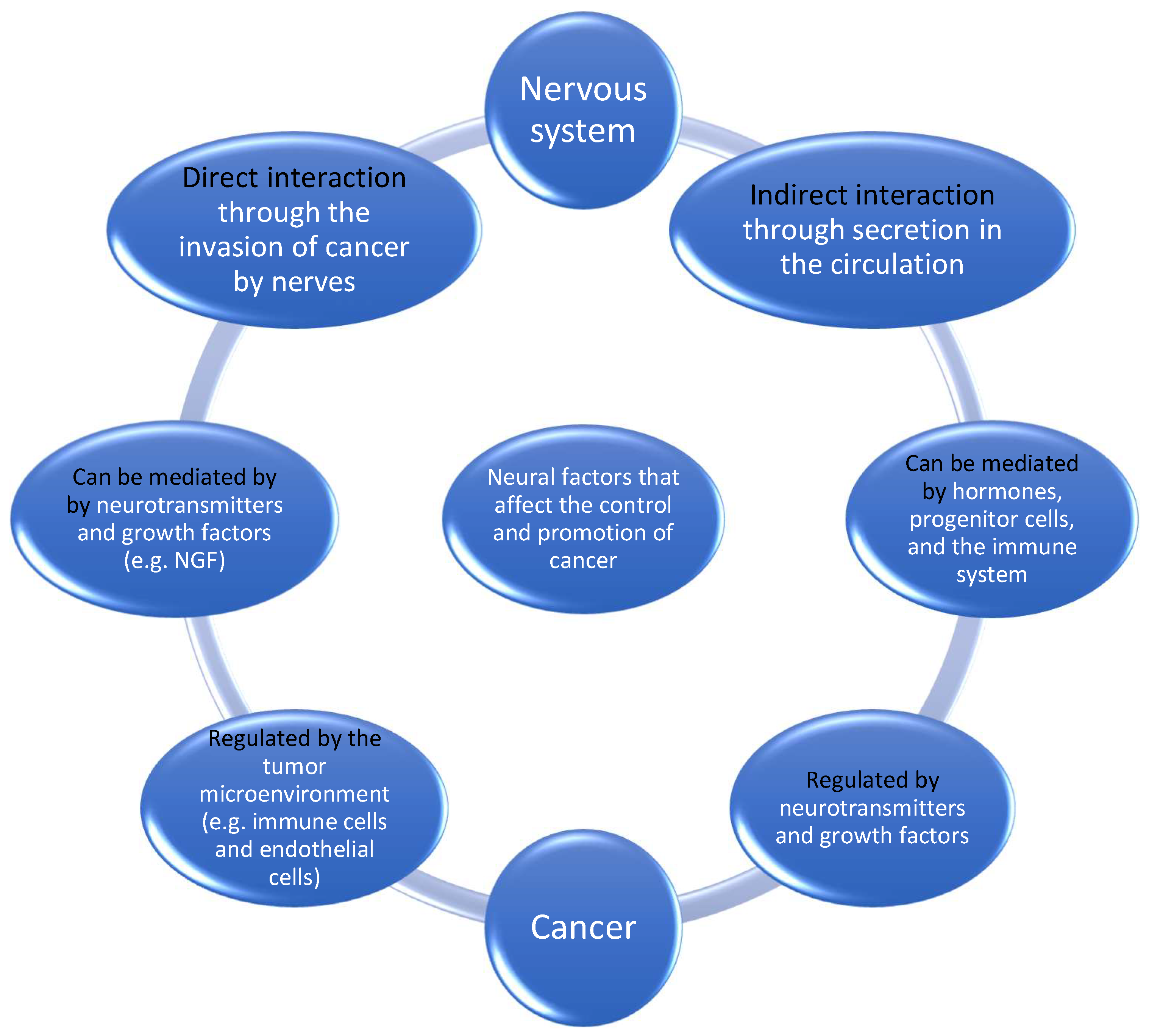
3.3. The Crosstalk between Nerves and Cancer
3.4. What We Know Now about the Interaction between the NGF and Cancer
3.5. A Common Feature in Both PCa and PDAC
3.6. The NGF, the Immune System, and Inflammation
3.7. The NGF and Pain
3.8. Can Nerve–Cancer Interactions Help Explain the Connection between Stress and Cancer?
4. What Is Known about the Interaction between Nerves and Cancers in PCa and PDAC?
4.1. Crosstalk in Prostate Cancer
4.2. Denervation as a Therapeutic Approach
4.3. Radiation Therapy as a Therapeutic Approach
4.4. Beta-Blockers as a Therapeutic Approach
4.5. Perineural Invasion (PNI) in Prostate Cancer
4.6. The NGF in Prostate Cancer
4.7. Crosstalk in Pancreatic Cancer
4.8. The NGF in Pancreatic Cancer
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mauffrey, P.; Tchitchek, N.; Barroca, V.; Bemelmans, A.-P.; Firlej, V.; Allory, Y.; Roméo, P.-H.; Magnon, C. Progenitors from the central nervous system drive neurogenesis in cancer. Nature 2019, 569, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Gola, M.; Sejda, A.; Godlewski, J.; Cieślak, M.; Starzyńska, A. Neural component of the tumor microenvironment in pancreatic ductal adenocarcinoma. Cancers 2022, 14, 5246. [Google Scholar] [CrossRef] [PubMed]
- Magnon, C.; Hondermarck, H. The neural addiction of cancer. Nat. Rev. Cancer 2023, 23, 317–334. [Google Scholar] [CrossRef] [PubMed]
- Dlamini, Z.; Khanyile, R.; Molefi, T.; Damane, B.P.; Bates, D.O.; Hull, R. Genomic Interplay between Neoneurogenesis and Neoangiogenesis in Carcinogenesis: Therapeutic Interventions. Cancers 2023, 15, 1805. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.E.; Dai, H.; Powell, M.; Li, R.; Ding, Y.; Wheeler, T.M.; Shine, D.; Kadmon, D.; Thompson, T.; Miles, B.J. Cancer-related axonogenesis and neurogenesis in prostate cancer. Clin. Cancer Res. 2008, 14, 7593–7603. [Google Scholar] [CrossRef] [PubMed]
- Shi, D.D.; Guo, J.A.; Hoffman, H.I.; Su, J.; Mino-Kenudson, M.; Barth, J.L.; Schenkel, J.M.; Loeffler, J.S.; Shih, H.A.; Hong, T.S. Therapeutic avenues for cancer neuroscience: Translational frontiers and clinical opportunities. Lancet Oncol. 2022, 23, e62–e74. [Google Scholar] [CrossRef] [PubMed]
- Ebendal, T. Function and evolution in the NGF family and its receptors. J. Neurosci. Res. 1992, 32, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Monje, M.; Borniger, J.C.; D’Silva, N.J.; Deneen, B.; Dirks, P.B.; Fattahi, F.; Frenette, P.S.; Garzia, L.; Gutmann, D.H.; Hanahan, D. Roadmap for the emerging field of cancer neuroscience. Cell 2020, 181, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Marchesi, F.; Piemonti, L.; Mantovani, A.; Allavena, P. Molecular mechanisms of perineural invasion, a forgotten pathway of dissemination and metastasis. Cytokine Growth Factor Rev. 2010, 21, 77–82. [Google Scholar] [CrossRef]
- Liebig, C.; Ayala, G.; Wilks, J.A.; Berger, D.H.; Albo, D. Perineural invasion in cancer: A review of the literature. Cancer 2009, 115, 3379–3391. [Google Scholar] [CrossRef]
