
Evaluating the Effectiveness of Visuospatial Memory Stimulation Using Virtual Reality in Head and Neck Cancer Patients—Pilot Study


Abstract
Simple Summary
Abstract
1. Introduction
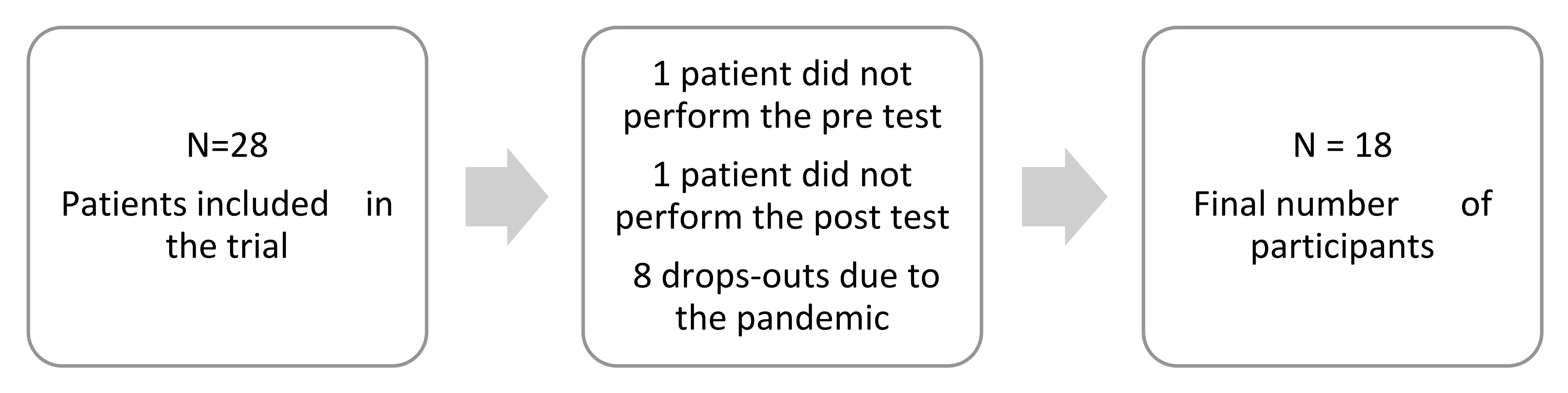
2. Material and Methods
3. Results
Correlations
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CRCI | cancer-related cognitive Impairment |
| VR | virtual reality |
| HCN | head and neck cancer |
| CHT | chemotherapy |
| RT | radiation therapy |
| VSWM | visuospatial working memory |
| HMD | head mounted display |
| CTTPs | computerized cognitive training programs |
References
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.-W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [PubMed]
- Global Cancer Observatory. International Agency for Research on Cancer. World Health Organization. Available online: https://gco.iarc.fr/ (accessed on 6 June 2021).
- Cognetti, D.M.; Weber, R.S.; Lai, S.Y. Head and neck cancer: An evolving treatment paradigm. Cancer 2008, 113 (Suppl. 7), 1911–1932. [Google Scholar] [CrossRef]
- Camina, E.; Güell, F. The Neuroanatomical, Neurophysiological and Psychological Basis of Memory: Current Models and Their Origins. Front. Pharmacol. 2017, 8, 438. [Google Scholar] [CrossRef] [PubMed]
- Gates, P.; Krishnasamy, M.; Wilson, C.; Hawkes, E.A.; Doré, V.; Perchyonok, Y.; Rowe, C.C.; Walker, A.K.; Vardy, J.L.; de Ruiter, M.B.; et al. Cancer-related cognitive impairment in patients with newly diagnosed aggressive lymphoma undergoing standard chemotherapy: A longitudinal feasibility study. Support Care Cancer 2022, 30, 7731–7743. [Google Scholar] [CrossRef]
- Rizzo, A.A.; Buckwalter, J.G.; Bowerly, T.; Van Der Zaag, C.; Humphrey, L.; Neumann, U.; Chua, C.; Kyriakakis, C.; Van Rooyen, A.; Sisemore, D. The virtual classroom: A virtual reality environment for the assessment and rehabilitation of attention deficits. CyberPsychol. Behav. 2000, 3, 483–499. [Google Scholar] [CrossRef]
- Parsons, T.D.; Rizzo, A.A. Neuropsychological assessment of attentional processing using virtual reality. Annu. Rev. CyberTher. Telemed. 2008, 6, 23–28. [Google Scholar]
- Knight, R.G.; Titov, N. Use of virtual reality tasks to assess prospective memory: Applicability and evidence. Brain Impair. 2009, 10, 3–13. [Google Scholar] [CrossRef]
- Albani, G.; Raspelli, S.; Carelli, L.; Morganti, F.; Weiss, P.L.; Kizony, R.; Katz, N.; Mauro, A.; Riva, G. Executive functions in a virtual world: A study in Parkinson’s disease. Stud. Health Technol. Inform. 2010, 154, 92–96. [Google Scholar] [CrossRef]
- Kim, E.; Han, J.; Choi, H.; Prié, Y.; Vigier, T.; Bulteau, S.; Kwon, G.H. Examining the Academic Trends in Neuropsychological Tests for Executive Functions Using Virtual Reality: Systematic Literature Review. JMIR Serious Games 2021, 9, e30249. [Google Scholar] [CrossRef]
