

MUC1 Expressions and Its Prognostic Values in US Gastric Cancer Patients
 , , ,
, , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Gastric Cancer Treatment
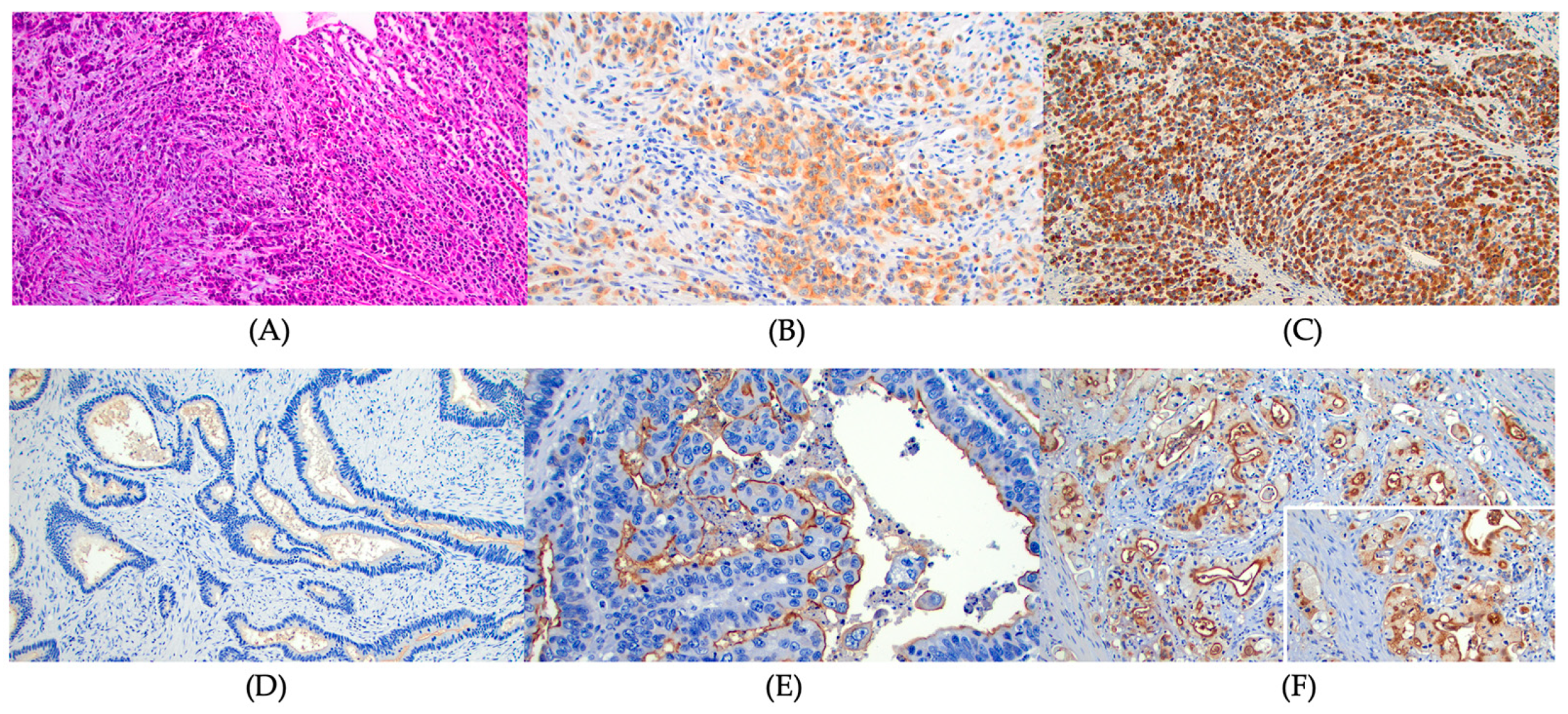
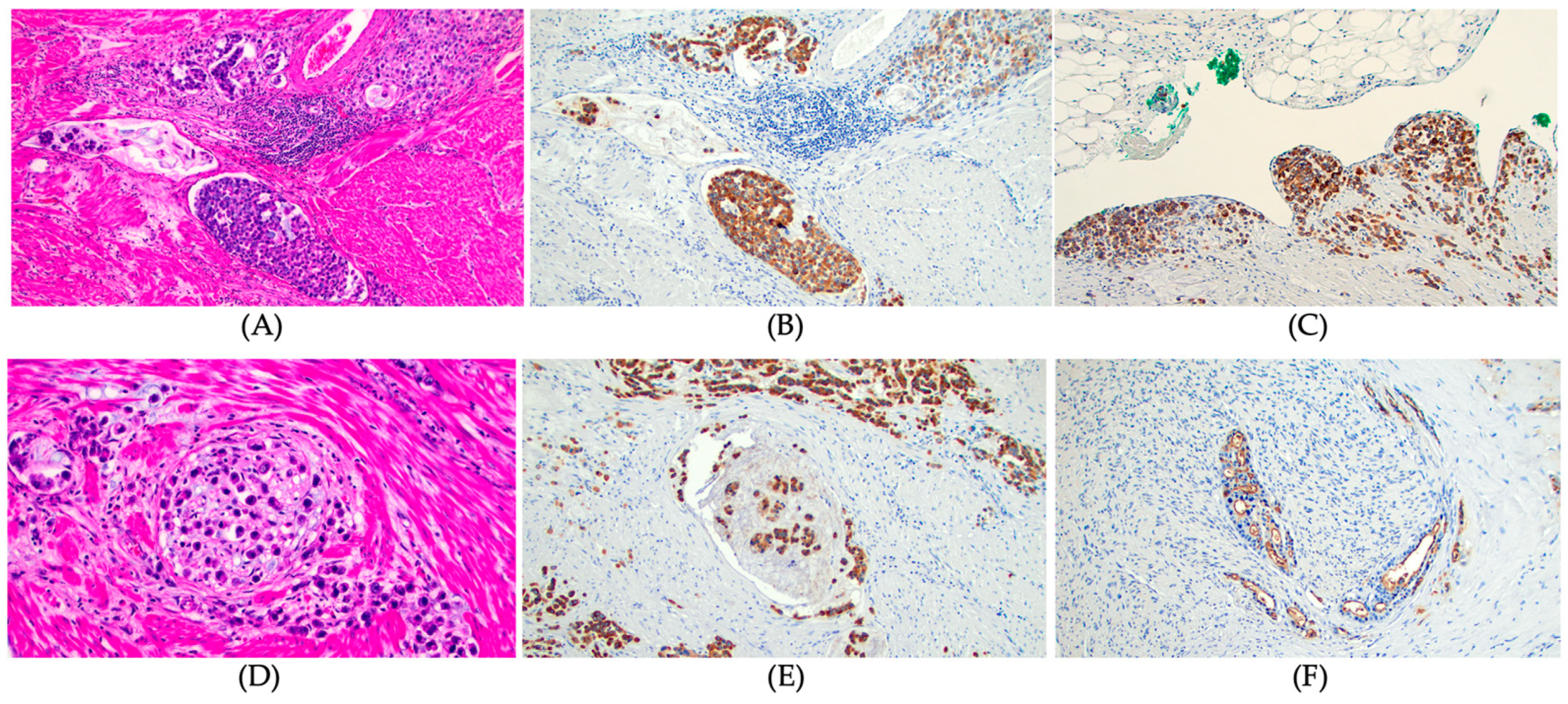
2.3. Immunohistochemical (IHC) Stain and Evaluation of MUC Expression
