
Radiotherapy for Mobile Spine and Sacral Chordoma: A Critical Review and Practical Guide from the Spine Tumor Academy

 ,
,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
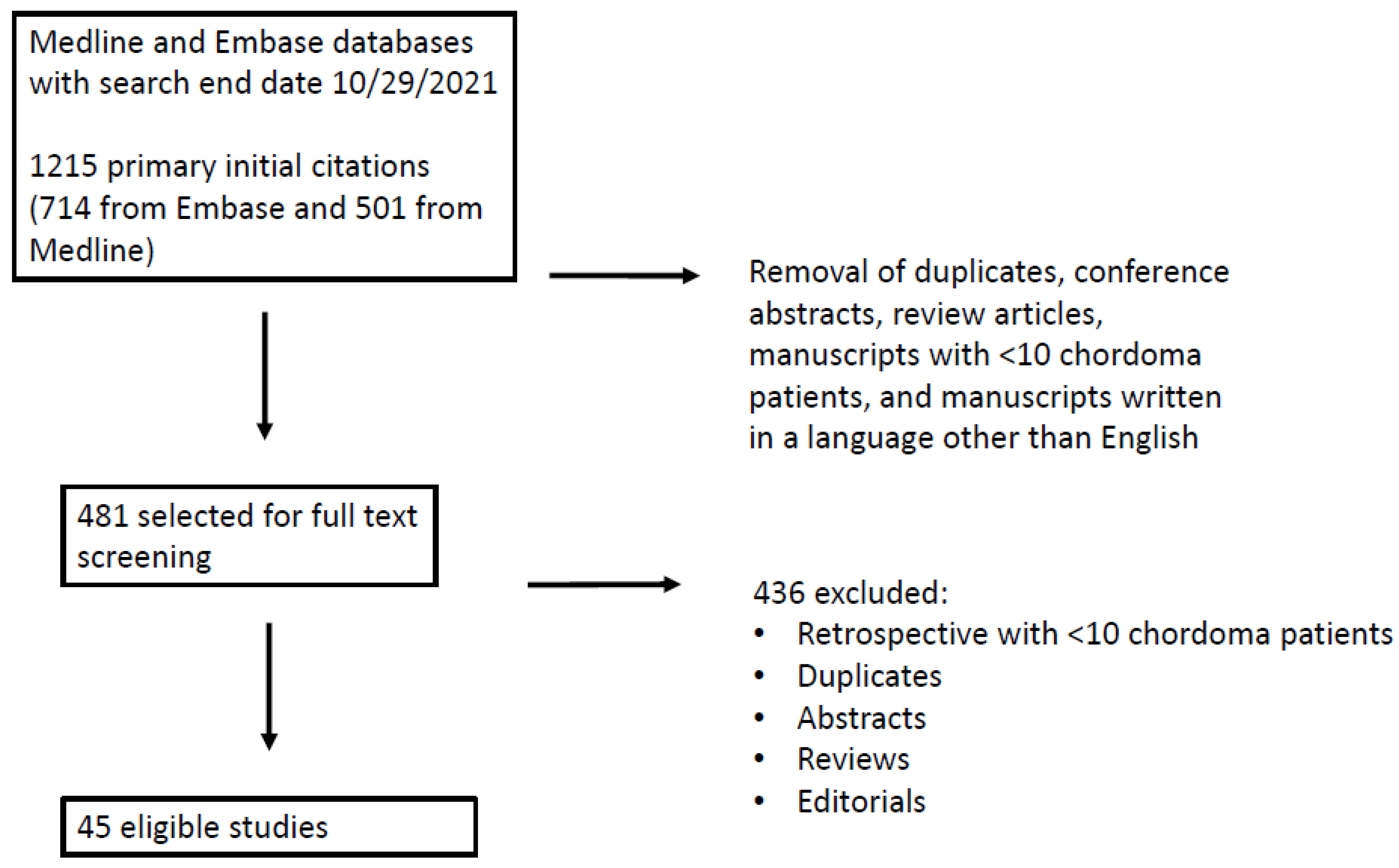
2.1. Search Strategy
2.2. Outcome Measures
3. Results
3.1. Proton Beam Therapy
3.2. Carbon Ion and Other Heavy Particle Therapy
3.3. Stereotactic Body Radiation Therapy (SBRT)
3.4. Radiation Alone
3.5. Timing of RT
3.6. Summary of Ongoing Clinical Trials
3.7. Summary of Radiotherapy Recommendations
3.8. Limitations
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Scampa, M.; Tessitore, E.; Dominguez, D.E.; Hannouche, D.; Buchs, N.C.; Kalbermatten, D.F.; Oranges, C.M. Sacral Chordoma: A Population-Based Analysis of Epidemiology and Survival Outcomes. Anticancer Res. 2022, 42, 929–937. [Google Scholar] [CrossRef] [PubMed]
- McPherson, C.M.; Suki, D.; McCutcheon, I.E.; Gokaslan, Z.L.; Rhines, L.D.; Mendel, E. Metastatic Disease from Spinal Chordoma: A 10-Year Experience. J. Neurosurg. Spine 2006, 5, 277–280. [Google Scholar] [CrossRef] [PubMed]
- DeLaney, T.F.; Liebsch, N.J.; Pedlow, F.X.; Adams, J.; Dean, S.; Yeap, B.Y.; McManus, P.; Rosenberg, A.E.; Nielsen, G.P.; Harmon, D.C.; et al. Phase II Study of High-Dose Photon/Proton Radiotherapy in the Management of Spine Sarcomas. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 732–739. [Google Scholar] [CrossRef] [PubMed]
- DeLaney, T.F.; Liebsch, N.J.; Pedlow, F.X.; Adams, J.; Weyman, E.A.; Yeap, B.Y.; Depauw, N.; Nielsen, G.P.; Harmon, D.C.; Yoon, S.S.; et al. Long-Term Results of Phase II Study of High Dose Photon/Proton Radiotherapy in the Management of Spine Chordomas, Chondrosarcomas, and Other Sarcomas. J. Surg. Oncol. 2014, 110, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Stieb, S.; Snider, J.W., 3rd; Placidi, L.; Kliebsch, U.; Lomax, A.J.; Schneider, R.A.; Weber, D.C. Long-Term Clinical Safety of High-Dose Proton Radiation Therapy Delivered with Pencil Beam Scanning Technique for Extracranial Chordomas and Chondrosarcomas in Adult Patients: Clinical Evidence of Spinal Cord Tolerance. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Indelicato, D.J.; Rotondo, R.L.; Begosh-Mayne, D.; Scarborough, M.T.; Gibbs, C.P.; Morris, C.G.; Mendenhall, W.M. A Prospective Outcomes Study of Proton Therapy for Chordomas and Chondrosarcomas of the Spine. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 297–303. [Google Scholar] [CrossRef]
- Wagner, T.D.; Kobayashi, W.; Dean, S.; Goldberg, S.I.; Kirsch, D.G.; Suit, H.D.; Hornicek, F.J.; Pedlow, F.X.; Raskin, K.A.; Springfield, D.S.; et al. Combination Short-Course Preoperative Irradiation, Surgical Resection, and Reduced-Field High-Dose Postoperative Irradiation in the Treatment of Tumors Involving the Bone. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 259–266. [Google Scholar] [CrossRef]
- Chen, Y.L.; Liebsch, N.; Kobayashi, W.; Goldberg, S.; Kirsch, D.; Calkins, G.; Childs, S.; Schwab, J.; Hornicek, F.; DeLaney, T. Definitive High-Dose Photon/Proton Radiotherapy for Unresected Mobile Spine and Sacral Chordomas. Spine 2013, 38, 930. [Google Scholar] [CrossRef]
- Beddok, A.; Saint-Martin, C.; Mammar, H.; Feuvret, L.; Helfre, S.; Bolle, S.; Froelich, S.; Goudjil, F.; Zefkili, S.; Amessis, M.; et al. High-Dose Proton Therapy and Tomotherapy for the Treatment of Sacral Chordoma: A Retrospective Monocentric Study. Acta Oncol. 2021, 60, 245–251. [Google Scholar] [CrossRef]
- Hug, E.B.; Fitzek, M.M.; Liebsch, N.J.; Munzenrider, J.E. Locally Challenging Osteo- and Chondrogenic Tumors of the Axial Skeleton: Results of Combined Proton and Photon Radiation Therapy using Three-Dimensional Treatment Planning. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 467–476. [Google Scholar] [CrossRef]
- Houdek, M.T.; Rose, P.S.; Hevesi, M.; Schwab, J.H.; Griffin, A.M.; Healey, J.H.; Petersen, I.A.; DeLaney, T.F.; Chung, P.W.; Yaszemski, M.J.; et al. Low Dose Radiotherapy is Associated with Local Complications but Not Disease Control in Sacral Chordoma. J. Surg. Oncol. 2019, 119, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Austin, J.P.; Urie, M.M.; Cardenosa, G.; Munzenrider, J.E. Probable Causes of Recurrence in Patients with Chordoma and Chondrosarcoma of the Base of Skull and Cervical Spine. Int. J. Radiat. Oncol. Biol. Phys. 1993, 25, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Fagundes, M.A.; Hug, E.B.; Liebsch, N.J.; Daly, W.; Efird, J.; Munzenrider, J.E. Radiation Therapy for Chordomas of the Base of Skull and Cervical Spine: Patterns of Failure and Outcome After Relapse. Int. J. Radiat. Oncol. Biol. Phys. 1995, 33, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Tsuda, Y.; Stevenson, J.; Parry, M.; Jeys, L. Sacral Chordoma: Do the Width of Surgical Margin and the Use of Photon/Proton Radiotherapy Affect Local Disease Control? Int. Orthop. 2020, 44, 381–389. [Google Scholar] [CrossRef]
- Park, L.; Delaney, T.F.; Liebsch, N.J.; Hornicek, F.J.; Goldberg, S.; Mankin, H.; Rosenberg, A.E.; Rosenthal, D.I.; Suit, H.D. Sacral Chordomas: Impact of High-Dose Proton/Photon-Beam Radiation Therapy Combined with Or without Surgery for Primary Versus Recurrent Tumor. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 1514–1521. [Google Scholar] [CrossRef]
- Chowdhry, V.K.; Liu, L.; Goldberg, S.; Adams, J.A.; De Amorim Bernstein, K.; Liebsch, N.J.; Niemierko, A.; Chen, Y.L.; DeLaney, T.F. Thoracolumbar Spinal Cord Tolerance to High Dose Conformal Proton-Photon Radiation Therapy. Radiother. Oncol. 2016, 119, 35–39. [Google Scholar] [CrossRef]
- Kabolizadeh, P.; Chen, Y.L.; Liebsch, N.; Hornicek, F.J.; Schwab, J.H.; Choy, E.; Rosenthal, D.I.; Niemierko, A.; DeLaney, T.F. Updated Outcome and Analysis of Tumor Response in Mobile Spine and Sacral Chordoma Treated with Definitive High-Dose Photon/Proton Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 254–262. [Google Scholar] [CrossRef]