- Dos Santos, M.; Hardy-Léger, I.; Rigal, O.; Licaj, I.; Dauchy, S.; Levy, C.; Noal, S.; Segura, C.; Delcambre, C.; Allouache, D.; et al. Cognitive rehabilitation program to improve cognition of cancer patients treated with chemotherapy: A 3-arm randomized trial. Cancer 2020, 126, 5328–5336. [Google Scholar] [CrossRef]
- Lehrl, S.; Fischer, B. The basic parameters of human information processing: Their role in the determination of intelligence. Personal. Individ. Differ. 1988, 9, 883–896. [Google Scholar] [CrossRef]
- Rostoft, S.; van den Bos, F.; Pedersen, R.; Hamaker, M.E. Shared decision-making in older patients with cancer—What does the patient want? J. Geriatr. Oncol. 2021, 12, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Leão, I.; Garcia, C.; Antunes, P.; Campolargo, A.; Dias, I.; Coimbra, E.; Oliveira, P.; Zenha, H.; Costa, H.; Capela, A.; et al. Acute Impact of Cancer Treatment on Head and Neck Cancer Patients: FIT4TREATMENT. Cancers 2022, 14, 2698. [Google Scholar] [CrossRef] [PubMed]
- Raji, M.A.; Kuo, Y.F.; Freeman, J.L.; Goodwin, J.S. Effect of a dementia diagnosis on survival of older patients after a diagnosis of breast, colon, or prostate cancer: Implications for cancer care. Arch. Intern. Med. 2008, 168, 2033–2040. [Google Scholar] [CrossRef]
- Mohile, S.G.; Mohamed, M.R.; Xu, H.; Culakova, E.; Loh, K.P.; Magnuson, A.; Flannery, M.A.; Obrecht, S.; Gilmore, N.; Ramsdale, E.; et al. Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): A cluster-randomised study. Lancet 2021, 398, 1894–1904. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, G.F.; Šaltytė Benth, J.; Grønberg, B.H.; Rostoft, S.; Kirkevold, Ø.; Bergh, S.; Hjelstuen, A.; Rolfson, D.; Slaaen, M. Cognitive Trajectories in Older Patients with Cancer Undergoing Radiotherapy—A Prospective Observational Study. Curr. Oncol. 2022, 29, 5164–5178. [Google Scholar] [CrossRef]
- Korsten, L.H.A.; Jansen, F.; de Haan, B.J.F.; Sent, D.; Cuijpers, P.; Leemans, C.R.; Verdonck-de Leeuw, I.M. Factors associated with depression over time in head and neck cancer patients: A systematic review. Psychooncology 2019, 28, 1159–1183. [Google Scholar] [CrossRef]
- Mirosevic, S.; Thewes, B.; van Herpen, C.; Kaanders, J.; Merkx, T.; Humphris, G.; Baatenburg de Jong, R.J.; Langendijk, J.A.; Leemans, C.R.; Terhaard, C.H.J.; et al. Prevalence and clinical and psychological correlates of high fear of cancer recurrence in patients newly diagnosed with head and neck cancer. Head Neck 2019, 41, 3187–3200. [Google Scholar] [CrossRef]
- Odynets, T.; Briskin, Y.; Todorova, V.; Bondarenko, O. Impact of different exercise interventions on anxiety and depression in breast cancer patients. Physiother. Q. 2019, 27, 31–36. [Google Scholar] [CrossRef]
- Davis, J.; Ahlberg, F.M.; Berk, M.; Ashley, D.M.; Khasraw, M. Emerging pharmacotherapy for cancer patients with cognitive dysfunction. BMC Neurol. 2013, 13, 153. [Google Scholar] [CrossRef]
