
Potential of Fecal Carcinoembryonic Antigen for Noninvasive Detection of Colorectal Cancer: A Systematic Review

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Risk of Bias and Applicability Assessment of Each Study
3. Results
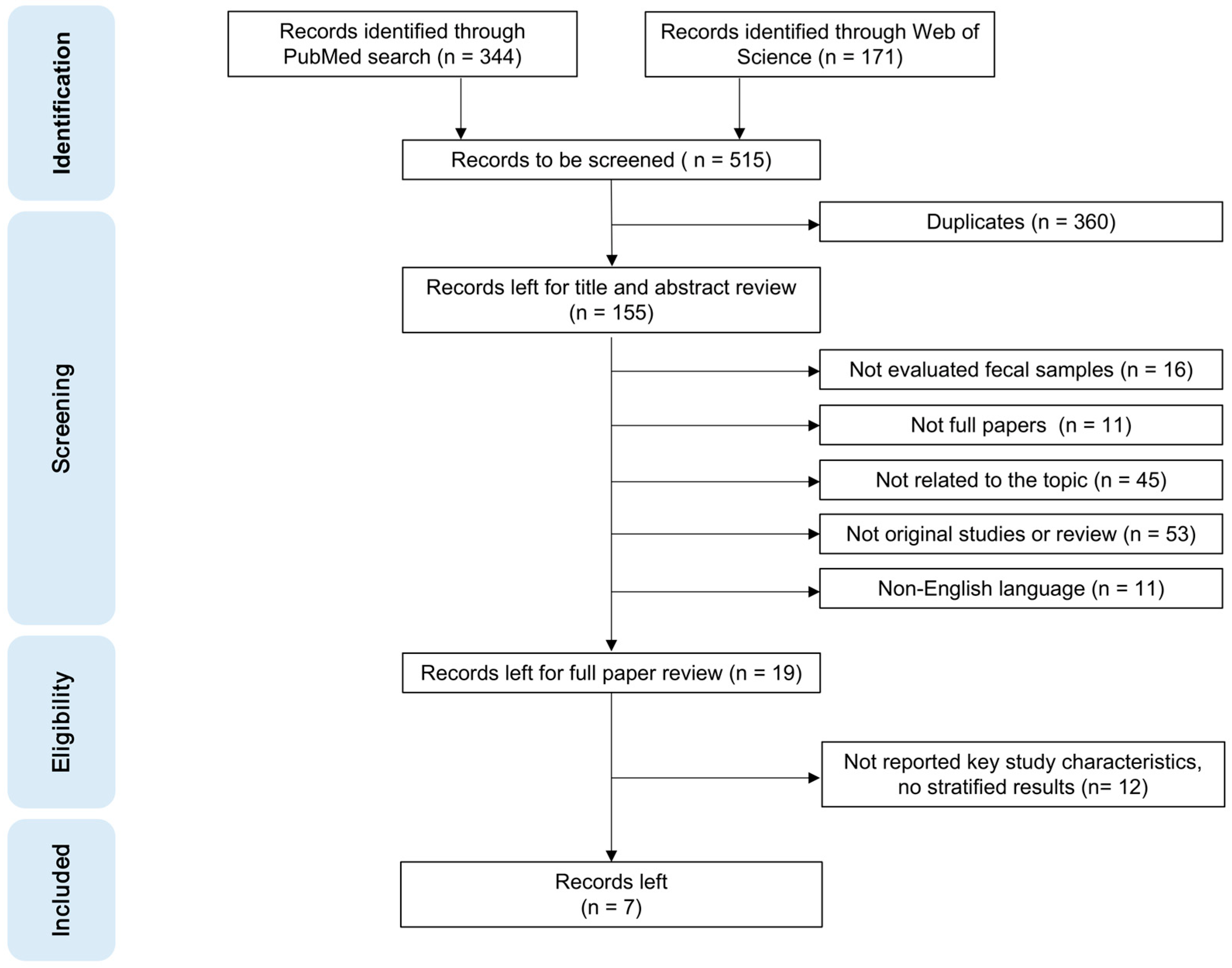
3.1. Literature Search Results
3.2. Study Characteristics
3.3. FCEA and SCEA Concentrations in Different Groups
3.4. Different Methods for Stool Sampling and Fecal CEA Quantitative Detection
3.5. Diagnostic Performance of Fecal CEA Compared with Serum CEA
3.6. Assessment of Risk of Bias and Applicability across Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Morgan, E.; Arnold, M.; Gini, A.; Lorenzoni, V.; Cabasag, C.J.; Laversanne, M.; Vignat, J.; Ferlay, J.; Murphy, N.; Bray, F. Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from globocan. Gut 2023, 72, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Brenner, H.; Chen, C. The colorectal cancer epidemic: Challenges and opportunities for primary, secondary and tertiary prevention. Br. J. Cancer 2018, 119, 785–792. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, R.; Guo, F.; Heisser, T.; Hackl, M.; Ihle, P.; De Schutter, H.; Van Damme, N.; Valerianova, Z.; Atanasov, T.; Májek, O.; et al. Colorectal cancer incidence, mortality, and stage distribution in european countries in the colorectal cancer screening era: An international population-based study. Lancet Oncol. 2021, 22, 1002–1013. [Google Scholar] [CrossRef] [PubMed]
- González-Suárez, B.; Pagés, M.; Araujo, I.K.; Romero, C.; Rodríguez de Miguel, C.; Ayuso, J.R.; Pozo, À.; Vila-Casadesús, M.; Serradesanferm, A.; Ginès, À.; et al. Colon capsule endoscopy versus CT colonography in FIT-positive colorectal cancer screening subjects: A prospective randomised trial-the VICOCA study. BMC Med. 2020, 18, 255. [Google Scholar] [CrossRef]
- Rabeneck, L.; Saskin, R.; Paszat, L.F. Onset and clinical course of bleeding and perforation after outpatient colonoscopy: A population-based study. Gastrointest. Endosc. 2011, 73, 520–523. [Google Scholar] [CrossRef]
- Rabeneck, L.; Paszat, L.F.; Hilsden, R.J.; Saskin, R.; Leddin, D.; Grunfeld, E.; Wai, E.; Goldwasser, M.; Sutradhar, R.; Stukel, T.A. Bleeding and perforation after outpatient colonoscopy and their risk factors in usual clinical practice. Gastroenterology 2008, 135, 1899–1906. [Google Scholar] [CrossRef]
- Frazier, A.L.; Colditz, G.A.; Fuchs, C.S.; Kuntz, K.M. Cost-effectiveness of screening for colorectal cancer in the general population. JAMA 2000, 284, 1954–1961. [Google Scholar] [CrossRef]