- Walser, M.; Bojaxhiu, B.; Kawashiro, S.; Tran, S.; Beer, J.; Leiser, D.; Pica, A.; Bachtiary, B.; Weber, D.C. Clinical Outcome of Sacral Chordoma Patients Treated with Pencil Beam Scanning Proton Therapy. Clin. Oncol. 2021, 33, e578–e585. [Google Scholar] [CrossRef]
- Rotondo, R.L.; Folkert, W.; Liebsch, N.J.; Chen, Y.L.; Pedlow, F.X.; Schwab, J.H.; Rosenberg, A.E.; Nielsen, G.P.; Szymonifka, J.; Ferreira, A.E.; et al. High-Dose Proton-Based Radiation Therapy in the Management of Spine Chordomas: Outcomes and Clinicopathological Prognostic Factors. J. Neurosurg. Spine 2015, 23, 788–797. [Google Scholar] [CrossRef]
- Snider, J.W.; Schneider, R.A.; Poelma-Tap, D.; Stieb, S.; Murray, F.R.; Placidi, L.; Albertini, F.; Lomax, A.; Bolsi, A.; Kliebsch, U.; et al. Long-Term Outcomes and Prognostic Factors after Pencil-Beam Scanning Proton Radiation Therapy for Spinal Chordomas: A Large, Single-Institution Cohort. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 226–233. [Google Scholar] [CrossRef]
- Aibe, N.; Demizu, Y.; Sulaiman, N.S.; Matsuo, Y.; Mima, M.; Nagano, F.; Terashima, K.; Tokumaru, S.; Hayakawa, T.; Suga, M.; et al. Outcomes of Patients with Primary Sacral Chordoma Treated with Definitive Proton Beam Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Murray, F.R.; Snider, J.W.; Schneider, R.A.; Walser, M.; Bolsi, A.; Pica, A.; Lomax, A.J.; Weber, D.C. Prognostic Factors for Spinal Chordomas and Chondrosarcomas Treated with Postoperative Pencil-Beam Scanning Proton Therapy: A Large, Single-Institution Experience. J. Neurosurg. Spine 2020, 32, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Tsugawa, D.; Komatsu, S.; Demizu, Y.; Sulaiman, N.S.; Suga, M.; Kido, M.; Toyama, H.; Okimoto, T.; Sasaki, R.; Fukumoto, T. Space-Making Particle Therapy with Surgical Spacer Placement in Patients with Sacral Chordoma. J. Am. Coll. Surg. 2020, 230, 207–215. [Google Scholar] [CrossRef]
- Staab, A.; Rutz, H.P.; Ares, C.; Timmermann, B.; Schneider, R.; Bolsi, A.; Albertini, F.; Lomax, A.; Goitein, G.; Hug, E. Spot-Scanning-Based Proton Therapy for Extracranial Chordoma. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 489. [Google Scholar] [CrossRef]
- Kim, Y.J.; Cho, K.H.; Lim, Y.K.; Park, J.; Kim, J.Y.; Shin, K.H.; Kim, T.H.; Moon, S.H.; Lee, S.H.; Yoo, H. The Volumetric Change and Dose-Response Relationship Following Hypofractionated Proton Therapy for Chordomas. Acta Oncol. 2014, 53, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Mastella, E.; Molinelli, S.; Magro, G.; Mirandola, A.; Russo, S.; Vai, A.; Mairani, A.; Choi, K.; Fiore, M.R.; Fossati, P.; et al. Dosimetric Characterization of Carbon Fiber Stabilization Devices for Post-Operative Particle Therapy. Phys. Med. 2017, 44, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Ringel, F.; Ryang, Y.M.; Kirschke, J.S.; Müller, B.S.; Wilkens, J.J.; Brodard, J.; Combs, S.E.; Meyer, B. Radiolucent Carbon Fiber-Reinforced Pedicle Screws for Treatment of Spinal Tumors: Advantages for Radiation Planning and Follow-Up Imaging. World Neurosurg. 2017, 105, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Mima, M.; Demizu, Y.; Jin, D.; Hashimoto, N.; Takagi, M.; Terashima, K.; Fujii, O.; Niwa, Y.; Akagi, T.; Daimon, T.; et al. Particle Therapy using Carbon Ions Or Protons as a Definitive Therapy for Patients with Primary Sacral Chordoma. Br. J. Radiol. 2014, 87, 20130512. [Google Scholar] [CrossRef]
- Combs, S.E.; Schulz-Ertner, D.; Herfarth, K.K.; Krempien, R.; Debus, J. Advances in Radio-Oncology. from Precision Radiotherapy with Photons to Ion Therapy with Protons and Carbon Ions. Chirurg 2006, 77, 1126–1132. [Google Scholar] [CrossRef]
- Ilicic, K.; Combs, S.E.; Schmid, T.E. New Insights in the Relative Radiobiological Effectiveness of Proton Irradiation. Radiat. Oncol. 2018, 13, 6–9. [Google Scholar] [CrossRef]
- Liermann, J.; Naumann, P.; Fortunato, F.; Schmid, T.E.; Weber, K.J.; Debus, J.; Combs, S.E. Phytotherapeutics Oridonin and Ponicidin show Additive Effects Combined with Irradiation in Pancreatic Cancer in vitro. Radiol. Oncol. 2017, 51, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Rieken, S.; Rieber, J.; Brons, S.; Habermehl, D.; Rief, H.; Orschiedt, L.; Lindel, K.; Weber, K.J.; Debus, J.; Combs, S.E. Radiation-Induced Motility Alterations in Medulloblastoma Cells. J. Radiat. Res. 2015, 56, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Habermehl, D.; Ilicic, K.; Dehne, S.; Rieken, S.; Orschiedt, L.; Brons, S.; Haberer, T.; Weber, K.J.; Debus, J.; Combs, S.E. The Relative Biological Effectiveness for Carbon and Oxygen Ion Beams using the Raster-Scanning Technique in Hepatocellular Carcinoma Cell Lines. PLoS ONE 2014, 9, e113591. [Google Scholar] [CrossRef] [PubMed]
- Schlaich, F.; Brons, S.; Haberer, T.; Debus, J.; Combs, S.E.; Weber, K.J. Comparison of the Effects of Photon Versus Carbon Ion Irradiation when Combined with Chemotherapy In Vitro. Radiat. Oncol. 2013, 8, 260. [Google Scholar] [CrossRef]
- El Shafie, R.A.; Habermehl, D.; Rieken, S.; Mairani, A.; Orschiedt, L.; Brons, S.; Haberer, T.; Weber, K.J.; Debus, J.; Combs, S.E. In Vitro Evaluation of Photon and Raster-Scanned Carbon Ion Radiotherapy in Combination with Gemcitabine in Pancreatic Cancer Cell Lines. J. Radiat. Res. 2013, 54 (Suppl. S1), 113. [Google Scholar] [CrossRef]
- Harrabi, S.; Combs, S.E.; Brons, S.; Haberer, T.; Debus, J.; Weber, K.J. Temozolomide in Combination with Carbon Ion Or Photon Irradiation in Glioblastoma Multiforme Cell Lines—Does Scheduling Matter? Int. J. Radiat. Biol. 2013, 89, 692–697. [Google Scholar] [CrossRef]
- Combs, S.E.; Zipp, L.; Rieken, S.; Habermehl, D.; Brons, S.; Winter, M.; Haberer, T.; Debus, J.; Weber, K.J. In Vitro Evaluation of Photon and Carbon Ion Radiotherapy in Combination with Chemotherapy in Glioblastoma Cells. Radiat. Oncol. 2012, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Dobiasch, S.; Schneider, G.; Schmid, R.M.; Azimzadeh, O.; Kanev, K.; Buschmann, D.; Pfaffl, M.W.; Bartzsch, S.; Schmid, T.E.; et al. Impact of DNA Repair and Reactive Oxygen Species Levels on Radioresistance in Pancreatic Cancer. Radiother. Oncol. 2021, 159, 265–276. [Google Scholar] [CrossRef]
