

Diagnostic Performance of 99mTc-iPSMA SPECT/CT in the Initial Staging of Patients with Unfavorable Intermediate-, High-, and Very High-Risk Prostate Cancer: A Comparative Analysis with 18F-PSMA-1007 PET/CT

 ,
,  ,
,  ,
,  ,
,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Synthesis of the Tracers
2.3. Imaging Protocol
2.4. Image Interpretation
2.5. Statistical Analysis
3. Results
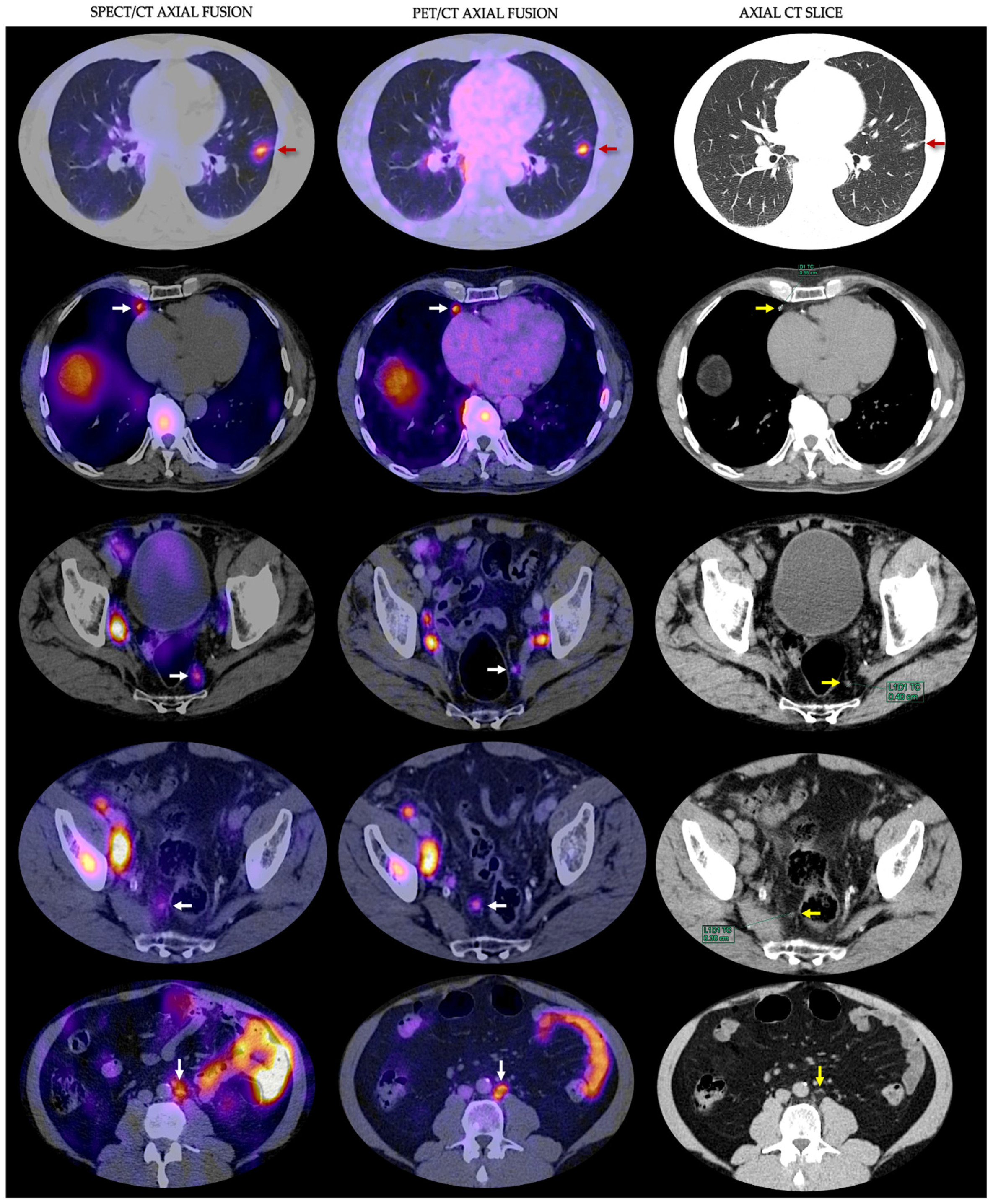
3.1. Detection Rates
3.2. Interobserver Agreement
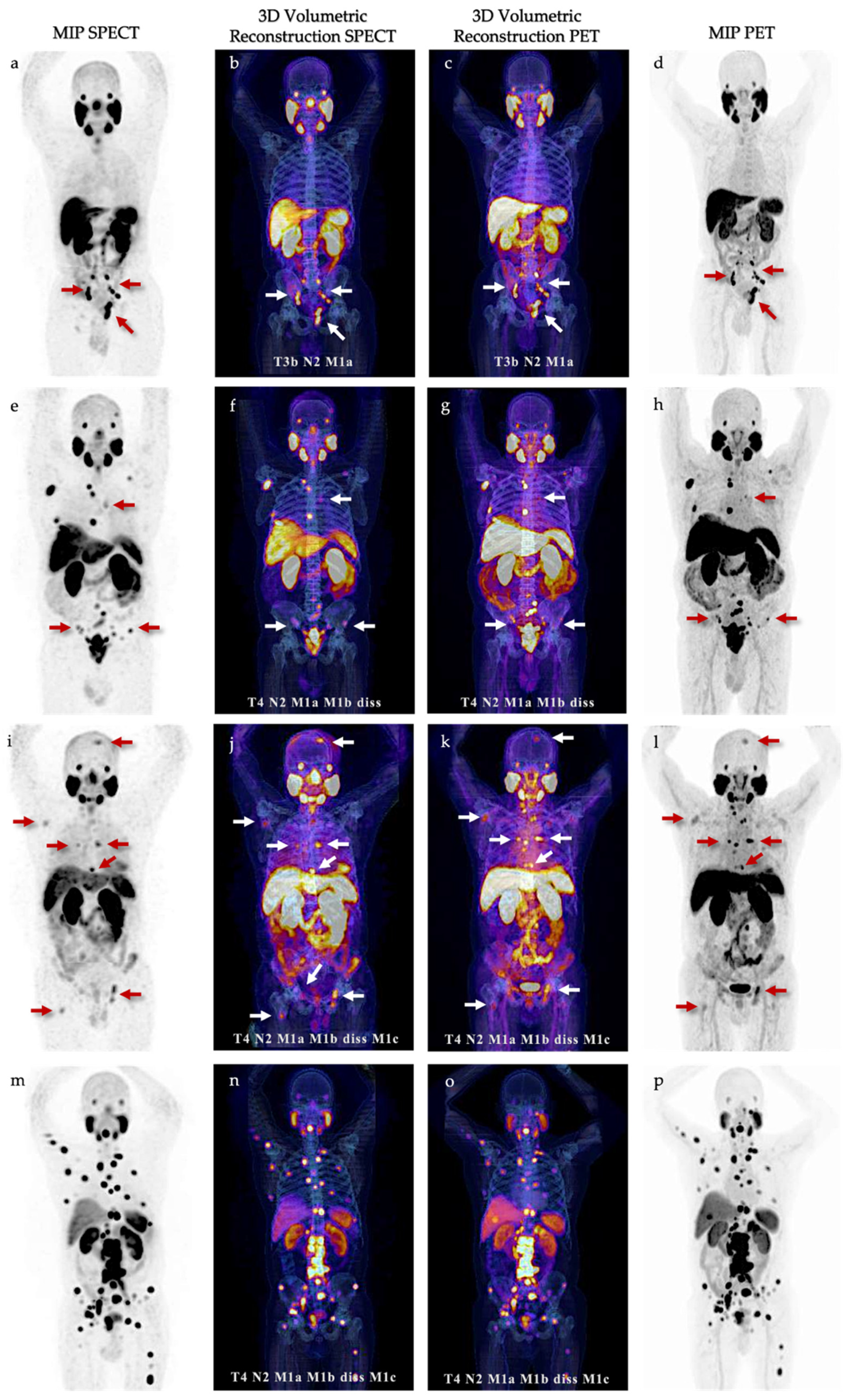
3.3. Volumetric Parameters and mi TNM classification
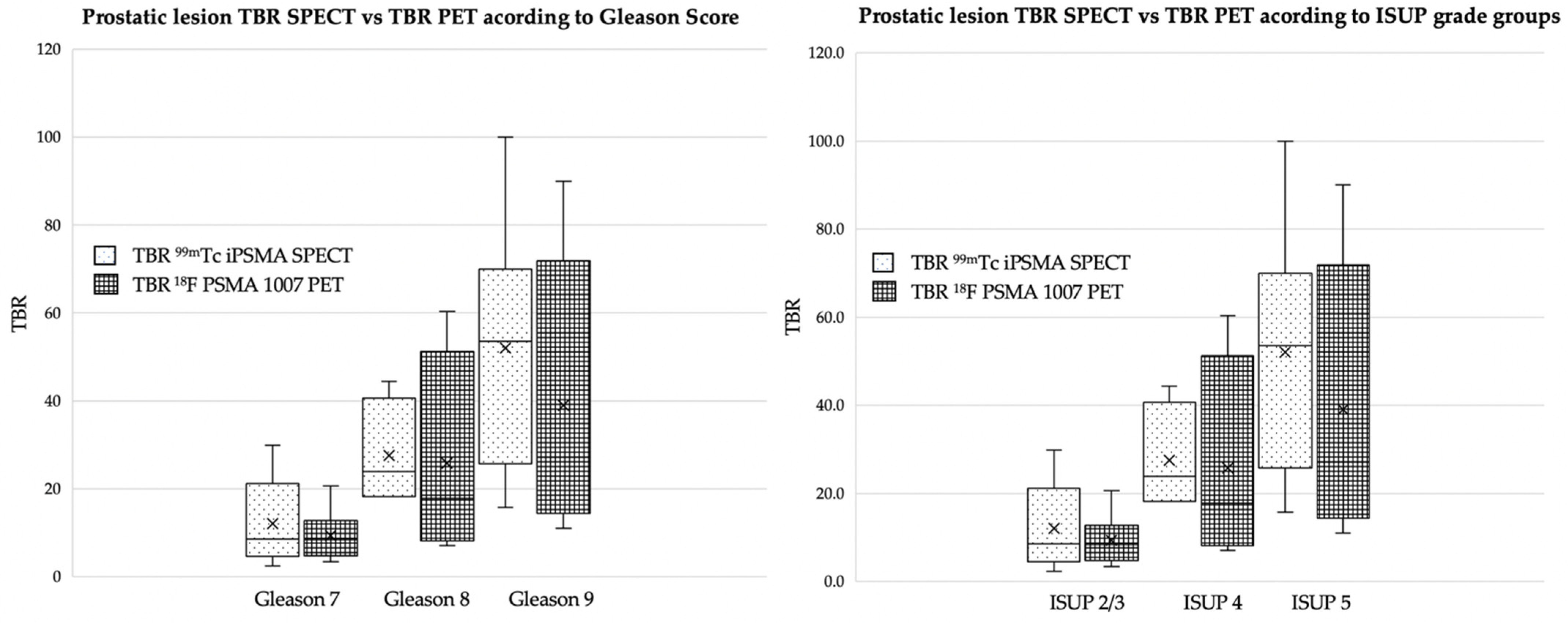
