
Correlation between Imaging Markers Derived from PET/MRI and Invasive Acquired Biomarkers in Newly Diagnosed Breast Cancer
 , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PET/MRI
- (i)
- A transversal T2-weighted (T2w) turbo-spin echo (TSE) fat-saturated sequence with a slice thickness of 7 mm (TE 97 ms; TR 2840 ms; FOV 400 mm; phase FOV 75%; acquisition matrix 256 × 192, in-plane resolution 1.6 × 1.6 mm2)
- (ii)
- A transversal diffusion-weighted echo-planar imaging (EPI) sequence with a slice thickness of 5.0 mm (TR 8000 ms; TE 81 ms; b-values: 0, 400 and 800 s/mm2, matrix size 192 × 156; FOV 420 mm, phase FOV, 81.3%; GRAPPA, acceleration factor 2; in-plane resolution 2.2 × 2.2 mm2)
- (iii)
- Six repetitions of a transversal 3-dimensional fast low-angle shot (FLASH) T1w sequence with a slice thickness of 7 mm (TE 3.62 ms; TR 185 ms; FOV 400 mm; phase FOV 75%; acquisition matrix 320 × 240, in-plane resolution 1.3 × 1.3 mm2) for dynamic contrast-enhanced imaging. A dose of 0.2 mmol/kg bodyweight gadoterate meglumine (Dotarem, Guerbet, Sulzbach, Germany) was injected intravenously after the first FLASH sequence with a flow of 2 mL/s using an automated injector (Spectris Solaris, MR Injection System; Medrad, Pittsburg, PA, USA). Subsequent automated image subtraction was performed.
- (i)
- A transverse T2-w half Fourier acquisition single-shot turbo spin echo (HASTE) sequence in breath-hold technique with a slice thickness of 7 mm (TE 97 ms; TR 1500 ms; turbo factor (TF) 194; FOV 400 mm; phase FOV 75%; acquisition matrix 320 × 240 mm; in-plane resolution 1.3 × 1.3 mm2; TA 0:47 min/bed position)
- (ii)
- A transversal diffusion-weighted (DWI) echo-planar imaging (EPI) sequence in free breathing with a slice thickness of 5.0 mm (TR 7400 ms; TE 72 ms; b-values: 0, 500 and 1000 s/mm2, matrix size 160 × 90; FOV 400, phase FOV, 75%; GRAPPA, acceleration factor 2; in-plane resolution 2.6 × 2.6 mm2; TA 2:06 min/bed position)
- (iii)
- A fat-saturated post-contrast transverse 3-dimensional volumetric interpolated breath-hold examination (VIBE) sequence with a slice thickness of 3 mm (TE, 1.53 ms; TR, 3.64 ms; flip angle 9°; FOV 400; phase FOV 75%; acquisition matrix 512 × 384, in-plane resolution 0.7 × 0.7 mm2; TA 0:19 min/bed position)
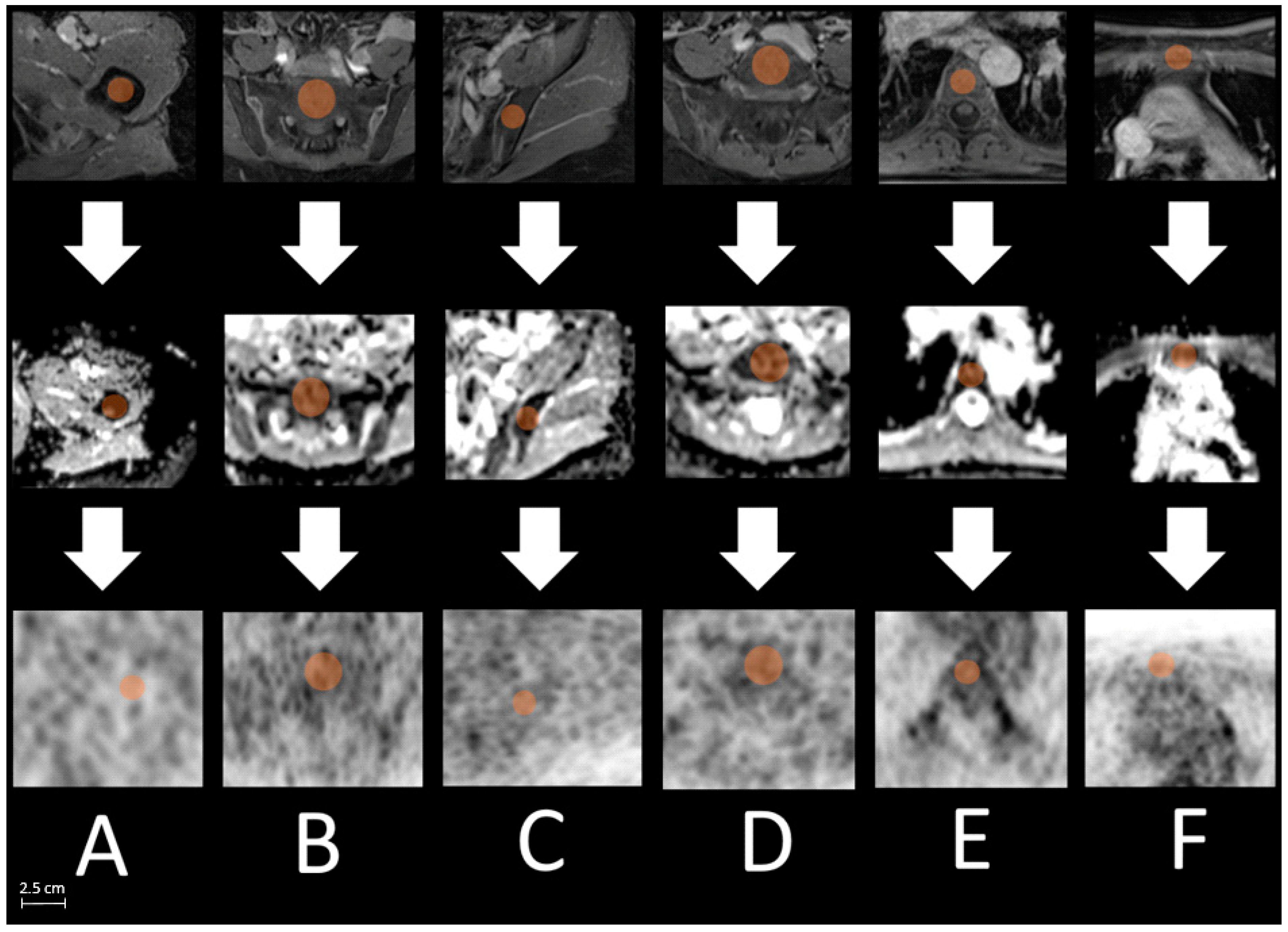
2.3. Image Analysis
2.4. Histopathological Examination
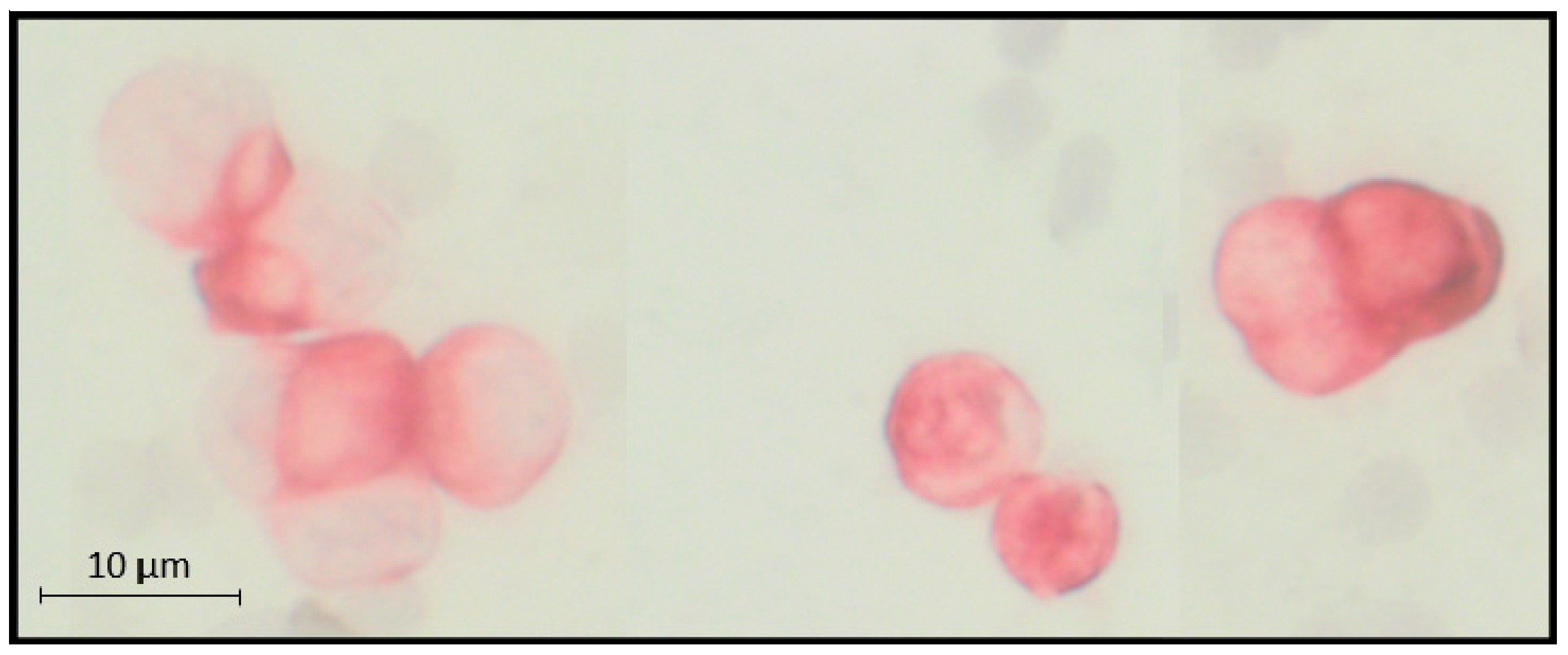
2.5. Selection and Detection of Disseminated Tumor Cells (DTCs)
2.6. Statistical Analysis
3. Results
3.1. Patient Population and Histopathological Findings
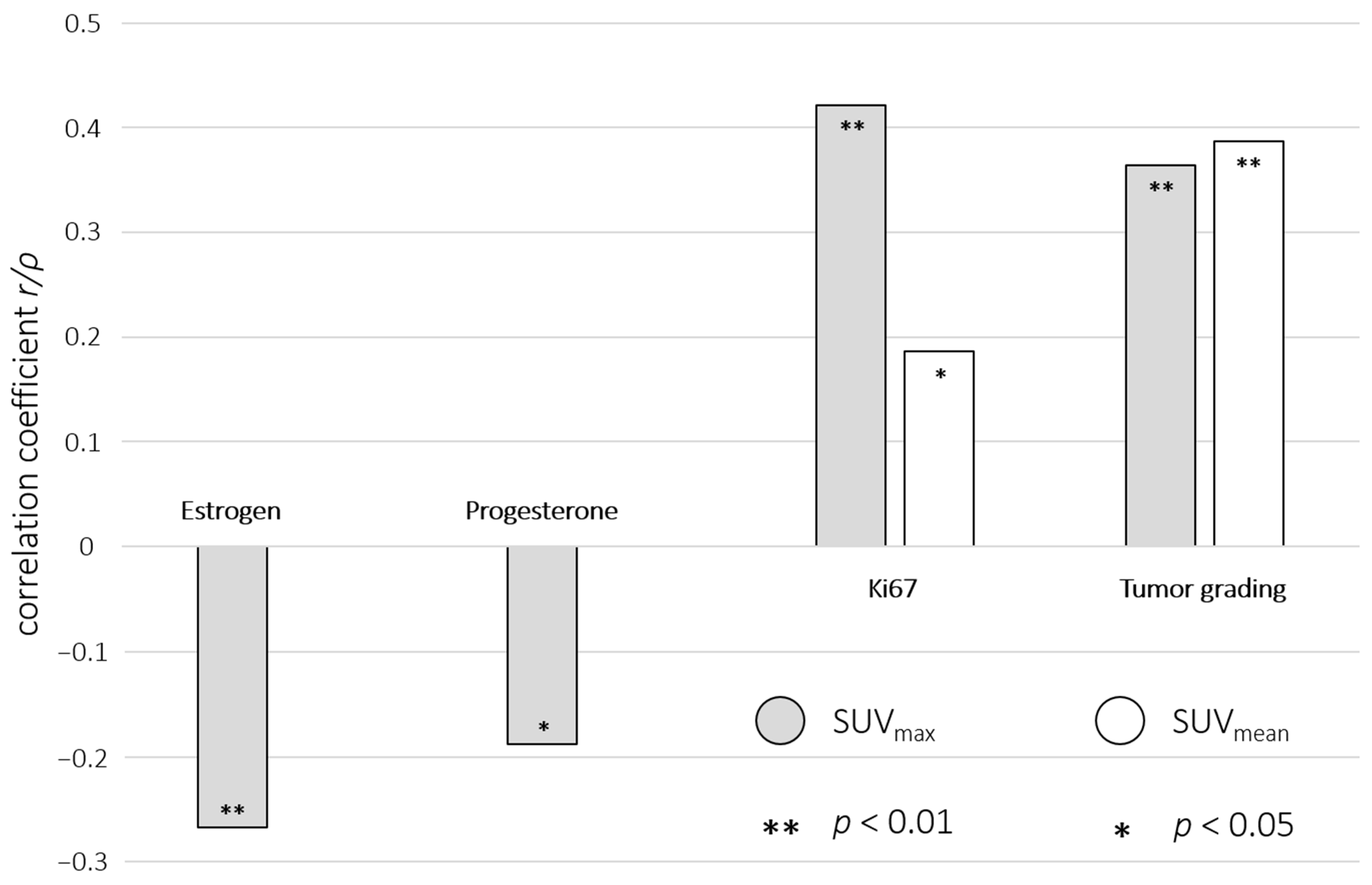
3.2. Correlation of Breast Cancer SUV and ADC with Histopathological Breast Cancer Parameters
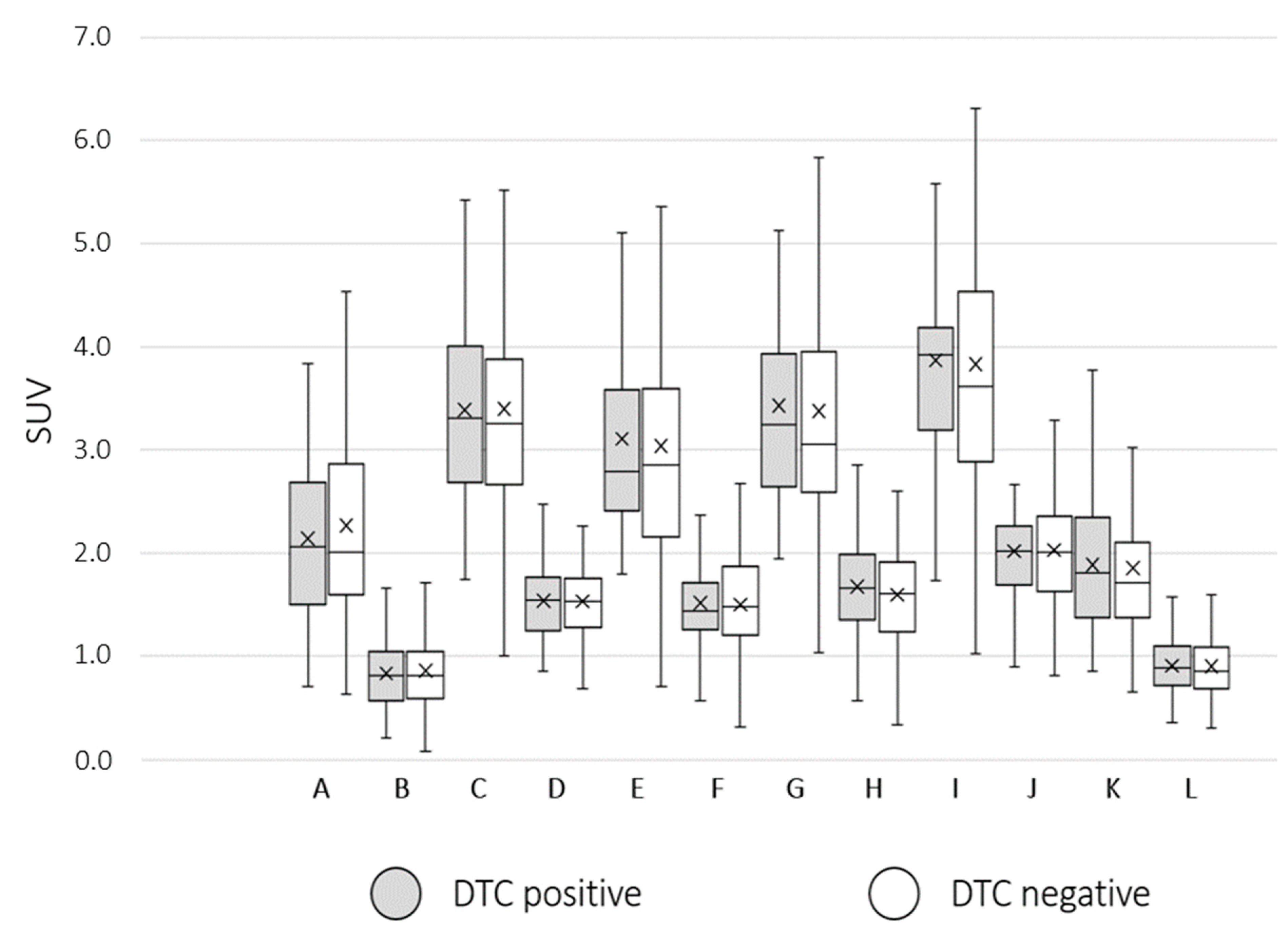
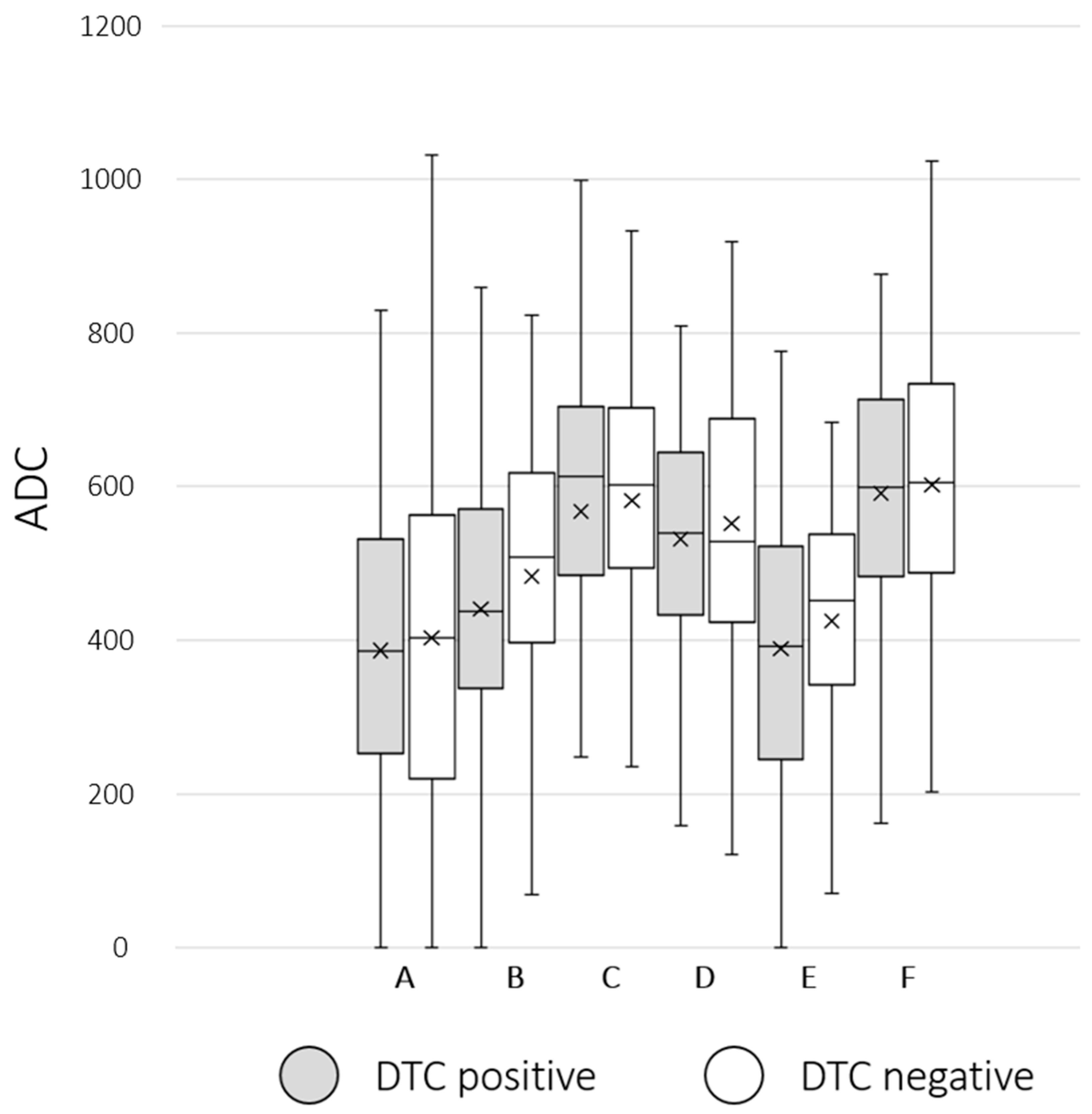