- Koto, M.; Ikawa, H.; Kaneko, T.; Hagiwara, Y.; Hayashi, K.; Tsuji, H. Long-Term Outcomes of Skull Base Chordoma Treated with High-Dose Carbon-Ion Radiotherapy. Head Neck 2020, 42, 2607–2613. [Google Scholar] [CrossRef]
- Uhl, M.; Mattke, M.; Welzel, T.; Roeder, F.; Oelmann, J.; Habl, G.; Jensen, A.; Ellerbrock, M.; Jäkel, O.; Haberer, T.; et al. Highly Effective Treatment of Skull Base Chordoma with Carbon Ion Irradiation using a Raster Scan Technique in 155 Patients: First Long-Term Results. Cancer 2014, 120, 3410–3417. [Google Scholar] [CrossRef]
- Bostel, T.; Nicolay, N.H.; Welzel, T.; Bruckner, T.; Mattke, M.; Akbaba, S.; Sprave, T.; Debus, J.; Uhl, M. Sacral Insufficiency Fractures After High-Dose Carbon-Ion Based Radiotherapy of Sacral Chordomas. Radiat. Oncol. 2018, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- Schoenthaler, R.; Castro, J.R.; Petti, P.L.; Baken-Brown, K.; Phillips, T.L. Charged Particle Irradiation of Sacral Chordomas. Int. J. Radiat. Oncol. Biol. Phys. 1993, 26, 291–298. [Google Scholar] [CrossRef]
- Breteau, N.; Demasure, M.; Favre, A.; Leloup, R.; Lescrainier, J.; Sabattier, R. Fast Neutron Therapy for Inoperable or Recurrent Sacrococcygeal Chordomas. Bull. Cancer Radiother. 1996, 83, 142s–145s. [Google Scholar] [CrossRef]
- Pennington, Z.; Ehresman, J.; McCarthy, E.F.; Ahmed, A.K.; Pittman, P.D.; Lubelski, D.; Goodwin, C.R.; Sciubba, D.M. Chordoma of the Sacrum and Mobile Spine: A Narrative Review. Spine J. 2021, 21, 500–517. [Google Scholar] [CrossRef] [PubMed]
- Uhl, M.; Welzel, T.; Jensen, A.; Ellerbrock, M.; Haberer, T.; Jäkel, O.; Herfarth, K.; Debus, J. Carbon Ion Beam Treatment in Patients with Primary and Recurrent Sacrococcygeal Chordoma. Strahlenther. Onkol. 2015, 191, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Imai, R.; Kamada, T.; Araki, N.; Working Group for Bone and Soft Tissue Sarcomas. Carbon Ion Radiation Therapy for Unresectable Sacral Chordoma: An Analysis of 188 Cases. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Imai, R.; Kamada, T.; Sugahara, S.; Tsuji, H.; Tsujii, H. Carbon Ion Radiotherapy for Sacral Chordoma. Br. J. Radiol. 2011, 84, 48. [Google Scholar] [CrossRef] [PubMed]
- Demizu, Y.; Imai, R.; Kiyohara, H.; Matsunobu, A.; Okamoto, M.; Okimoto, T.; Tsuji, H.; Ohno, T.; Shioyama, Y.; Nemoto, K.; et al. Carbon Ion Radiotherapy for Sacral Chordoma: A Retrospective Nationwide Multicentre Study in Japan. Radiother. Oncol. 2021, 154, 1–5. [Google Scholar] [CrossRef]
- Evangelisti, G.; Fiore, M.R.; Bandiera, S.; Barbanti Brodano, G.; Terzi, S.; Girolami, M.; Pipola, V.; Righi, A.; Nanni, C.; Fanti, S.; et al. Carbon Ions Therapy as Single Treatment in Chordoma of the Sacrum. Histologic and Metabolic Outcome Studies. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4002–4009. [Google Scholar]
- Serizawa, I.; Imai, R.; Kamada, T.; Tsuji, H.; Kishimoto, R.; Kandatsu, S.; Tsujii, H.; Tatezaki, S. Changes in Tumor Volume of Sacral Chordoma after Carbon Ion Radiotherapy. J. Comput. Assist. Tomogr. 2009, 33, 795–798. [Google Scholar] [CrossRef]
- Imai, R.; Kamada, T.; Tsuji, H.; Sugawara, S.; Serizawa, I.; Tsujii, H.; Tatezaki, S.; Working Group for Bone and Soft Tissue Sarcomas. Effect of Carbon Ion Radiotherapy for Sacral Chordoma: Results of Phase I-II and Phase II Clinical Trials. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 1470–1476. [Google Scholar] [CrossRef]
- Bostel, T.; Mattke, M.; Nicolay, N.H.; Welzel, T.; Wollschläger, D.; Akbaba, S.; Mayer, A.; Sprave, T.; Debus, J.; Uhl, M. High-Dose Carbon-Ion Based Radiotherapy of Primary and Recurrent Sacrococcygeal Chordomas: Long-Term Clinical Results of a Single Particle Therapy Center. Radiat. Oncol. 2020, 15, 206–208. [Google Scholar] [CrossRef] [PubMed]
- Preda, L.; Stoppa, D.; Fiore, M.R.; Fontana, G.; Camisa, S.; Sacchi, R.; Ghitti, M.; Viselner, G.; Fossati, P.; Valvo, F.; et al. MRI Evaluation of Sacral Chordoma Treated with Carbon Ion Radiotherapy Alone. Radiother. Oncol. 2018, 128, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Henderson, F.C.; McCool, K.; Seigle, J.; Jean, W.; Harter, W.; Gagnon, G.J. Treatment of Chordomas with CyberKnife: Georgetown University Experience and Treatment Recommendations. Neurosurgery 2009, 64, 44. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Laufer, I.; Cox, B.W.; Lovelock, D.M.; Maki, R.G.; Zatcky, J.M.; Boland, P.J.; Bilsky, M.H. Preliminary Results of High-Dose Single-Fraction Radiotherapy for the Management of Chordomas of the Spine and Sacrum. Neurosurgery 2013, 73, 673–680; discussion 680. [Google Scholar] [CrossRef] [PubMed]
- Chang, U.K.; Lee, D.H.; Kim, M.S. Stereotactic Radiosurgery for Primary Malignant Spinal Tumors. Neurol. Res. 2014, 36, 597–606. [Google Scholar] [CrossRef]
- Jung, E.W.; Jung, D.L.; Balagamwala, E.H.; Angelov, L.; Suh, J.H.; Djemil, T.; Magnelli, A.; Chao, S.T. Single-Fraction Spine Stereotactic Body Radiation Therapy for the Treatment of Chordoma. Technol. Cancer. Res. Treat. 2017, 16, 302–309. [Google Scholar] [CrossRef]
- Lockney, D.T.; Shub, T.; Hopkins, B.; Lockney, N.A.; Moussazadeh, N.; Lis, E.; Yamada, Y.; Schmitt, A.M.; Higginson, D.S.; Laufer, I.; et al. Spinal Stereotactic Body Radiotherapy Following Intralesional Curettage with Separation Surgery for Initial or Salvage Chordoma Treatment. Neurosurg. Focus. 2017, 42, E4. [Google Scholar] [CrossRef]
- Lu, S.; Peng, X.; Zou, B.; Zhou, C.; Feng, M.; Lang, J. Adjuvant Gamma Knife Surgery and Image-Guided, Intensity-Modulated Radiation Therapy for the Treatment of Sacral Chordomas. Rep. Pract. Oncol. Radiother. 2019, 24, 74–79. [Google Scholar] [CrossRef]
