

MR-Class: A Python Tool for Brain MR Image Classification Utilizing One-vs-All DCNNs to Deal with the Open-Set Recognition Problem

 , , , , and
, , , , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Datasets
2.2. MR Scans
2.3. DCNNs Comparison Study
2.3.1. Data Preprocessing
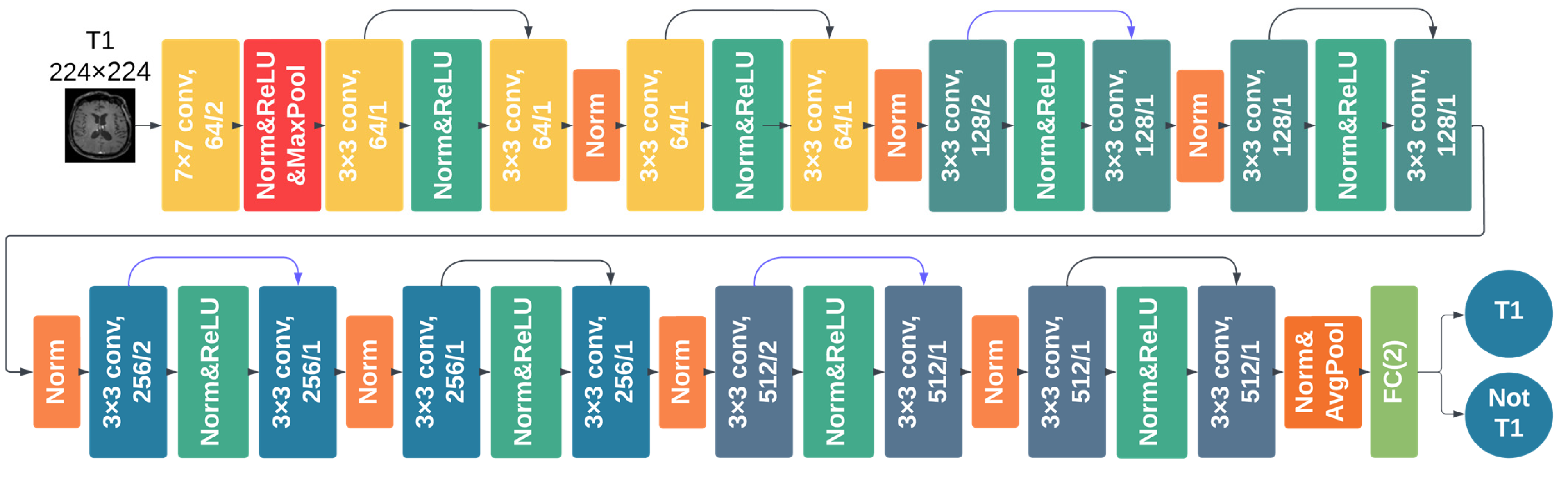
2.3.2. DCNN Training and Testing
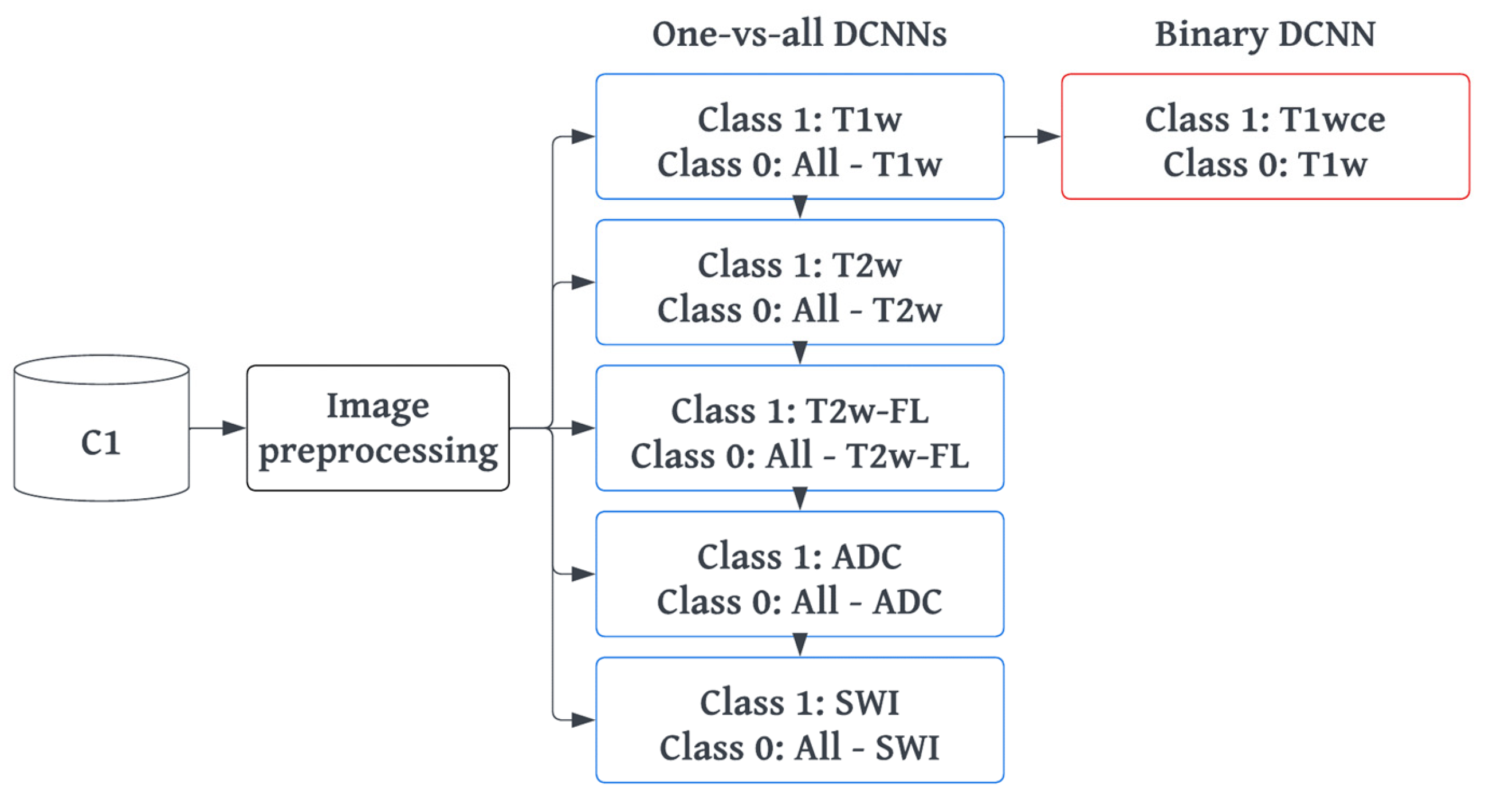
2.4. MR-Class: One-vs-All DCNNs
2.4.1. Training and Preprocessing
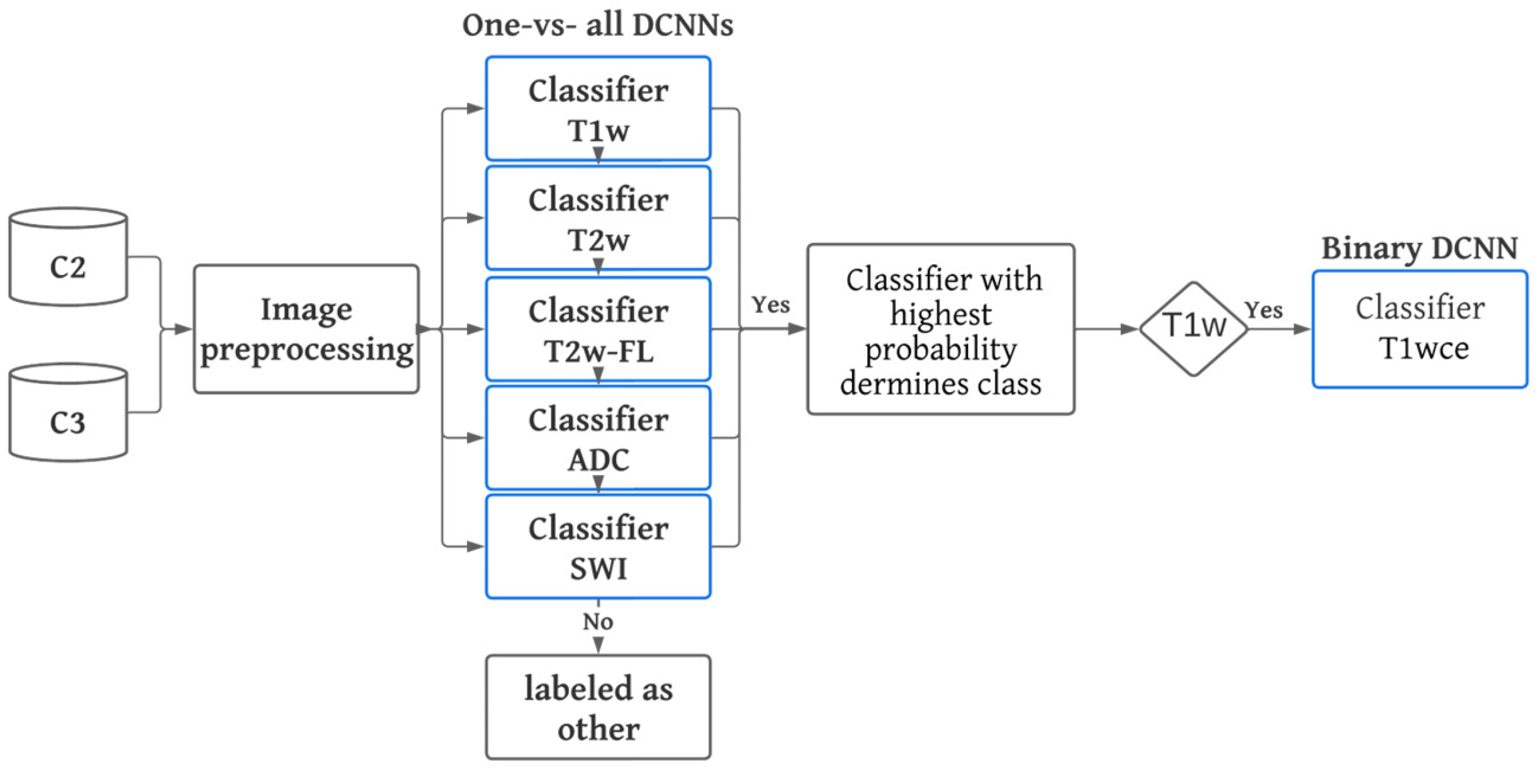
2.4.2. Inference and Testing
2.5. MR-Class Application: Progression-Free Survival Prediction Modeling
3. Results
3.1. Metadata Consistency
3.2. DCNN Comparison Study
3.3. MR-Class: One-vs-All DCNNs
3.4. Analyses of Misclassified Images
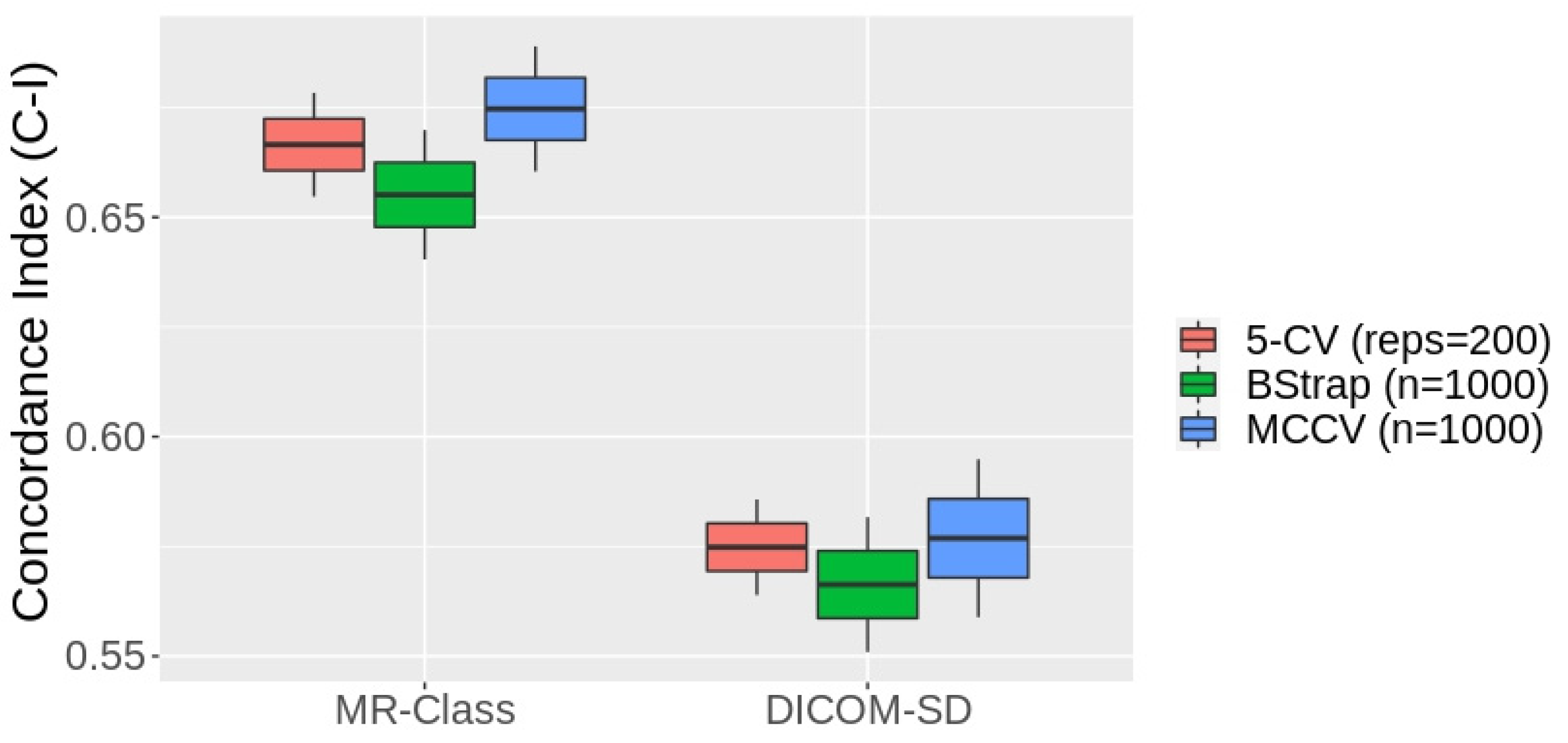
3.5. MR-Class Application: Progression-Free Survival Prediction Modeling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Westbrook, C.; Talbot, J. MRI in Practice; John Wiley & Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- Kickingereder, P.; Isensee, F.; Tursunova, I.; Petersen, J.; Neuberger, U.; Bonekamp, D.; Brugnara, G.; Schell, M.; Kessler, T.; Foltyn, M.; et