- Ayala, G.E.; Wheeler, T.M.; Shine, H.D.; Schmelz, M.; Frolov, A.; Chakraborty, S.; Rowley, D. In vitro dorsal root ganglia and human prostate cell line interaction: Redefining perineural invasion in prostate cancer. Prostate 2001, 49, 213–223. [Google Scholar] [CrossRef]
- Bueker, E.D. Implantation of tumors in the hind limb field of the embryonic chick and the developmental response of the lumbosacral nervous system. Anat. Rec. 1948, 102, 369–389. [Google Scholar] [CrossRef]
- Lutzelschwab, R.; Klambt, C.; Rossa, R.; Schmidt, O. by R. Levi-Montalcini The EMBO Journal, 6, 1145-1154, 1987. EMBO J. 1987, 6, 1145–1154. [Google Scholar]
- Aloe, L. Rita Levi-Montalcini: The discovery of nerve growth factor and modern neurobiology. Trends Cell Biol. 2004, 14, 395–399. [Google Scholar] [CrossRef]
- Sidorova, Y.A. Neurotrophic Factors Neurodegeneration. In Frontiers in Clinical Drug Research-CNS and Neurological Disorders; Bentham Science Publishers: Sharjah, United Arab Emirates, 2022; Volume 10, p. 132. [Google Scholar]
- Cowan, W.M. Viktor Hamburger and Rita Levi-Montalcini: The path to the discovery of nerve growth factor. Annu. Rev. Neurosci. 2001, 24, 551–600. [Google Scholar] [CrossRef]
- Levi-Montalcini, R. Developmental neurobiology and the natural history of nerve growth factor. Annu. Rev. Neurosci. 1982, 5, 341–362. [Google Scholar] [CrossRef]
- Bradshaw, R.A.; Mobley, W.; Rush, R.A. Nerve growth factor and related substances: A brief history and an introduction to the international NGF meeting series. Int. J. Mol. Sci. 2017, 18, 1143. [Google Scholar] [CrossRef]
- Ishii, D.; Shooter, E. Regulation of Nerve Growth Factor Synthesis in Mouse Submaxillary Glands by Testosterone 1. J. Neurochem. 1975, 25, 843–851. [Google Scholar] [CrossRef]
- Angeletti, R.H.; Bradshaw, R.A. Nerve growth factor from mouse submaxillary gland: Amino acid sequence. Proc. Natl. Acad. Sci. USA 1971, 68, 2417–2420. [Google Scholar] [CrossRef] [PubMed]
- Marsland, M.; Dowdell, A.; Faulkner, S.; Jobling, P.; Rush, R.A.; Gedye, C.; Lynam, J.; Griffin, C.P.; Baker, M.; Marsland, J. ProNGF Expression and Targeting in Glioblastoma Multiforme. Int. J. Mol. Sci. 2023, 24, 1616. [Google Scholar] [CrossRef] [PubMed]
- Rocco, M.L.; Soligo, M.; Manni, L.; Aloe, L. Nerve growth factor: Early studies and recent clinical trials. Curr. Neuropharmacol. 2018, 16, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Yu, Y.; Zhang, P.; Ma, G.; Zhang, M.; Liang, Y.; Jiao, W.; Niu, H. Identification of NTRK3 as a potential prognostic biomarker associated with tumor mutation burden and immune infiltration in bladder cancer. BMC Cancer 2021, 21, 458. [Google Scholar] [CrossRef]
- Li, W.; Lu, Y.; Yu, X.; Yong, M.; Ma, D.; Gao, Q. Detection of exosomal tyrosine receptor kinase B as a potential biomarker in ovarian cancer. J. Cell. Biochem. 2019, 120, 6361–6369. [Google Scholar] [CrossRef] [PubMed]