- Jin, C.J.; Berry-Candelario, J.; Reiner, A.S.; Laufer, I.; Higginson, D.S.; Schmitt, A.M.; Lis, E.; Barzilai, O.; Boland, P.; Yamada, Y.; et al. Long-Term Outcomes of High-Dose Single-Fraction Radiosurgery for Chordomas of the Spine and Sacrum. J. Neurosurg. Spine 2019, 32, 79–88. [Google Scholar] [CrossRef]
- Chen, X.; Lo, S.L.; Bettegowda, C.; Ryan, D.M.; Gross, J.M.; Hu, C.; Kleinberg, L.; Sciubba, D.M.; Redmond, K.J. High-Dose Hypofractionated Stereotactic Body Radiotherapy for Spinal Chordoma. J. Neurosurg. Spine 2021, 35, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Eid, A.S.; Chang, U.K.; Lee, S.Y.; Jeon, D.G. The Treatment Outcome Depending on the Extent of Resection in Skull Base and Spinal Chordomas. Acta Neurochir. 2011, 153, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Cox, B.W.; Spratt, D.E.; Lovelock, M.; Bilsky, M.H.; Lis, E.; Ryu, S.; Sheehan, J.; Gerszten, P.C.; Chang, E.; Gibbs, I.; et al. International Spine Radiosurgery Consortium Consensus Guidelines for Target Volume Definition in Spinal Stereotactic Radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 597. [Google Scholar] [CrossRef] [PubMed]
- Redmond, K.J.; Robertson, S.; Lo, S.S.; Soltys, S.G.; Ryu, S.; McNutt, T.; Chao, S.T.; Yamada, Y.; Ghia, A.; Chang, E.L.; et al. Consensus Contouring Guidelines for Postoperative Stereotactic Body Radiation Therapy for Metastatic Solid Tumor Malignancies to the Spine. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 64–74. [Google Scholar] [CrossRef]
- Radaelli, S.; Fossati, P.; Stacchiotti, S.; Akiyama, T.; Ascencio, J.M.; Bandiera, S.; Boglione, A.; Boland, P.; Bolle, S.; Bruland, O.; et al. The Sacral Chordoma Margin. Eur. J. Surg. Onc. 2020, 46, 1415–1422. [Google Scholar] [CrossRef]
- Ailon, T.; Torabi, R.; Fisher, C.G.; Rhines, L.D.; Clarke, M.J.; Bettegowda, C.; Boriani, S.; Yamada, Y.J.; Kawahara, N.; Varga, P.P.; et al. Management of Locally Recurrent Chordoma of the Mobile Spine and Sacrum: A Systematic Review. Spine 2016, 41, S193–S198. [Google Scholar] [CrossRef]
- Walcott, B.P.; Nahed, B.V.; Mohyeldin, A.; Coumans, J.V.; Kahle, K.T.; Ferreira, M.J. Chordoma: Current Concepts, Management, and Future Directions. Lancet Oncol. 2012, 13, e69–e76. [Google Scholar] [CrossRef]


{kind=link}
| Author, Journal, Year Published | Study Type | Number of Patients | Median Follow-Up (mo) | Extent of Resection | Radiation Timing | Prescription Dose (Range)/Dose per Fraction | Local Control | Overall Survival | Toxicity |
|---|---|---|---|---|---|---|---|---|---|
| Austin, IJROBP, 1993 [12] | Retrospective | 26 | NR | Biopsy, STR, GTR | RT alone, adjuvant | Gross disease—70 Gy RBE/1.8–2 Gy RBE fractions Microscopic disease—45–50 Gy | Crude 62% | NR | NR |
| Fagundes, IJROBP, 1995 [13] | Retrospective | 69 | 39 | STR, GTR | Adjuvant | Median 70.1 Gy RBE (66.6–77.4) | Crude 65% | NR | NR |
| Hug, IJROBP, 1995 [10] | Retrospective | 14 ‡ | 38 | Biopsy, STR, GTR | RT alone, pre/postoperative, adjuvant | Mean 74.6 Gy RBE (67.1–82)/1.8–2 Gy fractions | 5 yr 53% | 5 yr 50% | 6% attributable to RT |
| Park, IJROBP, 2006 [15] | Retrospective | 27 | 47 | Biopsy, STR, GTR | RT alone, adjuvant | Primary—Mean 71 Gy RBE/1.97 Gy RBE fractions Recurrent—Mean 77 Gy RBE/1.88 Gy RBE fractions | 5 yr 71.7% | 5 yr 82.5% | 37% abnormal bowel function; 30% pain; 19% abnormal bladder function; 11% difficulty ambulating |
| Wagner, IJROBP, 2009 [7] | Retrospective | 25 | 32 | STR, GTR | Pre/postoperative, adjuvant | Preoperative—Median 20 Gy RBE (9–29.4) Postoperative—Median 50.4 Gy RBE (18–61.2) | 5 yr 73.3% | 5 yr 65% | 21% delayed wound healing; 11% late toxicity |
| Staab, IJROBP, 2011 [24] | Retrospective | 40 | NR | Biopsy, STR, GTR | RT alone, adjuvant | Mean 72.5 Gy RBE (59.4–75.2)/1.8–2 Gy RBE fractions (93% received ≥ 70 Gy RBE) | 5 yr 62% | 5 yr 80% | 4% G3 osteonecrosis, 4% subcutaneous fistula requiring wound debridement; 0% G3 neuro, kidney, and bowel toxicity |
| Chen, Spine, 2013 [8] | Retrospective | 24 | 56 | Biopsy | RT alone | Median 77.4 Gy (70.2–79)/1.8–2 Gy RBE fractions Median photon contribution 34 Gy (0–57.6) Median proton contribution 45 Gy RBE (9.8–79.2) | 5 yr 79.8% | 5 yr 78.1% | 33% sacral insufficiency fracture (none requiring stabilization); 17% G2 rectal bleeding; 8% worsening fecal/urine incontinence; 4% foot drop; 4% perineal numbness; 4% erectile dysfunction; 1% secondary malignancy |
| Kim, Acta Oncol, 2014 [25] | Retrospective | 12 | 43 | STR, GTR | RT alone, adjuvant | Median NR (64.8–79.2)/2.4 Gy RBE fractions | Crude 83% | NR | 17% G3 skin/subcutaneous contracture; 8% G3 rectal bleeding |
| Delaney, J Surg Onc, 2014 [4] | Prospective phase II | 29 | 88 (among alive patients) | Biopsy, STR, GTR | RT alone, pre/postoperative, adjuvant | Median 76.6 Gy (59.4–77.4)/1.8–2 Gy RBE fractions | 5 yr 81% | 5 yr 84% | 13% 8 yr actuarial risk of G3–G4 late RT morbidity; 3 sacral neuropathies (all after doses of 76.6–77.4 Gy); no myelopathies |
| Rotondo, J Neurosurg Spine, 2015 [19] | Retrospective | 126 | 47 | Biopsy, STR, GTR | RT alone, pre/postoperative, adjuvant | Median 72.4 Gy RBE (46.3–83.6)/1.8–2 Gy RBE fractions | 5 yr 62% | 5 yr 81% | 22% wound complications with preoperative RT, 12% with postoperative RT; 5% insufficiency fracture; 3% motor neuropathy; 2% spine non-union/hardware failure; 1% secondary malignancy; 1% proctitis; 1% osteonecrosis; 1% erectile dysfunction |
| Indelicato, IJROBP, 2016 [6] | Retrospective | 34 | 44 | Biopsy, STR, GTR | RT alone, adjuvant | CTV + 5 mm–Median 45 Gy RBE/1.8–2 Gy RBE fractions GTV + 5 mm–Median 70.2 Gy RBE (65–75)/1.8–2 Gy RBE fractions daily or 1.2 Gy RBE fractions BID | 4 yr 67% | 4 yr 72% | 5% G3–G4 soft tissue toxicity/wound healing; 5% secondary malignancy; 2% compression fracture requiring stabilization; 2% bilateral G2 radiation nephritis |
| Chowdhry, IJROBP, 2016 [16] | Retrospective | 29 | 13 | NR | Pre/postoperative, adjuvant | Preoperative—Median 36 Gy RBE (18–78.2)/1.8–2 Gy RBE fractions Adjuvant—Median 70.2 Gy RBE (59.4–78.2)/1.8–2 Gy RBE fractions Photon contribution—19.8–30.6 Gy Proton contribution—Remaining dose | NR | 5 yr 86.9% | 7% G2+ neurologic injury |
