
Machine Learning to Predict the Response to Lenvatinib Combined with Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
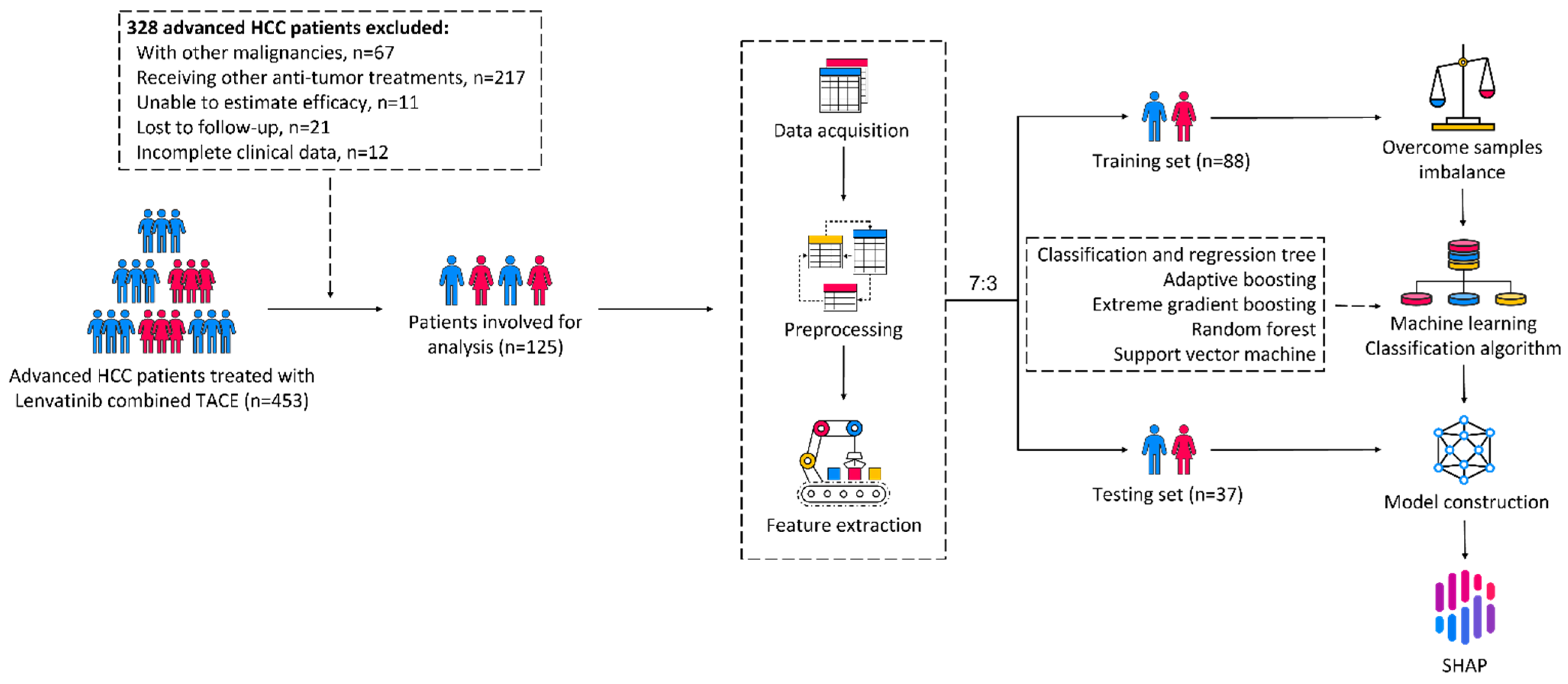
2.1. Study Population
2.2. Treatment Protocol and Response Evaluation
2.3. Data Acquisition, Preprocessing, and Feature Extraction
2.4. Machine Learning Approach
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Treatment Response
3.2. Predictive Performance of the Machine Learning
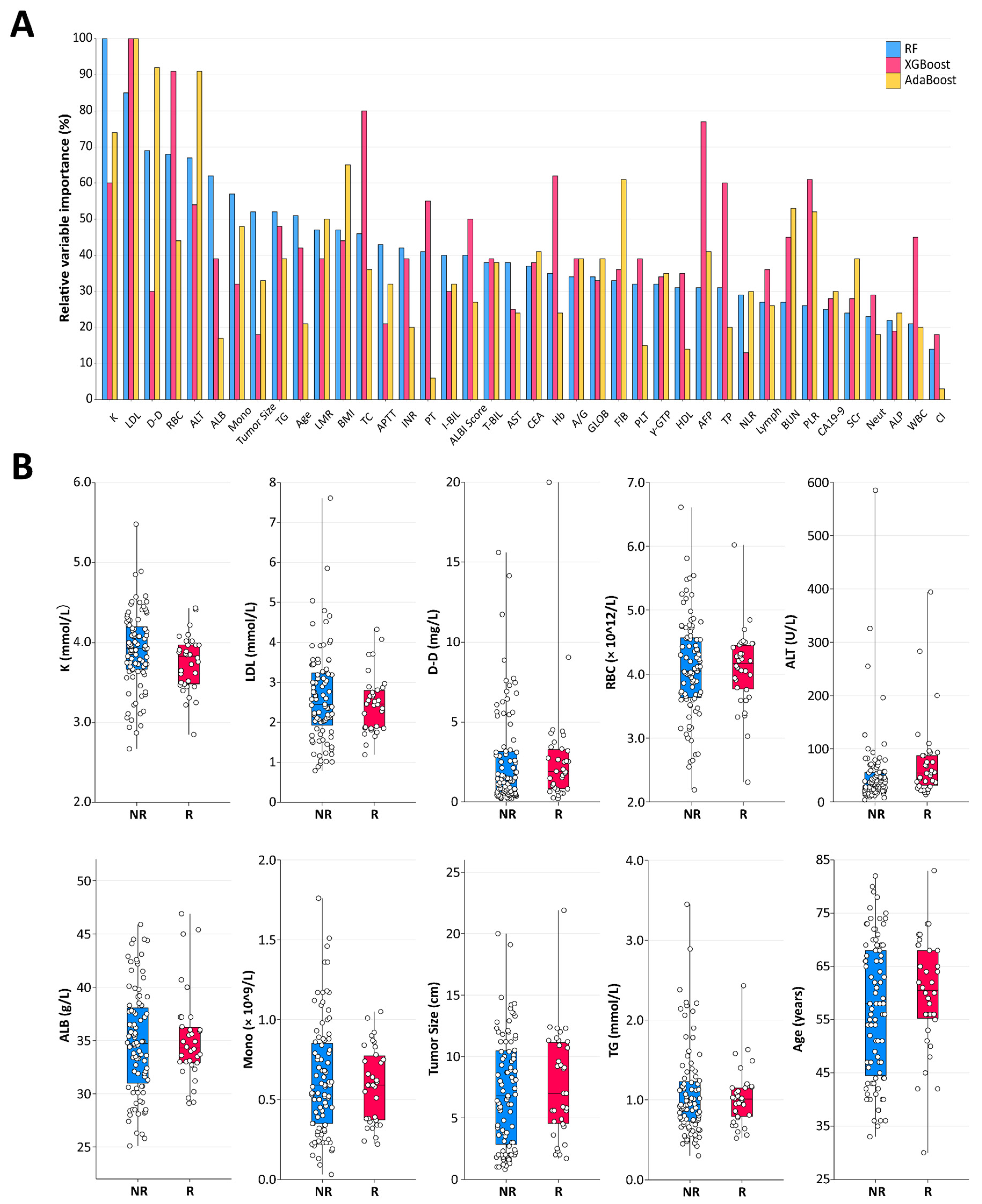
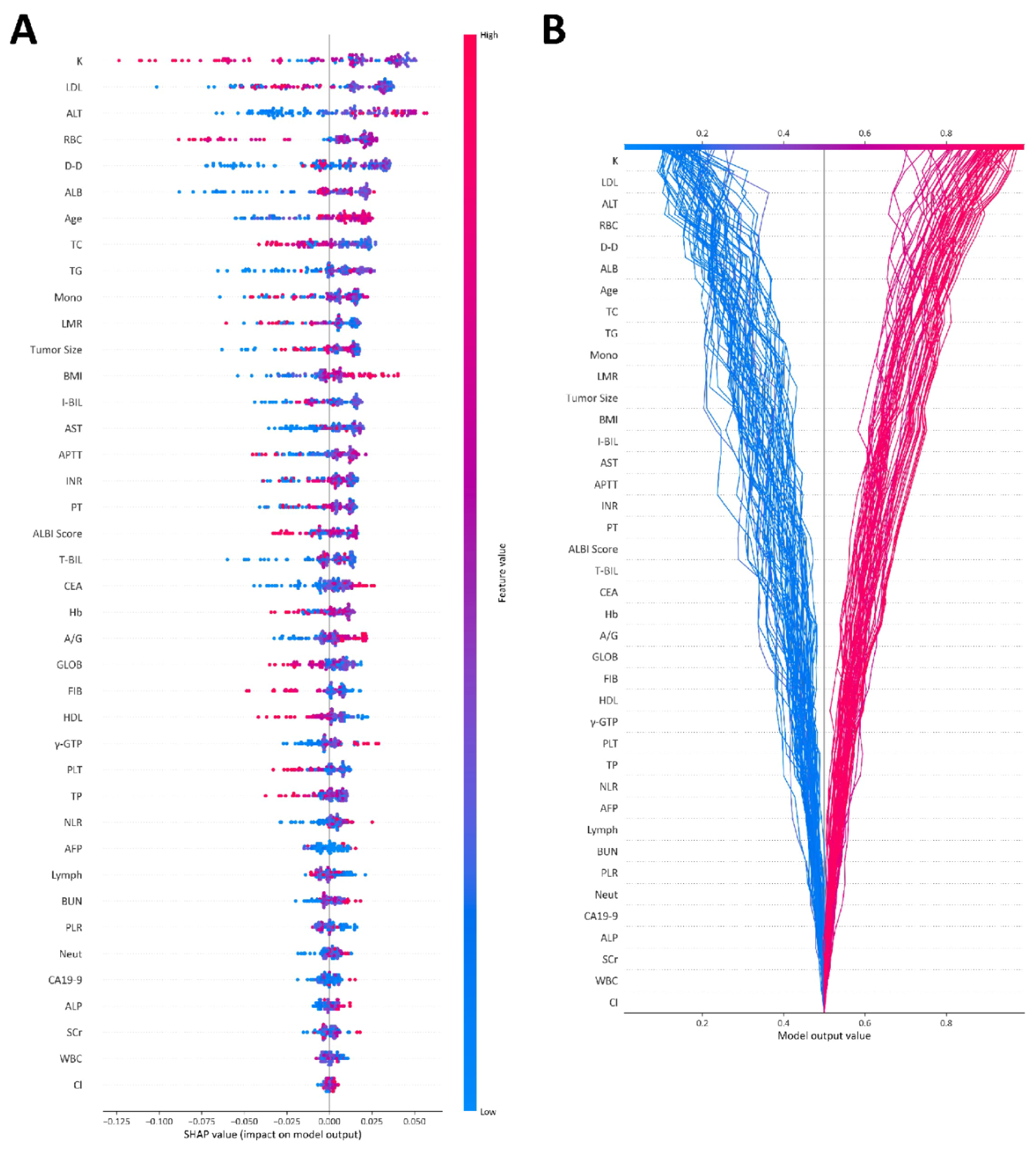
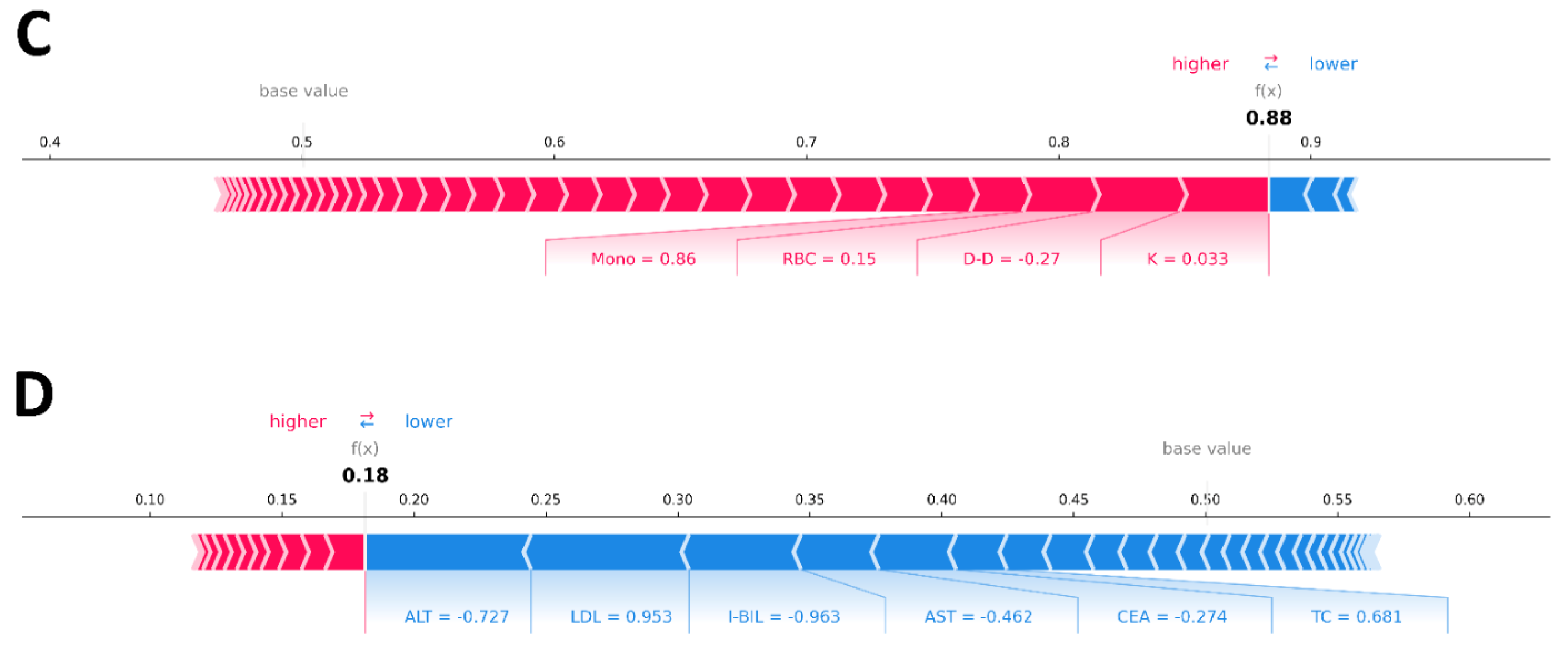
3.3. Explainability of the Machine Learning Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.F.; Beal, E.W.; Bagante, F.; Chakedis, J.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; et al. Early versus late recurrence of intrahepatic cholangiocarcinoma after resection with curative intent. Br. J. Surg. 2018, 105, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Gingold, J.A.; Zhu, D.; Lee, D.F.; Kaseb, A.; Chen, J. Genomic Profiling and Metabolic Homeostasis in Primary Liver Cancers. Trends Mol. Med. 2018, 24, 395–411. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Viatour, P. Hepatocellular carcinoma: Old friends and new tricks. Exp. Mol. Med. 2020, 52, 1898–1907. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.J.; von Felden, J.; Garcia-Lezana, T.; Sarcognato, S.; Villanueva, A. Tumour evolution in hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 139–152. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, Y.N.; Wang, K.T.; Chen, L. Lenvatinib for hepatocellular carcinoma: From preclinical mechanisms to anti-cancer therapy. Biochim. Biophys. Acta Rev. Cancer 2020, 1874, 188391. [Google Scholar] [CrossRef]
- Al-Salama, Z.T.; Syed, Y.Y.; Scott, L.J. Lenvatinib: A Review in Hepatocellular Carcinoma. Drugs 2019, 79, 665–674. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Fu, Z.; Li, X.; Zhong, J.; Chen, X.; Cao, K.; Ding, N.; Liu, L.; Zhang, X.; Zhai, J.; Qu, Z. Lenvatinib in combination with transarterial chemoembolization for treatment of unresectable hepatocellular carcinoma (uHCC): A retrospective controlled study. Hepatol. Int. 2021, 15, 663–675. [Google Scholar] [CrossRef]