- Lange, M.; Joly, F.; Vardy, J.; Ahles, T.; Dubois, M.; Tron, L.; Winocur, G.; De Ruiter, M.B.; Castel, H. Cancer-related cognitive impairment: An update on state of the art, detection, and management strategies in cancer survivors. Ann. Oncol. 2019, 30, 1925–1940. [Google Scholar] [CrossRef] [PubMed]
- Vizer, L.M.; Mikles, S.P.; Piepmeier, A.T. Cancer-related cognitive impairment in survivors of adolescent and young adult non-central nervous system cancer: A scoping review. Psychooncology 2022, 31, 1275–1285. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, T.; Voinescu, A.; Petrini, K.; Stanton Fraser, D. Efficacy and Moderators of Virtual Reality for Cognitive Training in People with Dementia and Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. J. Alzheimers Dis. 2022, 88, 1341–1370. [Google Scholar] [CrossRef]
- Chen, X.; Liu, F.; Lin, S.; Yu, L.; Lin, R. Effects of Virtual Reality Rehabilitation Training on Cognitive Function and Activities of Daily Living of Patients with Poststroke Cognitive Impairment: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2022, 103, 1422–1435. [Google Scholar] [CrossRef]
- Chirico, A.; Lucidi, F.; De, L.M.; Milanese, C.; Napoli, A.; Giordano, A. Virtual Reality in Health System: Beyond Entertainment. A Mini-Review on the Efficacy of VR During Cancer Treatment. J. Cell. Physiol. 2016, 231, 275–287. [Google Scholar] [CrossRef]
- Zeng, Y.; Zeng, L.; Cheng, A.S.K.; Wei, X.; Wang, B.; Jiang, J.; Zhou, J. The Use of Immersive Virtual Reality for Cancer-Related Cognitive Impairment Assessment and Rehabilitation: A Clinical Feasibility Study. Asia-Pac. J. Oncol. Nurs. 2022, 9, 100079. [Google Scholar] [CrossRef]
- Zeng, Y.; Zhang, J.E.; Cheng, A.S.K.; Cheng, H.; Wefel, J.S. Meta-Analysis of the Efficacy of Virtual Reality-Based Interventions in Cancer-Related Symptom Management. Integr. Cancer Ther. 2019, 18, 1534735419871108. [Google Scholar] [CrossRef]
- Pandrangi, V.C.; Shah, S.N.; Bruening, J.D.; Wax, M.K.; Clayburgh, D.; Andersen, P.E.; Li, R.J. Effect of Virtual Reality on Pain Management and Opioid Use Among Hospitalized Patients After Head and Neck Surgery: A Randomized Clinical Trial. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 724–730. [Google Scholar] [CrossRef]
- Mazurek, J.; Kiper, P.; Cieślik, B.; Rutkowski, S.; Mehlich, K.; Turolla, A.; Szczepańska-Gieracha, J. Virtual reality in medicine: A brief overview and future research directions. Hum. Mov. 2019, 20, 16–22. [Google Scholar] [CrossRef]
- House, G.; Burdea, G.; Grampurohit, N.; Polistico, K.; Roll, D.; Damiani, F.; Hundal, J.; Demesmin, D. A feasibility study to determine the benefits of upper extremity virtual rehabilitation therapy for coping with chronic pain post-cancer surgery. Br. J. Pain 2016, 10, 186–197. [Google Scholar] [CrossRef]