3.4. Quantitative Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Cancer Institute—Surveillance, Epidemiology, and End Results Program (SEER). Cancer Stat Facts: Prostate Cancer. Available online: https://seer.cancer.gov/statfacts/html/prost.html (accessed on 9 October 2023).
- World Health Organization. International Agency for Research on Cancer—GLOBOCAN 2020. Available online: https://gco.iarc.fr/ (accessed on 9 October 2023).
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Litwin, M.S.; Tan, H.J. The Diagnosis and Treatment of Prostate Cancer: A Review. JAMA 2017, 317, 2532–2542. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.B.L.; MacLennan, S.; Willemse, P.M.; Mason, M.D.; Plass, K.; Shepherd, R.; Baanders, R.; Bangma, C.H.; Bjartell, A.; Bossi, A.; et al. EAU-EANM-ESTRO-ESUR-SIOG Prostate Cancer Guideline Panel Consensus Statements for Deferred Treatment with Curative Intent for Localised Prostate Cancer from an International Collaborative Study (DETECTIVE Study). Eur. Urol. 2019, 76, 790–813. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Han, D.; Wu, P.; Ren, J.; Ma, S.; Zhang, J.; Song, W.; Lin, X.; Jiao, D.; Shi, S.; et al. Comparison of 68Ga-PSMA-617 PET/CT with mpMRI for the detection of PCa in patients with a PSA level of 4–20 ng/mL before the initial biopsy. Sci. Rep. 2020, 10, 10963. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Prostate Cancer (Version 4.2023). Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 10 October 2023).