| Kabolizadeh, IJROBP, 2017 [17] | Retrospective | 40 | 50 | Biopsy | RT alone | Median 77.4 Gy RBE (64.8–79.2) Photon contribution—Median 30.6 Gy (0–68) Proton contribution—Median 46.8 Gy RBE (0–79.2) | 5 yr 85.4% | 5 yr 81.9% | 25% sacral stress fracture (none requiring surgical stabilization); 10% G2 rectal bleeding; 5% urinary/fecal incontinence; 5% secondary malignancy; 5% foot drop; 3% erectile dysfunction; 3% perineal numbness; 3% bowel fistula/perforation |
| Stieb, IJROBP, 2018 [5] | Retrospective | 55 | 66 | Biopsy, STR, GTR | RT alone, adjuvant | Median 73.9 Gy RBE (59–75.2)/1.8–2 Gy RBE fractions | 5 yr 61% | Median 65 mo 5 yr 75% | 5% acute RT-induced neurotoxicity (1% G1, 4% G2); 16% late neurologic toxicity (9% G1, 5% G2, 1% G4) |
| Snider, IJROBP, 2018 [20] | Retrospective | 100 | 65 | Biopsy | RT alone, adjuvant | Median 74 Gy RBE (59.4–77)/1.8–2 Gy RBE fractions (95% received ≥ 70 Gy) | 5 yr 63% | Median 157 mo 5 yr 81% | 11% G3 |
| Aibe, IJROBP, 2018 [21] | Retrospective | 33 | 37 | Biopsy | RT alone | 70.4 Gy RBE/2.2 Gy RBE fractions | 3 yr 89.6% | 3 yr 92.7% | 13% acute G3; 3% leg numbness |
| Tsugawa, J Am Coll Surg, 2020 [23] | Retrospective | 21 | 50 | Biopsy | RT alone | Early treatment era—70.4 Gy RBE/4.4 Gy RBE fractions Modern era—70.4 Gy RBE/2.2 Gy RBE fractions | 4 yr 68.4% | 5 yr 100% | 19% acute G3 dermatitis; 5% late G4 dermatitis |
| Houdek, J Surg Onc, 2019 [11] | Retrospective | 89 | 84 | STR, GTR | Pre/postoperative, neoadjuvant, adjuvant | Pre/postoperative—Mean 70.9 Gy RBE (±5.7) Neoadjuvant—50 Gy RBE Adjuvant—Mean 60.2 Gy RBE (±9.9) | 5 yr 80% | Median 60 mo | 39% wound dehiscence/delayed healing; 20% sacral stress fracture; 3% secondary malignancy; 3% small bowel obstruction; 1% enteric fistula |
| Fujiwara, Int Orthop, 2020 [14] | Retrospective | 11 | 77 | GTR | Adjuvant | NR | 5 yr 82% | NR | NR |
| Murray, J Neurosurg Spine, 2020 [22] | Retrospective | 116 | 65 | STR, GTR | Adjuvant | Median 74 Gy RBE (59.4–77) | 5 yr 67.9% | 5 yr 81.6% | 34% long-term RT-induced toxicity: 7% G3, 1% G4 (myelitis causing quadriplegia, laryngeal necrosis requiring hyperbaric oxygen) |
| Beddok, Acta Oncologica, 2021 [9] | Retrospective | 28 | 34 | Biopsy, STR | RT alone, adjuvant | CTV—Median NR (52.2–54 Gy RBE)/1.8–2 Gy RBE fractions GTV + 5 mm–Median NR (70–73.8 Gy RBE)/1.8–2 Gy RBE fractions | 5 yr 75% | 5 yr 74.5% | 14% G2 & 4% G3 late pain; 4% G2 late fibrosis; 9% G2 late cauda equina syndrome |
| Walser, Clinical Oncology, 2021 [18] | Retrospective | 60 | 48 | Biopsy, STR, GTR | RT alone, adjuvant | Median 74 Gy RBE (60–77)/1.8–3 Gy RBE fractions | 4 yr 77% | 4 yr 85% | Acute: 43% G2, 10% G3 Late: 30% G2, 5% G3 (3% sacral insufficiency fracture, 1% neuropathic pain interfering with ADL), 3% G4–G5 (secondary malignancy) |
| Author, Journal, Year Published | Study Type | Number of Patients | Median Follow-Up (mo) | Extent of Resection | Radiation Type and Timing | Prescription Dose (Range)/Dose per Fraction | Local Control | Overall Survival | Toxicity |
|---|---|---|---|---|---|---|---|---|---|
| Mima, Br J Radiol, 2014 [28] | Retrospective | 23 | 38 | Biopsy | Carbon ion or proton alone | 70.4 Gy RBE/2.2 or 4.4 Gy RBE fractions | 3 yr 94% | 3 yr 83% | 39% grade 3 or greater acute 22% late grade 4 dermatitis; 17% grade 3 neuropathies; 9% grade 3 myositis |
| Uhl, Strahlenther Onkol, 2015 [45] | Retrospective | 56 | 25 | Biopsy, STR, GTR | Carbon ion alone or adjuvant ± photon | Median 66 Gy RBE (range 60–74)/3 Gy RBE fractions | 3 yr 53% | 100% | 0% new grade 3 or greater toxicity |
| Imai, IJROBP, 2016 [46] | Retrospective | 188 | 62 | Biopsy | Carbon ion alone | Mean 67.2 Gy RBE (64–73.6)/4–4.6 Gy RBE fractions | 5 yr 77.2% | 5 yr 81.1% | 3% grade 3 neuropathies; 1% grade 4 skin toxicity |
| Imai, Br J Radiol, 2011 [47] | Retrospective | 84 | 42 | Definitive | Carbon ion | Median 70.4 Gy RBE (52.8–73.6)/3.3–4.6 Gy RBE fractions | 5 yr 86% | 5 yr 88% | 2% skin or soft tissue complications requiring skin graft; 16% severe sciatic nerve complications requiring medication |
| Demizu, Radiat Oncol, 2021 [48] | Retrospective | 219 | 56 | Definitive | Carbon ion | 67.2 Gy RBE, 70.4 Gy RBE, 79.2 Gy RBE/2.2–4.4 Gy RBE fractions | 5 yr 72% * | 5 yr 84% * | 1.4% grade 3 myositis; 1% insufficiency fracture; 1% skin disorders; 1% tissue necrosis; 2% grade 4 skin disorders |
| Evangelisti, Eur Rev Med Pharmacol Sci, 2019 [49] | Prospective | 18 | 23.3 | Biopsy | Carbon ion alone | 70.4 Gy RBE/4.4 Gy RBE fractions | 2 yr 84.6% | 2 yr 100% | 44% late neuropathy; 62.5% grade 1 parasthesia; 37.5% grade 2–3 pain; 5.5% grade 2 late gastrointestinal toxicity |
| Serizawa, J Compt Assist Tomogr, 2009 [50] | Retrospective | 34 | 46 | Biopsy, resection (unspecified extent) | Carbon ion alone or salvage | Range 52.8–73.6 Gy RBE, fraction dose not stated | 5 yr 93.8% | 5 yr 85.4% | NR |
| Imai, IJROBP, 2010 [51] | Phase 1–2 and 2 | 30 | 80 | Definitive | Carbon ion | Median 70.4 Gy RBE (52.8–73.6)/3.3–4.6 Gy RBE fractions | 5 yr 89% | 5 yr 86% | 5% skin or soft tissue complications requiring skin graft * |
| Bostel, Radiat Oncol, 2020 [52] | Retrospective | 68 | 60.3 | Biopsy, STR, GTR | Carbon ion alone, salvage | Median 80 Gy RBE (range, 68.8–96 Gy RBE) | 5 yr 53% | 5 yr 74% | Grade 3 or greater late effects in 21%; Sacral insufficiency fractures in 49% (36% symptomatic); peripheral neuropathy 9%; skin toxicity 9%; intestine 3% * |
| Preda, Radiother Oncol, 2018 [53] | Retrospective | 39 | 18 | Biopsy | Carbon ion alone | 70.4 Gy RBE/4.4 Gy RBE fractions | Cumulative 80% | NR | NR |
| Bostel, Radiother Oncol, 2018 [41] | Retrospective | 56 | 35.5 | Biopsy, STR, GTR | Carbon ion +/− photon alone or adjuvant | Median 66 Gy RBE (range, 60–74 Gy RBE)/3 Gy RBE fractions | NR | NR | 52% sacral insufficiency fracture |