- Lencioni, R.; de Baere, T.; Soulen, M.C.; Rilling, W.S.; Geschwind, J.F. Lipiodol transarterial chemoembolization for hepatocellular carcinoma: A systematic review of efficacy and safety data. Hepatology 2016, 64, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Raoul, J.L.; Forner, A.; Bolondi, L.; Cheung, T.T.; Kloeckner, R.; de Baere, T. Updated use of TACE for hepatocellular carcinoma treatment: How and when to use it based on clinical evidence. Cancer Treat. Rev. 2019, 72, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Sun, W.; Li, W.; Shen, Y.; Guo, X.; Teng, Y.; Liu, X.; Zheng, L.; Li, W.; Chen, J. Transarterial chemoembolization plus lenvatinib versus transarterial chemoembolization plus sorafenib as first-line treatment for hepatocellular carcinoma with portal vein tumor thrombus: A prospective randomized study. Cancer 2021, 127, 3782–3793. [Google Scholar] [CrossRef]
- Handelman, G.S.; Kok, H.K.; Chandra, R.V.; Razavi, A.H.; Lee, M.J.; Asadi, H. eDoctor: Machine learning and the future of medicine. J. Intern. Med. 2018, 284, 603–619. [Google Scholar] [CrossRef]
- Ngiam, K.Y.; Khor, I.W. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef]
- Saberi-Karimian, M.; Khorasanchi, Z.; Ghazizadeh, H.; Tayefi, M.; Saffar, S.; Ferns, G.A.; Ghayour-Mobarhan, M. Potential value and impact of data mining and machine learning in clinical diagnostics. Crit. Rev. Clin. Lab. Sci. 2021, 58, 275–296. [Google Scholar] [CrossRef]
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial intelligence in cancer diagnosis and prognosis: Opportunities and challenges. Cancer Lett. 2020, 471, 61–71. [Google Scholar] [CrossRef]
- Goecks, J.; Jalili, V.; Heiser, L.M.; Gray, J.W. How Machine Learning Will Transform Biomedicine. Cell 2020, 181, 92–101. [Google Scholar] [CrossRef]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef]
- Yang, B.; Jie, L.; Yang, T.; Chen, M.; Gao, Y.; Zhang, T.; Zhang, Y.; Wu, H.; Liao, Z. TACE Plus Lenvatinib Versus TACE Plus Sorafenib for Unresectable Hepatocellular Carcinoma With Portal Vein Tumor Thrombus: A Prospective Cohort Study. Front. Oncol. 2021, 11, 821599. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Lencioni, R. mRECIST for HCC: Performance and novel refinements. J. Hepatol. 2020, 72, 288–306. [Google Scholar] [CrossRef] [PubMed]