- Ross, J.S.; Sheehan, C.E.; Fisher, H.A.; Kaufman, R.P., Jr.; Kaur, P.; Gray, K.; Webb, I.; Gray, G.S.; Mosher, R.; Kallakury, B.V. Correlation of primary tumor prostate-specific membrane antigen expression with disease recurrence in prostate cancer. Clin. Cancer Res. 2003, 9, 6357–6362. [Google Scholar]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar] [PubMed]
- Paschalis, A.; Sheehan, B.; Riisnaes, R.; Rodrigues, D.N.; Gurel, B.; Bertan, C.; Ferreira, A.; Lambros, M.B.K.; Seed, G.; Yuan, W.; et al. Prostate-specific Membrane Antigen Heterogeneity and DNA Repair Defects in Prostate Cancer. Eur. Urol. 2019, 76, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Hope, T.A.; Eiber, M.; Armstrong, W.R.; Juarez, R.; Murthy, V.; Lawhn-Heath, C.; Behr, S.C.; Zhang, L.; Barbato, F.; Ceci, F.; et al. Diagnostic Accuracy of 68Ga-PSMA-11 PET for Pelvic Nodal Metastasis Detection Prior to Radical Prostatectomy and Pelvic Lymph Node Dissection: A Multicenter Prospective Phase 3 Imaging Trial. JAMA Oncol. 2021, 7, 1635–1642. [Google Scholar] [CrossRef]
- Pienta, K.J.; Gorin, M.A.; Rowe, S.P.; Carroll, P.R.; Pouliot, F.; Probst, S.; Saperstein, L.; Preston, M.A.; Alva, A.S.; Patnaik, A.; et al. A Phase 2/3 Prospective Multicenter Study of the Diagnostic Accuracy of Prostate Specific Membrane Antigen PET/CT with 18F-DCFPyL in Prostate Cancer Patients (OSPREY). J. Urol. 2021, 206, 52–61. [Google Scholar] [CrossRef]
- Fendler, W.P.; Weber, M.; Iravani, A.; Hofman, M.S.; Calais, J.; Czernin, J.; Ilhan, H.; Saad, F.; Small, E.J.; Smith, M.R.; et al. Prostate-Specific Membrane Antigen Ligand Positron Emission Tomography in Men with Nonmetastatic Castration-Resistant Prostate Cancer. Clin. Cancer Res. 2019, 25, 7448–7454. [Google Scholar] [CrossRef]
- Ferro-Flores, G.; Luna-Gutiérrez, M.; Ocampo-García, B.; Santos-Cuevas, C.; Azorín-Vega, E.; Jiménez-Mancilla, N.; Orocio-Rodríguez, E.; Davanzo, J.; García-Pérez, F.O. Clinical translation of a PSMA inhibitor for 99mTc-based SPECT. Nucl. Med. Biol. 2017, 48, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, J.; Xu, X.; Lu, L.; Hu, S.; Liu, C.; Cheng, J.; Song, S.; Zhang, Y.; Shi, L.Q. Evaluation of Radiation dosimetry of 99mTc-HYNIC-PSMA and imaging in prostate cancer. Sci. Rep. 2020, 10, 4179. [Google Scholar] [CrossRef] [PubMed]
- García-Pérez, F.O.; Davanzo, J.; López-Buenrostro, S.; Santos-Cuevas, C.; Ferro-Flores, G.; Jímenez-Ríos, M.A.; Scavuzzo, A.; Santana-Ríos, Z.; Medina-Ornelas, S. Head to head comparison performance of 99mTc-EDDA/HYNIC-iPSMA SPECT/CT and 68Ga-PSMA-11 PET/CT a prospective study in biochemical recurrence prostate cancer patients. Am. J. Nucl. Med. Mol. Imaging 2018, 8, 332–340. [Google Scholar] [PubMed]
- Cardinale, J.; Martin, R.; Remde, Y.; Schäfer, M.; Hienzsch, A.; Hübner, S.; Zerges, A.M.; Marx, H.; Hesse, R.; Weber, K.; et al. Procedures for the GMP-Compliant Production and Quality Control of [18F]PSMA-1007: A Next Generation Radiofluorinated Tracer for the Detection of Prostate Cancer. Pharmaceuticals 2017, 10, 77. [Google Scholar] [CrossRef]