- Sonnenberg, A.; Delcò, F.; Inadomi, J.M. Cost-effectiveness of colonoscopy in screening for colorectal cancer. Ann. Intern. Med. 2000, 133, 573–584. [Google Scholar] [CrossRef]
- Helsingen, L.M.; Vandvik, P.O.; Jodal, H.C.; Agoritsas, T.; Lytvyn, L.; Anderson, J.C.; Auer, R.; Murphy, S.B.; Almadi, M.A.; Corley, D.A.; et al. Colorectal cancer screening with faecal immunochemical testing, sigmoidoscopy or colonoscopy: A clinical practice guideline. BMJ 2019, 367, l5515. [Google Scholar] [CrossRef] [PubMed]
- Grobbee, E.J.; van der Vlugt, M.; van Vuuren, A.J.; Stroobants, A.K.; Mallant-Hent, R.C.; Lansdorp-Vogelaar, I.; Bossuyt, P.M.M.; Kuipers, E.J.; Dekker, E.; Spaander, M.C.W. Diagnostic yield of one-time colonoscopy vs. one-time flexible sigmoidoscopy vs. multiple rounds of mailed fecal immunohistochemical tests in colorectal cancer screening. Clin. Gastroenterol. Hepatol. 2020, 18, 667–675.e1. [Google Scholar] [CrossRef] [PubMed]
- Young, G.P.; Symonds, E.L.; Allison, J.E.; Cole, S.R.; Fraser, C.G.; Halloran, S.P.; Kuipers, E.J.; Seaman, H.E. Advances in fecal occult blood tests: The FIT revolution. Dig. Dis. Sci. 2015, 60, 609–622. [Google Scholar] [CrossRef]
- Lee, J.K.; Liles, E.G.; Bent, S.; Levin, T.R.; Corley, D.A. Accuracy of fecal immunochemical tests for colorectal cancer: Systematic review and meta-analysis. Ann. Intern. Med. 2014, 160, 171. [Google Scholar] [CrossRef] [PubMed]
- Gies, A.; Cuk, K.; Schrotz-King, P.; Brenner, H. Direct comparison of diagnostic performance of 9 quantitative fecal immunochemical tests for colorectal cancer screening. Gastroenterology 2018, 154, 93–104. [Google Scholar] [CrossRef]
- Morikawa, T.; Kato, J.; Yamaji, Y.; Wada, R.; Mitsushima, T.; Shiratori, Y. A comparison of the immunochemical fecal occult blood test and total colonoscopy in the asymptomatic population. Gastroenterology 2005, 129, 422–428. [Google Scholar] [CrossRef]
- Konishi, T.; Shimada, Y.; Hsu, M.; Tufts, L.; Jimenez-Rodriguez, R.; Cercek, A.; Yaeger, R.; Saltz, L.; Smith, J.J.; Nash, G.M.; et al. Association of preoperative and postoperative serum carcinoembryonic antigen and colon cancer outcome. JAMA Oncol. 2018, 4, 309–315. [Google Scholar] [CrossRef]
- Goldstein, M.J.; Mitchell, E.P. Carcinoembryonic antigen in the staging and follow-up of patients with colorectal cancer. Cancer Investig. 2005, 23, 338–351. [Google Scholar] [CrossRef]
- Wang, Y.-R.; Yan, J.-X.; Wang, L.-N. The diagnostic value of serum carcino-embryonic antigen, alpha fetoprotein and carbohydrate antigen 19-9 for colorectal cancer. J. Cancer Res. Ther. 2014, 10 (Suppl. S4), 307–309. [Google Scholar] [CrossRef]