| Schoenthaler, IJROBP, 1993 [42] | Retrospective | 14 | 60 | Biopsy, STR, GTR | Adjuvant helium and neon | Median dose 75.65 Gy RBE (range, 70–80.5 Gy RBE)/1.8–2.12 Gy RBE fractions | 5 yr 62% neon and 34% helium (55% overall) | 5 yr 85% | 7% colostomy for rectal injury; 7% second malignancy; 35% chronic wound |
| Breteau, Bull Cancer Radiother, 1996 [43] | Retrospective | 12 | NR | Biopsy, STR, GTR | Neutrons alone, salvage | three regimens based on tumor size and intent of therapy: (1) 40 Gy photons plus 15–25 neutron Gy (2) Curative 17.6 neutron Gy, 16 fractions (3) Palliative 10 neutron Gy, 12 fractions | 4 yr 54% | 4 yr 61% | 17% moist desquamation; 25% diarrhea |
| Author, Journal, Year Published | Study Type | Number of Patients | Median Follow-Up (mo) | Extent of Resection | Radiation Timing | Prescription Dose (Range)/Number of Fractions | Local Control | Overall Survival | Toxicity |
|---|---|---|---|---|---|---|---|---|---|
| Henderson, Neurosurgery, 2009 [54] | Retrospective | 11 (15 targets) | 46 | Biopsy, STR and/or GTR (margins NR) | RT alone, adjuvant | Median 35 Gy (24–40)/4–5 fractions | 5 yr 59.1% | 5 yr 74.3% | Hypersthesia with radiculopathy and transient paresthesias in one patient (received 37.5 Gy to cord); abdominal infections in two patients after neoadjuvant SBRT; no other complications attributable to SBRT in patients with spinal or sacral chordoma |
| Yamada, Neurosurgery, 2013 [55] | Retrospective | 24 | 24 | Biopsy, STR | RT alone, neoadjuvant, adjuvant | Median 24 Gy (18–24)/one fraction | Actuarial 95% | Crude 66% | 100% G1–G2 odynophagia in patients with cervical or mid thoracic tumors; 13% fracture of lumbar spine or sacrum; 4% sciatic neuropathy (tumor involved sciatic nerve); 4% vocal cord paralysis |
| Chang, Neurol Res, 2014 [56] | Retrospective | 11 | 50 | Biopsy, STR and/or GTR (margins NR) | RT alone, adjuvant | Median 35 Gy (30–50)/3–6 fractions (median 3) | Crude 45% | Mean 84 mo (95% CI: 71–97) | NR |
| Jung, Technol Cancer Res Treat, 2017 [57] | Retrospective | 8 (12 targets) | 10 | Biopsy, STR and/or GTR (margins NR) | RT alone, adjuvant | Median 16 Gy (11–16)/one fraction | Crude 75% | NR | 13% G2 spinal cord myelopathy (resolved with steroids) |
| Lockney, Neurosurg Focus, 2017 [58] | Retrospective | 12 | 26 | Cytoreductive separation surgery | Adjuvant | Median 24 Gy (24–36)/1–3 fractions (median 1) | Upfront (n = 5): crude 80% Salvage (n = 7): crude 57.1% | All: mean 77.6 mo Upfront: 76.6 mo Salvage: 68.6 mo | 27% RT-associated major complications (dysphagia, mucositis, vocal paralysis) |
| Lu, Rep Pract Oncol Radiother, 2019 [59] | Retrospective | 26 | 44 | STR, GTR | Adjuvant | Mean 22.6 Gy/two fractions | 5 yr 18.3% (95% CI: 3.0–33.6) | 5 yr 59.3% (95% CI: 34.1–84.5) | 8% acute G1 skin, GI, and urinary toxicity; 8% acute G2 skin and GI toxicity; no acute G3+ or late G1+ after SBRT |
| Jin, J Neurosurg Spine, 2020 [60] | Retrospective | 35 | 39 | Biopsy, STR, GTR, separation surgery | RT alone, neoadjuvant, adjuvant | Median 24 Gy (18–24)/one fraction | 5 yr 80.5% (95% CI: 64.4–96.5) | 5 yr 84.3% | 31% late G2+; 20% late G3 (tissue necrosis, recurrent laryngeal nerve palsy, myelopathy, fracture, secondary malignancy) |
| Chen, J Neurosurg Spine, 2021 [61] | Retrospective | 28 (30 targets) | 21 | Biopsy, STR, GTR | RT alone, neoadjuvant, adjuvant | Median 40 Gy (15–50)/1–5 fractions (median 5) | 2 yr 96% (95% CI: 74–99) | 2 yr 92% (95% CI: 71–98) | 12% G3 wound complications in neoadjuvant SBRT arm; 4% G2 PE; 4% G2 stroke; 4% G3 large bowel obstruction; 4% G3 empyema (away from RT field) |
| Author, Journal, Year Published | Study Type | Number of Patients | Median Follow-Up (mo) | Treatment Intent | Radiation Modality | Prescription Dose (Range)/Dose per Fraction | Local Control | Overall Survival | Toxicity |
|---|---|---|---|---|---|---|---|---|---|
| Chen, Spine, 2013 [8] | Retrospective | 24 | 56 | Definitive | Photon, proton | Median 77.4 Gy RBE (70.2–79)/1.8–2.5 Gy RBE fractions | 5 yr 79.8% | 5 yr 78.1% | 33% sacral insufficiency fractions (none requiring surgery); 4% secondary malignancy; 4% erectile dysfunction; 4% perineal numbness; 8% worsening fecal/urinary incontinence; 17% grade 2 rectal bleeding (none requiring new colostomy) |
| Imai, Br J Radiol, 2011 [47] | Retrospective | 84 | 42 | Definitive | Carbon ion | Median 70.4 Gy RBE (52.8–73.6)/3.3–4.6 Gy RBE fractions | 5 yr 86% | 5 yr 88% | 2% skin or soft tissue complications requiring skin graft; 16% severe sciatic nerve complications requiring medication |
| Imai, IJROBP, 2010 [51] | Phase 1–2 and 2 | 30 | 80 | Definitive | Carbon ion | Median 70.4 Gy RBE (52.8–73.6)/3.3–4.6 Gy RBE fractions | 5 yr 89% | 5 yr 86% | 5% skin or soft tissue complications requiring skin graft |
| Yamada, Neurosurgery, 2013 [55] | Retrospective | 10 | 28.5 | Definitive, recurrent, metastatic | SBRT | Median 24 Gy (18–24)/18–24 Gy fractions | 2 yr 100% | NR | 100% G1–G2 odynophagia in patients with cervical or mid thoracic tumors; 13% fracture of lumbar spine or sacrum; 4% sciatic neuropathy (tumor involved sciatic nerve); 4% vocal cord paralysis |
| Bostel, Radiat Oncol, 2020 [52] | Retrospective | 28 | 60.3 | Definitive, recurrent | Carbon ion +/− IMRT | Median 80 Gy RBE (range, 68.8–96 Gy RBE) | 5 yr 62% | 5 yr 74% | Grade 3 or greater late effects in 21%; Sacral insufficiency fractures in 49% (36% symptomatic); peripheral neuropathy 9%; skin toxicity 9%; intestine 3% |
| Mima, Br J Radiol, 2014 [28] | Retrospective | 23 | 38 | Definitive | Carbon ion or proton | Median 70.4 Gy RBE/2.2 or 4.4 Gy RBE fractions | 3 yr 94% | 3 yr 83% | Grade 4 dermatitis 22%; grade 3 neuropathy in 17%; grade 3 myositis 9% |
| Aibe, IJROBP, 2018 [21] | Retrospective | 33 | 37 | Definitive | Proton | 70.4 Gy RBE/2.2 Gy RBE fractions | 3 yr PFS 89.6% | 3 yr 92.7% | 3% grade 3 acute dermatitis; 3% ileus; 6% pain due to sacral insufficiency fractures |