3.3. Group Comparison of Bone Marrow SUV/ADC between DTC-Positive and DTC-Negative Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Rose, J.; Puckett, Y. Breast Reconstruction Free Flaps. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Goldhirsch, A.; Glick, J.H.; Gelber, R.D.; Coates, A.S.; Thürlimann, B.; Senn, H.J. Meeting highlights: International expert consensus on the primary therapy of early breast cancer 2005. Ann. Oncol. 2005, 16, 1569–1583. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoi, H.; Litière, S.; Piccart, M.; MacGrogan, G.; Fumoleau, P.; Brain, E.; Petit, T.; Rouanet, P.; Jassem, J.; Moldovan, C.; et al. Pathological complete response after neoadjuvant chemotherapy is an independent predictive factor irrespective of simplified breast cancer intrinsic subtypes: A landmark and two-step approach analyses from the EORTC 10994/BIG 1-00 phase III trial. Ann. Oncol. 2014, 25, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Groheux, D.; Hindie, E. Breast cancer: Initial workup and staging with FDG PET/CT. Clin. Transl. Imaging 2021, 9, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Shawky, M.; Ali, Z.A.E.; Hashem, D.H.; Houseni, M. Role of positron-emission tomography/computed tomography (PET/CT) in breast cancer. Egypt. J. Radiol. Nucl. Med. 2020, 51, 125. [Google Scholar] [CrossRef]
- Han, S.; Choi, J.Y. Prognostic value of (18)F-FDG PET and PET/CT for assessment of treatment response to neoadjuvant chemotherapy in breast cancer: A systematic review and meta-analysis. Breast Cancer Res. 2020, 22, 119. [Google Scholar] [CrossRef]
- Piscopo, L.; Nappi, C.; Volpe, F.; Romeo, V.; Nicolai, E.; Gallicchio, R.; Giordano, A.; Storto, G.; Pace, L.; Cavaliere, C.; et al. Prognostic Value of Hybrid PET/MR Imaging in Patients with Differentiated Thyroid Cancer. Cancers 2022, 14, 2958. [Google Scholar] [CrossRef]
- Klain, M.; Nappi, C.; Nicolai, E.; Romeo, V.; Piscopo, L.; Giordano, A.; Gaudieri, V.; Zampella, E.; Pace, L.; Carlo, C.; et al. Comparison of simultaneous (18)F-2-[18F] FDG PET/MR and PET/CT in the follow-up of patients with differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 3066–3073. [Google Scholar] [CrossRef]
- Bruckmann, N.M.; Morawitz, J.; Fendler, W.P.; Ruckhäberle, E.; Bittner, A.K.; Giesel, F.L.; Herrmann, K.; Antoch, G.; Umutlu, L.; Kirchner, J. A Role of PET/MR in Breast Cancer? Semin. Nucl. Med. 2022, 52, 611–618. [Google Scholar] [CrossRef]
- Murthy, V.; Sonni, I.; Jariwala, N.; Juarez, R.; Reiter, R.E.; Raman, S.S.; Hope, T.A. The Role of PSMA PET/CT and PET/MRI in the Initial Staging of Prostate Cancer. Eur. Urol. Focus 2021, 7, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Heacock, L.; Weissbrot, J.; Raad, R.; Campbell, N.; Friedman, K.P.; Ponzo, F.; Chandarana, H. PET/MRI for the evaluation of patients with lymphoma: Initial observations. AJR. Am. J. Roentgenol. 2015, 204, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Kirchner, J.; Grueneisen, J.; Martin, O.; Oehmigen, M.; Quick, H.H.; Bittner, A.-K.; Hoffmann, O.; Ingenwerth, M.; Catalano, O.A.; Heusch, P.; et al. Local and whole-body staging in patients with primary breast cancer: A comparison of one-step to two-step staging utilizing 18F-FDG-PET/MRI. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2328–2337. [Google Scholar] [CrossRef] [PubMed]
- Bruckmann, N.M.; Kirchner, J.; Morawitz, J.; Umutlu, L.; Herrmann, K.; Bittner, A.K.; Hoffmann, O.; Mohrmann, S.; Ingenwerth, M.; Schaarschmidt, B.M.; et al. Prospective comparison of CT and 18F-FDG PET/MRI in N and M staging of primary breast cancer patients: Initial results. PLoS ONE 2021, 16, e0260804. [Google Scholar] [CrossRef]