- Cruz, A.; Carvalho, C.M.; Cunha, A.; Crespo, A.; Iglesias, Á.; García-Nimo, L.; Freitas, P.P.; Cubiella, J. Faecal diagnostic biomarkers for colorectal cancer. Cancers 2021, 13, 5568. [Google Scholar] [CrossRef]
- Li, L.; Gu, W.; Wu, X.; Ao, Y.; Song, Y.; Li, X.; Zeng, Q. Superiority of fecal carcinoembryonic antigen as diagnosis marker for adenomatous polyposis coli and asymptomatic colorectal cancer. Ther. Adv. Gastroenterol. 2021, 14, 17562848211062792. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Xing, S.; Wu, M.; Ao, Y.; Zheng, X.; Cai, R.; Han, R.; Li, J.; Li, X.; Zeng, Q. Fecal CEA has an advantage in the diagnosis of colorectal cancer at early stage. Cancer Control J. Moffitt Cancer Cent. 2021, 28, 10732748211048292. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, S.; Park, S.; Jeon, H.; Lee, W.; Kim, J.K.; Cho, M.; Kim, M.; Lim, J.; Kang, C.S.; et al. Gastrointestinal tract cancer screening using fecal carcinoembryonic antigen. Ann. Clin. Lab. Sci. 2003, 33, 32–38. [Google Scholar] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Sugano, K.; Ohkura, H.; Hirohashi, S.; Shimosato, Y.; Sakurai, Y.; Kodaira, S.; Abe, O. Detection of increased fecal carcinoembryonic antigen and its characterization as a membrane-bound form in colorectal carcinoma and other gastrointestinal disorders. Jpn. J. Cancer Res. Gann 1989, 80, 1156–1160. [Google Scholar] [CrossRef]
- Stubbs, R.S.; Nadkarni, D.M.; Monsey, H.A. Faecal carcinoembryonic antigen in colorectal cancer patients. Gut 1986, 27, 901–905. [Google Scholar] [CrossRef]
- Kitsukawa, Y. Immunoreactive carcinoembryonic antigen [CEA] levels in feces from colorectal cancer patients. Jpn. J. Surg. 1979, 9, 102–109. [Google Scholar] [CrossRef]
- Fujimoto, S.; Kitsukawa, U.; Itoh, K. Carcinoembryonic antigen (CEA) in gastric juice or feces as an aid in the diagnosis of gastrointestinal cancer. Ann. Surg. 1979, 189, 34–38. [Google Scholar] [CrossRef]
- Lin, J.S.; Perdue, L.A.; Henrikson, N.B.; Bean, S.I.; Blasi, P.R. Screening for colorectal cancer: Updated evidence report and systematic review for the US preventive services task force. JAMA 2021, 325, 1978–1998. [Google Scholar] [CrossRef]
- Mo, S.; Dai, W.; Wang, H.; Lan, X.; Ma, C.; Su, Z.; Xiang, W.; Han, L.; Luo, W.; Zhang, L.; et al. Early detection and prognosis prediction for colorectal cancer by circulating tumour DNA methylation haplotypes: A multicentre cohort study. EClinicalMedicine 2023, 55, 101717. [Google Scholar] [CrossRef] [PubMed]
- Ewald, N.; Toepler, M.; Akinci, A.; Kloer, H.U.; Bretzel, R.G.; Hardt, P.D. Pyruvate kinase M2 (tumor M2-PK) as a screening tool for colorectal cancer (CRC). A review of current published data. Z. Gastroenterol. 2005, 43, 1313–1317. [Google Scholar] [CrossRef] [PubMed]