- Hao, M.; Wang, Y.; Bryant, S.H. An efficient algorithm coupled with synthetic minority over-sampling technique to classify imbalanced PubChem BioAssay data. Anal. Chim. Acta 2014, 806, 117–127. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Erion, G.; Chen, H.; DeGrave, A.; Prutkin, J.M.; Nair, B.; Katz, R.; Himmelfarb, J.; Bansal, N.; Lee, S.I. From Local Explanations to Global Understanding with Explainable AI for Trees. Nat. Mach. Intell. 2020, 2, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.C.; Connell, A.; Simonetto, D.A.; Hughes, C.; Shah, V.H. Application of Artificial Intelligence for the Diagnosis and Treatment of Liver Diseases. Hepatology 2021, 73, 2546–2563. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. A New Treatment Option for Intermediate-Stage Hepatocellular Carcinoma with High Tumor Burden: Initial Lenvatinib Therapy with Subsequent Selective TACE. Liver Cancer 2019, 8, 299–311. [Google Scholar] [CrossRef]
- Kawamura, Y.; Kobayashi, M.; Shindoh, J.; Kobayashi, Y.; Okubo, S.; Tominaga, L.; Kajiwara, A.; Kasuya, K.; Iritani, S.; Fujiyama, S.; et al. Lenvatinib-Transarterial Chemoembolization Sequential Therapy as an Effective Treatment at Progression during Lenvatinib Therapy for Advanced Hepatocellular Carcinoma. Liver Cancer 2020, 9, 756–770. [Google Scholar] [CrossRef]
- Shimose, S.; Iwamoto, H.; Tanaka, M.; Niizeki, T.; Shirono, T.; Noda, Y.; Kamachi, N.; Okamura, S.; Nakano, M.; Suga, H.; et al. Alternating Lenvatinib and Trans-Arterial Therapy Prolongs Overall Survival in Patients with Inter-Mediate Stage HepatoCellular Carcinoma: A Propensity Score Matching Study. Cancers 2021, 13, 160. [Google Scholar] [CrossRef]
- Peng, Z.; Fan, W.; Zhu, B.; Wang, G.; Sun, J.; Xiao, C.; Huang, F.; Tang, R.; Cheng, Y.; Huang, Z.; et al. Lenvatinib Combined With Transarterial Chemoembolization as First-Line Treatment for Advanced Hepatocellular Carcinoma: A Phase III, Randomized Clinical Trial (LAUNCH). J. Clin. Oncol. 2022, 41, 117–127. [Google Scholar] [CrossRef]