2.4. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics and Pathological Findings
3.2. Mucin Expression and Pathological Features of Gastric Cancer
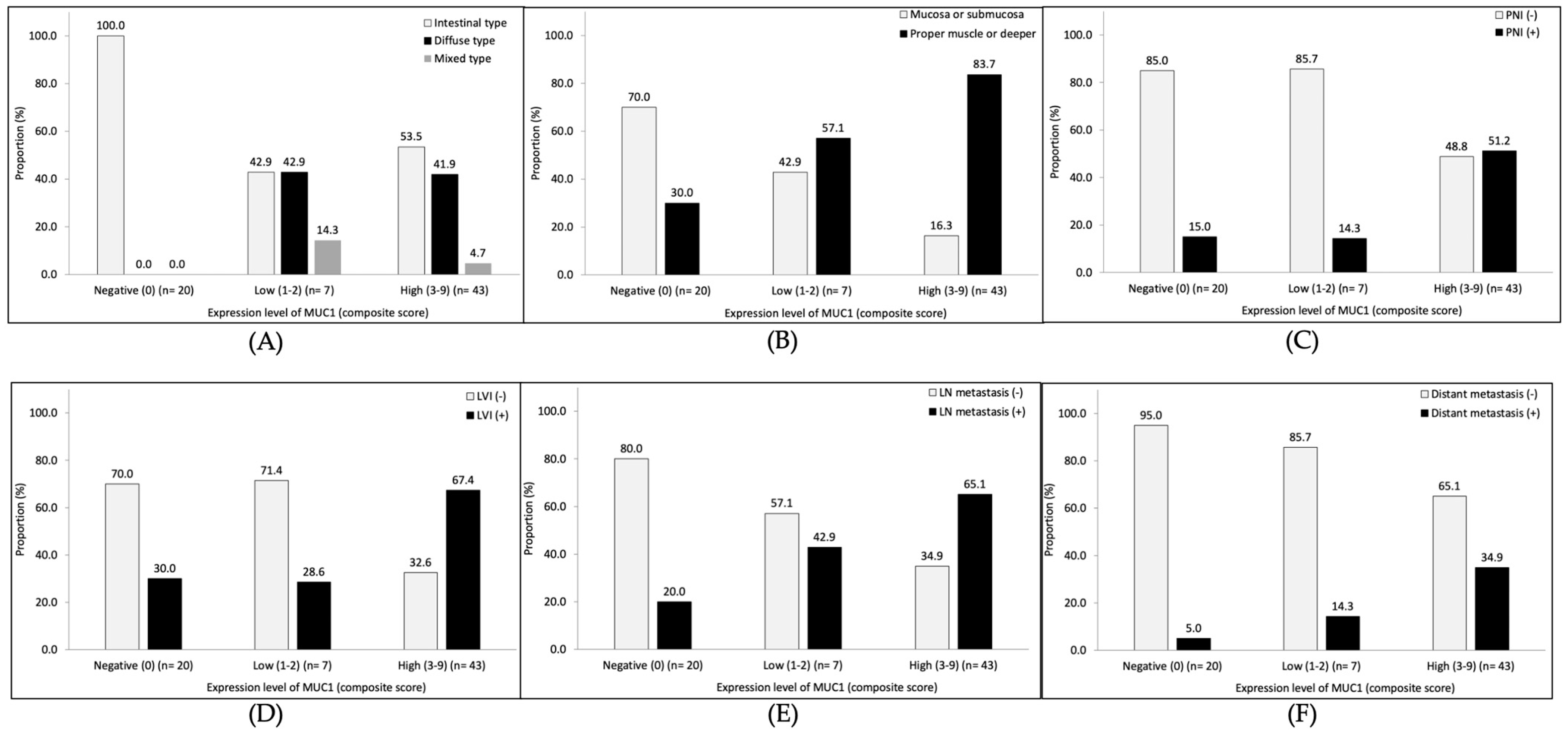
3.3. Pathological Features of Gastric Cancer According to MUC1 Expression Levels