| Walser, Clinical Onoclogy 2021 [18] | Retrospective | 10 | 48 | Definitive | Proton | Median 74 Gy RBE (range 60–77)/4–4.6 Gy REB fractions | 4 yr 77% * | 4 yr 85% | 7% acute grade 3 dermatitis; 3.5% sacral insufficiency; 1.5% neuropathic pain interfering with ADLs; 3% secondary malignancies |
| Imai, IJROBP 2016 [46] | Retrospective | 188 | 62 | Definitive | Carbon ion | 64–73.6 Gy RBE/4–4.6 Gy RBE fractions | 5 yr 77.2% | 5 yr 81.1% | 3% grade 3 toxicity of peripheral nerves; 1% grade 4 skin toxicity |
| Demizu, Radiat Oncol, 2021 [48] | Retrospective | 219 | 56 | Definitive | Carbon ion | 67.2 Gy RBE, 70.4 Gy RBE, 79.2 Gy RBE/2.2–4.4 Gy RBE fractions | 5 yr 72% | 5 yr 84% | 1.4% grade 3 myositis; 1% insufficiency fracture; 1% skin disorders; 1% tissue necrosis; 2% grade 4 skin disorders |
| Evangelisti, Eur Rev Med Pharmacol Sci, 2019 [49] | Prospective | 18 | 23.3 | Biopsy | RT alone | 70.4 Gy RBE/4.4 Gy RBE fractions | 2 yr 84.6% | 2 yr 100% | 44% late neuropathy; 62.5% grade 1 parasthesia; 37.5% grade 2–3 pain; 5.5% grade 2 late gastrointestinal toxicity |
| Author, Journal, Year Published | Study Type | Anatomic Location | Number of Patients | Modality | Prescription Dose (Range)/Dose per Fraction | Local Control | Overall Survival |
|---|---|---|---|---|---|---|---|
| Rotondo, J Neurosurg Spine, 2015 [19] | Retrospective | Mobile spine and sacrum | Preop + Postop: 44 Postop: 51 | Proton and photon | Preop 19.8–50.4 GyRBE plus postop to bring dose to 70.2 Gy RBE/1.8–2 Gy RBE fractions | Preop + postop: 5 yr 85% | Pre-op + postop: 5 yr 85% |
| Postop: 77.4 GyRBE (range 70.2–77.4 GyRBE)/1.8–2 Gy RBE fractions | Post-op: 5 yr 56% | Post-op: 5 yr 80% | |||||
| Houdek, J Surg Oncol, 2019 [11] | Retrospective | Sacrum | Preop: 30 Postop: 17 Preop + Postop: 42 | Proton and photon | Preop: 50 Gy/1.8–2 Gy RBE fractions Postop: 60.2 +/− 9.9 Gy/1.8–2 Gy RBE fractions Preop + Postop: 70.9 +/− 5.7 Gy RBE/1.8–2 Gy RBE fractions | Not individually reported | Not individually reported |
| Chen, J Neurosurg Spine, 2021 [61] | Retrospective | Mobile spine and sacrum | Preop: 17 Postop: 5 | SBRT | Preop: 40–50 Gy in 5 fractions, 18–21 Gy in 3 fractions, or 16 Gy in 1 fraction | Pre-op 100% | Not individually reported |
| Postop: 40 Gy (range 30–50 Gy) in 5 fractions | Postop 80% | ||||||
| Jin, J Neurosurg Spine, 2019 [60] | Retrospective | Mobile spine and sacrum | Preop: 12 Postop: 11 | SBRT | 24 Gy (range 18–24 Gy/18–24 Gy fractions | Preop: 3-year LRFS 90% for sacral lesions Individual information not available for postop group | Not individually reported |
| Title and identifier | Sponsor | Phase | Recruitment Status | Estimated Enrollment | Estimated Completion Date | Primary Endpoint | Arms |
|---|---|---|---|---|---|---|---|
| Nilotinib With Radiation for High Risk Chordoma, NCT01407198 | Massachusetts General Hospital | I | Active, not recruiting | 29 | December 2025 | DLTs when treated above the maximum tolerated dose | Nilotinib + EBRT 50.4 Gy |
| BN Brachyury and Radiation in Chordoma, NCT03595228 | Bavarian Nordic | II | Active, not recruiting | 29 | January 2022 | Clinically meaningful objective response rate | BN-Brachyury + radiation |
| Sacral Chordoma: Surgery Versus Definitive Radiation Therapy in Primary Localized Disease (SACRO), NCT02986516 | Italian Sarcoma Group | NA | Recruiting | 100 | September 2022 | Relapse-free survival | Patients who agree to be randomized will receive surgery vs. definitive RT (carbon ion radiotherapy, proton therapy, mixed photons–proton therapy). Those who do not agree to randomization will choose their modality. |
| Nivolumab With or Without Stereotactic Radiosurgery in Treating Patients With Recurrent, Advanced, or Metastatic Chordoma, NCT02989636 | Johns Hopkins University | I | Recruiting | 33 | March 2022 | Incidence of dose limiting toxicities | Arm I: Nivolumab; Arm II: Nivolumab + SRS |
| Ion Irradiation of Sacrococcygeal Chordoma (ISAC), NCT01811394 | Heidelberg University | II | Recruiting | 100 | June 2022 | Safety and feasibility based on incidence of G3 = 5 toxicity | Arm I: 16 × 4 GyE protons; Arm II: 16 × 4 GyE carbon ions |
| QUILT-3.011 Phase 2 Yeast-Brachyury Vaccine Chordoma, NCT02383498 | NantCell, Inc. | II | Active, not recruiting | 55 | March 2020 | Proportion of patients whose tumors shrunk after therapy | Arm I: Radiation (SOC) + GI-6301 Vaccine + Actigraph; Arm II: Radiation + GI-6301 Placebo + Actigraph |
| Proton Beam Therapy for Chordoma Patients, NCT00496119 | MD Anderson Cancer Center | II | Active, not recruiting | 15 | December 2024 | Time to local recurrence | Arm I: 70 GyE PBT at 2 Gy/fx; Arm II: 70 GyE at 2 Gy/fx but using proton beam therapy combined with photon RT where combination improves final dose distribution. Both arms are treated with RT 2+ weeks after surgery. |
| Improvement of Local Control in Skull Base, Spine and Sacral Chordomas Treated by Surgery and Protontherapy Targeting Hypoxic Cells Revealed by [18F]FAZA) PET/CT Tracers (PROTONCHORDE01), NCT02802969 | Institut Curie | II | Recruiting | 64 | February 2024 | Improvement of local control according to RECIST criteria | In residual chordoma after surgery, 78 GyE proton beam therapy (70 GyE to tumor bed and macroscopic volume guided by conventional imaging (CT/MRI) and 8 GyE boost to hypoxic component guided by FAZA (PET/CT) |
| Hypoxia-positron Emission Tomography (PET) and Intensity Modulated Proton Therapy (IMPT) Dose Painting in Patients With Chordomas, NCT00713037 | Massachusetts General Hospital | NA | Completed | 20 | June 2016 | Evaluate if FMISO-PET is a feasible approach for the visualization of hypoxia in skull-base and spinal chordoma | Proton beam therapy + (18F)-FMISO/CT 2 weeks before PBT and 3 weeks after first PBT fraction after 24–36 GyE |
| Proton Therapy for Chordomas and/or Chondrosarcomas (CH01), NCT00797602 | University of Florida | Observational | Completed | 189 | December 2015 | Tumor control | Proton beam therapy |