- Jelski, W.; Mroczko, B. Biochemical markers of colorectal cancer—Present and future. Cancer Manag. Res. 2020, 12, 4789–4797. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Zhu, A.; Bhardwaj, M.; Schrotz-King, P.; Brenner, H. Fecal microRNAs, fecal microRNA panels, or combinations of fecal microRNAs with fecal hemoglobin for early detection of colorectal cancer and its precursors: A systematic review. Cancers 2021, 14, 65. [Google Scholar] [CrossRef]
- Hegedus, E.J.; Moody, J. Clinimetrics corner: The many faces of selection bias. J. Man. Manip. Ther. 2010, 18, 69–73. [Google Scholar] [CrossRef]
- Bell, K.J.; Macaskill, P.; Loy, C. Test accuracy and potential sources of bias in diagnostic test evaluation. Med. J. Aust. 2020, 212, 10–13. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| First Author, Year | Study Type | Country | Race | Study Groups | Population (n) | Mean Age (Range) | Sex, Female (%) | Fecal CEA (ng/mg) | p Value | Serum CEA (ng/mL) | p Value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Li, 2021 [21] | Case-control | China | Asian | CRC | 166 | 59 (25–87) | 70 (42.2) | 148.4 (80.91–245.7) | ref | 3.28 (1.95–8.73) | ref |
| APC | 46 | 53 (21–73) | 18 (39.1) | 115.7 (65.14–186.6) | 0.096 a | 1.75 (1.27–2.79) | <0.001 a | ||||
| NGIC | 60 | 52 (21–82) | 24 (40.0) | 97.58 (56.83–130.6) | <0.001 a | 2.29 (1.22–4.44) | 0.002 a | ||||
| HC | 164 | 40 (20–65) | 91 (55.5) | 53.54 (31.48–86.51) | <0.001 a | 1.47 (0.95–2.25) | <0.001 a | ||||
| Li, 2021 [22] | Case-control | China | Asian | CRC | 115 | 59 ± 11 | 51 (44.4) | 149.76 (81.0–240.9) | ref | 3.28 (1.75–9.92) | ref |
| APC | 35 | 46 ± 12 b | 89 (48.6) b | 113.58 (63.9–182.97) | 0.167 | 1.97 (1.34–3.21) | <0.001 | ||||
| NGIC | 46 | 83.58 (53.42–135.29) | <0.001 | 1.84 (1.17–4.67) | 0.033 | ||||||
| HC | 102 | 46.19 (26.17–84.72) | <0.001 | 1.50 (1.09–2.17) | <0.001 | ||||||
| Kim, 2003 [23] | Case-control | South Korea | Asian | CRC | 28 | 45.2 ± 63.8 | ref | 8.87 ± 13.28 | ref | ||
| Invasive GC | 19 | 42.9 ± 38.8 | 0.879 | 5.09 ± 8.57 | 0.242 | ||||||
| Early GC | 13 | 42.0 ± 89.6 | 0.909 | 3.13 ± 2.51 | 0.035 | ||||||
| BGID | 20 | 4.5 ± 8.2 | 0.002 | 1.66 ± 2.03 | 0.008 | ||||||
| HC | 240 | 3.7 ± 3.5 | 0.002 | 1.14 ± 1.0 | 0.005 | ||||||
| Sugano, 1989 [26] | Case-control | Japan | Asian | CRC | 24 | 0.46 ± 0.51 μg/mL | ref | / | / | ||
| BGID | 55 | 0.17± 0.19 μg/mL | <0.001 | / | / | ||||||
| HC | 15 | 0.04 ± 0.03 μg/mL | <0.001 | / | / | ||||||