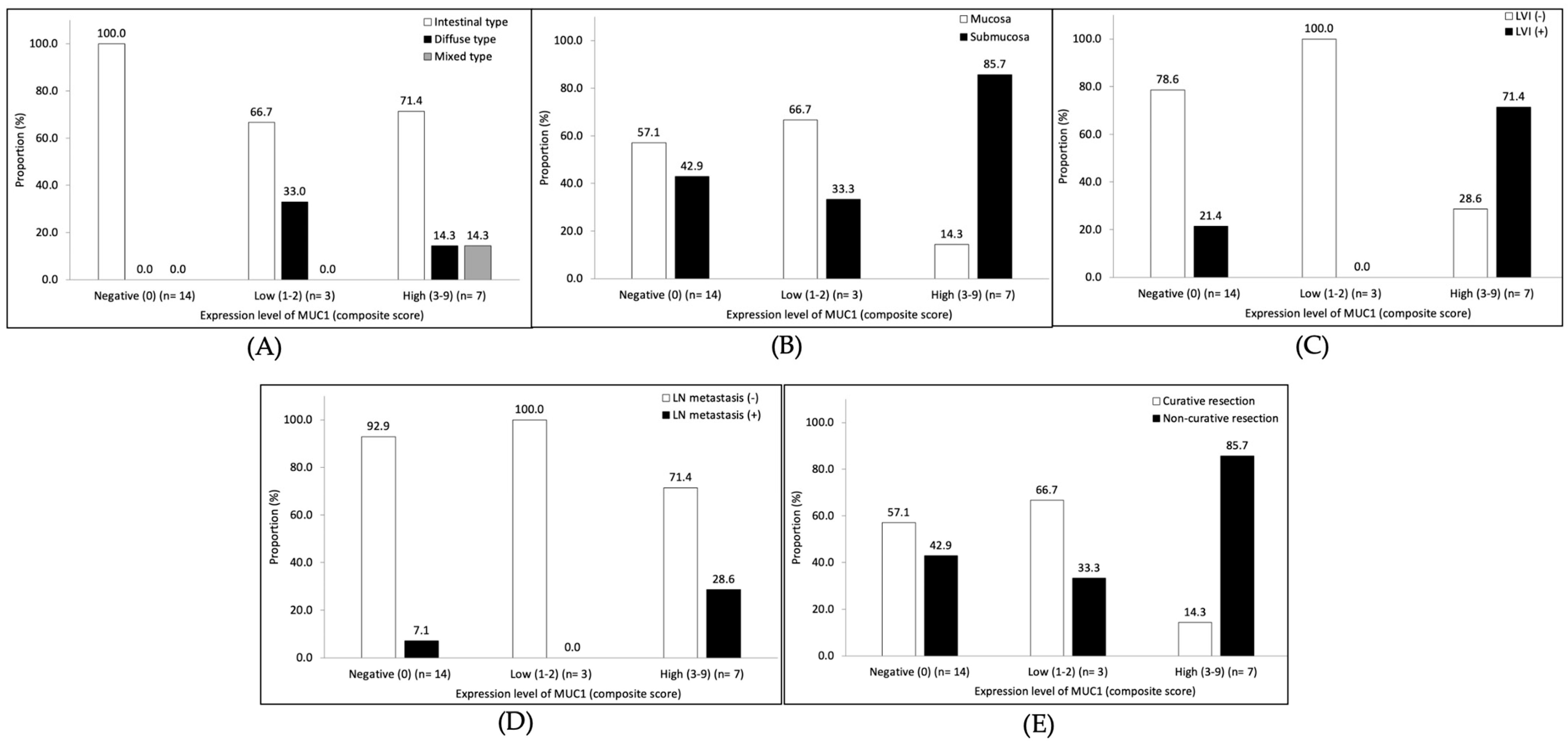
3.4. MUC1 Expression in Early Gastric Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Stomach Cancer. National Institutes of Health. Available online: https://seer.cancer.gov/statfacts/html/stomach.html (accessed on 25 June 2022).
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Tan, P.; Yeoh, K.G. Genetics and Molecular Pathogenesis of Gastric Adenocarcinoma. Gastroenterology 2015, 149, 1153–1162.e1153. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Gastric Cancer Version 2. 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf (accessed on 25 June 2022).