- Maurer, T.; Eiber, M.; Schwaiger, M.; Gschwend, J.E. Current use of PSMA-PET in prostate cancer management. Nature reviews. Urology 2016, 13, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Seifert, R.; Emmett, L.; Rowe, S.P.; Herrmann, K.; Hadaschik, B.; Calais, J.; Giesel, F.L.; Reiter, R.; Maurer, T.; Heck, M.; et al. Second Version of the Prostate Cancer Molecular Imaging Standardized Evaluation Framework Including Response Evaluation for Clinical Trials (PROMISE V2). Eur. Urol. 2023, 83, 405–412. [Google Scholar] [CrossRef]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Maurer, T.; Gschwend, J.E.; Rauscher, I.; Souvatzoglou, M.; Haller, B.; Weirich, G.; Wester, H.J.; Heck, M.; Kübler, H.; Beer, A.J.; et al. Diagnostic Efficacy of (68)Gallium-PSMA Positron Emission Tomography Compared to Conventional Imaging for Lymph Node Staging of 130 Consecutive Patients with Intermediate to High Risk Prostate Cancer. J. Urol. 2016, 195, 1436–1443. [Google Scholar] [CrossRef]
- Pepe, P.; Pepe, L.; Tamburo, M.; Marletta, G.; Savoca, F.; Pennisi, M.; Fraggetta, F. 68Ga-PSMA PET/CT and Prostate Cancer Diagnosis: Which SUVmax Value? In Vivo 2023, 37, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- Duncan, I.; Ingold, N.; Martinez-Marroquin, E.; Paterson, C. An Australian experience using Tc-PSMA SPECT/CT in the primary diagnosis of prostate cancer and for staging at biochemical recurrence after local therapy. Prostate 2023, 83, 970–979. [Google Scholar] [CrossRef] [PubMed]
- Schmidkonz, C.; Cordes, M.; Beck, M.; Goetz, T.I.; Schmidt, D.; Prante, O.; Bäuerle, T.; Uder, M.; Wullich, B.; Goebell, P.; et al. SPECT/CT with the PSMA Ligand 99mTc-MIP-1404 for Whole-Body Primary Staging of Patients with Prostate Cancer. Clin. Nucl. Med. 2018, 43, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Vetrone, L.; Mei, R.; Bianchi, L.; Giunchi, F.; Farolfi, A.; Castellucci, P.; Droghetti, M.; Presutti, M.; Degiovanni, A.; Schiavina, R.; et al. Histology and PSMA Expression on Immunohistochemistry in High-Risk Prostate Cancer Patients: Comparison with 68Ga-PSMA PET/CT Features in Primary Staging. Cancers 2023, 15, 1716. [Google Scholar] [CrossRef] [PubMed]
- Goffin, K.E.; Joniau, S.; Tenke, P.; Slawin, K.; Klein, E.A.; Stambler, N.; Strack, T.; Babich, J.; Armor, T.; Wong, V. Phase 2 Study of 99mTc-Trofolastat SPECT/CT to Identify and Localize Prostate Cancer in Intermediate- and High-Risk Patients Undergoing Radical Prostatectomy and Extended Pelvic LN Dissection. J. Nucl. Med. 2017, 58, 1408–1413. [Google Scholar] [CrossRef] [PubMed]
- Berrens, A.C.; Knipper, S.; Marra, G.; van Leeuwen, P.J.; van der Mierden, S.; Donswijk, M.L.; Maurer, T.; van Leeuwen, F.W.B.; van der Poel, H.G. State of the Art in Prostate-specific Membrane Antigen-targeted Surgery—A Systematic Review. Eur. Urol. Open Sci. 2023, 54, 43–55. [Google Scholar] [CrossRef]
- Langsteger, W.; Rezaee, A.; Pirich, C.; Beheshti, M. 18F-NaF-PET/CT and 99mTc-MDP Bone Scintigraphy in the Detection of Bone Metastases in Prostate Cancer. Semin. Nucl. Med. 2016, 46, 491–501. [Google Scholar] [CrossRef]