- Bruckmann, N.M.; Kirchner, J.; Umutlu, L.; Fendler, W.P.; Seifert, R.; Herrmann, K.; Bittner, A.-K.; Hoffmann, O.; Mohrmann, S.; Antke, C.; et al. Prospective comparison of the diagnostic accuracy of 18F-FDG PET/MRI, MRI, CT, and bone scintigraphy for the detection of bone metastases in the initial staging of primary breast cancer patients. Eur. Radiol. 2021, 31, 8714–8724. [Google Scholar] [CrossRef]
- Sawicki, L.M.; Grueneisen, J.; Schaarschmidt, B.M.; Buchbender, C.; Nagarajah, J.; Umutlu, L.; Antoch, G.; Kinner, S. Evaluation of 18F-FDG PET/MRI, 18F-FDG PET/CT, MRI, and CT in whole-body staging of recurrent breast cancer. Eur. J. Radiol. 2016, 85, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Grueneisen, J.; Nagarajah, J.; Buchbender, C.; Hoffmann, O.; Schaarschmidt, B.M.; Poeppel, T.; Forsting, M.; Quick, H.H.; Umutlu, L.; Kinner, S. Positron Emission Tomography/Magnetic Resonance Imaging for Local Tumor Staging in Patients With Primary Breast Cancer: A Comparison With Positron Emission Tomography/Computed Tomography and Magnetic Resonance Imaging. Investig. Radiol. 2015, 50, 505–513. [Google Scholar] [CrossRef]
- Mann, R.M.; Cho, N.; Moy, L. Breast MRI: State of the Art. Radiology 2019, 292, 520–536. [Google Scholar] [CrossRef]
- Morawitz, J.; Kirchner, J.; Martin, O.; Bruckmann, N.-M.; Dietzel, F.; Li, Y.; Rischpler, C.; Herrmann, K.; Umutlu, L.; Bittner, A.-K.; et al. Prospective Correlation of Prognostic Immunohistochemical Markers with SUV and ADC Derived from Dedicated Hybrid Breast 18F-FDG PET/MRI in Women with Newly Diagnosed Breast Cancer. Clin. Nucl. Med. 2020. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Friedman, K.; Chandarana, H.; Melsaether, A.; Moy, L.; Ding, Y.S.; Jhaveri, K.; Beltran, L.; Jain, R. Current Status of Hybrid PET/MRI in Oncologic Imaging. AJR Am. J. Roentgenol. 2016, 206, 162–172. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Gnant, M. Breast cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.J.; Chan, J.J.; Kamis, S.; Dent, R.A. What is the role of immunotherapy in breast cancer? Chin. Clin. Oncol. 2018, 7, 13. [Google Scholar] [CrossRef]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, D.K.; AWMF). S3-Leitlinie Früherkennung, Diagnose, Therapie und Nachsorge des Mammakarzinoms; Version 4.4.; 2021, Berlin (AWMF, DKG, DKH). AWMF Registernummer: 032-045OL. Available online: http://www.leitlinienprogramm-onkologie.de/leitlinien/mammakarzinom/ (accessed on 10 January 2023).
- Hartkopf, A.D.; Wallwiener, M.; Hahn, M.; Fehm, T.N.; Brucker, S.Y.; Taran, F.A. Simultaneous Detection of Disseminated and Circulating Tumor Cells in Primary Breast Cancer Patients. Cancer Res. Treat. 2016, 48, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Friberg, S.; Nyström, A. Cancer Metastases: Early Dissemination and Late Recurrences. Cancer Growth Metastasis 2015, 8, 43–49. [Google Scholar] [CrossRef]
- Pantel, K.; Brakenhoff, R.H.; Brandt, B. Detection, clinical relevance and specific biological properties of disseminating tumour cells. Nat. Rev. Cancer 2008, 8, 329–340. [Google Scholar] [CrossRef]