- Martínez-Esparza, I.C.; Olivares-Olivares, P.J.; Rosa-Alcázar, Á.; Rosa-Alcázar, A.I.; Storch, E.A. Executive Functioning and Clinical Variables in Patients with Obsessive-Compulsive Disorder. Brain Sci. 2021, 11, 267. [Google Scholar] [CrossRef] [PubMed]
- Sciancalepore, F.; Tariciotti, L.; Remoli, G.; Menegatti, D.; Carai, A.; Petruzzellis, G.; Miller, K.P.; Delli Priscoli, F.; Giuseppi, A.; Premuselli, R.; et al. Computer-Based Cognitive Training in Children with Primary Brain Tumours: A Systematic Review. Cancers 2022, 14, 3879. [Google Scholar] [CrossRef] [PubMed]
- Linden, M.; Hawley, C.; Blackwood, B.; Evans, J.; Anderson, V.; O’Rourke, C. Technological aids for the rehabilitation of memory and executive functioning in children and adolescents with acquired brain injury. Cochrane Database Syst. Rev. 2016, 7, CD011020. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sex | Age | Edu. | Diagnosis ICD-10 Code | TNM Classification | Treatment | |
|---|---|---|---|---|---|---|
| P1 | M | 51 | 3 | C01—Malignant neoplasm of base of tongue | T3 N0 M0 | Induction radiotherapy 69.96 Gy/33 fr. |
| P2 | M | 38 | 3 | C06.0 Cheek mucosa | T2 N3 M0 | Radical radiotherapy 66.96 Gy/33 fr. combined with chemotherapy |
| P3 | F | 49 | 3 | C09.9 –Tonsil, unspecified | T4a N2b M0 | Radical radiotherapy 69.96 Gy/33 fr. combined with chemotherapy |
| P4 | M | 58 | 3 | C15.0—Cervical part of esophagus | T3 N1 M0 | Radical radiotherapy 30 Gy/10 fr. |
| P5 | F | 66 | 4 | C.77—Secondary and unspecified malignant neoplasm of lymph nodes | T0 N3 M0 | Radical radiotherapy 69.96 Gy/33 fr. combined with chemotherapy |
| P6 | F | 66 | 4 | C32.8—Overlapping lesion of larynx | T4 N2 M0 | Radical radiotherapy 66.96 Gy/33 fr. combined with chemotherapy |
| P7 | F | 64 | 3 | C13—Malignant neoplasm of hypopharynx | T3 N0 M0 | Radical radiotherapy 69.96 Gy/33 fr. combined with chemotherapy |
| P8 | M | 67 | 4 | C77.9—Lymph node, unspecified | T1 N3 M0 | Radical radiotherapy 69.96 Gy/33 fr. combined with chemotherapy |
| P9 | M | 76 | 4 | C06.0—Cheek mucosa | T1 N1 M0 | Radical radiotherapy 60 Gy/30 fr. |
| P10 | F | 76 | 5 | C32—Glottis | T4 N2 M0 | Radical radiotherapy 66.96 Gy/33 fr. combined with chemotherapy |
| P11 | M | 49 | 5 | C01—Malignant neoplasm of base of tongue | T4a N2b M0 | Radical radiotherapy 66 Gy/33 fr. combined with chemotherapy |
| P12 | F | 62 | 2 | C32.9—Larynx, unspecified | T4a N0 M0 | Radical radiotherapy 69.96 Gy/33 fr. |
| P13 | F | 70 | 3 | C03.1—Malignant neoplasm of lower gum | T4 N1 M0 | Radical radiotherapy 69 Gy/33 fr. combined with chemotherapy |
| P14 | M | 67 | 1 | C09.9—Malignant neoplasm of tonsil, unspecified | T3N2 M0 | Radical radiotherapy 69.96 Gy/33 fr. combined with chemotherapy |
| P15 | M | 63 | 3 | C09.9 Malignant neoplasm of tonsil, unspecified | T3N2 M0 | Radical radiotherapy 69.96 Gy/33 fr. combined with chemotherapy |