- Demir, I.E.; Tieftrunk, E.; Schorn, S.; Friess, H.; Ceyhan, G.O. Nerve growth factor & TrkA as novel therapeutic targets in cancer. Biochim. Et Biophys. Acta (BBA)-Rev. Cancer 2016, 1866, 37–50. [Google Scholar]
- Theik, N.W.Y.; Muminovic, M.; Alvarez-Pinzon, A.M.; Shoreibah, A.; Hussein, A.M.; Raez, L.E. NTRK Therapy among Different Types of Cancers, Review and Future Perspectives. Int. J. Mol. Sci. 2024, 25, 2366. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Tan, X.; Sivakumar, S.; Bednarsch, J.; Wiltberger, G.; Kather, J.N.; Niehues, J.; de Vos-Geelen, J.; Valkenburg-van Iersel, L.; Kintsler, S.; Roeth, A. Nerve fibers in the tumor microenvironment in neurotropic cancer—Pancreatic cancer and cholangiocarcinoma. Oncogene 2021, 40, 899–908. [Google Scholar] [CrossRef]
- Hanahan, D. Hallmarks of cancer: New dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef]
- Ebben, J.D.; You, M. Brain metastasis in lung cancer: Building a molecular and systems-level understanding to improve outcomes. Int. J. Biochem. Cell Biol. 2016, 78, 288–296. [Google Scholar] [CrossRef]
- Grantyn, R.; Henneberger, C.; Jüttner, R.; Meier, J.C.; Kirischuk, S. Functional hallmarks of GABAergic synapse maturation and the diverse roles of neurotrophins. Front. Cell. Neurosci. 2011, 5, 13. [Google Scholar] [CrossRef]
- Huang, D.; Wang, Y.; Thompson, J.W.; Yin, T.; Alexander, P.B.; Qin, D.; Mudgal, P.; Wu, H.; Liang, Y.; Tan, L. Cancer-cell-derived GABA promotes β-catenin-mediated tumour growth and immunosuppression. Nat. Cell Biol. 2022, 24, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Malfait, A.-M.; Miller, R.E.; Block, J.A. Targeting neurotrophic factors: Novel approaches to musculoskeletal pain. Pharmacol. Ther. 2020, 211, 107553. [Google Scholar] [CrossRef]
- Mitsou, J.D.; Tseveleki, V.; Dimitrakopoulos, F.-I.; Konstantinidis, K.; Kalofonos, H. Radical Tumor Denervation Activates Potent Local and Global Cancer Treatment. Cancers 2023, 15, 3758. [Google Scholar] [CrossRef]
- Mohammed, S.; Sukumaran, S.; Bajgain, P.; Watanabe, N.; Heslop, H.E.; Rooney, C.M.; Brenner, M.K.; Fisher, W.E.; Leen, A.M.; Vera, J.F. Improving chimeric antigen receptor-modified T cell function by reversing the immunosuppressive tumor microenvironment of pancreatic cancer. Mol. Ther. 2017, 25, 249–258. [Google Scholar] [CrossRef]
- Majidpoor, J.; Mortezaee, K. The efficacy of PD-1/PD-L1 blockade in cold cancers and future perspectives. Clin. Immunol. 2021, 226, 108707. [Google Scholar] [CrossRef]
- Uddin, M.H.; Zhang, D.; Muqbil, I.; El-Rayes, B.F.; Chen, H.; Philip, P.A.; Azmi, A.S. Deciphering cellular plasticity in pancreatic cancer for effective treatments. Cancer Metastasis Rev. 2024, 43, 393–408. [Google Scholar] [CrossRef]
- Kritas, S.; Caraffa, A.; Antinolfi, P.; Saggini, A.; Pantalone, A.; Rosati, M.; Tei, M.; Speziali, A.; Saggini, R.; Pandolfi, F. Nerve growth factor interactions with mast cells. Int. J. Immunopathol. Pharmacol. 2014, 27, 15–19. [Google Scholar] [CrossRef]