| Stubbs, 1986 [27] | Case-control | United Kingdom | European | CRC | 24 | 10.43 ± 2.39 | ref | / | / | ||
| BGID | 14 | 7.12 ± 1.39 | <0.001 | / | / | ||||||
| HC | 20 | 5.43 ± 1.95 | <0.001 | / | / | ||||||
| Kitsukawa, 1979 [28] | Case-control | Japan | Asian | CRC | 20 | 215 ± 93 ng/g | ref | / | / | ||
| HC | 20 | 77.7 ± 42.9 ng/g | <0.001 | / | / | ||||||
| Fujimoto, 1979 [29] | Case-control | Japan | Asian | Dukes A | 4 | 55 (41–74) c | 12 (54.5) c | 193 ± 51 ng/g | 0.014 | / | / |
| Dukes B | 3 | 178 ± 73 ng/g | 0.135 | / | / | ||||||
| Dukes C | 9 | 213 ± 90 ng/g | 0.002 | / | / | ||||||
| Liver metastasis | 6 | 267 ± 95 ng/g | 0.004 | / | / | ||||||
| HC | 20 | 51 (40–67) | 2 (10.0) | 78 ± 42 ng/g | ref | / | / |
| Study | Stool Sampling and Processing Methods | Fecal CEA Detection Methods |
|---|---|---|
| Li, 2021 [21] | 0.1 mg of fresh feces was collected by fecal collection tubes from three different locations, homogenized for 2 min and then centrifuged for 10 min at 10,000 r/min. The supernatant was retained. The samples were filtered, if necessary. | ECLIA Kit (Roche Diagnostics, Mannheim,, Germany) |
| Li, 2021 [22] | Stool samples were collected from CRC patients within 7 days before surgery or treatment, and from healthy individuals on the day of the physical examination. Loose stools, watery stools, blood stools, or hard stools are excluded. Other steps including the amount of stool were the same as Li et al.’s study above. | ECLIA (Roche Diagnostics, Mannheim, Germany) |
| Kim, 2003 [23] | Stool samples were collected within 1 week after the histologic diagnoses were made. About 80 mg of each stool sample were added to 800 µL of pH 7.4 PBS. After twice freezing and thawing procedures, the mixtures were filtered through a polyvinyl alcohol sponge filter. | Automated immunoassay system (Elecsys 2010, Roche Diagnostics, Mannheim, Germany) |
| Sugano, 1989 [26] | Stool samples (20 mg) were dissolved in 5 mL of 0.1 M, pH 7.4 PBS containing 0.15 M NaCl and 0.2% sodium azide. After centrifugation at 3000 rpm for 15 min, supernatants were recovered. | A “forward sandwich” radioimmunometric assay |
| Stubbs, 1986 [27] | One entire stool sample was collected and weighed before surgery, homogenized with 100 mL 0–9% NaCl and an aliquot weighing about 500 mg stool was taken. 5 mL PBS, pH 7.1, were added, mixed thoroughly and incubated at 80 °C for 10 min in a water bath. After centrifuging for 15 min at 600× g, the supernatant was added to a further 5 mL pH 7.1 PBS and recentrifuged for 10 min at 600× g. Then the supernatant was filtered through a number 1 Whatman filter paper. | ELISA |