- Boltin, D.; Niv, Y. Mucins in Gastric Cancer—An Update. J. Gastrointest. Dig. Syst. 2013, 3, 15519. [Google Scholar] [CrossRef]
- Battista, S.; Ambrosio, M.R.; Limarzi, F.; Gallo, G.; Saragoni, L. Molecular Alterations in Gastric Preneoplastic Lesions and Early Gastric Cancer. Int. J. Mol. Sci. 2021, 22, 6652. [Google Scholar] [CrossRef]
- Gendler, S.J. MUC1, the renaissance molecule. J. Mammary Gland. Biol. Neoplasia 2001, 6, 339–353. [Google Scholar] [CrossRef]
- Nath, S.; Mukherjee, P. MUC1: A multifaceted oncoprotein with a key role in cancer progression. Trends Mol. Med. 2014, 20, 332–342. [Google Scholar] [CrossRef]
- Kufe, D.W. Mucins in cancer: Function, prognosis and therapy. Nat. Rev. Cancer 2009, 9, 874–885. [Google Scholar] [CrossRef]
- MacDermed, D.M.; Khodarev, N.N.; Pitroda, S.P.; Edwards, D.C.; Pelizzari, C.A.; Huang, L.; Kufe, D.W.; Weichselbaum, R.R. MUC1-associated proliferation signature predicts outcomes in lung adenocarcinoma patients. BMC Med. Genom. 2010, 3, 16. [Google Scholar] [CrossRef]
- Khodarev, N.N.; Pitroda, S.P.; Beckett, M.A.; MacDermed, D.M.; Huang, L.; Kufe, D.W.; Weichselbaum, R.R. MUC1-induced transcriptional programs associated with tumorigenesis predict outcome in breast and lung cancer. Cancer Res. 2009, 69, 2833–2837. [Google Scholar] [CrossRef]
- Ohno, T.; Aihara, R.; Kamiyama, Y.; Mochiki, E.; Asao, T.; Kuwano, H. Prognostic significance of combined expression of MUC1 and adhesion molecules in advanced gastric cancer. Eur. J. Cancer 2006, 42, 256–263. [Google Scholar] [CrossRef]
- Wang, J.Y.; Chang, C.T.; Hsieh, J.S.; Lee, L.W.; Huang, T.J.; Chai, C.Y.; Lin, S.R. Role of MUC1 and MUC5AC expressions as prognostic indicators in gastric carcinomas. J. Surg. Oncol. 2003, 83, 253–260. [Google Scholar] [CrossRef]
- Lee, H.S.; Lee, H.K.; Kim, H.S.; Yang, H.K.; Kim, Y.I.; Kim, W.H. MUC1, MUC2, MUC5AC, and MUC6 expressions in gastric carcinomas: Their roles as prognostic indicators. Cancer 2001, 92, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Draganov, P.P.; Wang, A.Y.; Othman, M.O.; Fukami, N. AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States. Clin. Gastroenterol. Hepatol. 2019, 17, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Durães, C.; Almeida, G.M.; Seruca, R.; Oliveira, C.; Carneiro, F. Biomarkers for gastric cancer: Prognostic, predictive or targets of therapy? Virchows Arch. 2014, 464, 367–378. [Google Scholar] [CrossRef]
- Wang, X.T.; Kong, F.B.; Mai, W.; Li, L.; Pang, L.M. MUC1 Immunohistochemical Expression as a Prognostic Factor in Gastric Cancer: Meta-Analysis. Dis. Markers 2016, 2016, 9421571. [Google Scholar] [CrossRef]
- Shimada, H.; Noie, T.; Ohashi, M.; Oba, K.; Takahashi, Y. Clinical significance of serum tumor markers for gastric cancer: A systematic review of literature by the Task Force of the Japanese Gastric Cancer Association. Gastric Cancer 2014, 17, 26–33. [Google Scholar] [CrossRef]
- Matsuoka, T.; Yashiro, M. Biomarkers of gastric cancer: Current topics and future perspective. World J. Gastroenterol. 2018, 24, 2818–2832. [Google Scholar] [CrossRef] [PubMed]