| P16 | M | 65 | 3 | C06.0 Cheek mucosa | T3 N2a M0(x) | Radical radiotherapy 66.96 Gy/33 fr. combined with chemotherapy |
| P17 | M | 64 | 3 | C05—Malignant neoplasm of palate | T4 N2b M0 | Radical radiotherapy 50 Gy/20 fr. |
| P18 | M | 63 | 3 | C02—Malignant neoplasm of other and unspecified parts of tongue | T1 N3 M0 | Radical radiotherapy 50 Gy/20 fr. |
| Study | Variables | p-Value | ||
|---|---|---|---|---|
| Age | Sex | Education | ||
| Pre | time (s) | 0.53 | 0.53 | 0.74 |
| VSWM | 0.82 | 0.82 | 0.53 | |
| correct | 0.86 | 0.86 | 0.67 | |
| incorrect | 0.25 | 0.25 | 0.48 | |
| omitted | 0.45 | 0.45 | 0.22 | |
| sequence error | 0.44 | 0.44 | 0.66 | |
| Post | time (s) | 0.45 | 0.45 | 0.93 |
| VSWM | 0.85 | 0.85 | 0.19 | |
| correct | 0.93 | 0.93 | 0.26 | |
| incorrect | 0.89 | 0.89 | 0.15 | |
| omitted | 0.46 | 0.46 | 0.44 | |
| sequence error | 0.96 | 0.96 | 1.00 | |
| Variables | N | T | Z | p | Study | Median | Min | Max |
|---|---|---|---|---|---|---|---|---|
| time | 18 | 49 | 1.59 | 0.11 | pre | 196 | 73 | 320 |
| post | 228 | 80 | 307 | |||||
| VSWM | 7 | 10.5 | 0.59 | 0.55 | pre | 4 | 2 | 5 |
| post | 4 | 2 | 5 | |||||
| correct | 15 | 31 | 1.65 | 0.09 | pre | 6 | 0 | 8 |
| post | 5 | 1 | 9 | |||||
| incorrect | 14 | 47 | 0.35 | 0.72 | pre | 4 | 3 | 6 |
| post | 4 | 3 | 6 | |||||
| omitted | 3 | 0 | 1.60 | 0.1 | pre | 0 | 0 | 1 |
| post | 0 | 0 | 3 | |||||
| sequence error | 16 | 63.5 | 0.23 | 0.81 | pre | 2 | 0 | 4 |
| post | 2 | 0 | 4 |
| Study | P | Time (s) | D | VSWM | D | Correct | D | Incorrect | D | Omitted | D | Sequence Error | D |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | P1 | 186 | + | 4 | + | 6 | + | 4 | + | 0 | +/− | 3 | + |
| Post | 213 | 5 | 9 | 3 | 0 | 1 | |||||||
| Pre | P2 | 215 | + | 5 | +/− | 8 | + | 3 | − | 0 | +/− | 1 | − |
| Post | 239 | 5 | 9 | 4 | 0 | 3 | |||||||
| Pre | P3 | 205 | + | 5 | +/− | 8 | − | 4 | − | 0 | +/− | 2 | − |
| Post | 217 | 5 | 7 | 6 | 0 | 4 | |||||||
| Pre | P4 | 265 | − | 5 | +/− | 7 | + | 4 | + | 0 | +/− | 1 | +/− |
| Post | 245 | 5 | 8 | 3 | 0 | 1 | |||||||
| Pre | P5 | 246 | − | 4 | + | 6 | + | 6 | + | 0 | +/− | 0 | − |
| Post | 241 | 5 | 8 | 4 | 0 | 1 | |||||||
| Pre | P6 | 247 | + | 5 | +/− | 7 | + | 4 | + | 0 | − | 1 | + |
| Post | 307 | 5 | 8 | 3 | 1 | 0 | |||||||
| Pre | P7 | 219 | − | 4 | +/− | 6 | +/− | 5 | +/− | 0 | +/− | 3 | + |
| Post | 208 | 4 | 6 | 5 | 0 | 2 | |||||||
| Pre | P8 | 73 | + | 3 | + | 2 | + | 3 | +/− | 0 | +/− | 3 | + |
| Post | 131 | 4 | 5 | 3 | 0 | 2 | |||||||
| Pre | P9 | 320 | − | 4 | +/− | 6 | + | 6 | + | 0 | +/− | 3 | + |
| Post | 289 | 4 | 7 | 4 | 0 | 1 | |||||||
| Pre | P10 | 160 | + | 3 | + | 4 | + | 4 | +/− | 0 | +/− | 1 | − |
| Post | 190 | 4 | 5 | 4 | 0 | 3 | |||||||
| Pre | P11 | 137 | − | 4 | +/− | 5 | +/− | 4 | + | 0 | +/− | 4 | + |