- Terracina, S.; Ferraguti, G.; Tarani, L.; Fanfarillo, F.; Tirassa, P.; Ralli, M.; Iannella, G.; Polimeni, A.; Lucarelli, M.; Greco, A. Nerve Growth Factor and Autoimmune Diseases. Curr. Issues Mol. Biol. 2023, 45, 8950–8973. [Google Scholar] [CrossRef]
- Datta-Mitra, A.; Kundu-Raychaudhuri, S.; Mitra, A.; Raychaudhuri, S.P. Cross talk between neuroregulatory molecule and monocyte: Nerve growth factor activates the inflammasome. PLoS ONE 2015, 10, e0121626. [Google Scholar] [CrossRef] [PubMed]
- Minnone, G.; De Benedetti, F.; Bracci-Laudiero, L. NGF and its receptors in the regulation of inflammatory response. Int. J. Mol. Sci. 2017, 18, 1028. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yang, T.; Shi, S.; Xu, C.; Wang, F.; Dai, D.; Guan, G.; Zhang, Y.; Wang, S.; Wang, J. Heterogeneity-induced NGF-NGFR communication inefficiency promotes mitotic spindle disorganization in exhausted T cells through PREX1 suppression to impair the anti-tumor immunotherapy with PD-1 mAb in hepatocellular carcinoma. Cancer Med. 2024, 13, e6736. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, M.A. Peripheral Neuroinflammation and Pain: How Acute Pain Becomes Chronic. Curr. Neuropharmacol. 2024, 22, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Reis, C.; Chambel, S.; Ferreira, A.; Cruz, C.D. Involvement of nerve growth factor (NGF) in chronic neuropathic pain–a systematic review. Rev. Neurosci. 2023, 34, 75–84. [Google Scholar] [CrossRef]
- Enomoto, M.; Mantyh, P.W.; Murrell, J.; Innes, J.F.; Lascelles, B.D.X. Anti-nerve growth factor monoclonal antibodies for the control of pain in dogs and cats. Vet. Rec. 2019, 184, 23. [Google Scholar] [CrossRef]
- Watson, J.J.; Allen, S.J.; Dawbarn, D. Targeting nerve growth factor in pain: What is the therapeutic potential? BioDrugs 2008, 22, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Bannwarth, B.; Kostine, M. Nerve growth factor antagonists: Is the future of monoclonal antibodies becoming clearer? Drugs 2017, 77, 1377–1387. [Google Scholar] [CrossRef] [PubMed]
- Alleva, E.; Branchi, I. NGF: A social molecule. Psychoneuroendocrinology 2006, 3, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Blanc-Lapierre, A.; Rousseau, M.-C.; Parent, M.-E. Perceived workplace stress is associated with an increased risk of prostate cancer before age 65. Front. Oncol. 2017, 7, 269. [Google Scholar] [CrossRef]
- Hassan, S.; Pullikuth, A.; Nelson, K.C.; Flores, A.; Karpova, Y.; Baiz, D.; Zhu, S.; Sui, G.; Huang, Y.; Choi, Y.A. β2-Adrenoreceptor signaling increases therapy resistance in prostate cancer by upregulating MCL1. Mol. Cancer Res. 2020, 18, 1839–1848. [Google Scholar] [CrossRef]
- Kim-Fuchs, C.; Le, C.P.; Pimentel, M.A.; Shackleford, D.; Ferrari, D.; Angst, E.; Hollande, F.; Sloan, E.K. Chronic stress accelerates pancreatic cancer growth and invasion: A critical role for beta-adrenergic signaling in the pancreatic microenvironment. Brain Behav. Immun. 2014, 40, 40–47. [Google Scholar] [CrossRef]