- Hartkopf, A.D.; Brucker, S.Y.; Taran, F.A.; Harbeck, N.; von Au, A.; Naume, B.; Pierga, J.Y.; Hoffmann, O.; Beckmann, M.W.; Rydén, L.; et al. Disseminated tumour cells from the bone marrow of early breast cancer patients: Results from an international pooled analysis. Eur. J. Cancer 2021, 154, 128–137. [Google Scholar] [CrossRef]
- Janvier, L.; Olivier, P.; Blonski, M.; Morel, O.; Vignaud, J.M.; Karcher, G.; Taillandier, L.; Verger, A. Correlation of SUV-Derived Indices With Tumoral Aggressiveness of Gliomas in Static 18F-FDOPA PET: Use in Clinical Practice. Clin. Nucl. Med. 2015, 40, e429–e435. [Google Scholar] [CrossRef]
- Lee, D.W.; Chong, G.O.; Lee, Y.H.; Hong, D.G.; Cho, Y.L.; Jeong, S.Y.; Park, J.Y.; Lee, Y.S. Role of SUVmax and GLUT-1 Expression in Determining Tumor Aggressiveness in Patients With Clinical Stage I Endometrioid Endometrial Cancer. Int. J. Gynecol. Cancer 2015, 25, 843–849. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Bryant, A.S.; Ohja, B.; Bartolucci, A.A. The maximum standardized uptake values on positron emission tomography of a non-small cell lung cancer predict stage, recurrence, and survival. J. Thorac. Cardiovasc. Surg. 2005, 130, 151–159. [Google Scholar] [CrossRef]
- Song, P.J.; Lu, Q.Y.; Li, M.Y.; Li, X.; Shen, F. Comparison of effects of 18F-FDG PET-CT and MRI in identifying and grading gliomas. J. Biol. Regul. Homeost. Agents 2016, 30, 833–838. [Google Scholar]
- Incoronato, M.; Grimaldi, A.M.; Cavaliere, C.; Inglese, M.; Mirabelli, P.; Monti, S.; Ferbo, U.; Nicolai, E.; Soricelli, A.; Catalano, O.A.; et al. Relationship between functional imaging and immunohistochemical markers and prediction of breast cancer subtype: A PET/MRI study. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1680–1693. [Google Scholar] [CrossRef]
- Catalano, O.A.; Horn, G.L.; Signore, A.; Iannace, C.; Lepore, M.; Vangel, M.; Luongo, A.; Catalano, M.; Lehman, C.; Salvatore, M.; et al. PET/MR in invasive ductal breast cancer: Correlation between imaging markers and histological phenotype. Br. J. Cancer 2017, 116, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Meyer, H.J.; Wienke, A. Associations Between PET Parameters and Expression of Ki-67 in Breast Cancer. Transl. Oncol. 2019, 12, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Buchbender, C.; Heusner, T.A.; Lauenstein, T.C.; Bockisch, A.; Antoch, G. Oncologic PET/MRI, part 2: Bone tumors, soft-tissue tumors, melanoma, and lymphoma. J. Nucl. Med. 2012, 53, 1244–1252. [Google Scholar] [CrossRef] [PubMed]
- Razek, A.A. Diffusion magnetic resonance imaging of chest tumors. Cancer Imaging 2012, 12, 452–463. [Google Scholar] [CrossRef]
- Guo, Y.; Cai, Y.Q.; Cai, Z.L.; Gao, Y.G.; An, N.Y.; Ma, L.; Mahankali, S.; Gao, J.H. Differentiation of clinically benign and malignant breast lesions using diffusion-weighted imaging. J. Magn. Reson. Imaging 2002, 16, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Sinha, S.; Lucas-Quesada, F.A.; Sinha, U.; DeBruhl, N.; Bassett, L.W. In vivo diffusion-weighted MRI of the breast: Potential for lesion characterization. J. Magn. Reson. Imaging 2002, 15, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Oehmigen, M.; Lindemann, M.E.; Lanz, T.; Kinner, S.; Quick, H.H. Integrated PET/MR breast cancer imaging: Attenuation correction and implementation of a 16-channel RF coil. Med. Phys. 2016, 43, 4808. [Google Scholar] [CrossRef]