| Post | 118 | 4 | 5 | 3 | 0 | 3 | |||||||
| Pre | P12 | 126 | + | 2 | + | 0 | + | 3 | − | 0 | +/− | 0 | − |
| Post | 179 | 3 | 2 | 4 | 0 | 1 | |||||||
| Pre | P13 | 139 | + | 3 | +/− | 2 | + | 4 | − | 1 | +/− | 1 | − |
| Post | 249 | 3 | 3 | 5 | 1 | 2 | |||||||
| Pre | P14 | 185 | + | 2 | +/− | 1 | + | 5 | − | 1 | − | 0 | − |
| Post | 278 | 2 | 2 | 6 | 3 | 2 | |||||||
| Pre | P15 | 147 | + | 2 | +/− | 1 | + | 3 | − | 0 | − | 2 | + |
| Post | 289 | 2 | 2 | 5 | 2 | 0 | |||||||
| Pre | P16 | 111 | − | 2 | +/− | 1 | +/− | 4 | + | 0 | +/− | 2 | +/− |
| Post | 80 | 2 | 1 | 3 | 0 | 2 | |||||||
| Pre | P17 | 223 | + | 3 | − | 3 | − | 5 | +/− | 1 | +/− | 2 | + |
| Post | 256 | 2 | 1 | 5 | 1 | 0 | |||||||
| Pre | P18 | 223 | − | 4 | − | 6 | − | 4 | + | 0 | +/− | 3 | + |
| Post | 80 | 2 | 1 | 3 | 0 | 2 |
| A | VSWM | Correct | Incorrect | Omitted | Sequence Error | Time (s) |
|---|---|---|---|---|---|---|
| VSWM | 0.000 * | 0.642 | 0.113 | 0.530 | 0.003 * | |
| correct | 0.000 * | 0.502 | 0.121 | 0.584 | 0.001 * | |
| incorrect | 0.642 | 0.502 | 0.188 | 0.955 | 0.012 * | |
| omitted | 0.113 | 0.121 | 0.188 | 0.234 | 0.821 | |
| squence error | 0.530 | 0.584 | 0.955 | 0.234 | 0.793 | |
| time | 0.003 * | 0.001 * | 0.012 * | 0.821 | 0.793 | |
| B | VSWM | Correct | Incorrect | Omitted | Sequence error | Time (s) |
| VSWM | 0.000 * | 0.324 | 0.062 | 0.649 | 0.628 | |
| correct | 0.000 * | 0.446 | 0.160 | 0.889 | 0.293 | |
| incorrect | 0.324 | 0.446 | 0.044 * | 0.716 | 0.002 * | |
| omitted | 0.062 | 0.160 | 0.044 * | 0.078 | 0.002 * | |
| sequence error | 0.649 | 0.889 | 0.716 | 0.078 | 0.015 * | |
| time | 0.628 | 0.293 | 0.002 * | 0.002 * | 0.015 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serweta-Pawlik, A.; Lachowicz, M.; Żurek, A.; Rosen, B.; Żurek, G. Evaluating the Effectiveness of Visuospatial Memory Stimulation Using Virtual Reality in Head and Neck Cancer Patients—Pilot Study. Cancers 2023, 15, 1639. https://doi.org/10.3390/cancers15061639
Serweta-Pawlik A, Lachowicz M, Żurek A, Rosen B, Żurek G. Evaluating the Effectiveness of Visuospatial Memory Stimulation Using Virtual Reality in Head and Neck Cancer Patients—Pilot Study. Cancers. 2023; 15(6):1639. https://doi.org/10.3390/cancers15061639
Chicago/Turabian StyleSerweta-Pawlik, Anna, Maciej Lachowicz, Alina Żurek, Bill Rosen, and Grzegorz Żurek. 2023. "Evaluating the Effectiveness of Visuospatial Memory Stimulation Using Virtual Reality in Head and Neck Cancer Patients—Pilot Study" Cancers 15, no. 6: 1639. https://doi.org/10.3390/cancers15061639
APA StyleSerweta-Pawlik, A., Lachowicz, M., Żurek, A., Rosen, B., & Żurek, G. (2023). Evaluating the Effectiveness of Visuospatial Memory Stimulation Using Virtual Reality in Head and Neck Cancer Patients—Pilot Study. Cancers, 15(6), 1639. https://doi.org/10.3390/cancers15061639