- Feng, G.S.; Hanley, K.L.; Liang, Y.; Lin, X. Improving the Efficacy of Liver Cancer Immunotherapy: The Power of Combined Preclinical and Clinical Studies. Hepatology 2021, 73 (Suppl. S1), 104–114. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Friedman, S.L.; Goossens, N.; Hoshida, Y. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J. Hepatol. 2018, 68, 526–549. [Google Scholar] [CrossRef] [PubMed]
- Kariyama, K.; Hiraoka, A.; Kumada, T.; Yasuda, S.; Toyoda, H.; Tsuji, K.; Hatanaka, T.; Kakizaki, S.; Naganuma, A.; Tada, T.; et al. Chronological change in serum albumin as a prognostic factor in patients with hepatocellular carcinoma treated with lenvatinib: Proposal of albumin simplified grading based on the modified albumin-bilirubin score (ALBS grade). J. Gastroenterol. 2022, 57, 581–586. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Hiraoka, A.; Michitaka, K.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; et al. Neutrophil-to-lymphocyte ratio is associated with survival in patients with unresectable hepatocellular carcinoma treated with lenvatinib. Liver Int. 2020, 40, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Saeki, I.; Yamasaki, T.; Yamashita, S.; Hanazono, T.; Urata, Y.; Furutani, T.; Yokoyama, Y.; Oishi, T.; Maeda, M.; Kimura, T.; et al. Early Predictors of Objective Response in Patients with Hepatocellular Carcinoma Undergoing Lenvatinib Treatment. Cancers 2020, 12, 779. [Google Scholar] [CrossRef]
- Tada, T.; Kumada, T.; Hiraoka, A.; Michitaka, K.; Atsukawa, M.; Hirooka, M.; Tsuji, K.; Ishikawa, T.; Takaguchi, K.; Kariyama, K.; et al. Platelet-lymphocyte ratio predicts survival in patients with hepatocellular carcinoma who receive lenvatinib: An inverse probability weighting analysis. Eur. J. Gastroenterol. Hepatol. 2021, 32, 261–268. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 125) | Training Set (n = 88) | Testing Set (n = 37) | p-Value | |
|---|---|---|---|---|
| Demographic Characteristics | ||||
| Age, median (IQR), y | 58.0 (47.0, 68.0) | 58.0 (46.3, 69.0) | 59.0 (47.5, 67.5) | 0.963 |
| Gender | 0.890 | |||
| Male, n (%) | 109 (87.2) | 77 (87.5) | 32 (86.5) | |
| Female, n (%) | 16 (12.8) | 11 (12.5) | 5 (13.5) | |
| BMI, mean ± SD, kg/m2 | 22.0 ± 2.8 | 22.1 ± 2.6 | 21.8 ± 3.1 | 0.577 |
| Smoking History | 0.858 | |||
| Yes, n (%) | 42 (33.6) | 30 (34.1) | 12 (32.4) | |