- Guo, H.; Ren, Y.; Huang, B.; Wang, J.; Yang, X.; Wang, Y.; Zhao, E. Psychological status, compliance, serum brain-derived neurotrophic factor, and nerve growth factor levels of patients with depression after augmented mindfulness-based cognitive therapy. Genet. Res. 2022, 2022, e82. [Google Scholar] [CrossRef]
- Braadland, P.R.; Ramberg, H.; Grytli, H.H.; Taskén, K.A. β-adrenergic receptor signaling in prostate cancer. Front. Oncol. 2015, 4, 375. [Google Scholar] [CrossRef]
- Hassan, S.; Karpova, Y.; Baiz, D.; Yancey, D.; Pullikuth, A.; Flores, A.; Register, T.; Cline, J.M.; D’Agostino, R.; Danial, N. Behavioral stress accelerates prostate cancer development in mice. J. Clin. Investig. 2013, 123, 874–886. [Google Scholar] [CrossRef]
- Lu, D.; Sinnott, J.A.; Valdimarsdóttir, U.; Fang, F.; Gerke, T.; Tyekucheva, S.; Fiorentino, M.; Lambe, M.; Sesso, H.D.; Sweeney, C.J. Stress-related signaling pathways in lethal and nonlethal prostate cancer. Clin. Cancer Res. 2016, 22, 765–772. [Google Scholar] [CrossRef]
- Bauman, J.; McVary, K. Autonomic nerve development contributes to prostate cancer progression. Asian J. Androl. 2013, 15, 713. [Google Scholar] [CrossRef]
- Pan, C.; Winkler, F. Insights and opportunities at the crossroads of cancer and neuroscience. Nat. Cell Biol. 2022, 24, 1454–1460. [Google Scholar] [CrossRef]
- Magnon, C.; Hall, S.J.; Lin, J.; Xue, X.; Gerber, L.; Freedland, S.J.; Frenette, P.S. Autonomic nerve development contributes to prostate cancer progression. Science 2013, 341, 1236361. [Google Scholar] [CrossRef]
- Coarfa, C.; Florentin, D.; Putluri, N.; Ding, Y.; Au, J.; He, D.; Ragheb, A.; Frolov, A.; Michailidis, G.; Lee, M. Influence of the neural microenvironment on prostate cancer. Prostate 2018, 78, 128–139. [Google Scholar] [CrossRef]
- Guo, J.A.; Hoffman, H.I.; Shroff, S.G.; Chen, P.; Hwang, P.G.; Kim, D.Y.; Kim, D.W.; Cheng, S.W.; Zhao, D.; Mahal, B.A. Pan-cancer transcriptomic predictors of perineural invasion improve occult histopathologic detection. Clin. Cancer Res. 2021, 27, 2807–2815. [Google Scholar] [CrossRef]
- Saloman, J.L.; Albers, K.M.; Li, D.; Hartman, D.J.; Crawford, H.C.; Muha, E.A.; Rhim, A.D.; Davis, B.M. Ablation of sensory neurons in a genetic model of pancreatic ductal adenocarcinoma slows initiation and progression of cancer. Proc. Natl. Acad. Sci. USA 2016, 113, 3078–3083. [Google Scholar] [CrossRef]
- Campbell, J.P.; Karolak, M.R.; Ma, Y.; Perrien, D.S.; Masood-Campbell, S.K.; Penner, N.L.; Munoz, S.A.; Zijlstra, A.; Yang, X.; Sterling, J.A. Stimulation of host bone marrow stromal cells by sympathetic nerves promotes breast cancer bone metastasis in mice. PLoS Biol. 2012, 10, e1001363. [Google Scholar] [CrossRef]
- Griffin, N.; Faulkner, S.; Jobling, P.; Hondermarck, H. Targeting neurotrophin signaling in cancer: The renaissance. Pharmacol. Res. 2018, 135, 12–17. [Google Scholar] [CrossRef]