- Quick, H. Integrated PET/MR. J. Magn. Reson. Imaging 2014, 39, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Paulus, D.H.; Quick, H.H.; Geppert, C.; Fenchel, M.; Zhan, Y.; Hermosillo, G.; Faul, D.; Boada, F.; Friedman, K.P.; Koesters, T. Whole-Body PET/MR Imaging: Quantitative Evaluation of a Novel Model-Based MR Attenuation Correction Method Including Bone. J. Nucl. Med. 2015, 56, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Kartmann, R.; Paulus, D.H.; Braun, H.; Aklan, B.; Ziegler, S.; Navalpakkam, B.K.; Lentschig, M.; Quick, H.H. Integrated PET/MR imaging: Automatic attenuation correction of flexible RF coils. Med. Phys. 2013, 40, 82301. [Google Scholar] [CrossRef]
- AGO e. V. Guidelines Breast. Available online: https://www.ago-online.de/fileadmin/ago-online/downloads/_leitlinien/kommission_mamma/2022/englisch/Einzeldateien/AGO_2022E_02_Breast_Cancer_Risk_Genetics_and_Prevention.pdf (accessed on 5 December 2022).
- Prat, A.; Pineda, E.; Adamo, B.; Galván, P.; Fernández, A.; Gaba, L.; Díez, M.; Viladot, M.; Arance, A.; Muñoz, M. Clinical implications of the intrinsic molecular subtypes of breast cancer. Breast 2015, 24, S26–S35. [Google Scholar] [CrossRef] [PubMed]
- van’t Veer, L.J.; Paik, S.; Hayes, D.F. Gene expression profiling of breast cancer: A new tumor marker. J. Clin. Oncol. 2005, 23, 1631–1635. [Google Scholar] [CrossRef]
- Fehm, T.; Braun, S.; Muller, V.; Janni, W.; Gebauer, G.; Marth, C.; Schindlbeck, C.; Wallwiener, D.; Borgen, E.; Naume, B.; et al. A concept for the standardized detection of disseminated tumor cells in bone marrow from patients with primary breast cancer and its clinical implementation. Cancer 2006, 107, 885–892. [Google Scholar] [CrossRef]
- Kasimir-Bauer, S.; Reiter, K.; Aktas, B.; Bittner, A.K.; Weber, S.; Keller, T.; Kimmig, R.; Hoffmann, O. Different prognostic value of circulating and disseminated tumor cells in primary breast cancer: Influence of bisphosphonate intake? Sci. Rep. 2016, 6, 26355. [Google Scholar] [CrossRef]
- Borgen, E.; Naume, B.; Nesland, J.M.; Kvalheim, G.; Beiske, K.; Fodstad, O.; Diel, I.; Solomayer, E.F.; Theocharous, P.; Coombes, R.C.; et al. Standardization of the immunocytochemical detection of cancer cells in BM and blood: I. establishment of objective criteria for the evaluation of immunostained cells. Cytotherapy 1999, 1, 377–388. [Google Scholar] [CrossRef]
- Li, J.; Zhao, M.; Yuan, L.; Liu, Y.; Ma, N. [Correlation and Influencing Factors of SUVmax and Ki-67 in Non-Hodgkin Lymphoma]. Zhongguo Shi Yan Xue Ye Xue Za Zhi 2022, 30, 136–140. [Google Scholar] [CrossRef]
- Shen, G.-h.; Hu, S.; Liu, B.; Kuang, A.r. Degree of SUVmax correlates with Ki-67 index in patients with breast cancer: A meta-analysis. Int. J. Clin. Exp. Pathol. 2017, 10, 1488–1498. [Google Scholar]
- Kitajima, K.; Yamano, T.; Fukushima, K.; Miyoshi, Y.; Hirota, S.; Kawanaka, Y.; Miya, M.; Doi, H.; Yamakado, K.; Hirota, S. Correlation of the SUVmax of FDG-PET and ADC values of diffusion-weighted MR imaging with pathologic prognostic factors in breast carcinoma. Eur. J. Radiol. 2016, 85, 943–949. [Google Scholar] [CrossRef]