| Proton Radiation for Chordomas and Chondrosarcomas, NCT01449149 | University of Pennsylvania | NA | Active, not recruiting | 50 | December 2026 | Feasibility | Proton beam therapy 72 to 79.2 Gy RBE in 40–44 fractions |
| Charged Particle RT for Chordomas and Chondrosarcomas of the Base of Skull or Cervical Spine, NCT00592748 | Massachusetts General Hospital | I/II | Completed | 381 | May 2015 | Acute toxicity | Arm I: 40–44 treatments of charged particles; Arm II: 37–40 treatments of charged particles (most will be given with protons but may receive a small portion of photons to spare skin) |
| Image Assisted Optimization of Proton Radiation Therapy in Chordomas and Chondrosarcomas (CHIPT), NCT04832620 | Leiden University Medical Center | Observational | Recruiting | 40 | November 2023 | Determine if functional MRI parameters change within 6 months, and earlier than volumetric changes after start of proton beam therapy, determined by Volumetric and functional MR imaging parameters including permeability parameters | Proton beam therapy + volumetric and functional MR |
| Randomized Carbon Ions vs. Standard Radiotherapy for Radioresistant Tumors (ETOILE), NCT02838602 | Hospices Civils de Lyon | NA | Recruiting | 250 | December 2026 | Progression free survival | Arm I: Carbon; Arm II: photons or proton beam therapy |
| High Dose Intensity Modulated Proton Radiation Treatment +/− Surgical Resection of Sarcomas of the Spine, Sacrum and Base of Skull, NCT01346124 | Massachusetts General Hospital | NA | Active, not recruiting | 64 | March 2032 | Local control | Intensity modulated proton therapy |
| Comparing Carbon Ion Therapy, Surgery, and Proton Therapy for the Management of Pelvic Sarcomas Involving the Bone, the PROSPER Study, NCT05033288 | Mayo Clinic | Observational | Not yet recruiting | 180 | August 2028 | Patient-reported outcome—health-related quality of life; local control | Carbon, protons, surgery (non-randomized) |
| Spine Tumor Academy Recommendations | |
|---|---|
| Recommendation | Level of Strength of Evidence Recommendation |
| The best chance of cure for mobile spine and sacral chordoma is in the upfront setting. As such, multi-disciplinary expert involvement at time of initial diagnosis is essential to optimizing patient outcomes | III Consensus |
| Target delineation should be performed on CT scans with at minimum a co-registered T2 weighted MRI. For patients treated in the adjuvant setting the pre-operative T2 weighted MRI should similarly be co-registered. In the adjuvant setting, a comprehensive discussion between the spine surgeon and radiation oncologist should occur to review intraoperative surgical findings and highlight regions believed to be at high risk of recurrence, which may not be obvious based on imaging alone. In the neoadjuvant setting, the discussion should include a review of the surgical plans and intentions to sacrifice or preserve specific nerves in the operating room so that the dosimetric parameters may be adjusted accordingly. | III Consensus |
| Comprehensive target volumes that include regions of potential microscopic spread have superior local control to focal targets. For SBRT, target delineation according to the consensus contouring guidelines for solid tumor spinal metastases should be considered [63,64]. For proton and heavy ion therapy, comprehensive target delineation is based upon the Massachusetts General Hospital (MGH) Phase 2 data consisting of creation of a low-risk “microscopic” clinical target volume (CTV1) treated to a dose of 19.8–50.4 GyRBE (preoperatively) or 50.4 GyRBE). This is followed by a sequential boost to the high risk CTV2 to 70.2 GyRBE as defined by the original GTV (anatomically constrained) plus 5 mm. A further boost to gross residual disease without margin is performed after maximum safe resection and/or to the definitive GTV to 73.8–77.4 GyRBE [4,19]. PTV is institution specific based upon robustness and range uncertainty analysis. | III Consensus |
Although high-level data comparing outcomes comparing dose/fractionation regimens and treatment modalities are unavailable, dose escalation is critical in optimizing local control. Reasonable dose/fractionation schedules by treatment modality include the following:
| III Consensus |
| When utilizing proton and heavy ion therapy, efforts must be made to limit the dose to the skin to less than 66 GyRBE in order to minimize the risk of long-term wound healing complications [3]. | II Consensus |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Redmond, K.J.; Schaub, S.K.; Lo, S.-f.L.; Khan, M.; Lubelski, D.; Bilsky, M.; Yamada, Y.; Fehlings, M.; Gogineni, E.; Vajkoczy, P.; et al. Radiotherapy for Mobile Spine and Sacral Chordoma: A Critical Review and Practical Guide from the Spine Tumor Academy. Cancers 2023, 15, 2359. https://doi.org/10.3390/cancers15082359
Redmond KJ, Schaub SK, Lo S-fL, Khan M, Lubelski D, Bilsky M, Yamada Y, Fehlings M, Gogineni E, Vajkoczy P, et al. Radiotherapy for Mobile Spine and Sacral Chordoma: A Critical Review and Practical Guide from the Spine Tumor Academy. Cancers. 2023; 15(8):2359. https://doi.org/10.3390/cancers15082359
Chicago/Turabian StyleRedmond, Kristin J., Stephanie K. Schaub, Sheng-fu Larry Lo, Majid Khan, Daniel Lubelski, Mark Bilsky, Yoshiya Yamada, Michael Fehlings, Emile Gogineni, Peter Vajkoczy, and et al. 2023. "Radiotherapy for Mobile Spine and Sacral Chordoma: A Critical Review and Practical Guide from the Spine Tumor Academy" Cancers 15, no. 8: 2359. https://doi.org/10.3390/cancers15082359
APA StyleRedmond, K. J., Schaub, S. K., Lo, S.-f. L., Khan, M., Lubelski, D., Bilsky, M., Yamada, Y., Fehlings, M., Gogineni, E., Vajkoczy, P., Ringel, F., Meyer, B., Amin, A. G., Combs, S. E., & Lo, S. S. (2023). Radiotherapy for Mobile Spine and Sacral Chordoma: A Critical Review and Practical Guide from the Spine Tumor Academy. Cancers, 15(8), 2359. https://doi.org/10.3390/cancers15082359