- Guideline Committee of the Korean Gastric Cancer Association (KGCA). Korean Practice Guideline for Gastric Cancer 2018: An Evidence-based, Multi-disciplinary Approach. J. Gastric Cancer 2019, 19, 1–48. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef]
- Draganov, P.V.; Aihara, H.; Karasik, M.S.; Ngamruengphong, S.; Aadam, A.A.; Othman, M.O.; Sharma, N.; Grimm, I.S.; Rostom, A.; Elmunzer, B.J.; et al. Endoscopic Submucosal Dissection in North America: A Large Prospective Multicenter Study. Gastroenterology 2021, 160, 2317–2327.e2312. [Google Scholar] [CrossRef] [PubMed]
- Hatta, W.; Gotoda, T.; Oyama, T.; Kawata, N.; Takahashi, A.; Yoshifuku, Y.; Hoteya, S.; Nakagawa, M.; Hirano, M.; Esaki, M.; et al. A Scoring System to Stratify Curability after Endoscopic Submucosal Dissection for Early Gastric Cancer: “eCura system”. Am. J. Gastroenterol. 2017, 112, 874–881. [Google Scholar] [CrossRef]
- Kim, B.S.; Lee, I.; Yook, J.H.; Song, K.; Kim, B.S. Association between the MUC1 rs4072037 Polymorphism and Risk of Gastric Cancer and Clinical Outcomes. J. Gastric Cancer 2020, 20, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Saeki, N.; Saito, A.; Choi, I.J.; Matsuo, K.; Ohnami, S.; Totsuka, H.; Chiku, S.; Kuchiba, A.; Lee, Y.S.; Yoon, K.A.; et al. A functional single nucleotide polymorphism in mucin 1, at chromosome 1q22, determines susceptibility to diffuse-type gastric cancer. Gastroenterology 2011, 140, 892–902. [Google Scholar] [CrossRef]
- Palmer, A.J.; Lochhead, P.; Hold, G.L.; Rabkin, C.S.; Chow, W.H.; Lissowska, J.; Vaughan, T.L.; Berry, S.; Gammon, M.; Risch, H.; et al. Genetic variation in C20orf54, PLCE1 and MUC1 and the risk of upper gastrointestinal cancers in Caucasian populations. Eur. J. Cancer Prev. 2012, 21, 541–544. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total No = 70 | |
|---|---|
| Age (year), median (IQR) | 68 (58–79) |
| Sex, no (%) | |
| Female | 32 (45.7) |
| Male | 38 (54.3) |
| Smoking, no (%) | |
| Never | 31 (44.3) |
| Former | 29 (41.4) |
| Current | 10 (14.3) |
| Alcohol drinking, no (%) | |
| Never | 47 (67.1) |
| Former | 7 (10.0) |
| Current | 16 (22.9) |
| Diabetes mellitus, no (%) | 21 (30.0) |
| H. pylori infection, no (%) | |
| Negative | 36 (51.4) |
| Positive | 9 (12.9) |
| Unknown | 25 (35.7) |
| Body mass index (kg/m2), mean ± SD | 27.5 ± 7.7 |
| Treatment for gastric cancer, no (%) | |
| Endoscopic submucosal dissection | 4 (5.7) |
| Surgery | 66 (94.3) |
| Total No = 70 | |
|---|---|
| Tumor size (cm), mean ± SD | 3.7 ± 2.4 |
| Tumor location, no (%) | |
| Upper third | 38 (54.3) |
| Middle third | 15 (21.4) |
| Lower third | 17 (24.3) |
| Background intestinal metaplasia, * no (%) | |
| Absent | 30 (42.9) |
| Present | 40 (57.1) |
| Lauren classification, no (%) | |
| Intestinal type | 46 (65.7) |
| Diffuse type | 21 (30.0) |
| Mixed type | 3 (4.3) |
| Tumor depth, no (%) | |
| Mucosa | 11 (15.7) |
| Submucosa | 13 (18.6) |
| Proper muscle or deeper | 46 (65.7) |
| Perineural invasion, no (%) | |
| Absent | 44 (62.9) |
| Present | 26 (37.1) |