- Nakamura, K.; Kodama, J.; Okumura, Y.; Hongo, A.; Kanazawa, S.; Hiramatsu, Y. The SUVmax of 18F-FDG PET Correlates With Histological Grade in Endometrial Cancer. Int. J. Gynecol. Cancer 2010, 20, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Sanli, Y.; Kuyumcu, S.; Ozkan, Z.G.; Işık, G.; Karanlik, H.; Guzelbey, B.; Turkmen, C.; Ozel, S.; Yavuz, E.; Mudun, A. Increased FDG uptake in breast cancer is associated with prognostic factors. Ann. Nucl. Med. 2012, 26, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Yerushalmi, R.; Woods, R.; Ravdin, P.M.; Hayes, M.M.; Gelmon, K.A. Ki67 in breast cancer: Prognostic and predictive potential. Lancet Oncol. 2010, 11, 174–183. [Google Scholar] [CrossRef]
- Haroon, S.; Hashmi, A.A.; Khurshid, A.; Kanpurwala, M.A.; Mujtuba, S.; Malik, B.; Faridi, N. Ki67 index in breast cancer: Correlation with other prognostic markers and potential in pakistani patients. Asian Pac. J. Cancer Prev. 2013, 14, 4353–4358. [Google Scholar] [CrossRef]
- Afkari, H.; Makrufardi, F.; Hidayat, B.; Budiawan, H.; Sundawa Kartamihardja, A.H. Correlation between ER, PR, HER-2, and Ki-67 with the risk of bone metastases detected by bone scintigraphy in breast cancer patients: A cross sectional study. Ann. Med. Surg. 2021, 67, 102532. [Google Scholar] [CrossRef]
- Koo, H.R.; Park, J.S.; Kang, K.W.; Cho, N.; Chang, J.M.; Bae, M.S.; Kim, W.H.; Lee, S.H.; Kim, M.Y.; Kim, J.Y.; et al. 18F-FDG uptake in breast cancer correlates with immunohistochemically defined subtypes. Eur. Radiol. 2014, 24, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Hegazy, R.; Azzam, H. Value of apparent diffusion coefficient factor in correlation with the molecular subtypes, tumor grade, and expression of Ki-67 in breast cancer. Egypt. J. Radiol. Nucl. Med. 2022, 53, 198. [Google Scholar] [CrossRef]
- Park, E.K.; Cho, K.R.; Seo, B.K.; Woo, O.H.; Cho, S.B.; Bae, J.W. Additional Value of Diffusion-Weighted Imaging to Evaluate Prognostic Factors of Breast Cancer: Correlation with the Apparent Diffusion Coefficient. Iran J. Radiol. 2016, 13, e33133. [Google Scholar] [CrossRef]
- Sanaat, Z.; Nouri, O.; Khanzadeh, M.; Mostafaei, H.; Vahed, N.; Kabiri, N.; Khoei, R.A.A.; Salehi-Pourmehr, H. Bisphosphonates and Prevention of the Perimenopausal Breast Cancer Recurrence: A Systematic Review and Meta-Analysis. J. Breast Cancer 2022, 25, 454–472. [Google Scholar] [CrossRef]
- D’Oronzo, S.; Wood, S.; Brown, J.E. The use of bisphosphonates to treat skeletal complications in solid tumours. Bone 2021, 147, 115907. [Google Scholar] [CrossRef] [PubMed]
- Diel, I.J.; Jaschke, A.; Solomayer, E.F.; Gollan, C.; Bastert, G.; Sohn, C.; Schuetz, F. Adjuvant oral clodronate improves the overall survival of primary breast cancer patients with micrometastases to the bone marrow: A long-term follow-up. Ann. Oncol. 2008, 19, 2007–2011. [Google Scholar] [CrossRef] [PubMed]
- Diel, I.J.; Solomayer, E.F.; Costa, S.D.; Gollan, C.; Goerner, R.; Wallwiener, D.; Kaufmann, M.; Bastert, G. Reduction in new metastases in breast cancer with adjuvant clodronate treatment. N. Engl. J. Med. 1998, 339, 357–363. [Google Scholar] [CrossRef]