- Blondy, S.; Christou, N.; David, V.; Verdier, M.; Jauberteau, M.-O.; Mathonnet, M.; Perraud, A. Neurotrophins and their involvement in digestive cancers. Cell Death Dis. 2019, 10, 123. [Google Scholar] [CrossRef]
- Patel, N.; Ngo, K.; Hastings, J.; Ketchum, N.; Sepahpanah, F. Prevalence of prostate cancer in patients with chronic spinal cord injury. PMR 2011, 3, 633–636. [Google Scholar] [CrossRef]
- Lawrence. Celiac plexus radiosurgery for pain management in advanced cancer—an international pahse 2 trial. Lancet Oncol. 2024, 12, e050169. [Google Scholar]
- Goepel, M.; Wittmann, A.; Rübben, H.; Michel, M. Comparison of adrenoceptor subtype expression in porcine and human bladder and prostate. Urol. Res. 1997, 25, 199–206. [Google Scholar] [CrossRef]
- Archer, M.; Dogra, N.; Dovey, Z.; Ganta, T.; Jang, H.-S.; Khusid, J.; Lantz, A.; Mihalopoulos, M.; Stockert, J.; Zahalka, A. Role of α-and β-adrenergic signaling in phenotypic targeting: Significance in benign and malignant urologic disease. Cell Commun. Signal. 2021, 19, 1–21. [Google Scholar] [CrossRef]
- Murtola, T.; Tammela, T.; Määttänen, L.; Ala-Opas, M.; Stenman, U.-H.; Auvinen, A. Prostate cancer incidence among finasteride and alpha-blocker users in the Finnish Prostate Cancer Screening Trial. Br. J. Cancer 2009, 101, 843–848. [Google Scholar] [CrossRef]
- Lu, H.; Liu, X.; Guo, F.; Tan, S.; Wang, G.; Liu, H.; Wang, J.; He, X.; Mo, Y.; Shi, B. Impact of beta-blockers on prostate cancer mortality: A meta-analysis of 16,825 patients. OncoTargets Ther. 2015, 8, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Uleri, A.; Baboudjian, M.; Tedde, A.; Rajwa, P.; Pradere, B.; Gallioli, A.; Breda, A.; Ploussard, G. The association between beta-blockers use and prostate cancer mortality: A mini systematic review and meta-analysis. Prostate 2024, 84, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Zhang, S.; Jia, C.-M.; He, W.; Wu, L.-T.; Li, Y.-Q.; Wang, W.; Li, Z.; Ma, J. Antihypertensive drugs use and the risk of prostate cancer: A meta-analysis of 21 observational studies. BMC Urol. 2018, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Sivanesan, S.; Taskén, K.A.; Grytli, H.H. Association of β-Blocker Use at Time of Radical Prostatectomy With Rate of Treatment for Prostate Cancer Recurrence. JAMA Netw. Open 2022, 5, e2145230. [Google Scholar] [CrossRef] [PubMed]
- Badwe, R.A.; Parmar, V.; Nair, N.; Joshi, S.; Hawaldar, R.; Pawar, S.; Kadayaprath, G.; Borthakur, B.B.; Rao Thammineedi, S.; Pandya, S. Effect of peritumoral infiltration of local anesthetic before surgery on survival in early breast cancer. J. Clin. Oncol. 2023, 41, 3318–3328. [Google Scholar] [CrossRef] [PubMed]
- Niu, Y.; Förster, S.; Muders, M. The Role of Perineural Invasion in Prostate Cancer and Its Prognostic Significance. Cancers 2022, 14, 4065. [Google Scholar] [CrossRef] [PubMed]