- Even-Sapir, E.; Metser, U.; Mishani, E.; Lievshitz, G.; Lerman, H.; Leibovitch, I. The detection of bone metastases in patients with high-risk prostate cancer: 99mTc-MDP Planar bone scintigraphy, single- and multi-field-of-view SPECT, 18F-fluoride PET, and 18F-fluoride PET/CT. J. Nucl. Med. 2006, 47, 287–297. [Google Scholar] [PubMed]
- Calais, J.; Fendler, W.P.; Eiber, M.; Gartmann, J.; Chu, F.I.; Nickols, N.G.; Reiter, R.E.; Rettig, M.B.; Marks, L.S.; Ahlering, T.E.; et al. Impact of 68Ga-PSMA-11 PET/CT on the Management of Prostate Cancer Patients with Biochemical Recurrence. J. Nucl. Med. 2018, 59, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Kabunda, J.; Gabela, L.; Kalinda, C.; Aldous, C.; Pillay, V.; Nyakale, N. Comparing 99mTc-PSMA to 99mTc-MDP in Prostate Cancer Staging of the Skeletal System. Clin. Nucl. Med. 2021, 46, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Grünig, H.; Maurer, A.; Thali, Y.; Kovacs, Z.; Strobel, K.; Burger, I.A.; Müller, J. Focal unspecific bone uptake on [18F]-PSMA-1007 PET: A multicenter retrospective evaluation of the distribution, frequency, and quantitative parameters of a potential pitfall in prostate cancer imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4483–4494. [Google Scholar] [CrossRef]
- Grubmüller, B.; Rasul, S.; Baltzer, P.; Fajkovic, H.; D’Andrea, D.; Berndl, F.; Maj-Hes, A.; Grubmüller, K.H.; Mitterhauser, M.; Wadsak, W.; et al. Response assessment using [68Ga]Ga-PSMA ligand PET in patients undergoing systemic therapy for metastatic castration-resistant prostate cancer. Prostate 2020, 80, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Shagera, Q.A.; Karfis, I.; Sideris, S.; Guiot, T.; Woff, E.; Martinez-Chanza, N.; Roumeguere, T.; Gil, T.; Flamen, P.; Artigas, C. Tumor Volume on PSMA PET as a Prognostic Biomarker in Prostate Cancer Patients Treated with Cabazitaxel. Clin. Nucl. Med. 2023, 48, 775–780. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | |
|---|---|
| Number of patients (n) | 18 |
| Age (years) | |
| Median | 71 (54–75) |
| Mean | 68.16 |
| PSA at scan (ng/mL) | |
| Median | 23.3 (4.3–920) |
| Mean | 142.31 |
| ISUP Classification | |
| 2 | n = 1 (6%) |
| 3 | n = 5 (28%) |
| 4 | n = 4 (22%) |
| 5 | n = 8 (44%) |
| Clinical T stage | |
| Tx | n = 4 (22%) |
| T1c | n = 2 (11%) |
| T2a | n = 5 (28%) |
| T2b | n = 1 (6%) |
| T2c | n = 1 (6%) |
| T3 | n = 2 (11%) |
| T4 | n = 3 (16%) |
| Risk Classification according to NCCN | |
| Unfavorable Intermediate | 3 (17%) |
| High Risk | 7 (39%) |
| Very High Risk | 8 (44%) |
| Site | 18F-PSMA 1007 (n) | 99mTc-iPSMA (Observer 1) | 99mTc-iPSMA (Observer 2) |
|---|---|---|---|
| Prostate | 18 | 18 (100%) | 18 (100%) |
| Seminal vesicle | 12 | 12 (100%) | 12 (100%) |
| Locoregional lymph nodes | 62 | 56 (90%) | 55 (88%) |
| Non locoregional lymph nodes | 67 | 57 (85%) | 58 (86%) |
| Bone | 90 | 78 (86%) | 77 (85%) |
| Visceral | 8 | 8 (100%) | 8 (100%) |
| Total | 257 | 229 | 228 |
| Region | 18F-PSMA 1007 (n) | Lowest Diameter Detected | 99mTc-iPSMA (n) | Lowest Diameter Detected | |
|---|---|---|---|---|---|
| mi N1/N2 | |||||
| II | Internal iliac | 17 | 2 mm | 14 | 4 mm |
| EI | External iliac | 22 | 5 mm | 22 | 5 mm |