| No, n (%) | 83 (66.4) | 58 (65.9) | 25 (67.6) | |
| Drinking History | 0.689 | |||
| Yes, n (%) | 44 (35.2) | 30 (34.1) | 14 (37.8) | |
| No, n (%) | 81 (64.8) | 58 (65.9) | 23 (62.2) | |
| HBV Infection History | 0.239 | |||
| Yes, n (%) | 78 (62.4) | 52 (59.1) | 26 (70.1) | |
| No, n (%) | 47 (37.6) | 36 (40.9) | 11 (29.9) | |
| HCV Infection History | ||||
| Yes, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| No, n (%) | 125 (100.0) | 88 (100.0) | 37 (100.0) | |
| Hypertensive History | 0.683 | |||
| Yes, n (%) | 37 (29.6) | 27 (30.7) | 10 (27.0) | |
| No, n (%) | 88 (70.4) | 61 (69.3) | 27 (73.0) | |
| Diabetes History | 0.351 | |||
| Yes, n (%) | 18 (14.4) | 11 (12.5) | 7 (18.9) | |
| No, n (%) | 107 (85.6) | 77 (87.5) | 30 (81.1) | |
| Heart Disease history | 0.613 | |||
| Yes, n (%) | 2 (1.6) | 2 (2.3) | 0 (0.0) | |
| No, n (%) | 123 (98.4) | 86 (97.7) | 37 (100.0) | |
| NAFLD History | ||||
| Yes, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| No, n (%) | 125 (100.0) | 88 (100.0) | 37 (100.0) | |
| Cirrhosis, n (%) | 0.623 | |||
| Yes, n (%) | 105 (84.0) | 73 (83.0) | 32 (86.5) | |
| No, n (%) | 20 (16.0) | 15 (17.0) | 5 (13.5) | |
| ECOG-PS | 0.547 | |||
| Grade 0, n (%) | 66 (52.8) | 48 (54.5) | 18 (48.6) | |
| Grade 1, n (%) | 59 (47.2) | 40 (45.5) | 19 (51.4) | |
| Pretreatment Serum Biomarkers | ||||
| RBC, median (IQR), 1012/L | 4.1 (3.7, 4.5) | 4.2 (3.7, 4.5) | 3.9 (3.5, 4.3) | 0.048 |
| WBC, median (IQR), 109/L | 6.3 (4.9, 8.0) | 6.2 (5.1, 8.0) | 6.5 (4.6, 7.9) | 0.867 |
| Neut, median (IQR), 109/L | 4.1 (2.9, 6.0) | 4.2 (3.0, 5.9) | 3.8 (2.4, 6.1) | 0.400 |
| Mono, median (IQR), 109/L | 0.6 (0.4, 0.8) | 0.6 (0.3, 0.8) | 0.6 (0.4, 0.9) | 0.273 |
| Lymph, median (IQR), 109/L | 1.1 (0.8,1.7) | 1.1 (0.8, 1.6) | 1.2 (0.8, 1.8) | 0.253 |
| Hb, mean ± SD, g/L | 123.0 ± 22.7 | 124.3 ± 22.7 | 119.9 ± 22.4 | 0.322 |
| PLT, median (IQR), 109/L | 167.0 (112.5, 252.0) | 160.0 (109.3, 245.0) | 180.0 (127.5, 271.5) | 0.184 |
| PLR, median (IQR) | 138.3 (101.4, 219.3) | 136.2 (96.4, 230.7) | 140.4 (108.3, 214.2) | 0.735 |
| NLR, median (IQR) | 3.7 (1.9, 5.9) | 4.3 (2.0, 6.4) | 3.0 (1.9, 4.2) | 0.136 |
| LMR, median (IQR) | 2.0 (1.3, 3.6) | 2.0 (1.3, 3.8) | 1.8 (1.3, 3.5) | 0.756 |