- Quinn, D.I.; Henshall, S.M.; Brenner, P.C.; Kooner, R.; Golovsky, D.; O’Neill, G.F.; Turner, J.J.; Delprado, W.; Grygiel, J.J.; Sutherland, R.L. Prognostic significance of preoperative factors in localized prostate carcinoma treated with radical prostatectomy: Importance of percentage of biopsies that contain tumor and the presence of biopsy perineural invasion. Cancer 2003, 97, 1884–1893. [Google Scholar] [CrossRef] [PubMed]
- Al-Rashidi, R.R.; Noraldeen, S.A.M.; Kareem, A.K.; Mahmoud, A.K.; Kadhum, W.R.; Ramírez-Coronel, A.A.; Iswanto, A.H.; Obaid, R.F.; Jalil, A.T.; Mustafa, Y.F. Malignant function of nuclear factor-kappaB axis in prostate cancer: Molecular interactions and regulation by non-coding RNAs. Pharmacol. Res. 2023, 194, 106775. [Google Scholar] [CrossRef] [PubMed]
- Liss, M.A.; Gordon, A.; Morales, B.; Osann, K.; Skarecky, D.; Lusch, A.; Zaldivar, F.; Ahlering, T.E. Urinary nerve growth factor as an oncologic biomarker for prostate cancer aggressiveness. Urol. Oncol. 2014, 32, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Deborde, S.; Gusain, L.; Powers, A.; Marcadis, A.; Yu, Y.; Chen, C.-H.; Frants, A.; Kao, E.; Tang, L.H.; Vakiani, E. Reprogrammed Schwann cells organize into dynamic tracks that promote pancreatic cancer invasion. Cancer Discov. 2022, 12, 2454–2473. [Google Scholar] [CrossRef]
- Ceyhan, G.O.; Demir, I.E.; Rauch, U.; Bergmann, F.; Müller, M.W.; Büchler, M.W.; Friess, H.; Schäfer, K.-H. Pancreatic neuropathy results in “neural remodeling” and altered pancreatic innervation in chronic pancreatitis and pancreatic cancer. Off. J. Am. Coll. Gastroenterol. ACG 2009, 104, 2555–2565. [Google Scholar] [CrossRef]
- Chatterjee, D.; Katz, M.H.; Rashid, A.; Wang, H.; Iuga, A.C.; Varadhachary, G.R.; Wolff, R.A.; Lee, J.E.; Pisters, P.W.; Crane, C.H. Perineural and intra-neural invasion in posttherapy pancreaticoduodenectomy specimens predicts poor prognosis in patients with pancreatic ductal adenocarcinoma. Am. J. Surg. Pathol. 2012, 36, 409. [Google Scholar] [CrossRef]
- Jiang, W.; He, R.; Lu, Y.; Zhou, W. The relationships between antihypertensive medications and the overall survival of patients with pancreatic cancer: A systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2022, 16, 547–553. [Google Scholar] [CrossRef]
- Al-Wadei, H.A.; Al-Wadei, M.H.; Schuller, H.M. Prevention of pancreatic cancer by the beta-blocker propranolol. Anti-Cancer Drugs 2009, 20, 477–482. [Google Scholar] [CrossRef]
- Banh, R.S.; Biancur, D.E.; Yamamoto, K.; Sohn, A.S.; Walters, B.; Kuljanin, M.; Gikandi, A.; Wang, H.; Mancias, J.D.; Schneider, R.J. Neurons release serine to support mRNA translation in pancreatic cancer. Cell 2020, 183, 1202–1218.e1225. [Google Scholar] [CrossRef]
- Renz, B.W.; Takahashi, R.; Tanaka, T.; Macchini, M.; Hayakawa, Y.; Dantes, Z.; Maurer, H.C.; Chen, X.; Jiang, Z.; Westphalen, C.B. β2 adrenergic-neurotrophin feedforward loop promotes pancreatic cancer. Cancer Cell 2018, 33, 75–90.e77. [Google Scholar] [CrossRef]

{kind=link}
| Author | Finding | Reference |
|---|---|---|
| Hanahan | Innervation of tissue stem cell niches | [27] |