- Hoffmann, O.; Schroer-Zuendorf, I.A.; Kasimir-Bauer, S.; Oberhoff, C.; Kimmig, R.; Heubner, M. Evaluation of the prognostic significance of disseminated tumor cells in the bone marrow of primary, non-metastatic breast cancer patients after a 7-year follow-up. Arch. Gynecol. Obs. 2015, 292, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, O.; Aktas, B.; Goldnau, C.; Heubner, M.; Oberhoff, C.; Kimmig, R.; Kasimir-Bauer, S. Effect of ibandronate on disseminated tumor cells in the bone marrow of patients with primary breast cancer: A pilot study. Anticancer Res. 2011, 31, 3623–3628. [Google Scholar] [PubMed]
- Hartkopf, A.D.; Banys, M.; Krawczyk, N.; Wallwiener, M.; Schneck, H.; Neubauer, H.; Fehm, T. Circulating Tumor Cells in Early-Stage Breast Cancer. Geburtshilfe Frauenheilkd 2011, 71, 1067–1072. [Google Scholar] [CrossRef]
- Schindlbeck, C.; Andergassen, U.; Hofmann, S.; Jückstock, J.; Jeschke, U.; Sommer, H.; Friese, K.; Janni, W.; Rack, B. Comparison of circulating tumor cells (CTC) in peripheral blood and disseminated tumor cells in the bone marrow (DTC-BM) of breast cancer patients. J. Cancer Res. Clin. Oncol. 2013, 139, 1055–1062. [Google Scholar] [CrossRef]
- Balic, M.; Lin, H.; Young, L.; Hawes, D.; Giuliano, A.; McNamara, G.; Datar, R.H.; Cote, R.J. Most early disseminated cancer cells detected in bone marrow of breast cancer patients have a putative breast cancer stem cell phenotype. Clin. Cancer Res. 2006, 12, 5615–5621. [Google Scholar] [CrossRef]
- Reuben, J.M.; Lee, B.N.; Gao, H.; Cohen, E.N.; Mego, M.; Giordano, A.; Wang, X.; Lodhi, A.; Krishnamurthy, S.; Hortobagyi, G.N.; et al. Primary breast cancer patients with high risk clinicopathologic features have high percentages of bone marrow epithelial cells with ALDH activity and CD44+CD24lo cancer stem cell phenotype. Eur. J. Cancer 2011, 47, 1527–1536. [Google Scholar] [CrossRef]
- Kallergi, G.; Hoffmann, O.; Bittner, A.-K.; Papadimitriou, L.; Katsarou, S.D.; Zacharopoulou, N.; Zervakis, M.; Sfakianakis, S.; Stournaras, C.; Georgoulias, V.; et al. CXCR4 and JUNB double-positive disseminated tumor cells are detected frequently in breast cancer patients at primary diagnosis. Ther. Adv. Med. Oncol. 2020, 12, 1758835919895754. [Google Scholar] [CrossRef]
- Kolb, A.D.; Shupp, A.B.; Mukhopadhyay, D.; Marini, F.C.; Bussard, K.M. Osteoblasts are “educated” by crosstalk with metastatic breast cancer cells in the bone tumor microenvironment. Breast Cancer Res. 2019, 21, 31. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A | Molecular Subtypes | Luminal A | Luminal B HER2− | Triple Negative | HER2+ |
| total 169 | 7 (4%) | 42 (25%) | 23 (14%) | 97 (57%) | |
| B | Tumor Grading | Grade 1 | Grade 2 | Grade 3 | |
| total 169 | 3 (2%) | 100 (59%) | 66 (39%) |
| Malign Breast Lesion PET/MRI | |||
|---|---|---|---|
| SUVmax | SUVmean | ADCmean | |
| Estrogen | r = −0.27 ** | r = −0.07 | r = −0.06 |
| Progesterone | r = −0.19 * | r = −0.11 | r = −0.15 |
| HER2/neu | ρ = −0.07 | ρ = −0.04 | ρ = −0.06 |
| Ki67 | r = 0.42 ** | r = 0.19 * | r = −0.08 |
| Molecular subtype | ρ = 0.04 | ρ = 0.06 | ρ = −0.01 |
| Tumor grading | ρ = 0.36 ** | ρ = 0.39 ** | ρ = 0.02 |
| SUVmax | SUVmean | ADCmean | |||||
|---|---|---|---|---|---|---|---|
| DTC- Negative | DTC- Positive | DTC- Negative | DTC- Positive | DTC- Negative | DTC- Positive | ||