| OB | Obturator | 19 | 3 mm | 17 | 4 mm |
| PS | Presacral | 1 | 5 mm | 1 | 5 mm |
| OP | Other pelvic | 3 | 3 mm | 3 | 3 mm |
| mi M1a | |||||
| CI | Common Iliac | 19 | 4 mm | 17 | 5 mm |
| RP | Retroperitoneal | 35 | 3 mm | 28 | 3 mm |
| SD | Supradiaphragmatic | 11 | 4 mm | 10 | 5 mm |
| OE | Other extrapelvic | 2 | 6 mm | 2 | 6 mm |
| Patient Number | mi TNM PROMISE V2 PET | mi TNM PROMISE V2 SPECT |
|---|---|---|
| 1 | T3b N2 M0 | T3b N1 M0 |
| 2 | T3b N2 M1a M1b diss 1 | T3b N2 M1a M1b diss 1 |
| 3 | T3b N0 M0 | T3b N0 M0 |
| 4 | T3b N2 M1a | T3b N2 M1a |
| 5 | T2m N0 M0 | T2m N0 M0 |
| 6 | T4 N2 M1a M1b diss 1 M1c | T4 N2 M1a M1b diss 1 M1c |
| 7 | T2u N0 M0 | T2u N0 M0 |
| 8 | T2u N0 M1b diss 1 | T2u N0 M1b diss 1 |
| 9 | T2u N1 M0 | T2u N1 M0 |
| 10 | T4 N2 M1a M1b diss 1 | T4 N2 M1a M1b diss 1 |
| 11 | T3b N2 M1a | T3b N2 M1a |
| 12 | T3b N0 M0 | T3b N0 M0 |
| 13 | T3b N2 M1a M1b oligo 2 | T3b N2 M1a M1b oligo 2 |
| 14 | T2m N0 M0 | T2m N0 M0 |
| 15 | T2m N2 M1a | T2m N2 M1a |
| 16 | T4 N2 M1a M1b diss 1 M1c | T4 N2 M1a M1b diss 1 M1c |
| 17 | T4 N0 M0 | T4 N0 M0 |
| 18 | T3b N0 M0 | T3b N0 M0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vargas-Ahumada, J.E.; González-Rueda, S.D.; Sinisterra-Solís, F.A.; Casanova-Triviño, P.; Pitalúa-Cortés, Q.; Soldevilla-Gallardo, I.; Scavuzzo, A.; Jimenez-Ríos, M.A.; García-Pérez, F.O. Diagnostic Performance of 99mTc-iPSMA SPECT/CT in the Initial Staging of Patients with Unfavorable Intermediate-, High-, and Very High-Risk Prostate Cancer: A Comparative Analysis with 18F-PSMA-1007 PET/CT. Cancers 2023, 15, 5824. https://doi.org/10.3390/cancers15245824
Vargas-Ahumada JE, González-Rueda SD, Sinisterra-Solís FA, Casanova-Triviño P, Pitalúa-Cortés Q, Soldevilla-Gallardo I, Scavuzzo A, Jimenez-Ríos MA, García-Pérez FO. Diagnostic Performance of 99mTc-iPSMA SPECT/CT in the Initial Staging of Patients with Unfavorable Intermediate-, High-, and Very High-Risk Prostate Cancer: A Comparative Analysis with 18F-PSMA-1007 PET/CT. Cancers. 2023; 15(24):5824. https://doi.org/10.3390/cancers15245824
Chicago/Turabian StyleVargas-Ahumada, Joel E., Sofía Denisse González-Rueda, Fabio Andrés Sinisterra-Solís, Pamela Casanova-Triviño, Quetzali Pitalúa-Cortés, Irma Soldevilla-Gallardo, Anna Scavuzzo, Miguel Angel Jimenez-Ríos, and Francisco Osvaldo García-Pérez. 2023. "Diagnostic Performance of 99mTc-iPSMA SPECT/CT in the Initial Staging of Patients with Unfavorable Intermediate-, High-, and Very High-Risk Prostate Cancer: A Comparative Analysis with 18F-PSMA-1007 PET/CT" Cancers 15, no. 24: 5824. https://doi.org/10.3390/cancers15245824
APA StyleVargas-Ahumada, J. E., González-Rueda, S. D., Sinisterra-Solís, F. A., Casanova-Triviño, P., Pitalúa-Cortés, Q., Soldevilla-Gallardo, I., Scavuzzo, A., Jimenez-Ríos, M. A., & García-Pérez, F. O. (2023). Diagnostic Performance of 99mTc-iPSMA SPECT/CT in the Initial Staging of Patients with Unfavorable Intermediate-, High-, and Very High-Risk Prostate Cancer: A Comparative Analysis with 18F-PSMA-1007 PET/CT. Cancers, 15(24), 5824. https://doi.org/10.3390/cancers15245824