| Hanahan | Innervation causes resistance against cell death | [27] |
| Mauffrey | Axonal outgrowth for interaction with the TME with the regulation of tumorigenesis and metastasis | [1] |
| Monje | Direct and indirect nerve–cancer crosstalk interactions with immune and endothelial cells | [8] |
| Tan | Cancer-associated fibroblasts produce matrix metalloproteases that regulate neural development | [28] |
| Tan | Production of stellate cells favors nerve outgrowth during tumor development in the tumor microenvironment (TME) | [28] |
| Author | Finding | Reference |
|---|---|---|
| Hanahan | Glutamatergic neuronal activity can drive proliferative signaling in certain central nervous cancers | [57] |
| Magnon | Adrenergic signaling from sympathetic nerves in the TME promotes tumorigenesis | [58] |
| Magnon | Parasympathetic muscarinic receptors regulate tumor invasion and metastasis | [58] |
| Mitsou | Surgical denervation led to long-term survival in a rat model | [34] |
| Coarfa | Chemical denervation with Botox caused apoptosis in a mouse model | [59] |
| Guo | Perineural invasion is present in many different cancers and associated with cancer invasion, recurrence, and metastasis | [60] |
| Saloman | The capsaicin-induced ablation of the innervation of the neonatal pancreas causes a delay in tumor formation | [61] |
| Magnon | Axonogenesis in prostate cancer can contribute to cancer growth and dissemination in a mouse model | [58] |
| Campell | Adrenergic signaling activates osteoblasts that favor bone metastasis | [62] |
| Griffin | Cancer cells can release the NGF, which influences tumor neurogenesis. Nerves infiltrate the TME and secrete neurotransmitters, which stimulate tumor cell growth and angiogenesis | [63] |
| Blondy | Neurotrophins are key messengers in the crosstalk between cancer cells and peripheral nerve fibers | [64] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benzaquen, D.; Lawrence, Y.R.; Taussky, D.; Zwahlen, D.; Oehler, C.; Champion, A. The Crosstalk between Nerves and Cancer—A Poorly Understood Phenomenon and New Possibilities. Cancers 2024, 16, 1875. https://doi.org/10.3390/cancers16101875
Benzaquen D, Lawrence YR, Taussky D, Zwahlen D, Oehler C, Champion A. The Crosstalk between Nerves and Cancer—A Poorly Understood Phenomenon and New Possibilities. Cancers. 2024; 16(10):1875. https://doi.org/10.3390/cancers16101875
Chicago/Turabian StyleBenzaquen, David, Yaacov R. Lawrence, Daniel Taussky, Daniel Zwahlen, Christoph Oehler, and Ambroise Champion. 2024. "The Crosstalk between Nerves and Cancer—A Poorly Understood Phenomenon and New Possibilities" Cancers 16, no. 10: 1875. https://doi.org/10.3390/cancers16101875
APA StyleBenzaquen, D., Lawrence, Y. R., Taussky, D., Zwahlen, D., Oehler, C., & Champion, A. (2024). The Crosstalk between Nerves and Cancer—A Poorly Understood Phenomenon and New Possibilities. Cancers, 16(10), 1875. https://doi.org/10.3390/cancers16101875