| Right femur | Mdn (IQR) | 2.01 (1.27) | 2.06 (1.18) | 0.81 (0.46) | 0.80 (0.45) | 406.33 (334.25) | 389.45 (284.17) |
| Mann–Whitney-U | U = 1880.00, Z = −0.61, p = 0.54, rrb = −0.05 | U = 1940.50, Z = −0.33, p = 0.75, rrb = −0.03 | U = 1950.00, Z = −0.28, p = 0.78, rrb = −0.03 | ||||
| Os sacrum | Mdn (IQR) | 3.26 (1.23) | 3.31 (1.34) | 1.54 (0.46) | 1.53 (0.51) | 508.94 (196.60) | 438.55 (233.28) |
| Mann–Whitney-U | U = 2099.00, Z = −0.31, p = 0.76, rrb = 0.03 | U = 2149.00, Z = −0.08, p = 0.93, rrb = −0.01 | U = 1724.00, Z = −1.73, p = 0.08, rrb = −0.15 | ||||
| Right os ilium | Mdn (IQR) | 2.85 (1.39) | 2.06 (1.18) | 1.52 (0.66) | 1.44 (0.52) | 610.32 (206.80) | 622.52 (216.27) |
| Mann–Whitney-U | U = 1626.00, Z = −0.17, p = 0.86, rrb = 0.02 | U = 2138.50, Z = −0.13, p = 0.90, rrb = −0.01 | U = 2011.00, Z = −0.41, p = 0.68, rrb = −0.04 | ||||
| L5 | Mdn (IQR) | 3.05 (1.35) | 3.21 (1.22) | 1.61 (0.67) | 1.61 (0.64) | 528.70 (268.14) | 547.02 (218.11) |
| Mann–Whitney-U | U = 2005.50, Z = −0.62, p = 0.54, rrb = 0.05 | U = 1949.00, Z = −0.88, p = 0.38, rrb = −0.08 | U = 2071.00, Z = −0.13, p = 0.89, rrb = −0.01 | ||||
| T7 | Mdn (IQR) | 3.61 (1.52) | 3.92 (1.11) | 2.00 (0.72) | 2.03 (0.56) | 461.64 (200.83) | 411.32 (258.80) |
| Mann–Whitney-U | U = 2018.00, Z = −0.67, p = 0.50, rrb = 0.06 | U = 2141.00, Z = −0.12, p = 0.91, rrb = −0.01 | U = 1866.00, Z = −1.36, p = 0.18, rrb = −0.12 | ||||
| Sternum | Mdn (IQR) | 1.76 (0.74) | 1.75 (0.96) | 0.89 (0.41) | 0.88 (0.37) | 616.46 (232.97) | 597.26 (244.70) |
| Mann–Whitney-U | U = 1990.00, Z = −0.80, p = 0.43, rrb = 0.07 | U = 2122.00, Z = −0.21, p = 0.84, rrb = 0.02 | U = 1950.00, Z = −0.58, p = 0.56, rrb = −0.05 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jannusch, K.; Bittner, A.-K.; Bruckmann, N.M.; Morawitz, J.; Stieglitz, C.; Dietzel, F.; Quick, H.H.; Baba, H.A.; Herrmann, K.; Umutlu, L.; et al. Correlation between Imaging Markers Derived from PET/MRI and Invasive Acquired Biomarkers in Newly Diagnosed Breast Cancer. Cancers 2023, 15, 1651. https://doi.org/10.3390/cancers15061651
Jannusch K, Bittner A-K, Bruckmann NM, Morawitz J, Stieglitz C, Dietzel F, Quick HH, Baba HA, Herrmann K, Umutlu L, et al. Correlation between Imaging Markers Derived from PET/MRI and Invasive Acquired Biomarkers in Newly Diagnosed Breast Cancer. Cancers. 2023; 15(6):1651. https://doi.org/10.3390/cancers15061651
Chicago/Turabian StyleJannusch, Kai, Ann-Kathrin Bittner, Nils Martin Bruckmann, Janna Morawitz, Cleo Stieglitz, Frederic Dietzel, Harald H. Quick, Hideo A. Baba, Ken Herrmann, Lale Umutlu, and et al. 2023. "Correlation between Imaging Markers Derived from PET/MRI and Invasive Acquired Biomarkers in Newly Diagnosed Breast Cancer" Cancers 15, no. 6: 1651. https://doi.org/10.3390/cancers15061651
APA StyleJannusch, K., Bittner, A.-K., Bruckmann, N. M., Morawitz, J., Stieglitz, C., Dietzel, F., Quick, H. H., Baba, H. A., Herrmann, K., Umutlu, L., Antoch, G., Kirchner, J., Kasimir-Bauer, S., & Hoffmann, O. (2023). Correlation between Imaging Markers Derived from PET/MRI and Invasive Acquired Biomarkers in Newly Diagnosed Breast Cancer. Cancers, 15(6), 1651. https://doi.org/10.3390/cancers15061651