al. Automated quantitative tumour response assessment of MRI in neuro-oncology with artificial neural networks: A multicentre, retrospective study. Lancet Oncol. 2019, 20, 728–740. [Google Scholar] [CrossRef] [PubMed]
- Gueld, M.O.; Kohnen, M.; Keysers, D.; Schubert, H.; Wein, B.B.; Bredno, J.; Lehmann, T.M. Quality of DICOM header information for image categorization. In Proceedings of the Medical Imaging 2002: PACS and Integrated Medical Information Systems: Design and Evaluation, San Diego, CA, USA, 16 May 2002; pp. 280–287. [Google Scholar]
- Harvey, H.; Glocker, B. A standardized approach for preparing imaging data for machine learning tasks in radiology. In Artificial Intelligence in Medical Imaging; Springer: Berlin, Germany, 2019; pp. 61–72. [Google Scholar]
- Névéol, A.; Deserno, T.M.; Darmoni, S.J.; Güld, M.O.; Aronson, A.R. Natural language processing versus content-based image analysis for medical document retrieval. J. Am. Soc. Inf. Sci. Technol. 2009, 60, 123–134. [Google Scholar] [CrossRef]
- Wagle, S.; Mangai, J.A.; Kumar, V.S. An improved medical image classification model using data mining techniques. In Proceedings of the 2013 7th IEEE GCC Conference and Exhibition (GCC), Doha, Qatar, 17–20 November 2013; pp. 114–118. [Google Scholar]
- Varol, E.; Gaonkar, B.; Erus, G.; Schultz, R.; Davatzikos, C. Feature ranking based nested support vector machine ensemble for medical image classification. In Proceedings of the 2012 9th IEEE International Symposium on Biomedical Imaging (ISBI), Barcelona, Spain, 2–5 May 2012; pp. 146–149. [Google Scholar]
- Shen, D.; Wu, G.; Suk, H.-I. Deep Learning in Medical Image Analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [PubMed]
- Alom, M.Z.; Taha, T.M.; Yakopcic, C.; Westberg, S.; Sidike, P.; Nasrin, M.S.; Van Esesn, B.C.; Awwal, A.A.; Asari, V.K. The history began from alexnet: A comprehensive survey on deep learning approaches. arXiv 2018, arXiv:180301164. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Li, F.-F. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Liang, M.; Tang, W.; Xu, D.M.; Jirapatnakul, A.C.; Reeves, A.P.; Henschke, C.I.; Yankelevitz, D. Low-Dose CT Screening for Lung Cancer: Computer-aided Detection of Missed Lung Cancers. Radiology 2016, 281, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Setio, A.A.; Ciompi, F.; Litjens, G.; Gerke, P.; Jacobs, C.; van Riel, S.J.; Wille, M.M.; Naqibullah, M.; Sanchez, C.I.; van Ginneken, B. Pulmonary Nodule Detection in CT Images: False Positive Reduction Using Multi-View Convolutional Networks. IEEE Trans. Med. Imaging 2016, 35, 1160–1169. [Google Scholar] [CrossRef]
- Kang, G.; Liu, K.; Hou, B.; Zhang, N. 3D multi-view convolutional neural networks for lung nodule classification. PLoS ONE 2017, 12, e0188290. [Google Scholar] [CrossRef]
- Qayyum, A.; Anwar, S.M.; Awais, M.; Majid, M. Medical image retrieval using deep convolutional neural network. Neurocomputing 2017, 266, 8–20. [Google Scholar] [CrossRef]
- Ayyachamy, S.; Alex, V.; Khened, M.; Krishnamurthi, G. Medical image retrieval using Resnet-18. In Proceedings of the SPIE Medical Imaging, San Diego, CA, USA, 16–21 February 2019; Volume 1095410, pp. 233–241. [Google Scholar]
- Remedios, S.; Roy, S.; Pham, D.L.; Butman, J.A. Classifying magnetic resonance image modalities with convolutional neural networks. In Proceedings of the SPIE Medical Imaging, Houston, TX, USA, 10–15 February 2018; Volume 10575, pp. 558–563. [Google Scholar] [CrossRef]
- van der Voort, S.R.; Smits, M.; Klein, S. DeepDicomSort: An Automatic Sorting Algorithm for Brain Magnetic Resonance Imaging Data. Neuroinformatics 2021, 19, 159–184. [Google Scholar] [CrossRef]
- Scheirer, W.J.; de Rezende Rocha, A.; Sapkota, A.; Boult, T.E. Toward open set recognition. IEEE Trans. Pattern Anal. Mach. Intell. 2012, 35, 1757–1772. [Google Scholar] [CrossRef]
- Scarpace, L.; Mikkelsen, L.; Cha, T.; Rao, S.; Tekchandani, S.; Gutman, S.; Pierce, D. Radiology Data from the Cancer Genome Atlas Glioblastoma Multiforme [TCGA-GBM] Collection. The Cancer Imaging Archive. 2016. Available online: https://www.cancerimagingarchive.net (accessed on 2 December 2019).