| PT, median (IQR), s | 14.5 (13.6, 15.5) | 14.4 (13.5, 15.4) | 14.7 (14.1, 16.1) | 0.101 |
| FIB, median (IQR), g/L | 3.8 (2.9, 5.2) | 3.8 (2.9, 5.2) | 4.1 (3.0, 5.3) | 0.766 |
| APTT, median (IQR), s | 39.3 (36.3, 44.0) | 38.6 (36.2, 41.9) | 41.7 (36.9, 48.5) | 0.040 |
| TT, median (IQR), s | 17.3 (16.2, 18.4) | 17.4 (16.2, 18.4) | 16.9 (15.8, 18.5) | 0.381 |
| INR, median (IQR) | 1.1 (1.0, 1.2) | 1.1 (1.0, 1.2) | 1.1 (1.1, 1.2) | 0.101 |
| D-D, median (IQR), mg/L | 1.5 (0.7, 3.2) | 1.3 (0.6, 3.2) | 2.1 (0.8, 4.4) | 0.072 |
| AFP, median (IQR), ng/mL | 161.4 (5.5, 3326.5) | 113.2 (4.3, 2991.3) | 277.7 (17.0, 3575.5) | 0.318 |
| CEA, median (IQR), μg/L | 2.4 (1.6, 3.6) | 2.4 (1.4,3.4) | 2.6 (2.3, 4.1) | 0.056 |
| CA19-9, median (IQR), U/mL | 19.9 (10.5, 41.9) | 19.9 (9.7, 39.9) | 19.9 (13.0, 32.0) | 0.083 |
| T-BIL, median (IQR), μmol/L | 17.0 (11.5, 25.5) | 15.5 (11.0,25.0) | 19.0 (13.0, 32.0) | 0.191 |
| D-BIL, median (IQR), μmol/L | 8.0 (5.5, 13.0) | 7.0 (5.0, 12.0) | 10.0 (6.0, 16.0) | 0.029 |
| I-BIL, median (IQR), μmol/L | 8.0 (6.0, 12.0) | 8.0 (6.0, 12.0) | 8.0 (6.0, 12.5) | 0.766 |
| TP, mean ± SD, g/L | 69.9 ± 8.4 | 69.4 ± 8.2 | 71.1 ± 8.6 | 0.300 |
| ALB, median (IQR), g/L | 34.6 (31.9, 37.6) | 34.6 (32.1, 38.9) | 34.7 (29.7, 36.3) | 0.188 |
| GLOB, median (IQR), g/L | 34.1 (29.4, 38.7) | 33.4 (29.4, 37.5) | 36.8 (29.3, 42.8) | 0.045 |
| A/G, mean ± SD | 1.0 ± 0.3 | 1.1 ± 0.3 | 1.0 ± 0.2 | 0.011 |
| ALT, median (IQR), U/L | 39.0 (25.0, 68.0) | 38.5 (24.3, 63.5) | 40.0 (27.0, 68.5) | 0.918 |
| AST, median (IQR), U/L | 57.0 (39.0, 93.0) | 56.0 (35.5, 90.5) | 59.0 (41.5, 97.5) | 0.496 |
| ALP, median (IQR), U/L | 182.0 (115.0, 233.5) | 165.5 (112.5, 210.0) | 210.0 (124.0, 272.0) | 0.068 |
| γ-GTP, median (IQR), U/L | 182.0 (74.5, 257.5) | 163.0 (61.3,247.5) | 193.0 (103.5, 315.0) | 0.232 |
| BUN, median (IQR), mmol/L | 5.1 (3.8, 6.4) | 5.2 (3.8, 6.5) | 5.0 (3.8, 5.8) | 0.465 |
| SCr, median (IQR), μmol/L | 68.0 (56.5, 78.0) | 67.0 (57.0, 80.3) | 69.0 (55.0, 77.5) | 0.762 |
| K, mean ± SD, mmol/L | 3.9 ± 0.5 | 3.8 ± 0.5 | 4.0 ± 0.4 | 0.154 |
| Na, median (IQR), mmol/L | 137.0 (135.0, 139.0) | 137.0 (135.0, 139.0) | 136.0 (133.5, 138.5) | 0.052 |