| Lymphovascular invasion, no (%) | |
| Absent | 33 (47.1) |
| Present | 37 (52.9) |
| Lymph node metastasis, no (%) | |
| Absent | 35 (50.0) |
| Present | 35 (50.0) |
| Distant metastasis, no (%) | |
| Absent | 53 (75.7) |
| Present | 17 (24.3) |
| AJCC TNM stage, ** no (%) | |
| Stage I | 24 (34.3) |
| Stage II | 16 (22.9) |
| Stage III | 13 (18.6) |
| Stage IV | 17 (32.0) |
| MUC expression, no/total no. (%) | |
| MUC1 | 50/70 (71.4) |
| MUC2 | 55/70 (78.6) |
| MUC5AC | 52/69 (75.4) |
| MUC6 | 23/69 (33.3) |
| MUC1 | p | ||
|---|---|---|---|
| Negative | Positive | ||
| (No = 20) | (No = 50) | ||
| Tumor size (cm), mean ± SD | 3.1 ± 1.9 | 3.9 ± 2.5 | 0.171 |
| Tumor location, no (%) | 0.495 | ||
| Upper third | 5 (25.0) | 12 (24.0) | |
| Middle third | 6 (30.0) | 9 (18.0) | |
| Lower third | 9 (45.0) | 29 (58.0) | |
| Background intestinal metaplasia, no (%) | 0.015 | ||
| Absent | 4 (20.0) | 26 (52.0) | |
| Present | 16 (80.0) | 24 (48.0) | |
| Lauren classification, no (%) | <0.001 | ||
| Intestinal type | 20 (100) | 26 (52.0) | |
| Diffuse type | 0 (0) | 21 (42.0) | |
| Mixed type | 0 (0) | 3 (6.0) | |
| Tumor depth, no (%) | <0.001 | ||
| Mucosa | 8 (40.0) | 3 (6.0) | |
| Submucosa | 6 (30.0) | 7 (14.0) | |
| Proper muscle or deeper | 6 (30.0) | 40 (80.0) | |
| Perineural invasion, no (%) | 0.027 | ||
| Absent | 17 (85.0) | 27 (54.0) | |
| Present | 3 (15.0) | 23 (46.0) | |
| Lymphovascular invasion, no (%) | 0.015 | ||
| Absent | 14 (70.0) | 19 (38.0) | |
| Present | 6 (30.0) | 31 (62.0) | |
| Lymph node metastasis, no (%) | 0.001 | ||
| Absent | 16 (80.0) | 19 (38.0) | |
| Present | 4 (20.0) | 31 (62.0) | |
| Distant metastasis, no (%) | 0.017 | ||
| Absent | 19 (95.0) | 34 (68.0) | |
| Present | 1 (5.0) | 16 (32.0) | |
| AJCC TNM stage, * no (%) | <0.001 | ||
| Stage I | 14 (70.0) | 10 (20.0) | |
| Stage II | 4 (20.0) | 12 (24.0) | |
| Stage III | 1 (5.0) | 12 (24.0) | |
| Stage IV | 1 (5.0) | 16 (32.0) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-I.; Pecha, R.L.; Keihanian, T.; Mercado, M.; Pena-Munoz, S.V.; Lang, K.; Van Buren, G.; Dhingra, S.; Othman, M.O. MUC1 Expressions and Its Prognostic Values in US Gastric Cancer Patients. Cancers 2023, 15, 998. https://doi.org/10.3390/cancers15040998
Kim Y-I, Pecha RL, Keihanian T, Mercado M, Pena-Munoz SV, Lang K, Van Buren G, Dhingra S, Othman MO. MUC1 Expressions and Its Prognostic Values in US Gastric Cancer Patients. Cancers. 2023; 15(4):998. https://doi.org/10.3390/cancers15040998
Chicago/Turabian StyleKim, Young-Il, Robert Luke Pecha, Tara Keihanian, Michael Mercado, S. Valeria Pena-Munoz, Kailash Lang, George Van Buren, Sadhna Dhingra, and Mohamed O. Othman. 2023. "MUC1 Expressions and Its Prognostic Values in US Gastric Cancer Patients" Cancers 15, no. 4: 998. https://doi.org/10.3390/cancers15040998
APA StyleKim, Y.-I., Pecha, R. L., Keihanian, T., Mercado, M., Pena-Munoz, S. V., Lang, K., Van Buren, G., Dhingra, S., & Othman, M. O. (2023). MUC1 Expressions and Its Prognostic Values in US Gastric Cancer Patients. Cancers, 15(4), 998. https://doi.org/10.3390/cancers15040998