- Ellingson, B.M.; Bendszus, M.; Boxerman, J.; Barboriak, D.; Erickson, B.J.; Smits, M.; Nelson, S.J.; Gerstner, E.; Alexander, B.; Goldmacher, G.; et al. Consensus recommendations for a standardized Brain Tumor Imaging Protocol in clinical trials. Neuro. Oncol. 2015, 17, 1188–1198. [Google Scholar]
- Combs, S.E.; Kieser, M.; Rieken, S.; Habermehl, D.; Jäkel, O.; Haberer, T.; Nikoghosyan, A.; Haselmann, R.; Unterberg, A.; Wick, W.; et al. Randomized phase II study evaluating a carbon ion boost applied after combined radiochemotherapy with te-mozolomide versus a proton boost after radiochemotherapy with temozolomide in patients with primary glioblastoma: The CLEOPATRA Trial. BMC Cancer 2010, 10, 478. [Google Scholar] [CrossRef]
- Combs, S.E.; Burkholder, I.; Edler, L.; Rieken, S.; Habermehl, D.; Jäkel, O.; Haberer, T.; Haselmann, R.; Unterberg, A.; Wick, W.; et al. Randomized phase I/II study to evaluate carbon ion radiotherapy versus fractionated stereotactic radiotherapy in patients with recurrent or progressive gliomas: The CINDERELLA trial. BMC Cancer 2010, 10, 533. [Google Scholar] [CrossRef]
- Niyazi, M.; Adeberg, S.; Kaul, D.; Boulesteix, A.-L.; Bougatf, N.; Fleischmann, D.F.; Grün, A.; Krämer, A.; Rödel, C.; Eckert, F.; et al. Independent validation of a new reirradiation risk score (RRRS) for glioma patients predicting post-recurrence survival: A multicenter DKTK/ROG analysis. Radiother. Oncol. 2018, 127, 121–127. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:14091556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 Bias Correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L.; et al. PyTorch: An imperative style, high-performance deep learning library. Adv. Neural Inf. Process. Syst. 2019, 32, 8026–8037. [Google Scholar]
- Pérez-García, F.; Sparks, R.; Ourselin, S. TorchIO: A Python library for efficient loading, preprocessing, augmentation and patch-based sampling of medical images in deep learning. Comput. Methods Programs Biomed. 2021, 208, 106236. [Google Scholar] [CrossRef]
- Wallis, S. Binomial Confidence Intervals and Contingency Tests: Mathematical Fundamentals and the Evaluation of Alter-native Methods. J. Quant. Linguist. 2013, 20, 178–208. [Google Scholar] [CrossRef]
- Lin, D.Y.; Wei, L.J. The robust inference for the Cox proportional hazards model. J. Am. Stat. Assoc. 1989, 84, 1074–1078. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Sanders, H.; Saxe, J. Garbage in, Garbage out: How Purportedly Great ML Models can be Screwed up by Bad Data. In Proceedings of the Black Hat, Las Vegas, NV, USA, 22–27 July 2017; Available online: https://www.blackhat.com/us-17/call-for-papers.html#review (accessed on 14 March 2023).