| Cl, median (IQR), mmol/L | 102.0 (99.5, 105.0) | 103.0 (100.0, 105.0) | 101.0 (99.0, 104.0) | 0.066 |
| TC, median (IQR), mmol/L | 4.3 (3.4, 5.0) | 4.3 (3.5, 5.0) | 4.2 (3.3, 5.0) | 0.869 |
| TG, median (IQR), mmol/L | 1.0 (0.7, 1.2) | 1.0 (0.7, 1.2) | 0.9 (0.8, 1.4) | 0.534 |
| HDL, mean ± SD, mmol/L | 0.9 ± 0.3 | 0.9 ± 0.3 | 0.8 ± 0.3 | 0.105 |
| LDL, median (IQR), mmol/L | 2.5 (1.9,3.2) | 2.5 (1.8, 3.2) | 2.4 (1.9, 3.2) | 0.920 |
| Tumor Characteristics | ||||
| ALBI Score, mean ± SD | −2.1 ± 0.5 | −2.2 ± 0.5 | −2.0 ± 0.4 | 0.053 |
| Child–Pugh Score | 0.493 | |||
| A (5–6 scores), n (%) | 80 (64.0) | 58 (65.9) | 22 (59.5) | |
| B (7 scores), n (%) | 45 (36.0) | 30 (34.1) | 15 (40.5) | |
| T Stage | 0.415 | |||
| T1a, n (%) | 4 (3.2) | 4 (4.5) | 0 (0.0) | |
| T1b, n (%) | 10 (8.0) | 7 (8.0) | 3 (8.1) | |
| T2, n (%) | 28 (22.4) | 19 (21.6) | 9 (24.3) | |
| T3, n (%) | 40 (32.0) | 31 (35.2) | 9 (24.3) | |
| T4, n (%) | 43 (34.4) | 27 (30.7) | 16 (43.3) | |
| N Stage | 0.842 | |||
| N0, n (%) | 76 (60.8) | 54 (61.4) | 22 (59.5) | |
| N1, n (%) | 49 (39.2) | 34 (38.6) | 15 (40.5) | |
| M Stage | 0.351 | |||
| M0, n (%) | 107 (85.6) | 77 (87.5) | 30 (81.1) | |
| M1, n (%) | 18 (14.4) | 11 (12.5) | 7 (18.9) | |
| TNM Stage | 0.467 | |||
| IA, n (%) | 2 (1.6) | 2 (2.3) | 0 (0.0) | |
| IB, n (%) | 9 (7.2) | 7 (8.0) | 2 (5.4) | |
| II, n (%) | 17 (13.6) | 9 (10.2) | 8 (21.6) | |
| IIIA, n (%) | 21 16.8) | 17 (19.3) | 4 (10.8) | |
| IIIB, n (%) | 13 (10.4) | 9 (10.2) | 4 (10.8) | |
| IVA, n (%) | 45 (36.0) | 33 (37.5) | 12 (32.4) | |
| IVB, n (%) | 18 (14.4) | 11 (12.5) | 7 (18.9) | |
| BCLC Stage | 0.584 | |||
| A, n (%) | 12 (9.6) | 10 (11.4) | 2 (5.4) | |
| B, n (%) | 38 (30.4) | 26 (29.5) | 12 (32.4) | |
| C, n (%) | 75 (60.0) | 52 (59.1) | 23 (62.2) | |
| Tumor Size, median (IQR), mm | 6.9 (3.1, 11.1) | 6.7 (2.9, 11.2) | 7.0 (3.7, 9.9) | 0.920 |
| Tumor Number | 0.361 | |||
| Solitary, n (%) | 23 (18.4) | 18 (20.5) | 5 (13.5) | |
| Multiple, n (%) | 102 (81.6) | 70 (79.5) | 32 (86.5) | |
| Vascular Invasion, n (%) | 0.177 | |||
| Yes, n (%) | 43 (34.4) | 27 (30.7) | 16 (43.2) | |
| No, n (%) | 82 (65.6) | 61 (69.3) | 21 (56.8) | |
| Lymphatic Metastasis, n (%) | 0.523 | |||