| Kitsukawa, 1979 [28] | Stool samples were collected without barium, blood and diarrhea. About 500 mg stools were put into ten-fold the quantity of 0.1 M acetate buffer (pH 5.0) and were mixed by stirring. Then the stools were centrifuged at 2500× g for 10 min. The supernatant was diluted with an equal volume of acetate buffer, incubated at 85 °C for 10 min in a water bath and then centrifuged for 5 min at 2500× g. | Radioimmunoassay utilizing the “one step sandwich method” |
| Fujimoto, 1979 [29] | The same as Kitsukawa et al.’s study above. | Radioimmunoassay utilizing the “one step sandwich method” |
| Study | Groups | Fecal CEA | Serum CEA | ||||
|---|---|---|---|---|---|---|---|
| SEN (%) | SPE (%) | AUC | SEN (%) | SPE (%) | AUC | ||
| Li, 2021 [21] | CRC vs. NGIH+HC | / | / | 0.802 | / | / | 0.757 |
| APC vs. NGIH+HC | / | / | 0.704 | / | / | 0.525 | |
| CRC+APC vs. NGIC+HC | / | / | 0.781 | / | / | 0.861 | |
| Stage I CRC+ APC vs. NGIC+HC | / | / | 0.729 | / | / | 0.589 | |
| Li, 2021 [22] | CRC vs. NGIC+HC | 76.50 | 73.00 | 0.802 | 38.30 | 91.00 | 0.735 |
| Stage I+II CRC vs. HC | 78.70 | 73.50 | 0.831 | 29.80 | 98.04 | 0.750 | |
| Kim, 2003 [23] | CRC vs. HC | 85.70 | 92.92 | / | 39.29 | 96.66 | / |
| CRC vs. BGID | 85.70 | 95.00 | / | 39.29 | 90.00 | / | |
| Sugano, 1989 [26] | CRC vs. HC | 50.00 a | 100.00 a | ||||
| Kitsukawa, 1979 [28] | CRC vs. HC | 85.00 a | / | / | 35.00 a | / | / |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Stassen, L.; Schrotz-King, P.; Zhao, Z.; Cardoso, R.; Raut, J.R.; Bhardwaj, M.; Brenner, H. Potential of Fecal Carcinoembryonic Antigen for Noninvasive Detection of Colorectal Cancer: A Systematic Review. Cancers 2023, 15, 5656. https://doi.org/10.3390/cancers15235656
Li X, Stassen L, Schrotz-King P, Zhao Z, Cardoso R, Raut JR, Bhardwaj M, Brenner H. Potential of Fecal Carcinoembryonic Antigen for Noninvasive Detection of Colorectal Cancer: A Systematic Review. Cancers. 2023; 15(23):5656. https://doi.org/10.3390/cancers15235656
Chicago/Turabian StyleLi, Xianzhe, Lara Stassen, Petra Schrotz-King, Zitong Zhao, Rafael Cardoso, Janhavi R. Raut, Megha Bhardwaj, and Hermann Brenner. 2023. "Potential of Fecal Carcinoembryonic Antigen for Noninvasive Detection of Colorectal Cancer: A Systematic Review" Cancers 15, no. 23: 5656. https://doi.org/10.3390/cancers15235656
APA StyleLi, X., Stassen, L., Schrotz-King, P., Zhao, Z., Cardoso, R., Raut, J. R., Bhardwaj, M., & Brenner, H. (2023). Potential of Fecal Carcinoembryonic Antigen for Noninvasive Detection of Colorectal Cancer: A Systematic Review. Cancers, 15(23), 5656. https://doi.org/10.3390/cancers15235656