- Sforazzini, F.; Salome, P.; Kudak, A.; Ulrich, M.; Bougatf, N.; Debus, J.; Knoll, M.; Abdollahi, A. pyCuRT: An Automated Data Cura-tion Workflow for Radiotherapy Big Data Analysis using Pythons’ NyPipe. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, e772. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training | Validation | |||
|---|---|---|---|---|
| DCNN Classifier | Targeted Class | Remaining Images | Targeted Class | Remaining Images |
| T1w-vs-all | 3152 (15.7) | 12,929 (64.3) | 788 (3.9) | 3232 (16.1) |
| T2w-vs-all | 1576 (7.9) | 14,505 (72.1) | 394 (2.0) | 3626 (18.0) |
| T2w-FL-vs-all | 1535 (7.6) | 14,546 (72.4) | 384 (1.9) | 3636 (18.1) |
| ADC-vs-all | 1550 (7.7) | 14,530 (72.3) | 388 (1.9) | 3633 (18.1) |
| SWI-vs-all | 1183 (5.9) | 14,898 (74.1) | 296 (1.5) | 3724 (18.5) |
| C1 | C2 | C3 | ||||
|---|---|---|---|---|---|---|
| n | % Error | n | % Error | n | % Error | |
| T1w | 2023 | 15.1 | 1189 | 11.2 | 433 | 13.4 |
| T1wce | 1917 | 13.9 | 4315 | 13.4 | 1096 | 9.9 |
| T2w | 1970 | 9.3 | 630 | 11.7 | 347 | 10.3 |
| T2w-FL | 1919 | 7.2 | 811 | 10.5 | 389 | 8.2 |
| ADC | 1938 | 7.6 | 895 | 8.4 | 122 | 5.5 |
| SWI | 1479 | 6.3 | 486 | 6.6 | - | - |
| Other | 8855 | 13.1 | 3007 | 7.3 | 1135 | 12.1 |
| All | 20,101 | 11.4 | 11,333 | 10.6 | 3522 | 10.7 |
| 2D-ResNet | DeepDicomSort | Φ-Net | 3D-ResNet | |
|---|---|---|---|---|
| T1w | 98.4 | 98.8 | 97.7 | 96.5 |
| T1wce | 97.4 | 95.2 | 97.5 | 96.2 |
| T2w | 98.1 | 97.2 | 96.6 | 97.1 |
| T2w-FL | 99.7 | 99.4 | 96.5 | 98.7 |
| ADC | 99.9 | 99.3 | 98.5 | 99.2 |
| SWI | 98.2 | 98.5 | 97.5 | 98.9 |
| All | 98.6 | 98.1 | 97.4 | 97.8 |
| Classifier | Val Acc (%) | Classifier | Val Acc (%) |
|---|---|---|---|
| T1w-vs-all | 99.1 | T2wFL-vs-all | 99.4 |
| T1w-vs-T1wce | 97.7 | ADC-vs-all | 99.6 |
| T2w-vs-all | 99.3 | SWI-vs-all | 99.7 |
| Category | n | % |
|---|---|---|
| MR artifact-other | 146 | 26.84 |
| MR artifact-middle slice blurring | 127 | 23.35 |
| Tumor/GTV displacing ventricles | 122 | 22.43 |
| Similar content-different sequence | 80 | 14.71 |
| DWI as T2w | 76 | 13.97 |
| DICOM corrupted images | 69 | 12.68 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salome, P.; Sforazzini, F.; Brugnara, G.; Kudak, A.; Dostal, M.; Herold-Mende, C.; Heiland, S.; Debus, J.; Abdollahi, A.; Knoll, M. MR-Class: A Python Tool for Brain MR Image Classification Utilizing One-vs-All DCNNs to Deal with the Open-Set Recognition Problem. Cancers 2023, 15, 1820. https://doi.org/10.3390/cancers15061820
Salome P, Sforazzini F, Brugnara G, Kudak A, Dostal M, Herold-Mende C, Heiland S, Debus J, Abdollahi A, Knoll M. MR-Class: A Python Tool for Brain MR Image Classification Utilizing One-vs-All DCNNs to Deal with the Open-Set Recognition Problem. Cancers. 2023; 15(6):1820. https://doi.org/10.3390/cancers15061820
Chicago/Turabian StyleSalome, Patrick, Francesco Sforazzini, Gianluca Brugnara, Andreas Kudak, Matthias Dostal, Christel Herold-Mende, Sabine Heiland, Jürgen Debus, Amir Abdollahi, and Maximilian Knoll. 2023. "MR-Class: A Python Tool for Brain MR Image Classification Utilizing One-vs-All DCNNs to Deal with the Open-Set Recognition Problem" Cancers 15, no. 6: 1820. https://doi.org/10.3390/cancers15061820
APA StyleSalome, P., Sforazzini, F., Brugnara, G., Kudak, A., Dostal, M., Herold-Mende, C., Heiland, S., Debus, J., Abdollahi, A., & Knoll, M. (2023). MR-Class: A Python Tool for Brain MR Image Classification Utilizing One-vs-All DCNNs to Deal with the Open-Set Recognition Problem. Cancers, 15(6), 1820. https://doi.org/10.3390/cancers15061820