| Yes, n (%) | 52 (41.6) | 35 (39.8) | 17 (45.9) | |
| No, n (%) | 73 (58.4) | 53 (60.2) | 20 (54.1) | |
| Distant Metastasis, n (%) | 0.351 | |||
| Yes, n (%) | 18 (14.4) | 11 (12.5) | 7 (18.9) | |
| No, n (%) | 107 (85.6) | 77 (87.5) | 30 (81.1) |
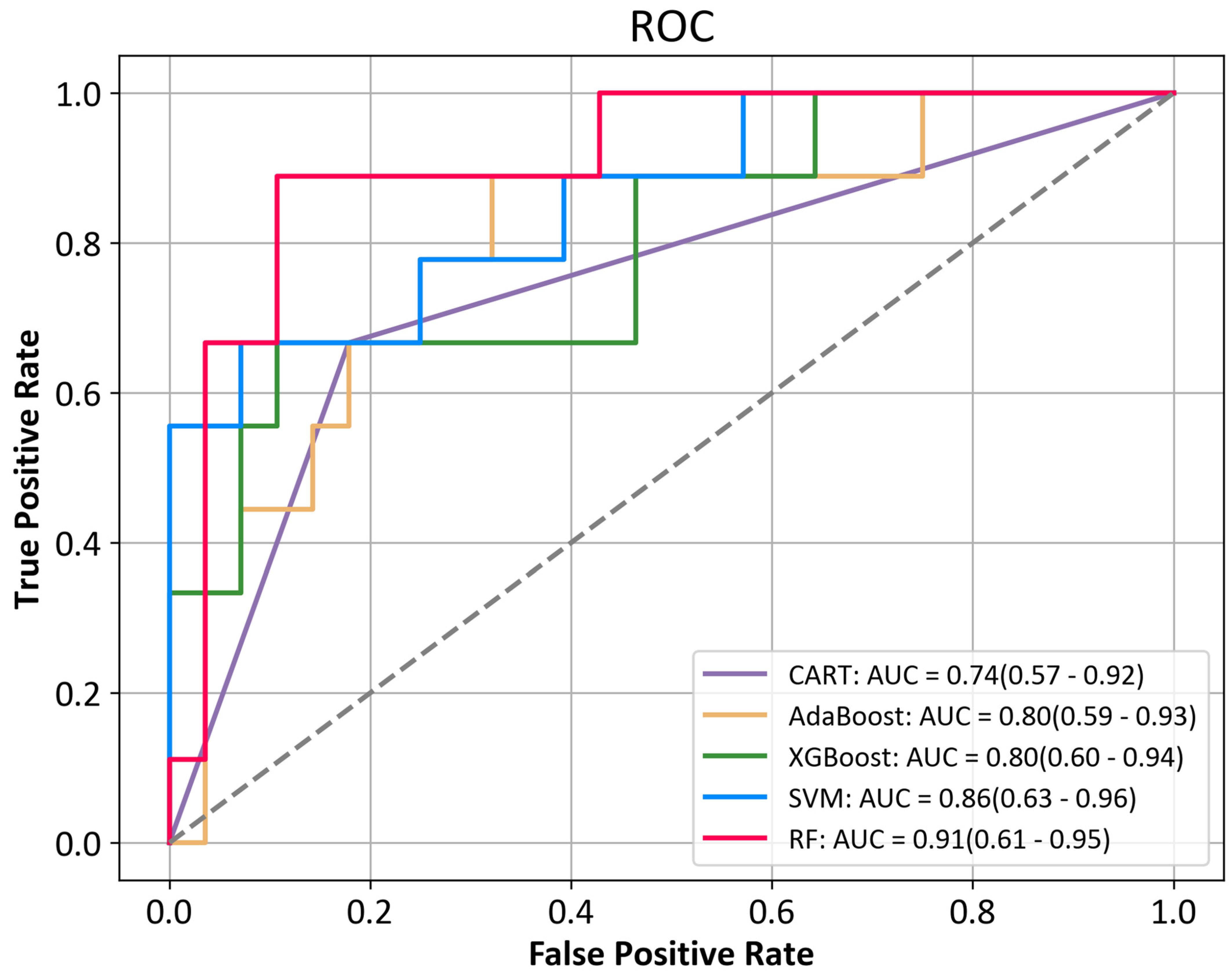
| Classifier | Accuracy | Precision | Recall | F1-Score | Sensitivity | Specificity | PPV | NPV | MCC | AUC (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|
| CART | 78.4% | 54.5% | 66.7% | 60.0% | 66.7% | 82.1% | 54.5% | 88.5% | 0.46 | 0.74 (0.57–0.92) |
| Adaboost | 78.4% | 54.5% | 66.7% | 60.0% | 66.7% | 82.1% | 54.5% | 88.9% | 0.46 | 0.80 (0.59–0.93) |
| XGBoost | 81.1% | 60.0% | 66.7% | 63.2% | 66.7% | 85.7% | 60.0% | 88.9% | 0.51 | 0.80 (0.60–0.94) |
| SVM | 86.5% | 75.0% | 66.7% | 70.6% | 66.7% | 92.9% | 75.0% | 89.7% | 0.62 | 0.86 (0.63–0.96) |
| RF | 86.5% | 75.0% | 66.7% | 70.6% | 66.7% | 92.9% | 75.0% | 89.7% | 0.62 | 0.91 (0.61–0.95) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, J.; Bo, Z.; Zhao, Z.; Yang, J.; Yang, Y.; Li, H.; Yang, Y.; Wang, J.; Su, Q.; Wang, J.; et al. Machine Learning to Predict the Response to Lenvatinib Combined with Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma. Cancers 2023, 15, 625. https://doi.org/10.3390/cancers15030625
Ma J, Bo Z, Zhao Z, Yang J, Yang Y, Li H, Yang Y, Wang J, Su Q, Wang J, et al. Machine Learning to Predict the Response to Lenvatinib Combined with Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma. Cancers. 2023; 15(3):625. https://doi.org/10.3390/cancers15030625
Chicago/Turabian StyleMa, Jun, Zhiyuan Bo, Zhengxiao Zhao, Jinhuan Yang, Yan Yang, Haoqi Li, Yi Yang, Jingxian Wang, Qing Su, Juejin Wang, and et al. 2023. "Machine Learning to Predict the Response to Lenvatinib Combined with Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma" Cancers 15, no. 3: 625. https://doi.org/10.3390/cancers15030625
APA StyleMa, J., Bo, Z., Zhao, Z., Yang, J., Yang, Y., Li, H., Yang, Y., Wang, J., Su, Q., Wang, J., Chen, K., Yu, Z., Wang, Y., & Chen, G. (2023). Machine Learning to Predict the Response to Lenvatinib Combined with Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma. Cancers, 15(3), 625. https://doi.org/10.3390/cancers15030625